

Characteristics of Mandibular Arch Forms in Patients with Skeletal Mandibular Prognathism
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
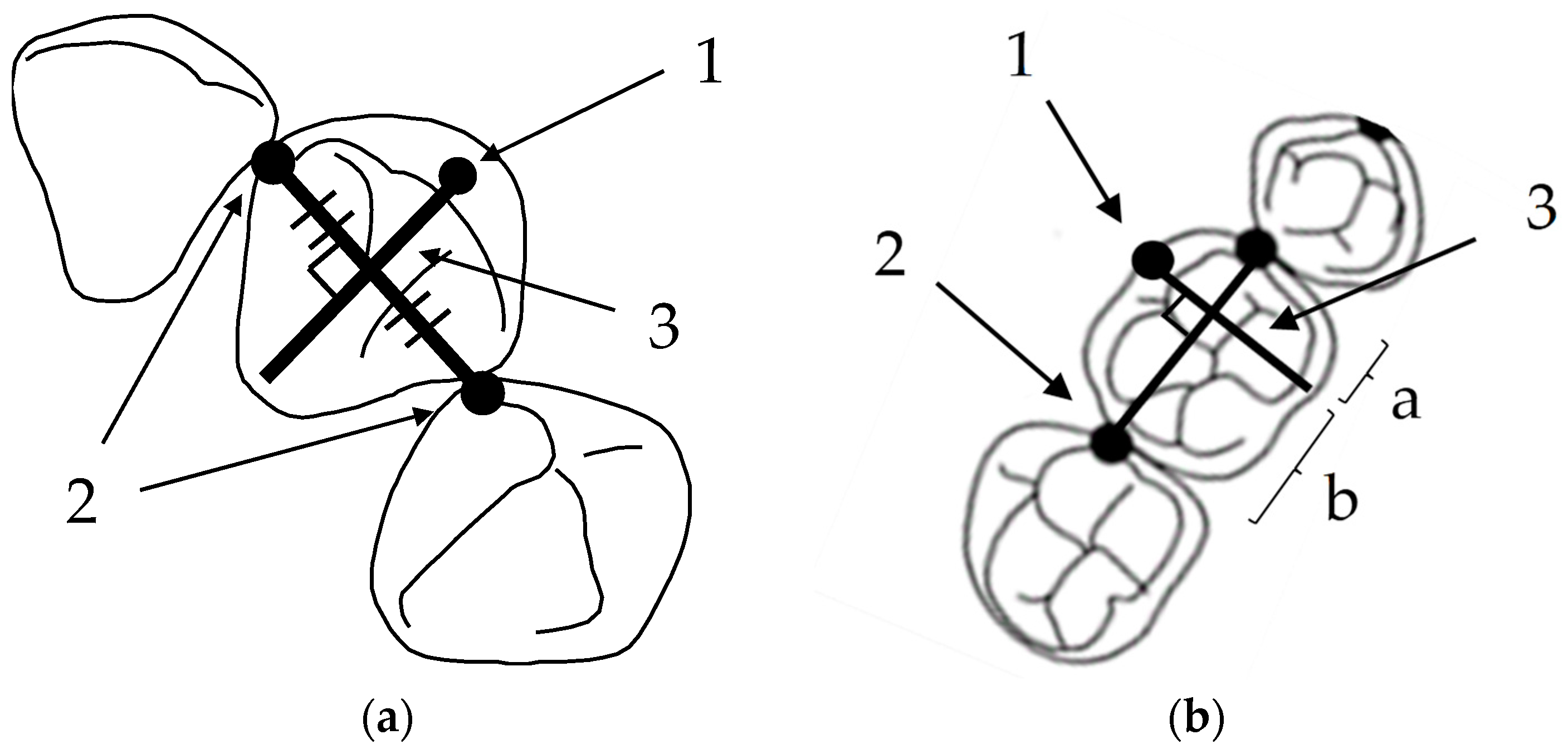
2.2. Measurement Method
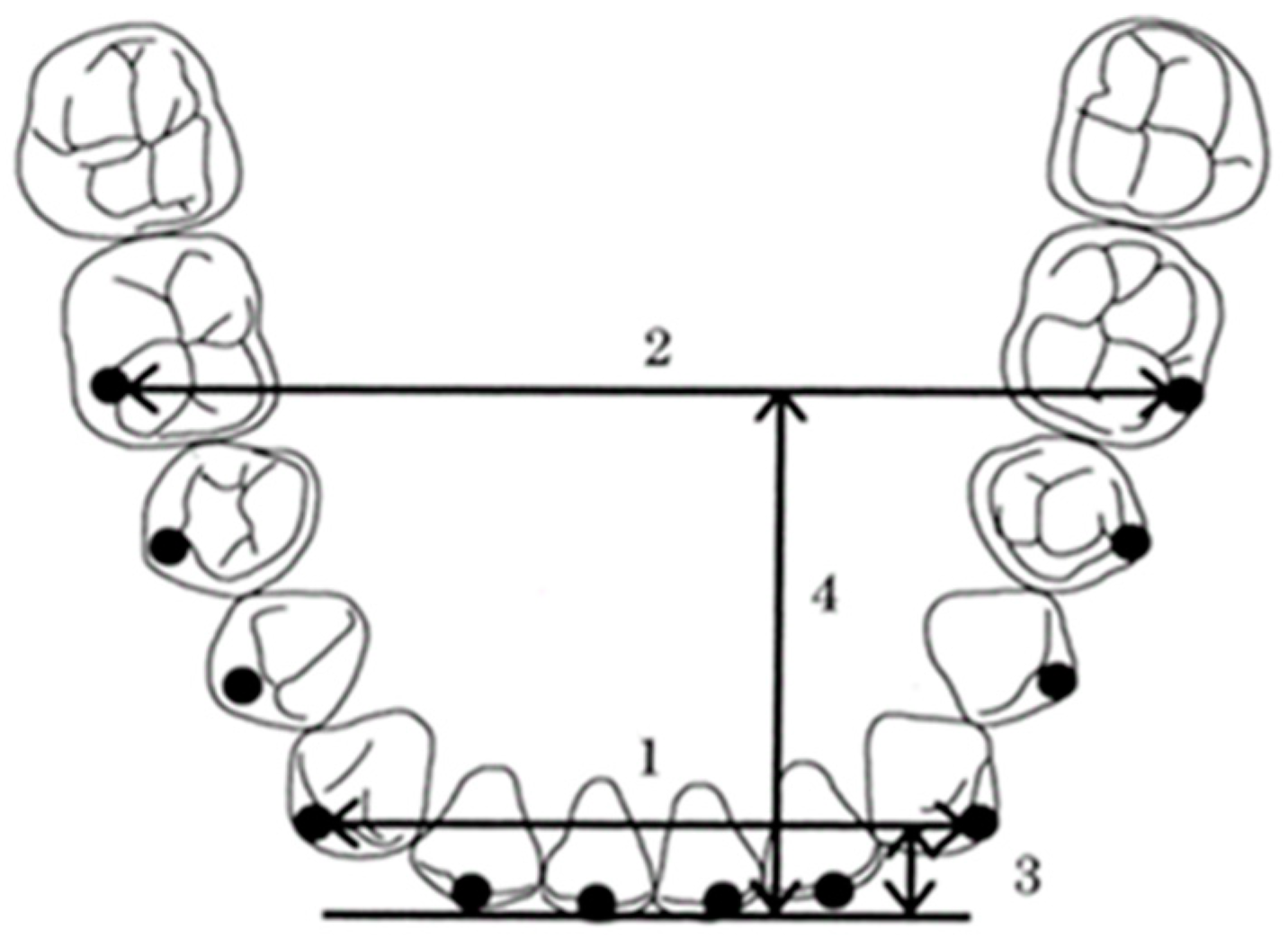
2.3. Measurement Items (Figure 3)
- Intercanine width, the distance between the canine clinical bracket points;
- Intermolar width, the distance between the first molar clinical bracket points;
- Canine depth, the shortest distance from a line connecting the canine clinical bracket points to the origin between the central incisors;
- Molar depth, the shortest distance from a line connecting the first molar clinical bracket points to the origin between the central incisors;
- Canine W/D ratio, the ratio of the intercanine width to the canine depth;
- Molar W/D ratio, the ratio of the intermolar width to the molar depth.

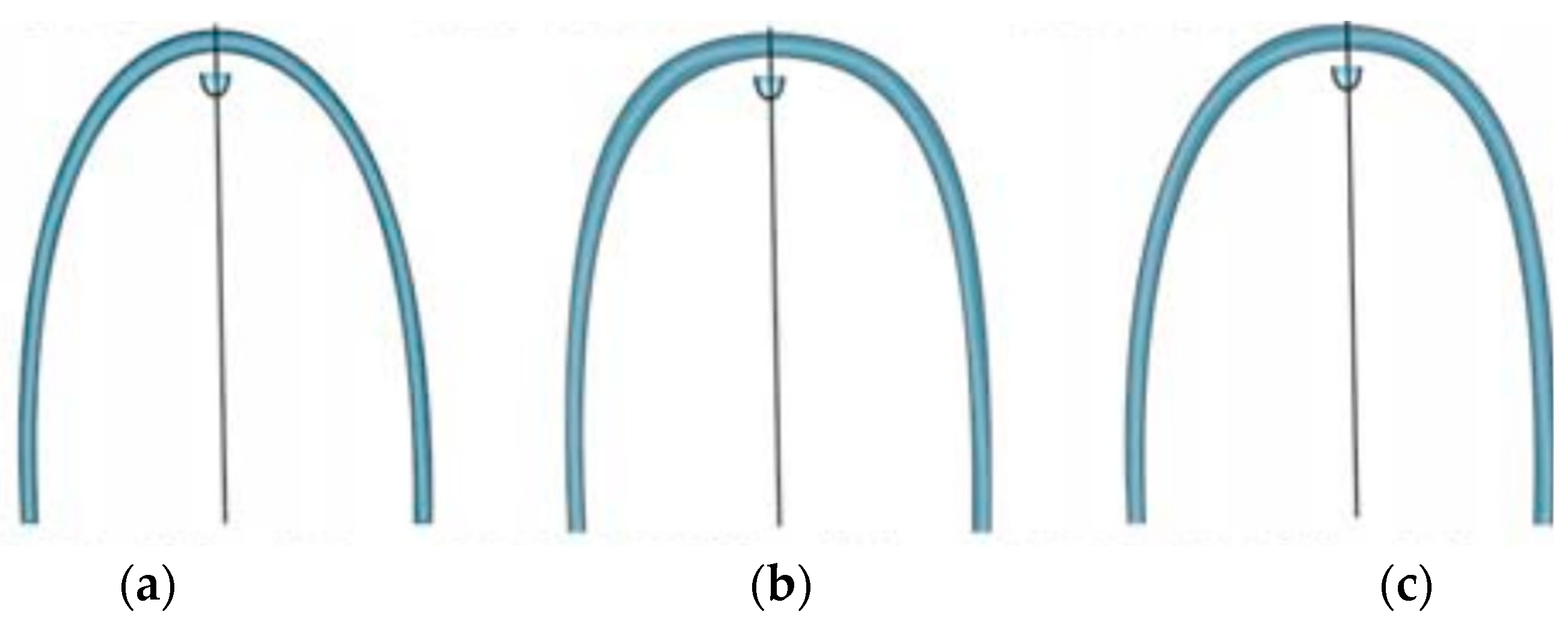
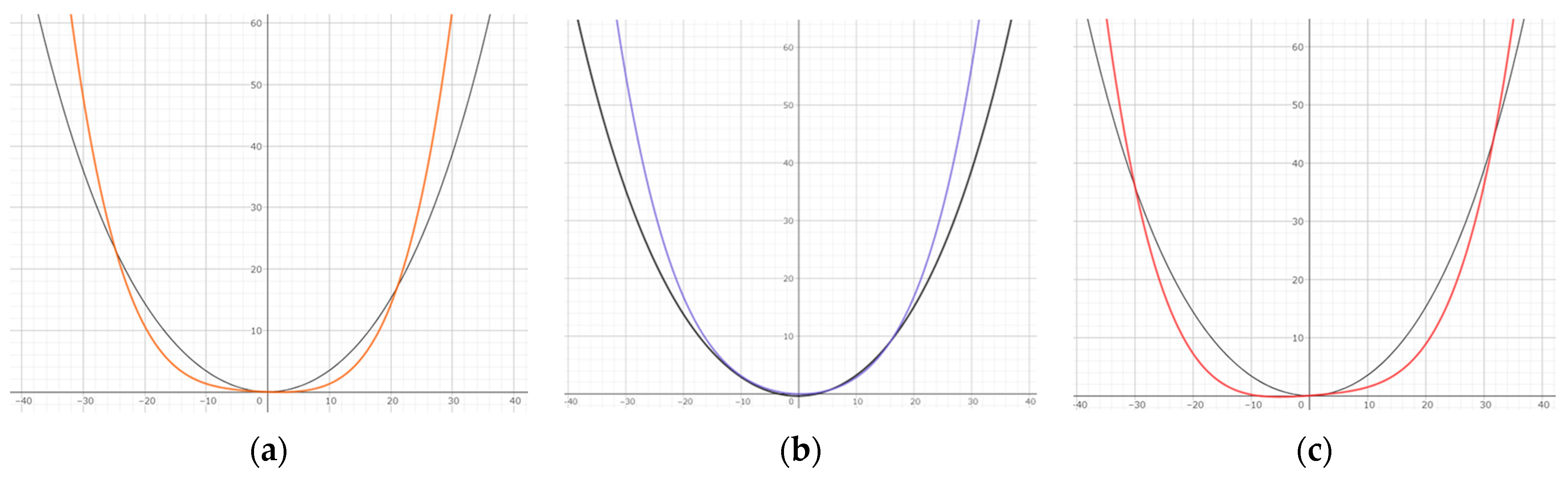
2.4. Arch form Comparison
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Naran, S.; Steinbacher, D.M.; Taylor, J.A. Current Concepts in Orthognathic Surgery. Plast. Reconstr. Surg. 2018, 141, 925e–936e. [Google Scholar] [CrossRef]
- De la Cruz, A.; Sampson, P.; Little, R.M.; Artun, J.; Shapiro, P.A. Long-term change in arch form after orthodontic treatment and retention. Am. J. Orthod. Dentofac. Orthop. 1995, 107, 518–530. [Google Scholar]
- Nojima, K.; Mclaughlin, R.P.; Isshiki, Y.; Sinclair, P.M. A comparative study of Caucasian and Japanese mandibular clinical arch forms. Angle Orthod. 2001, 71, 195–200. [Google Scholar]
- Gafni, Y.; Tzur-Gadassi, L.; Nojima, K.; Mclaughlin, R.P.; Abed, Y.; Redlich, M. Comparison of arch forms between Israeli and North American white populations. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 339–344. [Google Scholar] [CrossRef]
- Omar, H.; Alhajrasi, M.; Felemban, N.; Hassan, A. Dental arch dimensions, form and tooth size ratio among a Saudi sample. Saudi Med. J. 2018, 39, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Trang, V.T.; Park, J.H.; Bayome, M.; Shastry, S.; Mellion, A.; Kook, Y.A. Evaluation of arch form between Vietnamese and North American Caucasians using 3-dimensional virtual models. Anthropol. Anz. 2015, 72, 223–224. [Google Scholar] [CrossRef]
- Aoki, H.; Tsuta, A.; Ukiya, M. A morphological study and comparison of the dental arch form of Japanese and American adults: Detailed measurements of the transverse width. Bull. Tokyo Dent. Coll. 1971, 12, 9–14. [Google Scholar]
- Kayukawa, H. Studies on morphology of Mandibular overjet-Introduction and Part 1. Model Analysis. J. Jpn. Orthod. Soc. 1956, 15, 6–26. [Google Scholar]
- Imaizumi, Y. A Morphological Study on the Socalled Reversed Occlusion by Means of Modelanalysis; The Department of Orthodontics, Kyushu Dental College: Fukuoka, Japan, 1960; Volume 14, pp. 525–541. [Google Scholar]
- Nie, Q.; Lin, J. A comparison of dental arch forms between Class II Division 1 and normal occlusion assessed by euclidean distance matrix analysis. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Hu, W.; Zhou, Y. The compensation of dental arch and teeth in patients with skeletal protrusion and deviation of mandible. Zhonghua Kou Qiang Yi Xue Za Zhi 2002, 37, 180–182. [Google Scholar] [PubMed]
- Andrews, L.F. Straight Wire Appliance; LA Wells, Co.: San Diego, CA, USA, 1989; pp. 223–242. [Google Scholar]
- McLaughlin, R.P.; Bennett, J.C.; Trevisi, H.J. Systemized Orthodontic Treatment Mechanics; Mosby Ltd.: St. Louis, MI, USA, 1979; pp. 71–91. [Google Scholar]
- Little, R.M. Stability and relapse of dental arch alignment. Br. J. Orthod. 1990, 17, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Gardner, S.D.; Chaconas, S.J. Posttreatment and postretention changes following orthodontic therapy. Angle Orthod. 1976, 46, 151–161. [Google Scholar]
- Artun, J.; Garol, J.D.; Little, R.M. Long-term stability of mandibular incisors following successful treatment of Class II division 1, malocclusions. Angle Orthod. 1996, 66, 229–238. [Google Scholar] [PubMed]
- Sebata, E. An orthodontic study of teeth and dental arch form on the Japanese normal occlusions. Shikwa Gakuho 1980, 80, 945–969. [Google Scholar]
- Kosaka, H.; Kobayashi, T. A study of dental-arch forms and orthodontic arch-wire forms in Japanese subjects with normal occlusion. Shikwa Gakuho 1997, 97, 1029–1036. [Google Scholar]
- Saito, I.; Nihara, J.; Takahashi, K.; Takeyama, M. The Spread of Surgical Orthodontic Treatment with Quality Assurance-30 Years since Application of Public Health Insurance. Jpn. J. Jaw Deform. 2021, 31, 187–189. [Google Scholar] [CrossRef]
- Braun, S.; Hnat, W.P.; Fender, D.E.; Legan, H.L. The form of the human dental arch. Angle Orthod. 1998, 68, 29–36. [Google Scholar]
- Jacobson, A. Update on the Wits Appraisal. Angle Orthod. 1988, 58, 205–219. [Google Scholar]
- Engel, G.A. Preformed arch: Reliability of fit. Am. J. Orthod. 1979, 76, 497–504. [Google Scholar] [CrossRef]
- Raberin, M.; Laumon, B.; Martin, J.L.; Brunner, F. Dimensions and form of dental arches in subjects with normal occlusions. Am. J. Orthod. Dentofac. Orthop. 1993, 104, 67–72. [Google Scholar] [CrossRef]
- Asai, Y.; Tome, W.; Okumura, S.; Murabayashi, M.; Kitai, N. Three-dimensional morphology of dentition and the alveolar part in patients with lateral mandibular deviation. J. Gifu Dent. Soc. 2020, 47, 1–12. [Google Scholar]
- Leonardi, R.; Lo Giudice, A.; Rugeri, M.; Muraglie, S.; Cordasco, G.; Barbato, E. Three-dimensional evaluation on digital casts of maxillary palatal size and morphology in patients with functional posterior crossbite. Eur. J. Orthod. 2018, 40, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Perrotti, G.; Reda, R.; Rossi, O.; D’apolito, I.; Testori, T.; Testarelli, L. A radiation free alternative to CBCT volumetric rendering for soft tissue evaluation. Braz. Dent. Sci. 2023, 26, 3726. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | Male: 18 | ||
| Female: 29 | |||
| Age (year) | 24.3 ± 9.7 | ||
| ANB (°) | −2.5 ± 2.2 | Max.: 0 | Min.: −5.5 |
| Wits appraisal (mm) | −12.6 ± 4.5 | Max.: −6 | Min.: −25 |
| Facial pattern | Brachy: 24 | Mesio: 13 | Dolicho: 10 |
| Groups | Class IIIS Group | Control Group | |||
|---|---|---|---|---|---|
| Measurement Items | Average | SD | Average | SD | p-Value |
| Intercanine width (mm) | 29.17 | 1.87 | 29.89 | 1.52 | NS |
| Intermolar width (mm) | 48.69 | 3.11 | 50.70 | 2.81 | 0.001 |
| Canine depth (mm) | 4.64 | 1.14 | 5.66 | 1.01 | 0.000 |
| Molar depth (mm) | 24.91 | 2.15 | 26.28 | 1.94 | 0.000 |
| Canine W/D ratio | 6.73 | 1.94 | 5.43 | 0.87 | 0.000 |
| Molar W/D ratio | 1.97 | 0.21 | 1.94 | 0.15 | NS |
| Groups | Wits ≤ −10 | Wits > −10 | Brachy | Dolicho | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Measurement Items | Average | SD | Average | SD | p-Value | Average | SD | Average | SD | p-Value |
| Canine W/D ratio | 7.71 | 3.77 | 6.47 | 2.22 | NS | 6.08 | 1.10 | 8.28 | 3.03 | 0.004 |
| Molar W/D ratio | 1.97 | 0.18 | 1.99 | 0.25 | NS | 1.91 | 0.16 | 2.07 | 0.22 | 0.020 |
| Groups | Square | Ovoid | Tapered | p-Value |
|---|---|---|---|---|
| Class IIIS group | 20 (42.5%) | 15 (31.9%) | 12 (25.6%) | 0.016 |
| Control group | 32 (53.3%) | 23 (38.3%) | 5 (8.3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ichikawa, E.; Tachiki, C.; Nojima, K.; Matsunaga, S.; Sugahara, K.; Watanabe, A.; Kasahara, N.; Nishii, Y. Characteristics of Mandibular Arch Forms in Patients with Skeletal Mandibular Prognathism. Diagnostics 2023, 13, 3237. https://doi.org/10.3390/diagnostics13203237
Ichikawa E, Tachiki C, Nojima K, Matsunaga S, Sugahara K, Watanabe A, Kasahara N, Nishii Y. Characteristics of Mandibular Arch Forms in Patients with Skeletal Mandibular Prognathism. Diagnostics. 2023; 13(20):3237. https://doi.org/10.3390/diagnostics13203237
Chicago/Turabian StyleIchikawa, Erika, Chie Tachiki, Kunihiko Nojima, Satoru Matsunaga, Keisuke Sugahara, Akira Watanabe, Norio Kasahara, and Yasushi Nishii. 2023. "Characteristics of Mandibular Arch Forms in Patients with Skeletal Mandibular Prognathism" Diagnostics 13, no. 20: 3237. https://doi.org/10.3390/diagnostics13203237