
Subdural Lesions Linking Additional Intracranial Spaces and Chronic Subdural Hematomas: A Narrative Review with Mutual Correlation and Possible Mechanisms behind High Recurrence


{kind=link}
{kind=link}
Abstract
:1. Preface
2. A Potential Area Dissected by Acquired Factors, the Subdural Space—Clinical Considerations and Pathological States Derived from It
3. Subdural Fluid Collection
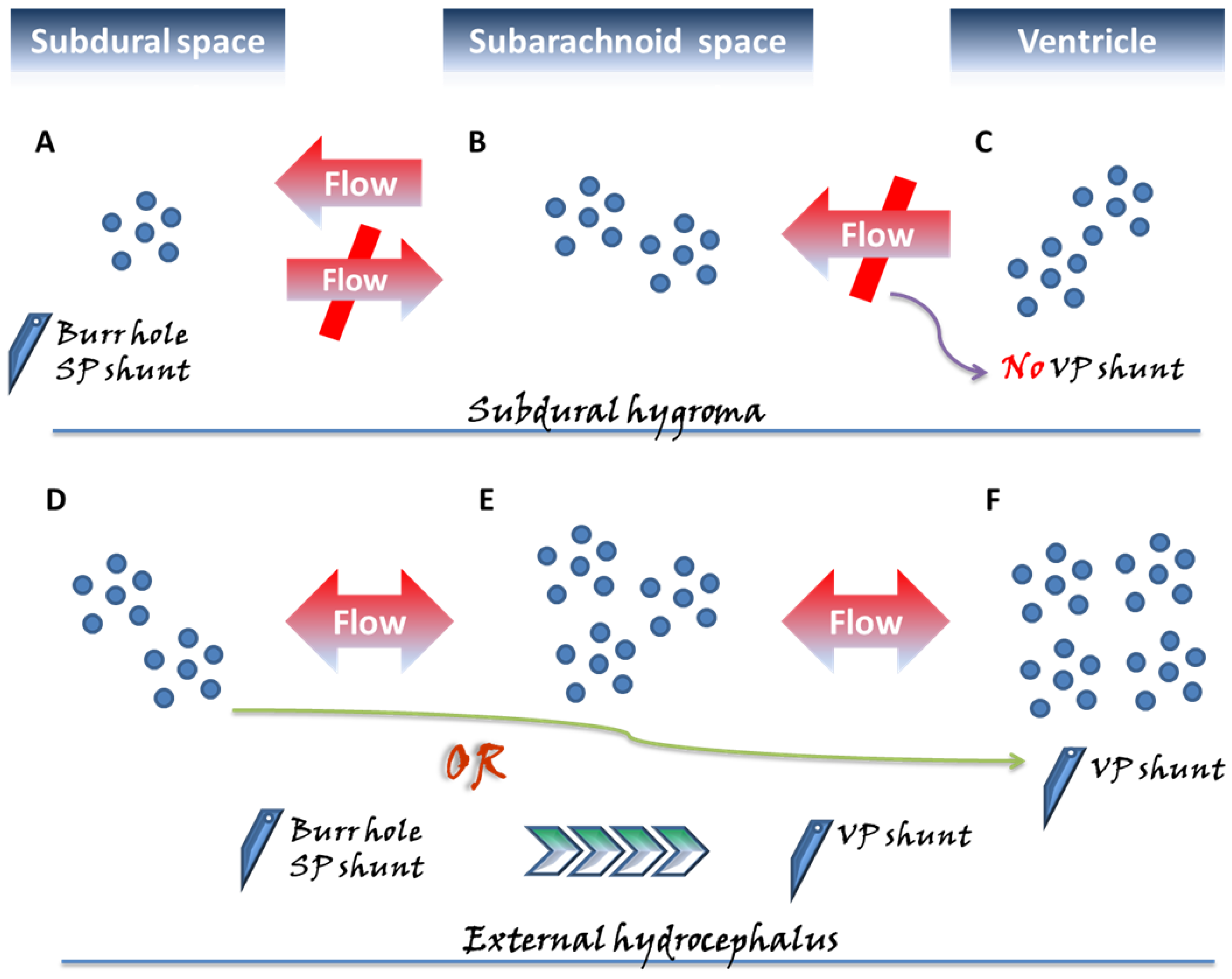
3.1. Subdural Hygroma and Its Special Case—External Hydrocephalus
- (i)
- Arachnoidal injury
- (ii)
- Inactivity of the blood–brain barrier (BBB)
- (iii)
- Neomembrane formation
3.2. Diverse Views on the Diagnosis and Clinical Management of the Two Distinguished Subdural Lesions [22,36]
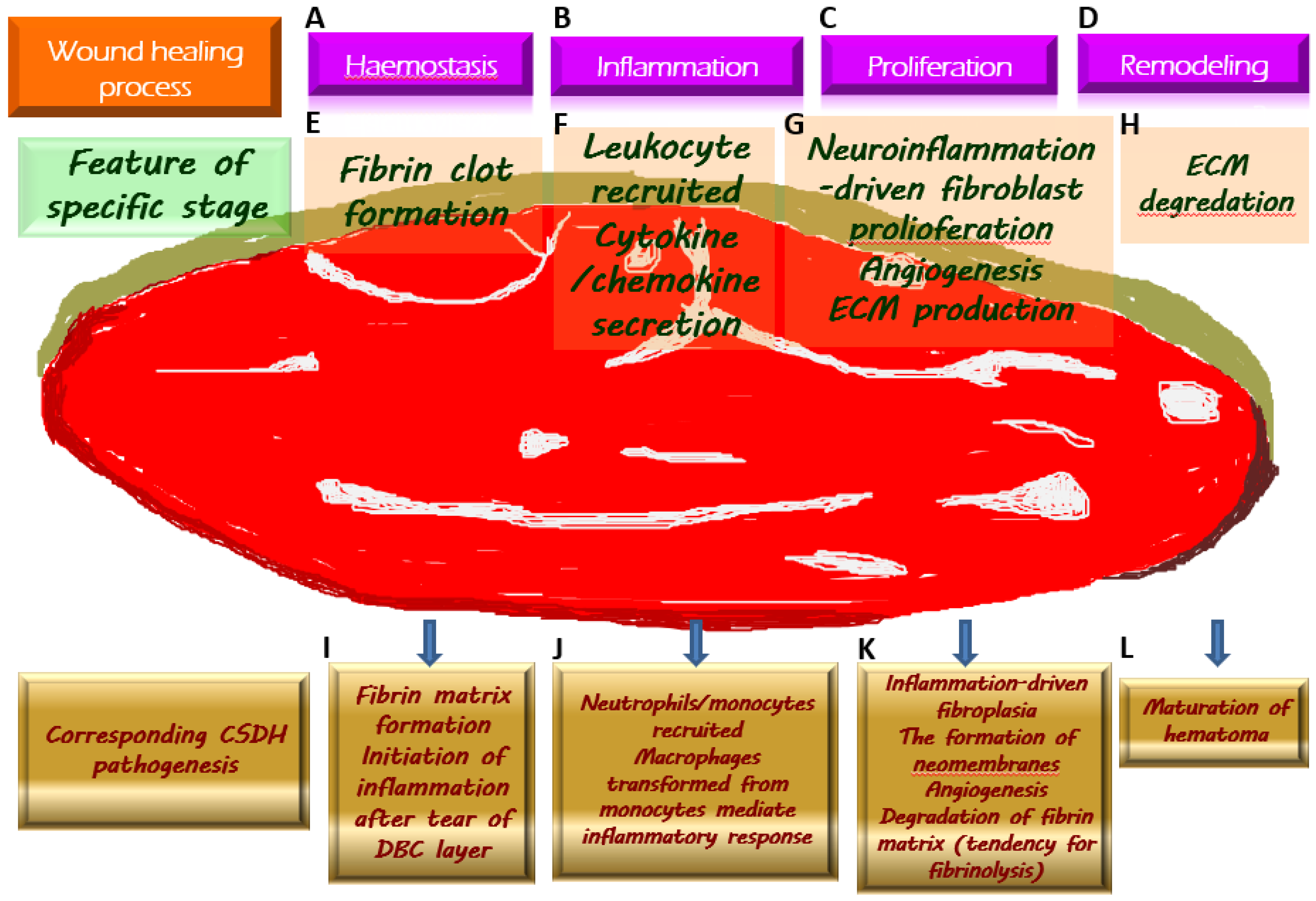
4. The Formation of Chronic Subdural Hematoma
4.1. Inflammatory Response Provoked by DBC Layer Damage as an Initiator of CSDH Development
4.2. Inappropriate Inflammation Promotes the Production of Neomembranes
4.3. Inflammation-Driven Angiogenesis Leads to Microhemorrhages on the Neomembrane Surrounding CSDH
4.4. Hyperfibrinolysis Causes CSDH to Be Less Susceptible to Coagulation, Creating a Vicious Cycle along with Microbleeding from Neovascularization
5. The Complex Pathogenesis Previously Described Accounted for the High Degree of Recurrence after Surgery
6. Concluding Remarks and Perspectives
Funding
Conflicts of Interest
References
- Rauhala, M.; Helén, P.; Seppä, K.; Huhtala, H.; Iverson, G.L.; Niskakangas, T.; Öhman, J.; Luoto, T.M. Long-term excess mortality after chronic subdural hematoma. Acta Neurochir. 2020, 162, 1467–1478. [Google Scholar] [CrossRef] [Green Version]
- Derk, J.; Jones, H.E.; Como, C.; Pawlikowski, B.; Siegenthaler, J.A. Living on the Edge of the CNS: Meninges Cell Diversity in Health and Disease. Front. Cell. Neurosci. 2021, 15, 703944. [Google Scholar] [CrossRef]
- Herath, H.; Matthias, A.T.; Kulatunga, A. Acute on chronic bilateral subdural hematoma presenting with acute complete flaccid paraplegia and urinary retention mimicking an acute spinal cord injury: A case report. BMC Res. Notes 2017, 10, 627. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.S.; Alugolu, R. Chronic subdural hematoma presenting as diplegia-A rare presentation. J. Neurosci. Rural Pract. 2014, 5, 445–446. [Google Scholar] [CrossRef] [PubMed]
- Monserrate, A.; De Jesus, O. Huge chronic subdural haematoma formation in an encephalomalacia stroke cavity. BMJ Case Rep. 2020, 13, e236928. [Google Scholar] [PubMed]
- Won, S.Y.; Dubinski, D.; Sautter, L.; Hattingen, E.; Seifert, V.; Rosenow, F.; Freiman, T.; Strzelczyk, A.; Konczalla, J. Seizure and status epilepticus in chronic subdural hematoma. Acta Neurol. Scand. 2019, 140, 194–203. [Google Scholar] [CrossRef]
- Sundblom, J.; Sandberg, E.; Ronne-Engström, E. Trauma Mechanisms and Surgical Outcomes in the Elderly Patient with Chronic Subdural Hematoma. Can. Geriatr. J. 2022, 25, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Link, T.W.; Boddu, S.; Paine, S.M.; Kamel, H.; Knopman, J. Middle Meningeal Artery Embolization for Chronic Subdural Hematoma: A Series of 60 Cases. Neurosurgery 2019, 85, 801–807. [Google Scholar] [CrossRef]
- Cofano, F.; Pesce, A.; Vercelli, G.; Mammi, M.; Massara, A.; Minardi, M.; Palmieri, M.; D’Andrea, G.; Fronda, C.; Lanotte, M.M.; et al. Risk of Recurrence of Chronic Subdural Hematomas After Surgery: A Multicenter Observational Cohort Study. Front. Neurol. 2020, 11, 560269. [Google Scholar] [CrossRef] [PubMed]
- Jang, K.M.; Choi, H.H.; Mun, H.Y.; Nam, T.K.; Park, Y.S.; Kwon, J.T. Critical Depressed Brain Volume Influences the Recurrence of Chronic Subdural Hematoma after Surgical Evacuation. Sci. Rep. 2020, 10, 1145. [Google Scholar] [CrossRef]
- Miah, I.P.; Tank, Y.; Rosendaal, F.R.; Peul, W.C.; Dammers, R.; Lingsma, H.F.; den Hertog, H.M.; Jellema, K.; van der Gaag, N.A. Radiological prognostic factors of chronic subdural hematoma recurrence: A systematic review and meta-analysis. Neuroradiology 2021, 63, 27–40. [Google Scholar] [CrossRef]
- Moshayedi, P.; Liebeskind, D.S. Middle Meningeal Artery Embolization in Chronic Subdural Hematoma: Implications of Pathophysiology in Trial Design. Front. Neurol. 2020, 11, 923. [Google Scholar] [CrossRef] [PubMed]
- Kinaci, A.; Bergmann, W.; Bleys, R.L.; van der Zwan, A.; van Doormaal, T.P. Histologic Comparison of the Dura Mater among Species. Comp. Med. 2020, 70, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Ghannam, J.Y.; Al Kharazi, K.A. Neuroanatomy, Cranial Meninges; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Castro Dias, M.; Mapunda, J.A.; Vladymyrov, M.; Engelhardt, B. Structure and Junctional Complexes of Endothelial, Epithelial and Glial Brain Barriers. Int. J. Mol. Sci. 2019, 20, 5372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weller, R.O.; Sharp, M.M.; Christodoulides, M.; Carare, R.O.; Møllgård, K. The meninges as barriers and facilitators for the movement of fluid, cells and pathogens related to the rodent and human CNS. Acta Neuropathol. 2018, 135, 363–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mortazavi, M.M.; Quadri, S.A.; Khan, M.A.; Gustin, A.; Suriya, S.S.; Hassanzadeh, T.; Fahimdanesh, K.M.; Adl, F.H.; Fard, S.A.; Taqi, M.A.; et al. Subarachnoid Trabeculae: A Comprehensive Review of Their Embryology, Histology, Morphology, and Surgical Significance. World Neurosurg. 2018, 111, 279–290. [Google Scholar] [CrossRef]
- DeSisto, J.; O’Rourke Bonney, S.R.; Jones, H.E.; Guimiot, F.; Jones, K.L.; Siegenthaler, J.A. A cellular atlas of the developing meninges reveals meningeal fibroblast diversity and function. bioRxiv 2019, 648642. [Google Scholar] [CrossRef]
- Kapeliotis, M.; Gavrila Laic, R.A.; Peñas, A.J.; Vander Sloten, J.; Vanden Berghe, P.; Famaey, N.; Depreitere, B. Collagen fibre orientation in human bridging veins. Biomech. Model. Mechanobiol. 2020, 19, 2455–2489. [Google Scholar] [CrossRef]
- Nouri, A.; Gondar, R.; Schaller, K.; Meling, T. Chronic Subdural Hematoma (cSDH): A review of the current state of the art. Brain Spine 2021, 1, 100300. [Google Scholar] [CrossRef] [PubMed]
- Filho, P.T.H.; Pereira, T.M.R.; Zanini, M.A. Epidemiological Features of Patients with Subdural Hygroma in a Prospective Case Series. Arq. Bras. De Neurocir. 2017, 46, 203–206. [Google Scholar]
- Wu, R.; Ye, Y.; Ma, T.; Jia, G.; Qin, H. Management of subdural effusion and hydrocephalus following decompressive craniectomy for posttraumatic cerebral infarction in a patient with traumatic brain injury: A case report. BMC Surg. 2019, 19, 26. [Google Scholar] [CrossRef] [PubMed]
- Murata, K. Chronic subdural hematoma may be preceded by persistent traumatic subdural effusion. Neurol. Med. Chir. 1993, 33, 691–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zahl, S.M.; Egge, A.; Helseth, E.; Wester, K. Benign external hydrocephalus: A review, with emphasis on management. Neurosurg. Rev. 2011, 34, 417–432. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Peng, H.; Shao, X.; Yao, L.; Liu, J.; Tian, J.; Sun, L.; Dai, Y.; Jiang, X.; Cheng, L. Prediction of Risk Factors for the Evolution of Traumatic Subdural Effusion into Chronic Subdural Hematoma. Neuropsychiatr. Dis. Treat. 2020, 16, 943–948. [Google Scholar] [CrossRef] [Green Version]
- Miki, K.; Abe, H.; Morishita, T.; Hayashi, S.; Yagi, K.; Arima, H.; Inoue, T. Double-crescent sign as a predictor of chronic subdural hematoma recurrence following burr-hole surgery. J. Neurosurg. 2019, 131, 1905–1911. [Google Scholar] [CrossRef]
- Kim, B.O.; Kim, J.Y.; Whang, K.; Cho, S.M.; Oh, J.W.; Koo, Y.M.; Hu, C.; Pyen, J.S.; Choi, J.W. The Risk Factors of Subdural Hygroma after Decompressive Craniectomy. Korean J. Neurotrauma 2018, 14, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Prieto, R.; Soriano, M.C.; Ortega, C.; Kalantari, T.; Rabanal, A.P. Subdural fluid accumulation caused by ventriculoperitoneal shunt underdrainage: A rare and paradoxical complication. Surg. Neurol. Int. 2020, 11, 451. [Google Scholar] [CrossRef]
- Singh, G.; Zuback, A.; Gattu, R.; Kilimnik, G.; Vaysberg, A. Subdural hygroma after spontaneous rupture of an arachnoid cyst in a pediatric patient: A case report. Radiol. Case Rep. 2021, 16, 309–311. [Google Scholar] [CrossRef]
- Jeon, S.W.; Choi, J.H.; Jang, T.W.; Moon, S.M.; Hwang, H.S.; Jeong, J.H. Risk factors associated with subdural hygroma after decompressive craniectomy in patients with traumatic brain injury: A comparative study. J. Korean Neurosurg. Soc. 2011, 49, 355–358. [Google Scholar] [CrossRef] [PubMed]
- Bora, A.; Yokuş, A.; Batur, A.; Bulut, M.D.; Yavuz, A.; Gülşen, İ.; Özgökçe, M.; Arslan, M. Spontaneous Rupture of the Middle Fossa Arachnoid Cyst into the Subdural Space: Case Report. Pol. J. Radiol. 2015, 80, 324–327. [Google Scholar]
- Marino, M.A.; Morabito, R.; Vinci, S.; Germanò, A.; Briguglio, M.; Alafaci, C.; Mormina, E.; Longo, M.; Granata, F. Benign external hydrocephalus in infants. A single centre experience and literature review. Neuroradiol. J. 2014, 27, 245–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gergelé, L.; Manet, R.; Kolias, A.; Czosnyka, M.; Lalou, A.; Smielewski, P.; Hutchinson, P.J.; Czosnyka, Z.H. External Hydrocephalus After Traumatic Brain Injury: Retrospective Study of 102 Patients. Acta Neurochir. Suppl. 2021, 131, 35–38. [Google Scholar] [PubMed]
- Akins, P.T.; Guppy, K.H. Are Hygromas and Hydrocephalus After Decompressive Craniectomy Caused by Impaired Brain Pulsatility, Cerebrospinal Fluid Hydrodynamics, and Glymphatic Drainage? Literature Overview and Illustrative Cases. World Neurosurg. 2019, 130, e941–e952. [Google Scholar] [CrossRef]
- Accogli, A.; Geraldo, A.F.; Piccolo, G.; Riva, A.; Scala, M.; Balagura, G.; Salpietro, V.; Madia, F.; Maghnie, M.; Zara, F.; et al. Diagnostic Approach to Macrocephaly in Children. Front. Pediatr. 2021, 9, 794069. [Google Scholar] [CrossRef] [PubMed]
- Tzerakis, N.; Orphanides, G.; Antoniou, E.; Sioutos, P.J.; Lafazanos, S.; Seretis, A. Subdural effusions with hydrocephalus after severe head injury: Successful treatment with ventriculoperitoneal shunt placement: Report of 3 adult cases. Case Rep. Med. 2010, 2010, 743784. [Google Scholar] [CrossRef] [Green Version]
- Scheffler, P.; Oertel, M.F.; Stieglitz, L.H. Comparison Between Flow-Regulated and Gravitational Shunt Valves in the Treatment of Normal Pressure Hydrocephalus: Flow-Grav Study. Neurosurgery 2021, 89, 413–419. [Google Scholar] [CrossRef]
- Paff, M.; Alexandru-Abrams, D.; Muhonen, M.; Loudon, W. Ventriculoperitoneal shunt complications: A review. Interdiscip. Neurosurg. 2018, 13, 66–70. [Google Scholar] [CrossRef]
- Njiokiktjien, C.J.; Valk, J.; Ponssen, H. Subdural hygroma: Results of treatment by ventriculo-abdominal shunt. Child’s Brain 1980, 7, 285–302. [Google Scholar] [CrossRef]
- Wiig, U.S.; Zahl, S.M.; Egge, A.; Helseth, E.; Wester, K. Epidemiology of Benign External Hydrocephalus in Norway-A Population-Based Study. Pediatr. Neurol. 2017, 73, 36–41. [Google Scholar] [CrossRef] [Green Version]
- Edlmann, E.; Whitfield, P.C.; Kolias, A.; Hutchinson, P.J. Pathogenesis of Chronic Subdural Hematoma: A Cohort Evidencing De Novo and Transformational Origins. J. Neurotrauma 2021, 38, 2580–2589. [Google Scholar] [CrossRef]
- Kostić, A.; Kehayov, I.; Stojanović, N.; Nikolov, V.; Kitov, B.; Milošević, P.; Kostić, E.; Zhelyazkov, H. Spontaneous chronic subdural hematoma in elderly people—Arterial hypertension and other risk factors. J. Chin. Med. Assoc. 2018, 81, 781–786. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.S. Chronic Subdural Hematoma in the Aged, Trauma or Degeneration? J. Korean Neurosurg. Soc. 2016, 59, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Dorrier, C.E.; Jones, H.E.; Pintarić, L.; Siegenthaler, J.A.; Daneman, R. Emerging roles for CNS fibroblasts in health, injury and disease. Nat. Rev. Neurosci. 2022, 23, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.N.; Noss, E.H.; Mizoguchi, F.; Huppertz, C.; Wei, K.S.; Watts, G.F.M.; Brenner, M.B. Autocrine Loop Involving IL-6 Family Member LIF, LIF Receptor, and STAT4 Drives Sustained Fibroblast Production of Inflammatory Mediators. Immunity 2017, 46, 220–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osuka, K.; Watanabe, Y.; Usuda, N.; Iwami, K.; Miyachi, S.; Takayasu, M. Expression of high mobility group B1 and toll-like receptor-nuclear factor κB signaling pathway in chronic subdural hematomas. PLoS ONE 2020, 15, e0233643. [Google Scholar] [CrossRef]
- Osuka, K.; Ohmichi, Y.; Ohmichi, M.; Nakura, T.; Iwami, K.; Watanabe, Y.; Miyachi, S. Sequential Expression of Chemokines in Chronic Subdural Hematoma Fluids after Trepanation Surgery. J. Neurotrauma 2021, 38, 1979–1987. [Google Scholar] [CrossRef]
- Weiskirchen, R.; Weiskirchen, S.; Tacke, F. Organ and tissue fibrosis: Molecular signals, cellular mechanisms and translational implications. Mol. Aspects Med. 2019, 65, 2–15. [Google Scholar] [CrossRef]
- Zhang, M.; Zhang, S. T Cells in Fibrosis and Fibrotic Diseases. Front. Immunol. 2020, 11, 1142. [Google Scholar] [CrossRef]
- Holl, D.C.; Volovici, V.; Dirven, C.M.F.; Peul, W.C.; van Kooten, F.; Jellema, K.; van der Gaag, N.A.; Miah, I.P.; Kho, K.H.; den Hertog, H.M.; et al. Pathophysiology and Nonsurgical Treatment of Chronic Subdural Hematoma: From Past to Present to Future. World Neurosurg. 2018, 116, 402–411.e2. [Google Scholar] [CrossRef]
- Heula, A.L.; Sajanti, J.; Majamaa, K. Glycosaminoglycans in subdural fluid and CSF after meningeal injury. Acta Neurochir. 2015, 157, 2105–2110; discussion 2110. [Google Scholar] [CrossRef]
- Barchitta, M.; Maugeri, A.; Favara, G.; Magnano San Lio, R.; Evola, G.; Agodi, A.; Basile, G. Nutrition and Wound Healing: An Overview Focusing on the Beneficial Effects of Curcumin. Int. J. Mol. Sci. 2019, 20, 1119. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Zhang, Z.; Xu, T.; Lou, Y.; Wang, Q.; Jin, H.; Zhang, L.; Feng, Y.; Xu, H.; Mao, C. Upregulating mTOR/ERK signaling with leonurine for promoting angiogenesis and tissue regeneration in a full-thickness cutaneous wound model. Food Funct. 2018, 9, 2374–2385. [Google Scholar] [CrossRef]
- Edlmann, E.; Giorgi-Coll, S.; Whitfield, P.C.; Carpenter, K.L.H.; Hutchinson, P.J. Pathophysiology of chronic subdural haematoma: Inflammation, angiogenesis and implications for pharmacotherapy. J. Neuroinflamm. 2017, 14, 108. [Google Scholar] [CrossRef] [Green Version]
- Han, J.M.; Gou, M.; Xiao, R. Neutrophils regulate the process of angiogenesis. Sheng Li Xue Bao 2017, 69, 843–851. [Google Scholar]
- Michaeli, S.; Dakwar, V.; Weidenfeld, K.; Granski, O.; Gilon, O.; Schif-Zuck, S.; Mamchur, A.; Shams, I.; Barkan, D. Soluble Mediators Produced by Pro-Resolving Macrophages Inhibit Angiogenesis. Front. Immunol. 2018, 9, 768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, G.J.; Gao, J.; Wu, C.W.; Zou, J.F.; Zhang, D.; Zhu, D.L.; Liu, J.; Zhang, J.H.; Huang, X.J. Serum Levels of MMP-8 and MMP-9 as Markers in Chronic Subdural Hematoma. J. Clin. Med. 2022, 11, 902. [Google Scholar] [CrossRef]
- Saito, H.; Tanaka, M.; Hadeishi, H. Angiogenesis in the Septum and Inner Membrane of Refractory Chronic Subdural Hematomas: Consideration of Findings after Middle Meningeal Artery Embolization with Low-concentration n-butyl-2-cyanoacrylate. NMC Case Rep. J. 2019, 6, 105–110. [Google Scholar] [CrossRef] [Green Version]
- Dian, J.; Linton, J.; Shankar, J.J. Risk of recurrence of subdural hematoma after EMMA vs surgical drainage—Systematic review and meta-analysis. Interv. Neuroradiol. 2021, 27, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Bayer, I.S. Advances in Fibrin-Based Materials in Wound Repair: A Review. Molecules 2022, 27, 4504. [Google Scholar] [CrossRef]
- Davidson, B.; Narvacan, K.; Munoz, D.G.; Rotondo, F.; Kovacs, K.; Zhang, S.; Cusimano, M.D. The Crucial Role of Eosinophils in the Life Cycle, Radiographical Architecture, and Risk of Recurrence of Chronic Subdural Hematomas. Neurotrauma Rep. 2021, 2, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Kung, W.M.; Lin, M.S. CT-Based Quantitative Analysis for Pathological Features Associated with Postoperative Recurrence and Potential Application Upon Artificial Intelligence: A Narrative Review with a Focus on Chronic Subdural Hematomas. Mol. Imaging 2020, 19, 1536012120914773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.S. History of Chronic Subdural Hematoma. Korean J. Neurotrauma 2015, 11, 27–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, T.-Y.; Chang, S.-T.; Lin, M.-S. Statistical relevance of mean hematoma density and its internal architecture: Potential clinical application in chronic subdural hematomas. Formos. J. Surg. 2018, 51, 228–233. [Google Scholar] [CrossRef]
- Ko, B.S.; Lee, J.K.; Seo, B.R.; Moon, S.J.; Kim, J.H.; Kim, S.H. Clinical analysis of risk factors related to recurrent chronic subdural hematoma. J. Korean Neurosurg. Soc. 2008, 43, 11–15. [Google Scholar] [CrossRef]
- Kung, W.M.; Hung, K.S.; Chiu, W.T.; Tsai, S.H.; Lin, J.W.; Wang, Y.C.; Lin, M.S. Quantitative assessment of impaired postevacuation brain re-expansion in bilateral chronic subdural haematoma: Possible mechanism of the higher recurrence rate. Injury 2012, 43, 598–602. [Google Scholar] [CrossRef]
- Mishra, R.; Deora, H.; Florez-Perdomo, W.A.; Moscote-Salazar, L.R.; Garcia-Ballestas, E.; Rahman, M.M.; Shrivastava, A.; Raj, S.; Chavda, V.; Montemurro, N.; et al. Clinical and Radiological Characteristics for Recurrence of Chronic Subdural Hematoma: A Systematic Review and Meta-Analysis. Neurol. Int. 2022, 14, 683–695. [Google Scholar] [CrossRef] [PubMed]
- Torihashi, K.; Sadamasa, N.; Yoshida, K.; Narumi, O.; Chin, M.; Yamagata, S. Independent predictors for recurrence of chronic subdural hematoma: A review of 343 consecutive surgical cases. Neurosurgery 2008, 63, 1125–1129; discussion 1129. [Google Scholar] [CrossRef]
- Shimizu, Y.; Park, C.; Tokuda, K. Gradation density hematoma is a predictor of chronic subdural hematoma recurrence associated with inflammation of the outer membrane. Clin. Neurol. Neurosurg. 2020, 194, 105839. [Google Scholar] [CrossRef]
- Lin, C.C.; Lu, Y.M.; Chen, T.H.; Wang, S.P.; Hsiao, S.H.; Lin, M.S. Quantitative assessment of post-operative recurrence of chronic subdural haematoma using mean haematoma density. Brain Inj. 2014, 28, 1082–1086. [Google Scholar] [CrossRef] [PubMed]
- Fang, H.; Zhang, Z.; Liu, Y.; Wang, L.; Yang, Y.; Li, S.; Jing, X.; Bai, G.; Sheng, H. Rigid Neuroendoscopy Assisted Hematoma Resection Reduces the Recurrence Rate of Chronic Subdural Hematoma with Mixed Density: A Retrospective Analytic Cohort Study. Front. Surg. 2022, 9, 789118. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, M.-S. Subdural Lesions Linking Additional Intracranial Spaces and Chronic Subdural Hematomas: A Narrative Review with Mutual Correlation and Possible Mechanisms behind High Recurrence. Diagnostics 2023, 13, 235. https://doi.org/10.3390/diagnostics13020235
Lin M-S. Subdural Lesions Linking Additional Intracranial Spaces and Chronic Subdural Hematomas: A Narrative Review with Mutual Correlation and Possible Mechanisms behind High Recurrence. Diagnostics. 2023; 13(2):235. https://doi.org/10.3390/diagnostics13020235
Chicago/Turabian StyleLin, Muh-Shi. 2023. "Subdural Lesions Linking Additional Intracranial Spaces and Chronic Subdural Hematomas: A Narrative Review with Mutual Correlation and Possible Mechanisms behind High Recurrence" Diagnostics 13, no. 2: 235. https://doi.org/10.3390/diagnostics13020235