
Comparisons of Dental Anomalies in Orthodontic Patients with Impacted Maxillary and Mandibular Canines

Abstract
:1. Introduction
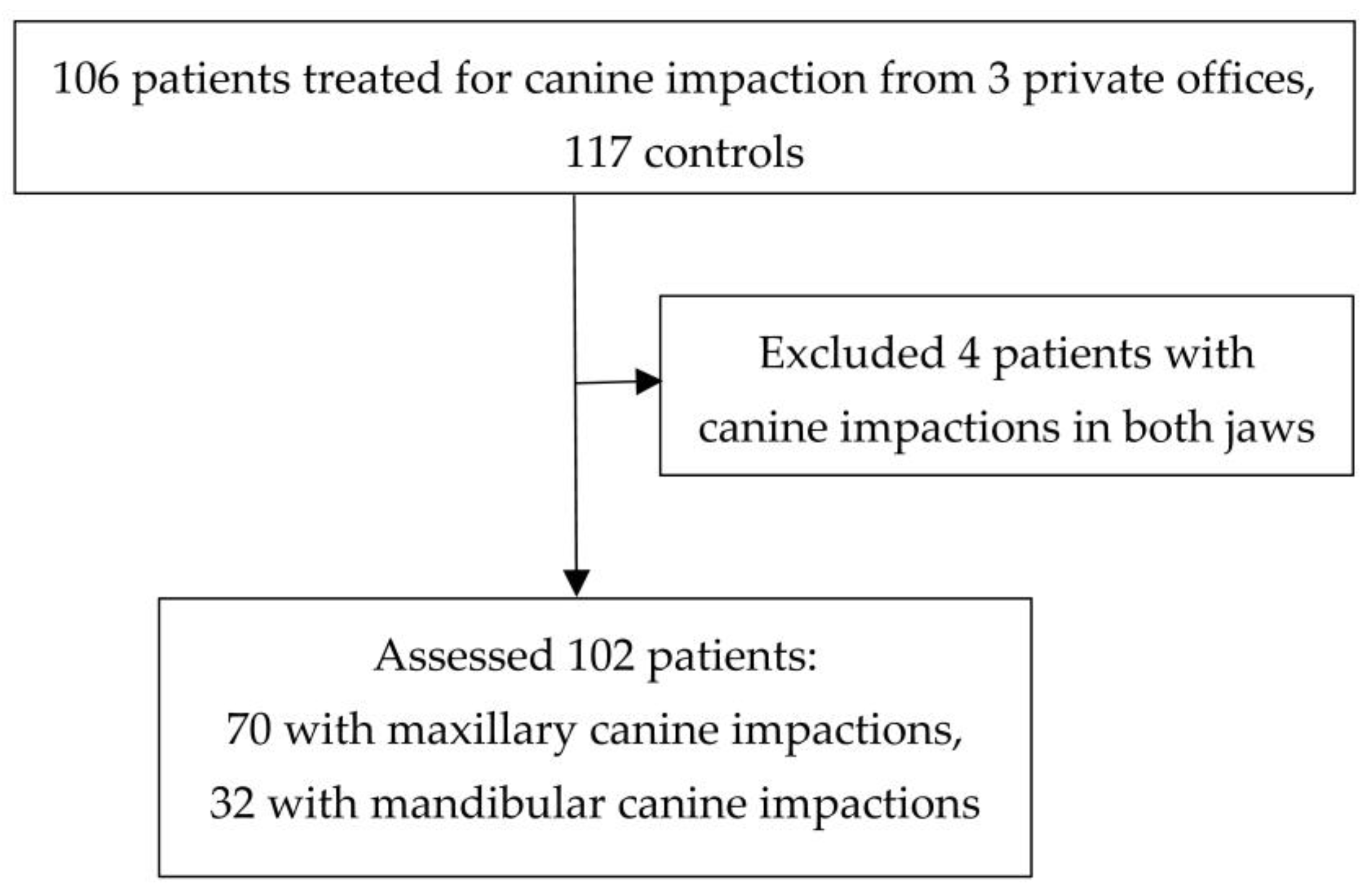
2. Materials and Methods
Statistical Analysis
3. Results
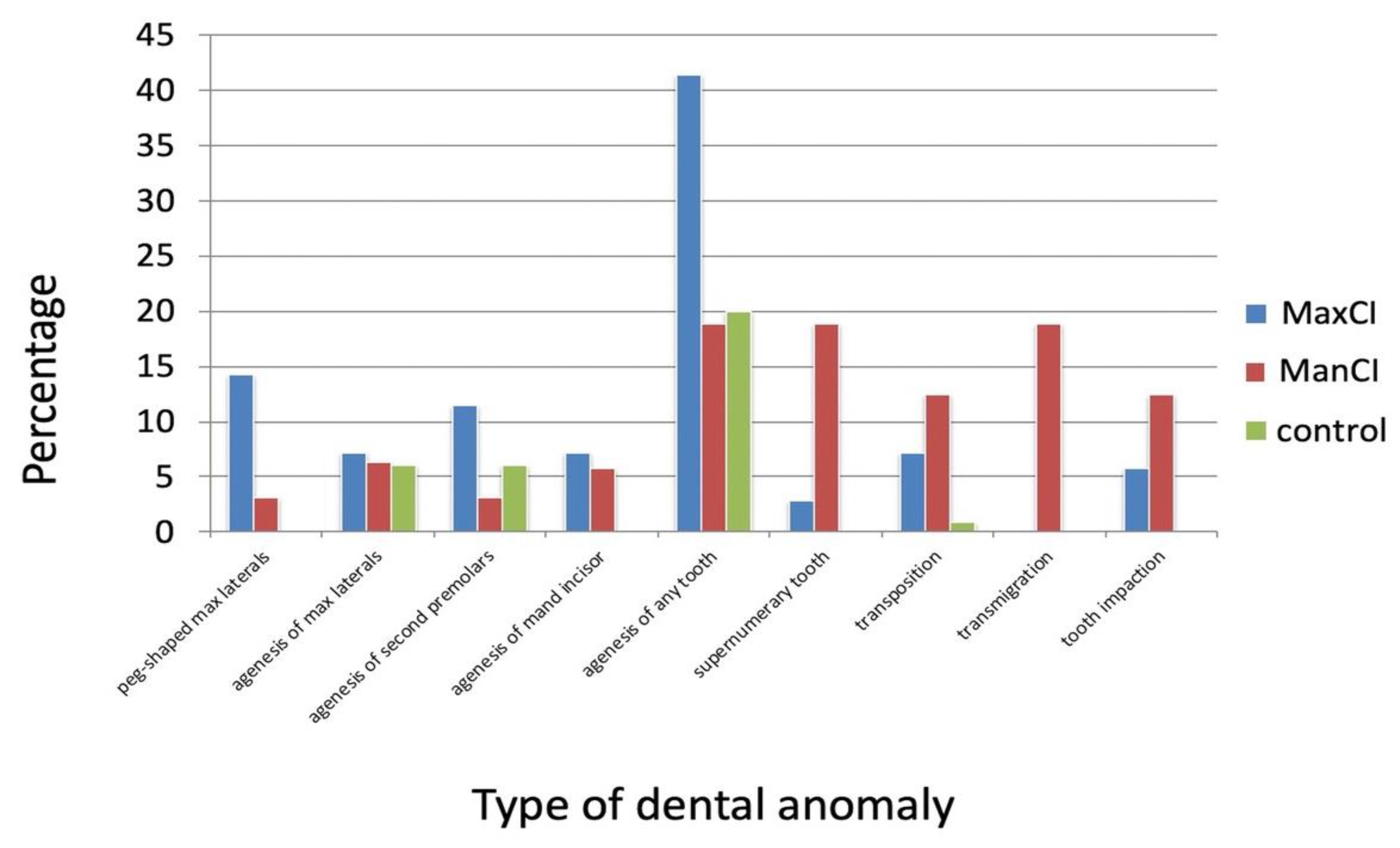
3.1. Prevalence of Dental Anomalies in Impaction and Control Groups
3.2. Comparisons of Dental Anomalies between Maxillary and Mandibular Canine Impaction Groups
3.3. Comparisons of Dental Anomalies between the Canine Impaction and the Control Groups
4. Discussion
4.1. Comparisons of the Presence of Different Dental Anomalies between Groups
4.2. Peg-Shaped Maxillary Incisors and Agenesis of Lateral Incisors
4.3. Tooth Agenesis
4.4. Supernumerary Teeth and Tooth Transposition
4.5. Transmigration
4.6. Tooth Impaction
4.7. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shah, R.M.; Boyd, M.A.; Vakil, T.F. Studies of permanent tooth anomalies in 7886 Canadian individuals. I: Impacted teeth. Dent. J. 1978, 44, 262–264. [Google Scholar]
- Grover, P.S.; Lorton, L. The incidence of unerupted permanent teeth and related clinical cases. Oral Surg. Oral Med. Oral Pathol. 1985, 59, 420–425. [Google Scholar] [CrossRef]
- Sağlam, A.A.; Tüzüm, M.S. Clinical and radiologic investigation of the incidence, complications, and suitable removal times for fully impacted teeth in the Turkish population. Quintessence Int. 2003, 34, 53–59. [Google Scholar]
- Becker, A. Orthodontic Treatment of Impacted Teeth, 3rd ed.; Wiley: New York, NY, USA, 2012; Volume 1–9, pp. 111–172. [Google Scholar]
- Ericson, S.; Kurol, P.J. Resorption of incisors after ectopic eruption of maxillary canines: A CT study. Angle Orthod. 2000, 70, 415–423. [Google Scholar]
- Baccetti, T.; Sigler, L.M.; McNamara, J.A. An RCT on treatment of palatally displaced canines with RME and/or a transpalatal arch. Eur. J. Orthod. 2011, 33, 601–607. [Google Scholar] [CrossRef]
- Bonetti, G.A.; Zanarini, M.; Parenti, S.I.; Marini, I.; Gatto, M.R. Preventive treatment of ectopically erupting maxillary permanent canines by extraction of deciduous canines and first molars: A randomized clinical trial. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 316–323. [Google Scholar] [CrossRef]
- Naoumova, J.; Kurol, J.; Kjellberg, H. Extraction of the deciduous canine as an interceptive treatment in children with palatal displaced canines–part I: Shall we extract the deciduous canine or not? Eur. J. Orthod. 2015, 37, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Parkin, N.; Furness, S.; Shah, A.; Thind, B.; Marshman, Z.; Glenroy, G.; Dyer, F.; E Benson, P. Extraction of primary (baby) teeth for unerupted palatally displaced permanent canine teeth in children. Cochrance Database Syst. Rev. 2012, 12, CD00462. [Google Scholar] [CrossRef] [PubMed]
- Bass, T.B. Observations on the misplaced upper canine tooth. Dent. Pract. Dent. Rec. 1967, 18, 25–33. [Google Scholar] [PubMed]
- Oliver, R.G.; Mannion, J.E.; Robinson, J.M. Morphology of the maxillary lateral incisor in cases of unilateral impaction of the maxillary canine. Br. J. Orthod. 1989, 16, 9–16. [Google Scholar] [CrossRef]
- Bjerklin, K.; Kurol, J.; Valentin, J. Ectopic eruption of maxillary first permanent molars and association with other tooth and developmental disturbances. Eur. J. Orthod. 1992, 14, 369–375. [Google Scholar] [CrossRef]
- Mossey, P.A.; Campbell, H.M.; Luffingham, J.K. The palatal canine and the adjacent lateral incisor: A study of a west of Scotland population. Br. J. Orthod. 1994, 21, 169–674. [Google Scholar] [CrossRef]
- Peck, S.; Peck, L.; Kataja, M. Prevalence of tooth agenesis and peg-shaped maxillary lateral incisor associated with palatally displaced canine (PDC) anomaly. Am. J. Orthod. Dentofac. Orthop. 1996, 110, 441–443. [Google Scholar] [CrossRef]
- Pirinen, S.; Arte, S.; Apajalahti, S. Palatal displacement of canine is genetic and related to congenital absence of teeth. J. Dent. Res. 1996, 75, 1742–1746. [Google Scholar] [CrossRef]
- Chaushu, S.; Sharabi, S.; Becker, A. Dental morphologic characteristics of normal versus delayed developing dentitions with palatally displaced canines. Am. J. Orthod. Dentofac. Orthop. 2002, 121, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Leifert, S.; Jonas, I. Dental anomalies as a micro symptom of palatal canine displacement. J. Orofac. Orthop. 2003, 64, 108–120. [Google Scholar] [CrossRef]
- Peck, S.; Peck, L.; Kataja, M. Concomitant occurrence of canine malposition and tooth agenesis: Evidence of orofacial genetic fields. Am. J. Orthod. Dentofac. Orthop. 2002, 122, 657–660. [Google Scholar] [CrossRef] [PubMed]
- Jena, A.K.; Duggal, R. The pattern of maxillary canine impaction in relation to anomalous lateral incisors. J. Clin. Pediatr. Dent. 2010, 35, 37–40. [Google Scholar] [CrossRef] [PubMed]
- Mercuri, E.; Cassetta, M.; Cavallini, C.; Vicari, D.; Leonardi, R.; Barbato, E. Dental anomalies and clinical features in patients with maxillary canine impaction. A retrospective study. Angle Orthod. 2013, 83, 22–28. [Google Scholar] [CrossRef]
- Yan, B.; Sun, Z.; Fields, H.; Wang, L.; Luo, L. Etiologic factors for buccal and palatal maxillary canine impaction: A perspective based on cone-beam computed tomography analyses. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 527–534. [Google Scholar] [CrossRef]
- Sajnani, A.K.; King, N.M. Dental anomalies associated with buccally and palatally impacted maxillary canines. J. Investig. Clin. Dent. 2014, 5, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Scerii, E.S.; McDonald, F.; Camileri, S. Comparison of the dental anomalies found in maxillary canine-first premolar transposition cases with those in palatally displaced canine cases. Eur. J. Orthod. 2016, 38, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Herrera-Atoche, J.R.; Agüayo-de-Pau MD, R.; Escoffié-Ramírez, M.; Aguilar-Ayala, F.J.; Carrillo-Ávila, B.A.; Rejón-Peraza, M.E. Impacted Maxillary Canine Prevalence and Its Association with Other Dental Anomalies in a Mexican Population. Int. J. Dent. 2017, 2017, 7326061. [Google Scholar] [CrossRef]
- Fardi, A.; Kondylidou-Sidira, A.; Bachour, Z.; Parisis, N.; Tsirlis, A. Incidence of impacted and supernumerary teeth—A radiographic study in a North Greek population. Med. Oral Patol. Oral Cir. Bucal. 2011, 16, 56–61. [Google Scholar] [CrossRef]
- Aydin, U.; Yilmaz, H.H.; Yildirim, D. Incidence of canine impaction and transmigration in a patient population. Dentomaxillofac. Radiol. 2004, 33, 164–169. [Google Scholar] [CrossRef] [PubMed]
- BBuyukkurt, M.C.; Aras, M.H.; Caglaroglu, M.; Gungormus, M. Transmigrant mandibular canine. J. Oral Maxillofac. Surg. 2007, 65, 2025–2029. [Google Scholar] [CrossRef] [PubMed]
- Tozoglu, S.; Yavuz, M.S.; Aras, M.H.; Büyükkurt, M.C. Impacted mandibular canines. J. Contemp. Dent. Pract. 2007, 8, 78–85. [Google Scholar] [CrossRef]
- González-Sánchez, M.A.; Berini-Aytés, L.; Gay-Escoda, C. Transmigrant impacted mandibular canines. A retrospective study of 15 cases. J. Am. Dent. Assoc. 2007, 138, 1450–1455. [Google Scholar] [CrossRef]
- Aktan, A.M.; Kara, S.; Akgünlü, F.; Malkoç, S. The incidence of canine transmigration and tooth impaction in a Turkish subpopulation. Eur. J. Orthod. 2010, 32, 575–581. [Google Scholar] [CrossRef]
- Celikoglu, M.; Kamak, H.; Oktay, H. Investigation of transmigrated and impacted maxillary and mandibular canine teeth in an orthodontic patient population. J. Oral Maxillofac. Surg. 2010, 68, 1001–1006. [Google Scholar] [CrossRef]
- Gündüz, K.; Açikgöz, A.; Eğrioğlu, E. Radiologic investigation of prevalence, associated pathologies and dental anomalies of non-third molar impacted teeth in Turkish oral patients. Chin. J. Dent. Res. 2011, 14, 141–146. [Google Scholar] [PubMed]
- Isa-Kara, M.; Ay, S.; Murat-Aktan, A.; Sener, I.; Bereket, C.; Ezirganli, S.; Demirkol, M. Analysis of different type of transmigrant mandibular teeth. Med. Oral Patol. Oral Cir. Bucal. 2011, 16, 335–340. [Google Scholar] [CrossRef]
- Aras, M.H.; Halicioğlu, K.; Yavuz, M.S.; Çağlaroğlu, M. Evaluation of surgical-orthodontic treatments on impacted mandibular canines. Med. Oral Patol. Oral Cir. Bucal. 2011, 16, 925–928. [Google Scholar] [CrossRef]
- Topkara, A.; Sari, Z. Impacted teeth in a Turkish orthodontic patient population: Prevalence, distribution and relationship with dental arch characteristics. Eur. J. Paediatr. Dent. 2012, 13, 311–316. [Google Scholar] [PubMed]
- Jain, S.; Shetty, K.S.; Prakash, A.T.; Agrawal, M.; Jain, S. Permanent mandibular canine(s) impaction: Expansion of our understanding. Aust. Orthod. J. 2014, 30, 39–44. [Google Scholar] [CrossRef]
- Kamiloglu, B.; Kelahmet, U. Prevalence of impacted and transmigrated canine teeth in a Cypriote orthodontic population in the Northern Cyprus area. BMC Res. Notes 2014, 7, 346. [Google Scholar] [CrossRef]
- Sajnani, A.K.; King, N.M. Success rates of different management techniques for impacted mandibular canines and associated complications in children and adolescents. J. Investig. Clin. Dent. 2015, 6, 228–233. [Google Scholar] [CrossRef]
- Bishara, S.E. Impacted maxillary canines: A review. Am. J. Orthod. Dentofac. Orthop. 1992, 101, 159–171. [Google Scholar] [CrossRef]
- Stabryła, J.; Plakwicz, P.; Kukuła, K.; Zadurska, M.; Czochrowska, E.M. Comparisons of different treatment methods and their outcomes for impacted maxillary and mandibular canines: A retrospective study. J. Am. Dent. Assoc. 2021, 152, 919–926. [Google Scholar] [CrossRef]
- Becker, A.; Smith, P.; Behar, R. The incidence of anomalous lateral incisors in relation to palatally displaced cuspids. Angle Orthod. 1981, 51, 24–29. [Google Scholar]
- Becktor, K.B.; Steinche, K.; Kjaer, I. Association between ectopic eruption of maxillary canines and first molars. Eur. J. Orthod. 2005, 27, 186–189. [Google Scholar] [CrossRef] [PubMed]
- Becker, A.; Peck, S.; Peck, L.; Kataja, M. Palatal canine displacement: Guidance theory or an anomaly of genetic origin? Angle Orthod. 1995, 65, 95–102. [Google Scholar]
- Lempesi, E.; Karamolegkou, M.; Pandis, N.; Mavragani, M. Maxillary canine impaction in orthodontic patients with and without agenesis: A cross-sectional radiographic study. Angle Orthod. 2014, 84, 11–17. [Google Scholar] [CrossRef]
- Papadopoulos, M.A.; Chatzoudi, M.; Kaklamanos, E.G. Prevalence of tooth transposition. A meta-analysis. Angle Orthod. 2010, 80, 275–285. [Google Scholar] [CrossRef]
- Gonnissen, H.; Politis, C.; Schepers, S.; Lambrichts, I.; Vrielinck, L.; Sun, Y.; Schuermans, J. Long-term success and survival rates of autogenously transplanted canines. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 110, 570–578. [Google Scholar] [CrossRef]
- Huth, K.C.; Nazet, M.; Paschos, E.; Linsenmann, R.; Hickel, R.; Nolte, D. Autotransplantation and surgical uprighting of impacted or retained teeth. A retrospective clinical study and evaluation of patient satisfaction. Acta Odontol. Scand. 2013, 71, 1538–1546. [Google Scholar] [CrossRef] [PubMed]
- Czochrowska, E.M.; Stenvik, A.; Bjercke, B.; Zachrisson, B.U. Outcome of tooth transplantation: Survival and success rates 17–41 years posttreatment. Am. J. Orthod. Dentofac. Orthop. 2002, 121, 110–119. [Google Scholar] [CrossRef]
- Atala-Acevedo, C.; Abarca, J.; Martínez-Zapata, M.J.; Díaz, J.; Olate, S.; Zaror, C. Success rate of autotransplantation of teeth with an open apex: Systematic review and meta-analysis. J. Oral Maxillofac. Surg. 2017, 75, 35–50. [Google Scholar] [CrossRef]
- Plakwicz, P.; Wojtaszek, J.; Zadurska, M. New bone formation at the site of autotransplanted developing mandibular canines: A case report. Int. J. Periodontics Restor. Dent. 2013, 33, 13–20. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author | Number of Patients/ Number of Impacted Canines | Number of Controls | Dental Anomaly in Total | Peg-Shaped/Small Maxillary Lateral Incisors | Maxillary Lateral Incisor Agenesis | Second Premolars Agenesis | Missing Third Molars | Tooth Agenesis | Transposition | Supernumerary Teeth | Impaction of Other Teeth | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Impacted Canine | Control Group | Impacted Canine | Control Group | Impacted Canine | Control Group | Impacted Canine | Control Group | Impacted Canine | Control Group | Impacted Canine | Control Group | Impacted Canine | Control Group | Impacted Canine | Control Group | ||||
| Oliver et al. [11] | 60 1 | - | 3.3% 1 | ||||||||||||||||
| Bjerklin et al. [12] | 91 1 | - | 5.5% 1 | ||||||||||||||||
| Mossey et al. [13] | 182 1 | - | 12.6% 1 | ||||||||||||||||
| Peck et al. [14] | 58 1/76 1 | - | 17.2% 1 | 3.4% 1 | 13.8% 1 | 39.7% 1 | 17.2% 1 | ||||||||||||
| Pirinen et al. [15] | 106/ 105 1, 1 2 | 9.4% 1 | 35.8% 1 | 1.9% 1 | 1.9% 1 | ||||||||||||||
| Chaushu et al. [16] | 58 1/58 1 | 40 | 18.1% 4/ 1.1% 5 | 14.6% 1 | 1.2% | 3.5% 1 | 0% | ||||||||||||
| Leifert et al. [17] | 235/281 1 | 235 | - | 11.5% 1 | 2.55% | 7.2% 1 | 0.85% | 11.5% 1 | 8.3% | 15.3% 1 | 8.1% | 12.8% 1 | 3% | ||||||
| Peck el al. [18] | 58 1 | 57% 4 | 3% 1 | 14% 1 | 40% 1 | ||||||||||||||
| Jena et al. [19] | 66 1 | 11.8% 1/ 38.9% 2 | 16.7% 1/ 2.9% 2 | 14.8% 1/ 2.9% 2 | |||||||||||||||
| Mercuri et al. [20] | 151/ 114 1, 37 2 | 151 | - | 10.5% 1/ 8.1% 2 | 2% | 6.1% 1/ 0% 2 | 2% | 2.7% 1/ 2.7% 2 | 2.7% | 5.3% 1/ 0% 2 | 0.7% | 0.9% 1/ 2.7% 2 | 0% | 17.5% 1/ 10.8% 2 | 6% | ||||
| Yan et al. [21] | 170/ 69 1, 101 2 | 170 | 42.4% 4/ 27% 5 | 40.3% 1/ 9.9% 2 | 4% | 4.3% 1/ 0% 2 | 0% | 36.2% 1/ 30.7% 2 | 23.8% | 15.5% 1/5.9% 2 | 3% | ||||||||
| Sajnani et al. [22] | 533 1 | 47.5% 4 | 10.1% 1/ 6.3% 2 | 11.4% 1/ 7.5% 2 | 6.9% 1/ 8.2% 2 | 4.6% 1/ 10.8% 2 | |||||||||||||
| Scerri et al. [23] | 477 1 | 500 | 78.2% 4/ 43.8% 5 | 20.1% 3 | 9% 3 | 20.1% 3 | 9% 3 | 9.2% | 6% | 37.9% | 28.8% | 1.9% | |||||||
| Herrera-Atoche et al. [24] | 52 1/65 1 | 808 | 52% 4/20 5 | 1.9% | 1.4% | 7.7% | 4.8% | 23.1% | 1.1% | 5.8% | 4.9% | 19.2% | 5.6% | ||||||
| Author | Number of Impacted Mandibular Canines | Material | Prevalence of Canine Impaction | Prevalence of Canine Transmigration | Other Dental Anomalies |
|---|---|---|---|---|---|
| Aydin et al. [26] | 22 | 4500 consecutive radiographs | 0.44% | 0.18% | |
| Buyukkurt et al. [27] | 15 | 4500 radiographs | 0.33% | 100% canine transmigration, tooth impaction in 6 patients | |
| Yavuz et al. [28] | 65 patients | 5022 radiographs | 1.29% | ||
| González-Sánchez et al. [29] | 15 | Retrospective evaluation | 100% canine transmigration, 2 supernumerary teeth | ||
| Aktan et al. [30] | 26 | 5000 radiographs | 0.46% | 0.34% | No anomalies except for pathologies such as cysts or odontomas |
| Celikoglu et al. [31] | 9 | 2215 orthodontic patients | 0.4% | 0.22% | |
| Gunduz et al. [32] | 86 | 12,129 radiographs | 0.71% | ||
| Kara et al. [33] | 85 | 112,873 radiographs | 0.075% | 100% canine transmigration; odontomas (4), other impactions (12), transposition (6), second premolar agenesis (4), upper lateral incisor agenesis (3), supernumerary molar (1) | |
| Aras et al. [34] | 63 patients, 23 canines evaluated | 5100 radiographs | 1.35% | ||
| Topkara et al. [35] | 14 patients | 1527 orthodontic patients | 0.92% | ||
| Jain et al. [36] | 43 patients | 10,422 patients | 0.41% | ||
| Kamiloglu and Kelahmet [37] | 4 | 453 orthodontic/ pedodontic patients | 0.88% | ||
| Sajnani and King [38] | 64 | 20,347 orthodontic/ pedodontic patients | 0.31% |
| Number of Dental Anomalies per Patient | MaxCI (%) | ManCI (%) | Control (%) |
|---|---|---|---|
| 0 | 33 (47.1) | 15 (46.9) | 93 (79.5) |
| 1 | 19 (27.1) | 8 (25) | 12 (10.3) |
| 2 | 9 (12.9) | 4 (12.5) | 8 (6.8) |
| 3 | 4 (5.7) | 3 (9.4) | 2 (1.7) |
| 4 | 1 (1.43) | 0 (0) | 1 (0.85) |
| 5 | 1 (1.43) | 1 (3.1) | 0 (0) |
| 6 | 1 (1.43) | 1 (3.1) | 1 (0.85) |
| 8 | 1 (1.43) | 0 (0) | |
| 10 | 1 (1.43) | 0 (0) | |
| Total | 70 (100) | 32 (100) | 117 (100) |
| Anomaly | Location | Prevalence (%) | OR (95% CI) | p-Value |
|---|---|---|---|---|
| Peg-shaped Maxillary Lateral Incisor | Maxillary | 10/70 (14.3) | 5.11 (0.67, 231.33) | 0.17 |
| Mandible | 1/32 (3.1) | Reference | ||
| Agenesis of Maxillary Lateral Incisor | Maxilla | 5/70 (7.1) | 1.15 (0.18, 12.75) | 0.87 |
| Mandible | 2/32 (6.3) | Reference | ||
| Agenesis of Second Premolar | Maxilla | 8/70 (11.4) | 3.96 (0.49, 183.12) | 0.32 |
| Mandible | 1/32 (3.1) | Reference | ||
| Agenesis of Mandibular Incisor | Maxilla | 4/70 (7.1) | 1.87 (0.18, 95.47) | 0.99 |
| Mandible | 1/32 (3.1) | Reference | ||
| Agenesis of Any Tooth | Maxilla | 29/70 (41.4) | 3.03 (1.04, 10.18) | 0.04 * |
| Mandible | 6/32 (18.8) | Reference | ||
| Supernumerary Tooth | Maxilla | 2/70 (2.9) | 0.13 (0.01, 0.79) | 0.02 * |
| Mandible | 6/32 (18.8) | Reference | ||
| Transposition | Maxilla | 4/70 (7.1) | 0.43 (0.07, 2.47) | 0.42 |
| Mandible | 4/32 (12.5) | Reference | ||
| Transmigration | Maxilla | 0/70 (0) | 0.05 (0.00, 0.35) | 0.001 ** |
| Mandible | 6/32 (18.8) | Reference | ||
| Tooth impaction | Maxilla | 4/70 (5.7) | 0.43 (0.07, 2,47) | 0.42 |
| Mandible | 4/32 (12.5) | Reference |
| Anomaly | Location | Prevalence (%) | OR (95% CI) | p-Value |
|---|---|---|---|---|
| Peg-shaped Maxillary Lateral Incisor | Maxilla | 10/70 (14.3) | 26.53 (4.16, +∞) | <0.001 *** |
| Mandible | 1/32 (3.1) | 3.66 (0.09, +∞) | 0.43 | |
| Control | 0/117 (0) | Reference | ||
| Agenesis of Maxillary Lateral Incisor | Maxilla | 5/70 (7.1) | 1.21 (0.29, 4.63) | 0.98 |
| Mandible | 2/32 (6.3) | 1.05 (0.10, 5.90) | 1 | |
| Control | 7/117 (6.0) | Reference | ||
| Agenesis of Second Premolar | Maxilla | 8/70 (11.4) | 1.59 (0.48, 6.88) | 0.29 |
| Mandible | 1/32 (3.1) | 0.51 (0.01, 4.21) | 0.91 | |
| Control | 7/117 (6.0) | Reference | ||
| Agenesis of Mandibular Incisor | Maxilla | 4/70 (7.1) | 9.18 (1.13, +∞) | 0.43 |
| Mandible | 1/32 (3.1) | 3.66 (0.09, +∞) | 0.04 * | |
| Control | 0/117 (0) | Reference | ||
| Agenesis of Any Tooth | Maxilla | 29/70 (41.4) | 2.87 (1.41, 5.89) | 0.003 ** |
| Mandible | 6/32 (18.8) | 0.94 (0.28, 2.72) | 1 | |
| Control | 23/117 (20.0) | Reference | ||
| Supernumerary Tooth | Maxilla | 2/70 (2.9) | Not estimable as all 0 in MaxCI vs. controls | |
| Mandible | 6/32 (18.8) | 34.97 (4.85, +∞) | <0.001 *** | |
| Control | 0/117 (0) | Reference | ||
| Transposition | Maxilla | 4/70 (7.1) | 6.96 (0.67, 349.13) | 0.13 |
| Mandible | 4/32 (12.5) | 16.15 (1.52, 822.8) | 0.02 * | |
| Control | 1/117 (0.9) | Reference | ||
| Transmigration | Maxilla | 0/70 (0) | 4.08 (0.32, +∞) | 0.28 |
| Mandible | 6/32 (18.8) | 34.97 (4.85, +∞) | <0.001 ** | |
| Control | 0/117 (0) | Reference | ||
| Tooth impaction | Maxilla | 4/70 (5.7) | 9.18 (1.13, +∞) | 0.04 * |
| Mandible | 4/32 (12.5) | 21.11 (2.56, +∞) | 0.004 ** | |
| Control | 0/117 (0) | Reference |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stabryła, J.; Zadurska, M.; Plakwicz, P.; Kukuła, K.T.; Czochrowska, E.M. Comparisons of Dental Anomalies in Orthodontic Patients with Impacted Maxillary and Mandibular Canines. Diagnostics 2023, 13, 2766. https://doi.org/10.3390/diagnostics13172766
Stabryła J, Zadurska M, Plakwicz P, Kukuła KT, Czochrowska EM. Comparisons of Dental Anomalies in Orthodontic Patients with Impacted Maxillary and Mandibular Canines. Diagnostics. 2023; 13(17):2766. https://doi.org/10.3390/diagnostics13172766
Chicago/Turabian StyleStabryła, Joanna, Małgorzata Zadurska, Paweł Plakwicz, Krzysztof Tadeusz Kukuła, and Ewa Monika Czochrowska. 2023. "Comparisons of Dental Anomalies in Orthodontic Patients with Impacted Maxillary and Mandibular Canines" Diagnostics 13, no. 17: 2766. https://doi.org/10.3390/diagnostics13172766