
Steatosis Quantification on Ultrasound Images by a Deep Learning Algorithm on Patients Undergoing Weight Changes
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
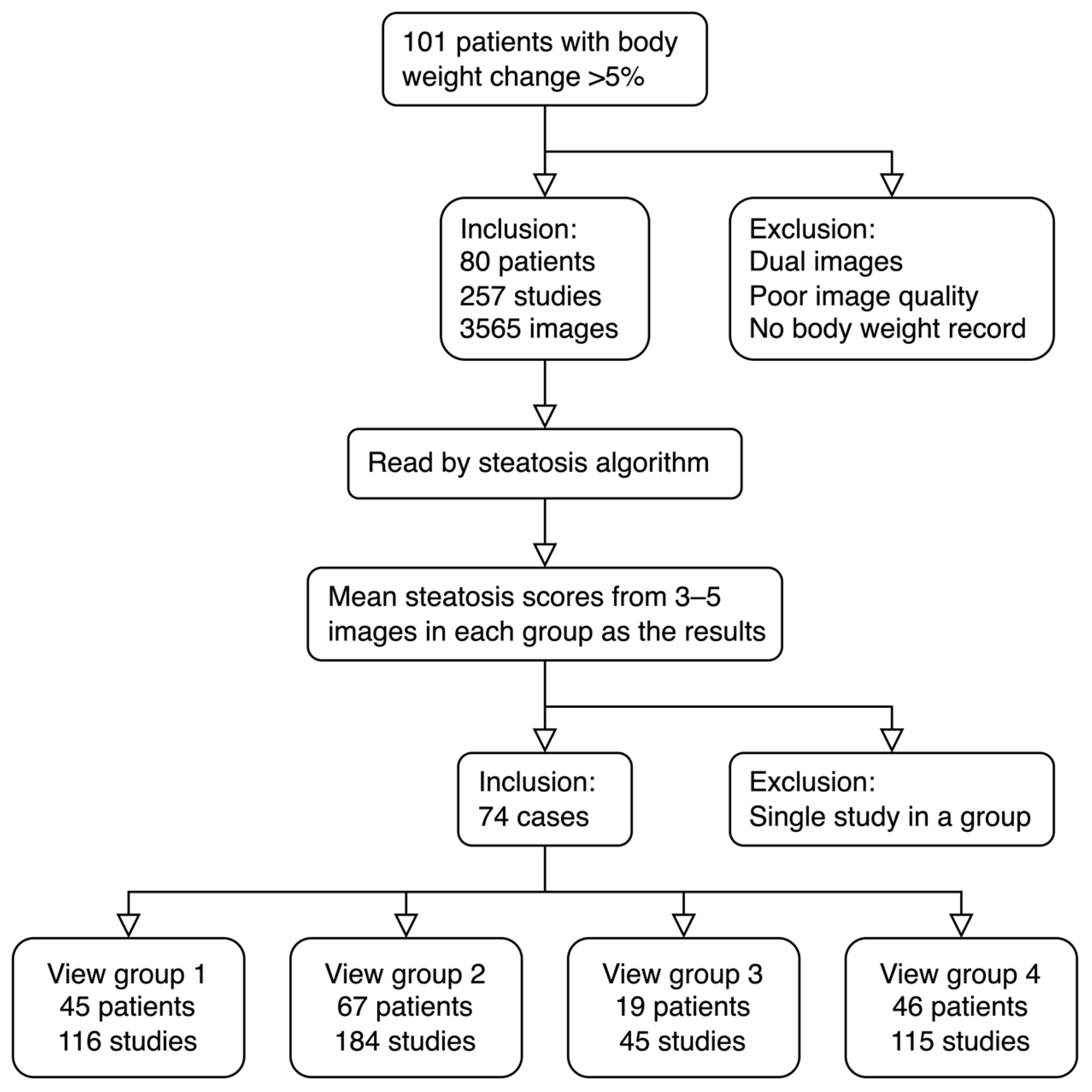
2.1. Patients
2.2. Image Views
2.3. Preparation and Reading of Images
2.4. Ultrasound Steatosis Score
2.5. Statistical Analysis
3. Results
3.1. View Groups of the Study
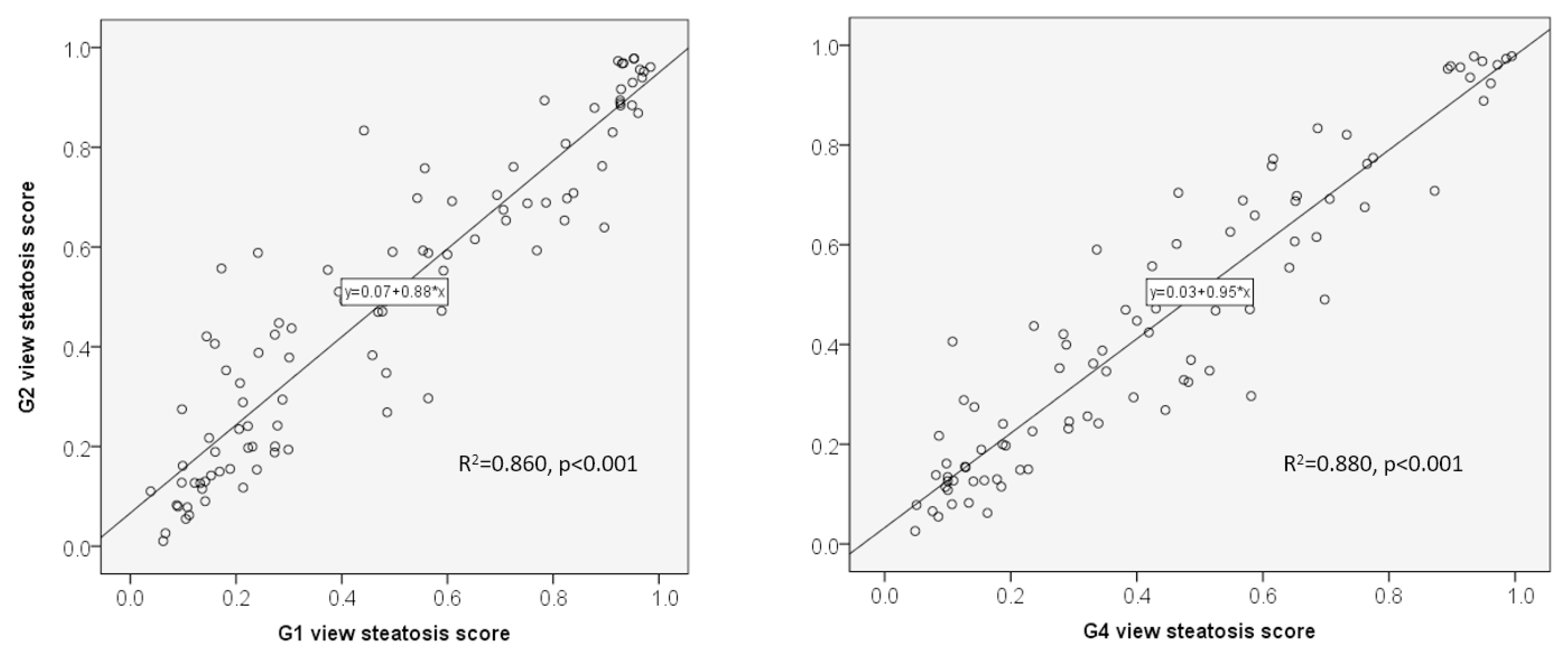
3.2. Head-to-Head Comparison of Steatosis Scores between Two Groups in the Same Patient
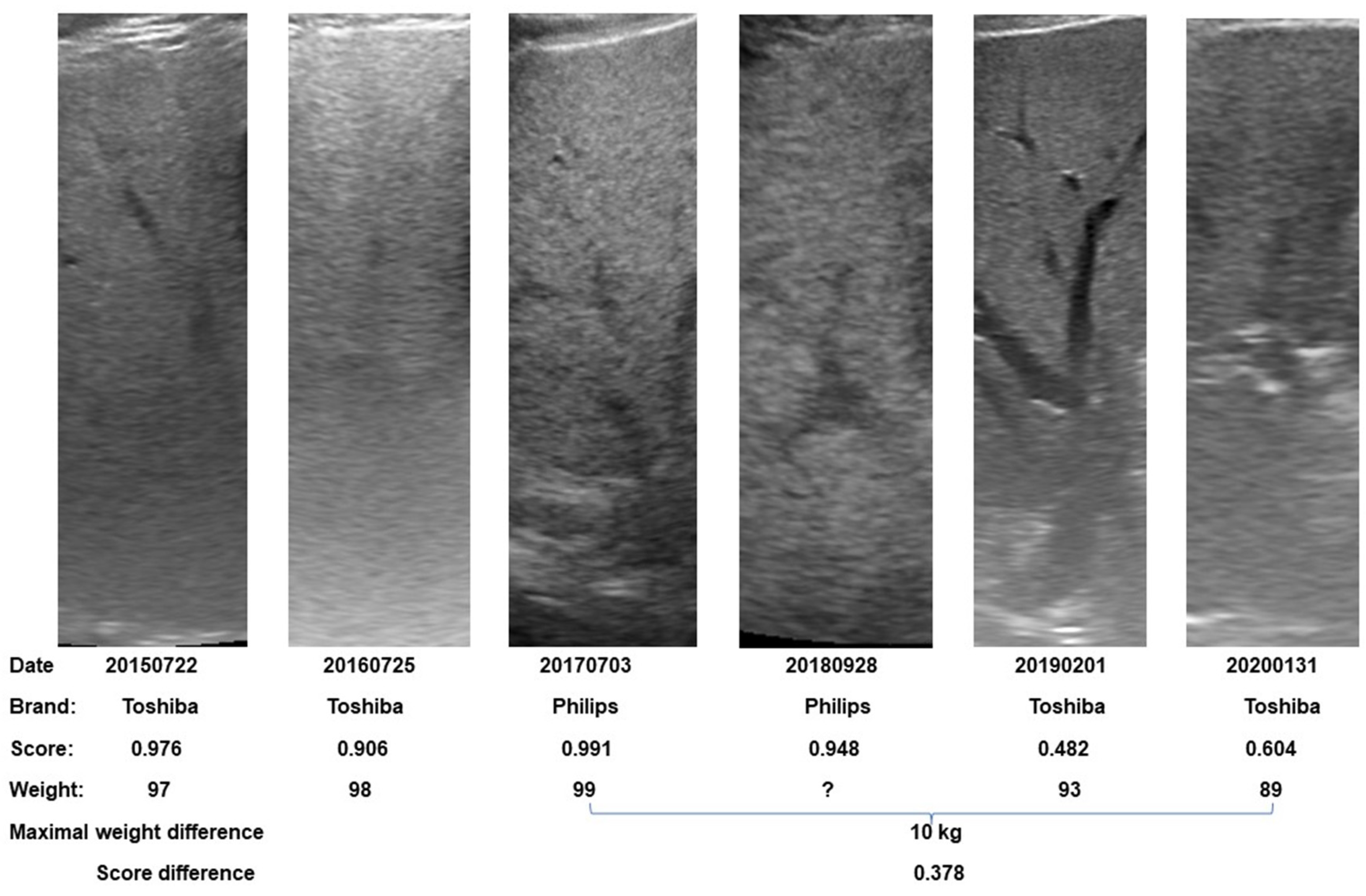
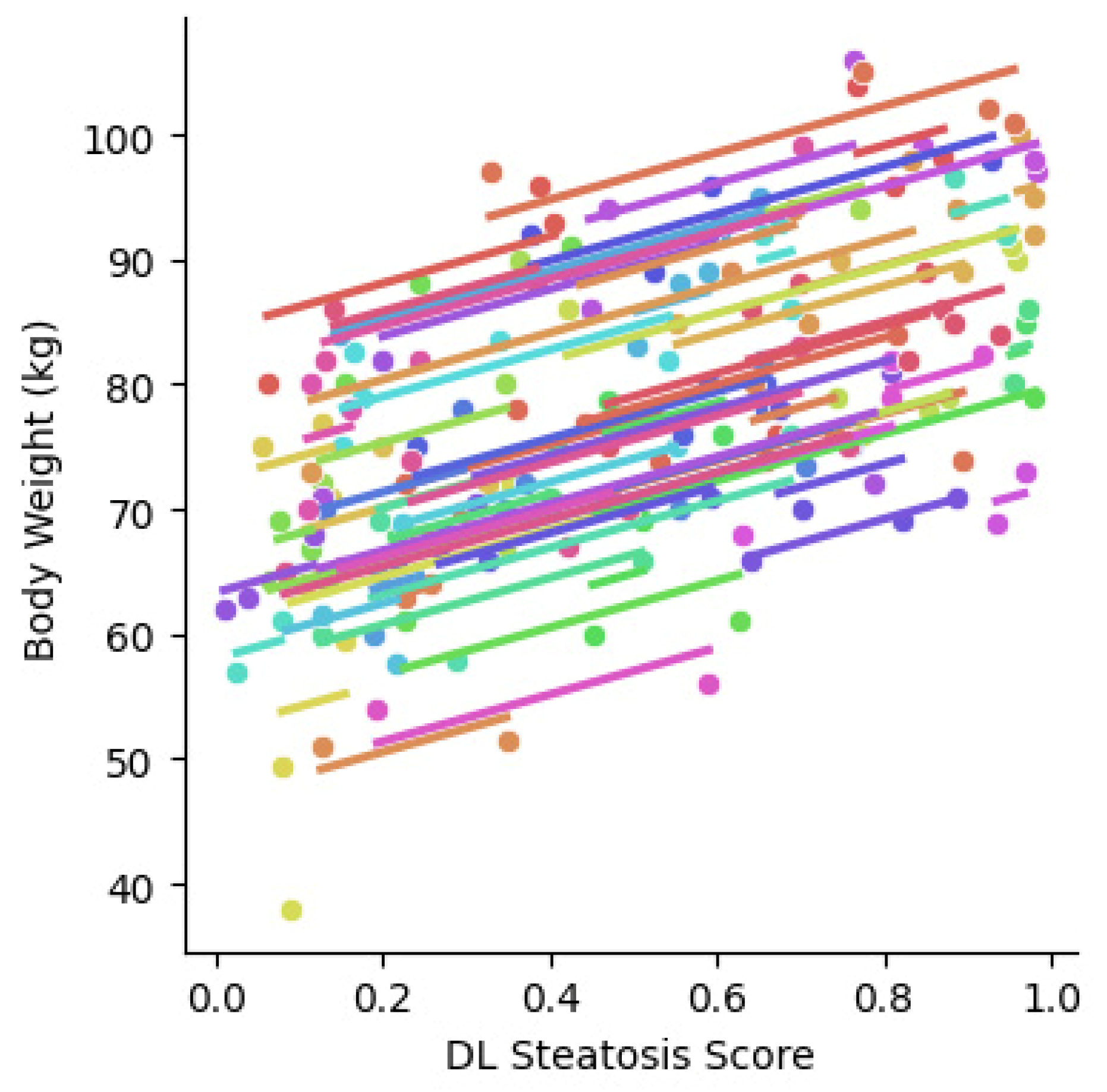
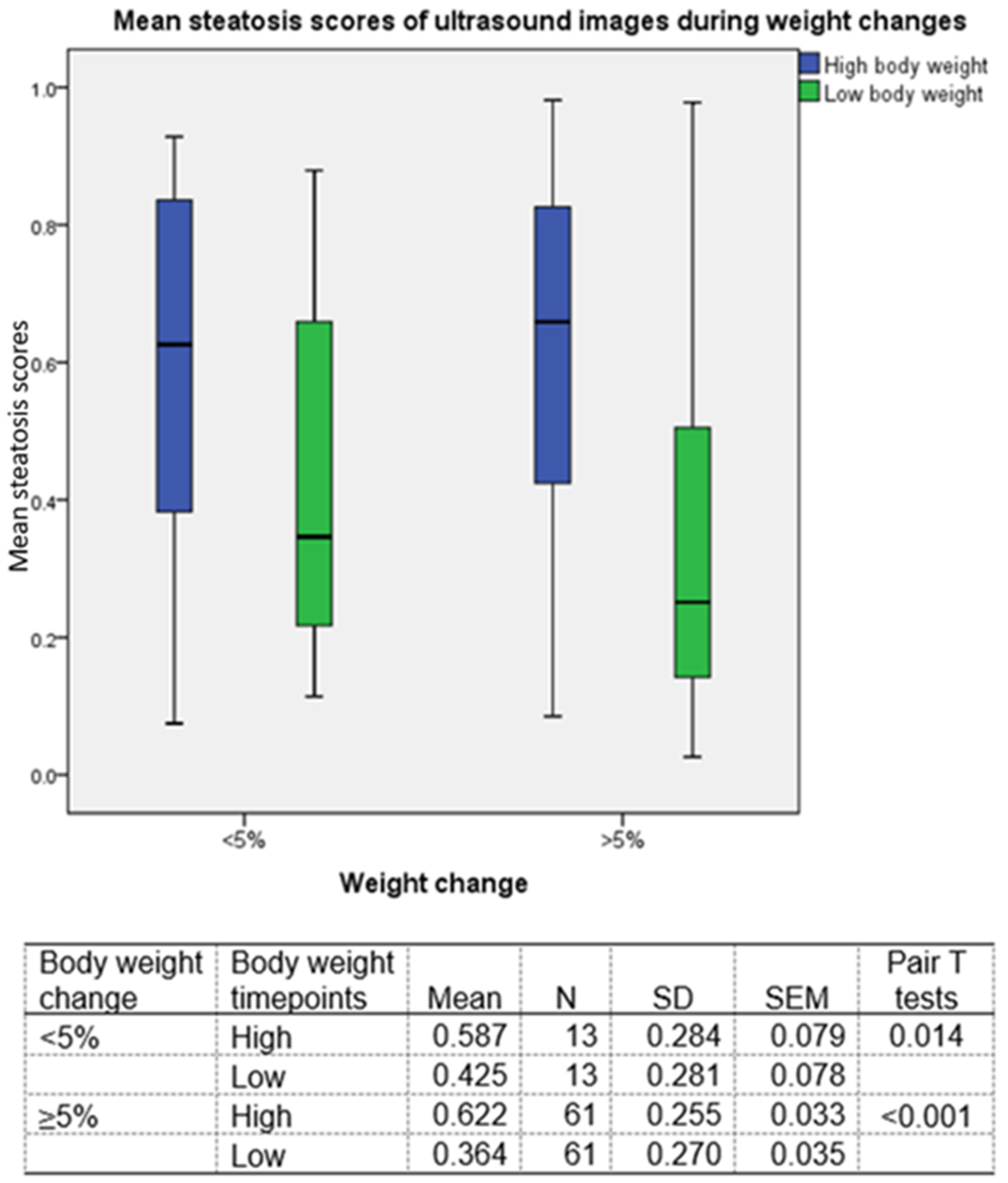
3.3. Correlation between Body Weight and Steatosis Score
3.4. Differences in Steatosis Scores across Gender Differences
3.5. Brands of Ultrasound Scanners Used in Different Viewpoints
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Younossi, Z.M.; Golabi, P.; Paik, J.M.; Henry, A.; Van Dongen, C.; Henry, L. The Global Epidemiology of Nonalcoholic Fatty Liver Disease (NAFLD) and Nonalcoholic Steatohepatitis (NASH): A Systematic Review. Hepatology 2023, 77, 1335–1347. [Google Scholar] [CrossRef]
- Caussy, C.; Reeder, S.B.; Sirlin, C.B.; Loomba, R. Noninvasive, Quantitative Assessment of Liver Fat by MRI-PDFF as an Endpoint in NASH Trials. Hepatology 2018, 68, 763–772. [Google Scholar] [CrossRef] [PubMed]
- Bae, J.S.; Lee, D.H.; Suh, K.-S.; Kim, H.; Lee, K.B.; Lee, J.Y.; Han, J.K. Noninvasive Assessment of Hepatic Steatosis Using a Pathologic Reference Standard: Comparison of CT, MRI, and US-Based Techniques. Ultrasonography 2022, 41, 344–354. [Google Scholar] [CrossRef] [PubMed]
- Fetzer, D.T.; Rosado-Mendez, I.M.; Wang, M.; Robbin, M.L.; Ozturk, A.; Wear, K.A.; Ormachea, J.; Stiles, T.A.; Fowlkes, J.B.; Hall, T.J.; et al. Pulse-Echo Quantitative US Biomarkers for Liver Steatosis: Toward Technical Standardization. Radiology 2022, 305, 265–276. [Google Scholar] [CrossRef]
- Castera, L.; Friedrich-Rust, M.; Loomba, R. Noninvasive Assessment of Liver Disease in Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2019, 156, 1264–1281.e4. [Google Scholar] [CrossRef]
- Bae, J.S.; Lee, D.H.; Lee, J.Y.; Kim, H.; Yu, S.J.; Lee, J.-H.; Cho, E.J.; Lee, Y.B.; Han, J.K.; Choi, B.I. Assessment of Hepatic Steatosis by Using Attenuation Imaging: A Quantitative, Easy-to-Perform Ultrasound Technique. Eur. Radiol. 2019, 29, 6499–6507. [Google Scholar] [CrossRef]
- Jung, J.; Han, A.; Madamba, E.; Bettencourt, R.; Loomba, R.R.; Boehringer, A.S.; Andre, M.P.; Erdman, J.W.; O’Brien, W.D.; Fowler, K.J.; et al. Direct Comparison of Quantitative US versus Controlled Attenuation Parameter for Liver Fat Assessment Using MRI Proton Density Fat Fraction as the Reference Standard in Patients Suspected of Having NAFLD. Radiology 2022, 304, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Jeon, S.K.; Lee, J.M.; Joo, I.; Yoon, J.H.; Lee, G. Two-Dimensional Convolutional Neural Network Using Quantitative US for Noninvasive Assessment of Hepatic Steatosis in NAFLD. Radiology 2023, 307, 221510. [Google Scholar] [CrossRef] [PubMed]
- Ormachea, J.; Parker, K.J. A Preliminary Study of Liver Fat Quantification Using Reported Ultrasound Speed of Sound and Attenuation Parameters. Ultrasound Med. Biol. 2022, 48, 675–684. [Google Scholar] [CrossRef]
- Li, B.; Tai, D.-I.; Yan, K.; Chen, Y.-C.; Chen, C.-J.; Huang, S.-F.; Hsu, T.-H.; Yu, W.-T.; Xiao, J.; Le, L.; et al. Accurate and Generalizable Quantitative Scoring of Liver Steatosis from Ultrasound Images via Scalable Deep Learning. World J. Gastroenterol. 2022, 28, 2494–2508. [Google Scholar] [CrossRef]
- Sanabria, S.J.; Pirmoazen, A.M.; Dahl, J.; Kamaya, A.; El Kaffas, A. Comparative Study of Raw Ultrasound Data Representations in Deep Learning to Classify Hepatic Steatosis. Ultrasound Med. Biol. 2022, 48, 2060–2078. [Google Scholar] [CrossRef]
- Han, A.; Byra, M.; Heba, E.; Andre, M.P.; Erdman, J.W.; Loomba, R.; Sirlin, C.B.; O’Brien, W.D. Noninvasive Diagnosis of Nonalcoholic Fatty Liver Disease and Quantification of Liver Fat with Radiofrequency Ultrasound Data Using One-Dimensional Convolutional Neural Networks. Radiology 2020, 295, 342–350. [Google Scholar] [CrossRef]
- Chen, J.-R.; Chao, Y.-P.; Tsai, Y.-W.; Chan, H.-J.; Wan, Y.-L.; Tai, D.-I.; Tsui, P.-H. Clinical Value of Information Entropy Compared with Deep Learning for Ultrasound Grading of Hepatic Steatosis. Entropy 2020, 22, 1006. [Google Scholar] [CrossRef]
- Cao, W.; An, X.; Cong, L.; Lyu, C.; Zhou, Q.; Guo, R. Application of Deep Learning in Quantitative Analysis of 2-Dimensional Ultrasound Imaging of Nonalcoholic Fatty Liver Disease. J. Ultrasound Med. 2020, 39, 51–59. [Google Scholar] [CrossRef]
- Byra, M.; Han, A.; Boehringer, A.S.; Zhang, Y.N.; O’Brien, W.D.; Erdman, J.W.; Loomba, R.; Sirlin, C.B.; Andre, M. Liver Fat Assessment in Multiview Sonography Using Transfer Learning With Convolutional Neural Networks. J. Ultrasound Med. 2022, 41, 175–184. [Google Scholar] [CrossRef]
- Alshagathrh, F.M.; Househ, M.S. Artificial Intelligence for Detecting and Quantifying Fatty Liver in Ultrasound Images: A Systematic Review. Bioengineering 2022, 9, 748. [Google Scholar] [CrossRef]
- Patel, N.S.; Doycheva, I.; Peterson, M.R.; Hooker, J.; Kisselva, T.; Schnabl, B.; Seki, E.; Sirlin, C.B.; Loomba, R. Effect of Weight Loss on MRI Estimation of Liver Fat and Volume in Patients With Nonalcoholic Steatohepatitis. Clin. Gastroenterol. Hepatol. 2015, 13, 561–568.e1. [Google Scholar] [CrossRef]
- Katsagoni, C.N.; Papatheodoridis, G.V.; Ioannidou, P.; Deutsch, M.; Alexopoulou, A.; Papadopoulos, N.; Papageorgiou, M.-V.; Fragopoulou, E.; Kontogianni, M.D. Improvements in Clinical Characteristics of Patients with Non-Alcoholic Fatty Liver Disease, after an Intervention Based on the Mediterranean Lifestyle: A Randomised Controlled Clinical Trial. Br. J. Nutr. 2018, 120, 164–175. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; IEEE: New York, NY, USA, 2016; pp. 770–778. [Google Scholar]
- Frank, E.; Hall, M. A simple approach to ordinal classification. In Proceedings of the Machine Learning: ECML 2001, Freiburg, Germany, 5–7 September 2001; De Raedt, L., Flach, P., Eds.; Springer: Berlin/Heidelberg, Germany, 2001; pp. 145–156. [Google Scholar]
- Bakdash, J.Z.; Marusich, L.R. Repeated Measures Correlation. Front. Psychol. 2017, 8, 456. [Google Scholar] [CrossRef]
- Vallat, R. Pingouin: Statistics in Python. J. Open Source Softw. 2018, 3, 1026. [Google Scholar] [CrossRef]
- Vilar-Gomez, E.; Martinez-Perez, Y.; Calzadilla-Bertot, L.; Torres-Gonzalez, A.; Gra-Oramas, B.; Gonzalez-Fabian, L.; Friedman, S.L.; Diago, M.; Romero-Gomez, M. Weight Loss Through Lifestyle Modification Significantly Reduces Features of Nonalcoholic Steatohepatitis. Gastroenterology 2015, 149, 367–378.e5. [Google Scholar] [CrossRef]
- Covarrubias, Y.; Fowler, K.J.; Mamidipalli, A.; Hamilton, G.; Wolfson, T.; Leinhard, O.D.; Jacobsen, G.; Horgan, S.; Schwimmer, J.B.; Reeder, S.B.; et al. Pilot Study on Longitudinal Change in Pancreatic Proton Density Fat Fraction during a Weight-Loss Surgery Program in Adults with Obesity. J. Magn. Reason. Imaging 2019, 50, 1092–1102. [Google Scholar] [CrossRef]
- Kim, T.; Lee, D.H.; Park, E.-K.; Choi, S. Deep Learning Techniques for Fatty Liver Using Multi-View Ultrasound Images Scanned by Different Scanners: Development and Validation Study. JMIR Med. Inform. 2021, 9, e30066. [Google Scholar] [CrossRef]
- Yang, Y.; Liu, J.; Sun, C.; Shi, Y.; Hsing, J.C.; Kamya, A.; Keller, C.A.; Antil, N.; Rubin, D.; Wang, H.; et al. Nonalcoholic Fatty Liver Disease (NAFLD) Detection and Deep Learning in a Chinese Community-Based Population. Eur. Radiol. 2023, 33, 5894–5906. [Google Scholar] [CrossRef]
- Ayonrinde, O.T.; Olynyk, J.K.; Beilin, L.J.; Mori, T.A.; Pennell, C.E.; de Klerk, N.; Oddy, W.H.; Shipman, P.; Adams, L.A. Gender-Specific Differences in Adipose Distribution and Adipocytokines Influence Adolescent Nonalcoholic Fatty Liver Disease. Hepatology 2011, 53, 800–809. [Google Scholar] [CrossRef]
- White, U.A.; Tchoukalova, Y.D. Sex Dimorphism and Depot Differences in Adipose Tissue Function. Biochim. Biophys. Acta 2014, 1842, 377–392. [Google Scholar] [CrossRef]
- Wawrzkiewicz-Jałowiecka, A.; Lalik, A.; Soveral, G. Recent Update on the Molecular Mechanisms of Gonadal Steroids Action in Adipose Tissue. Int. J. Mol. Sci. 2021, 22, 5226. [Google Scholar] [CrossRef]
- Lonardo, A.; Nascimbeni, F.; Ballestri, S.; Fairweather, D.; Win, S.; Than, T.A.; Abdelmalek, M.F.; Suzuki, A. Sex Differences in NAFLD: State of the Art and Identification of Research Gaps. Hepatology 2019, 70, 1457–1469. [Google Scholar] [CrossRef]
- Isacco, L.; Ennequin, G.; Boisseau, N. Influence of the Different Hormonal Status Changes during Their Life on Fat Mass Localisation in Women: A Narrative Review. Arch. Physiol. Biochem. 2021, 1–6. [Google Scholar] [CrossRef]
- Oh, S.; Tsujimoto, T.; Kim, B.; Uchida, F.; Suzuki, H.; Iizumi, S.; Isobe, T.; Sakae, T.; Tanaka, K.; Shoda, J. Weight-Loss-Independent Benefits of Exercise on Liver Steatosis and Stiffness in Japanese Men with NAFLD. JHEP Rep. 2021, 3, 100253. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | 1 Image | 2 Images | 3 Images | 4 Images | 5 Images |
|---|---|---|---|---|---|
| 1 | 0.4614 (0.4210, 0.5078) | 0.3263 (0.2957, 0.3552) | 0.2664 (0.2397, 0.2934) | 0.2307 (0.2089, 0.2555) | 0.2064 (0.1874, 0.2259) |
| 2 | 0.3665 (0.3385, 0.3942) | 0.2592 (0.2381, 0.2797) | 0.2116 (0.1955, 0.2298) | 0.1833 (0.1697, 0.1996) | 0.1639 (0.1508, 0.1763) |
| 3 | 0.5264 (0.4711, 0.5814) | 0.3722 (0.3292, 0.4135) | 0.3039 (0.2717, 0.3393) | 0.2632 (0.2350, 0.2906) | 0.2354 (0.2117, 0.2596) |
| 4 | 0.4583 (0.4150, 0.5029) | 0.3240 (0.2945, 0.3587) | 0.2646 (0.2361, 0.2920) | 0.2291 (0.2067, 0.2547) | 0.2049 (0.1833, 0.2267) |
| Category | Number (%) or Mean ± SD |
|---|---|
| Total No. | 74 |
| Gender | |
| Male | 48 (64.9%) |
| Female | 26 (35.1%) |
| Etiology | |
| NBNC | 26 (35.1%) |
| HBV | 43 (58.1%) |
| HCV | 4 (5.4%) |
| Alcoholic | 1 (1.4%) |
| Age (year) | 51.74 ± 9.85 |
| Initial body height (cm) | 165.88 ± 7.88 |
| Initial body weight (kg) | 80.74 ± 12.12 |
| Initial AST (U/L) | 33.34 ± 18.58 |
| Initial ALT (U/L) | 39.90 ± 31.77 |
| Initial total cholesterol (mg) | 204.72 ± 58.49 |
| Initial triglyceride (mg) | 202.56 ± 141.51 |
| Image View | Study No. | Steatosis Score | |||
|---|---|---|---|---|---|
| Mean | SD | SEM | p Value | ||
| G1 | 99 | 0.481 | 0.312 | 0.031 | 0.377 |
| G2 | 99 | 0.491 | 0.297 | 0.030 | |
| G2 | 89 | 0.441 | 0.289 | 0.031 | 0.357 |
| G4 | 89 | 0.431 | 0.286 | 0.030 | |
| Body Weight Timepoints | Category | Gender | No | Mean | SD | SEM | p Value |
|---|---|---|---|---|---|---|---|
| High | Steatosis score | M | 48 | 0.6458 | 0.2573 | 0.0371 | 0.173 |
| F | 26 | 0.5598 | 0.2560 | 0.0502 | |||
| BMI | M | 48 | 28.6137 | 3.3424 | 0.4824 | 0.071 | |
| F | 26 | 30.7566 | 5.3240 | 1.0441 | |||
| Steatosis score/BMI | M | 48 | 0.0223 | 0.0084 | 0.0012 | 0.026 | |
| F | 26 | 0.0179 | 0.0073 | 0.0014 | |||
| Low | Steatosis score | M | 48 | 0.3985 | 0.2847 | 0.0411 | 0.307 |
| F | 26 | 0.3307 | 0.2417 | 0.0474 | |||
| BMI | M | 48 | 26.0044 | 3.1512 | 0.4548 | 0.267 | |
| F | 26 | 27.0644 | 4.9994 | 0.9805 | |||
| Steatosis score/BMI | M | 48 | 0.0149 | 0.0100 | 0.0014 | 0.112 | |
| F | 26 | 0.0116 | 0.0074 | 0.0014 |
| View Groups | Brands | |||||
|---|---|---|---|---|---|---|
| Aloka SSD 5500 | Hitachi Preirus | Philips iU22 | Siemens S2000 | Toshiba TUS-A300 | Total | |
| 1 | 0 | 2 | 32 | 1 | 81 | 116 |
| 2 | 5 | 6 | 59 | 3 | 110 | 184 |
| 3 | 0 | 0 | 13 | 1 | 31 | 45 |
| 4 | 0 | 5 | 45 | 3 | 63 | 115 |
| Total (%) | 5 (1.1) | 13 (2.8) | 149 (32.4) | 8 (1.7) | 285 (62.0) | (100) 460 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harrison, A.P.; Li, B.; Hsu, T.-H.; Chen, C.-J.; Yu, W.-T.; Tai, J.; Lu, L.; Tai, D.-I. Steatosis Quantification on Ultrasound Images by a Deep Learning Algorithm on Patients Undergoing Weight Changes. Diagnostics 2023, 13, 3225. https://doi.org/10.3390/diagnostics13203225
Harrison AP, Li B, Hsu T-H, Chen C-J, Yu W-T, Tai J, Lu L, Tai D-I. Steatosis Quantification on Ultrasound Images by a Deep Learning Algorithm on Patients Undergoing Weight Changes. Diagnostics. 2023; 13(20):3225. https://doi.org/10.3390/diagnostics13203225
Chicago/Turabian StyleHarrison, Adam P., Bowen Li, Tse-Hwa Hsu, Cheng-Jen Chen, Wan-Ting Yu, Jennifer Tai, Le Lu, and Dar-In Tai. 2023. "Steatosis Quantification on Ultrasound Images by a Deep Learning Algorithm on Patients Undergoing Weight Changes" Diagnostics 13, no. 20: 3225. https://doi.org/10.3390/diagnostics13203225