
A Machine Learning-Based Severity Prediction Tool for the Michigan Neuropathy Screening Instrument
 , ,
, ,  , , ,
, , ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Database Description
2.2. Data Imputation
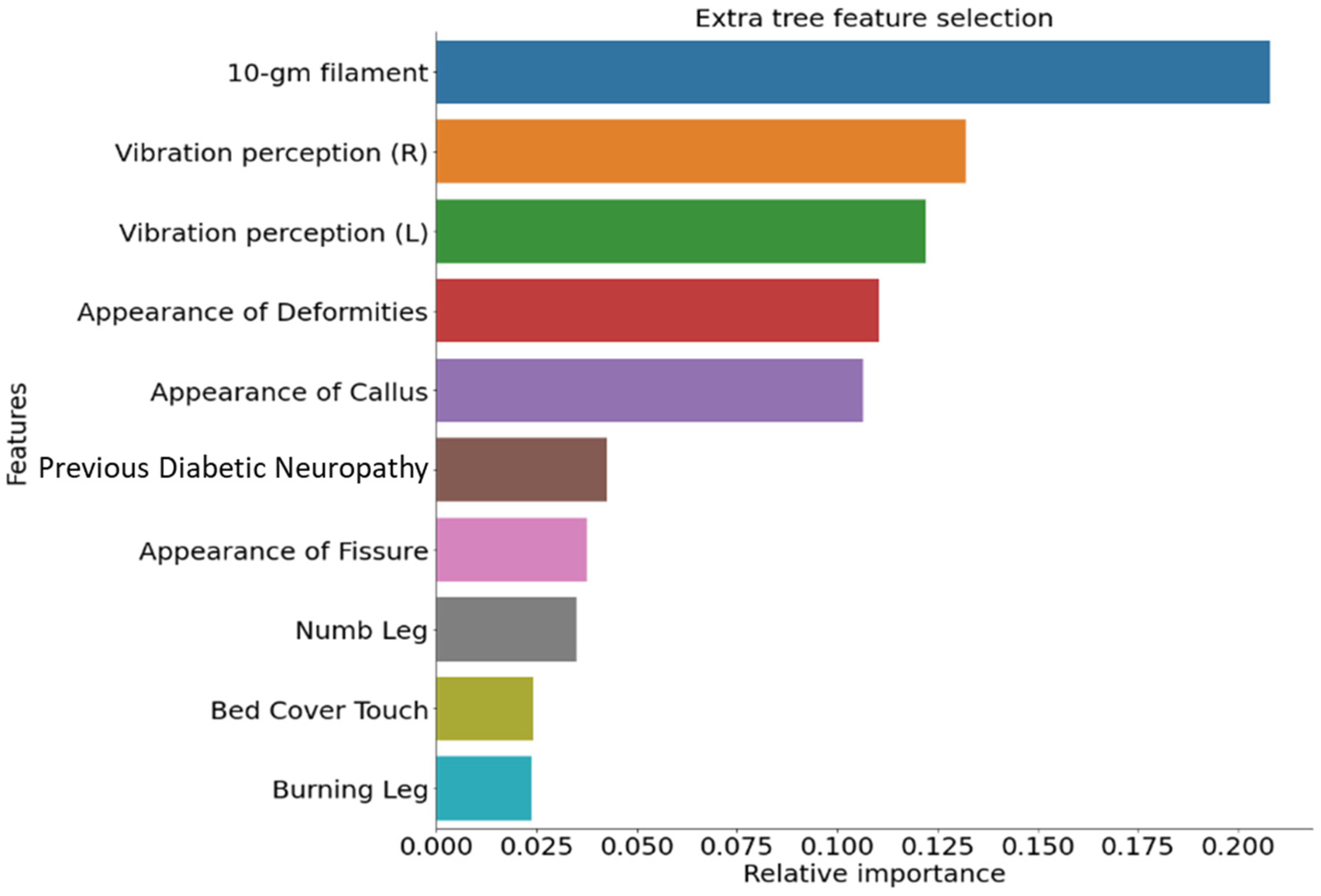
2.3. Feature Ranking
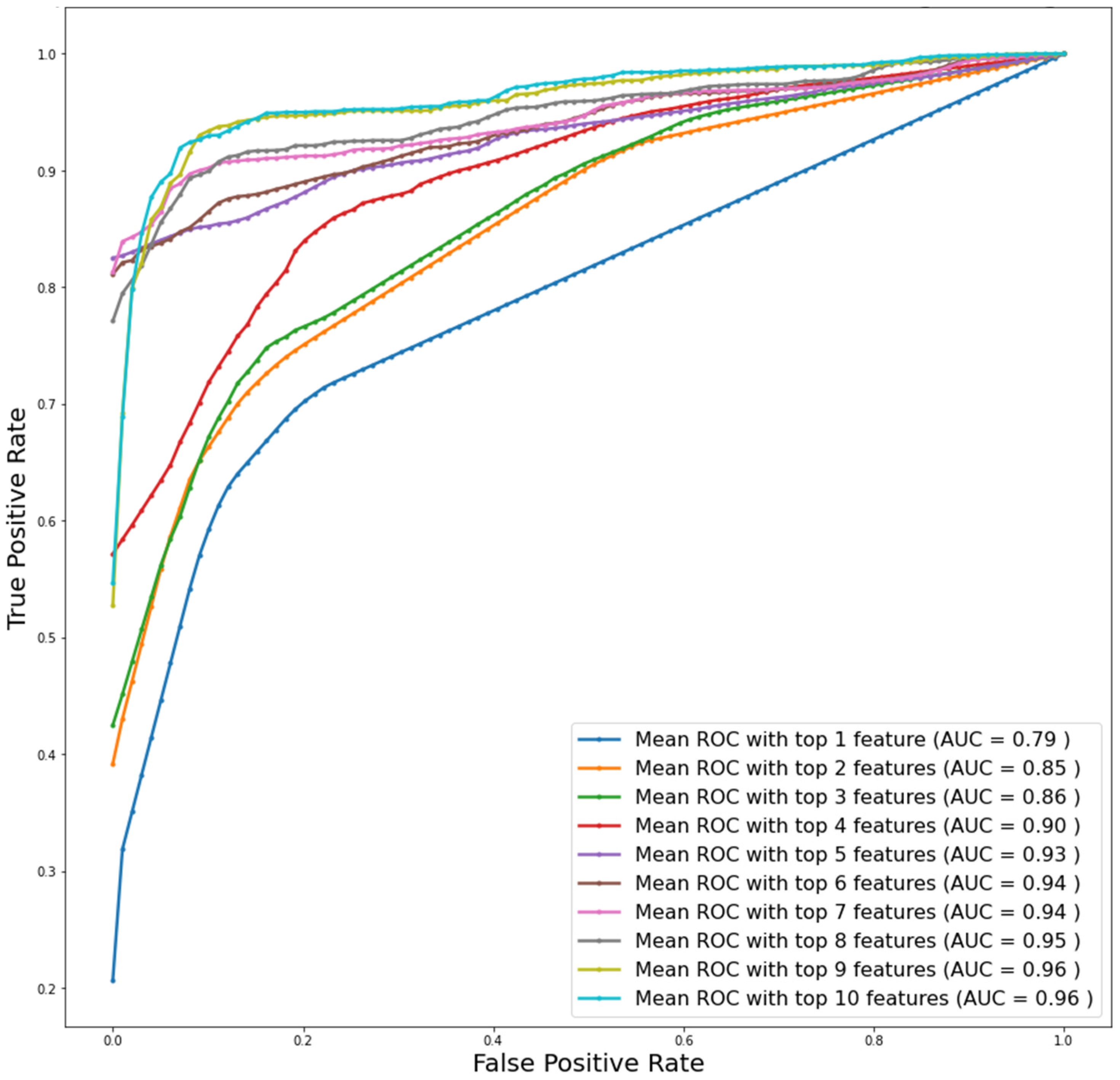
2.4. Logistic Regression Classifiers
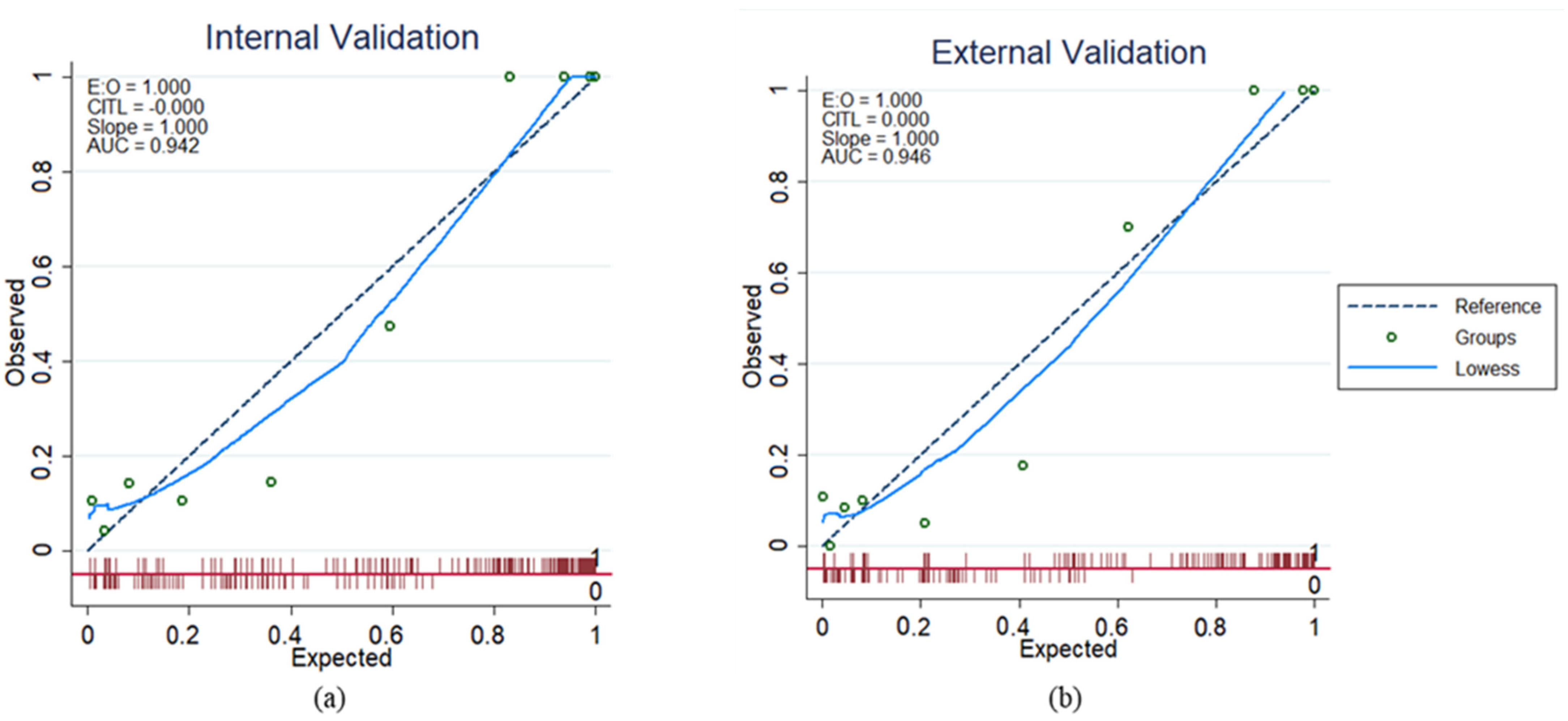
2.5. Development and Validation of Logistic Regression-Based Nomogram
2.6. Development and Validation of Severity Grading Score
3. Results
3.1. Patients’ Characteristics and Clinical Outcomes
3.2. Univariate Logistic Regression Model for Identifying Variables Significantly Associated with DSPN
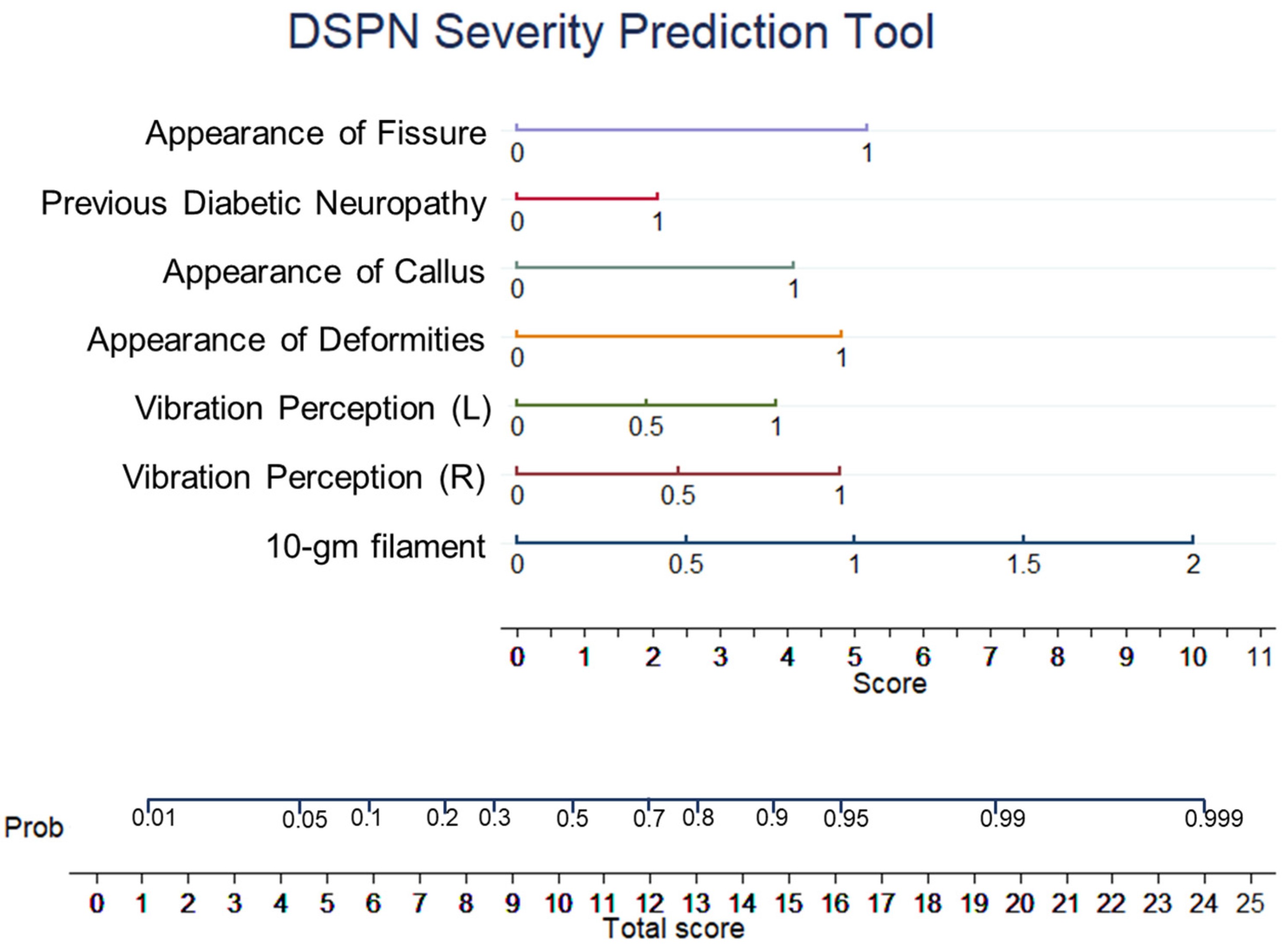
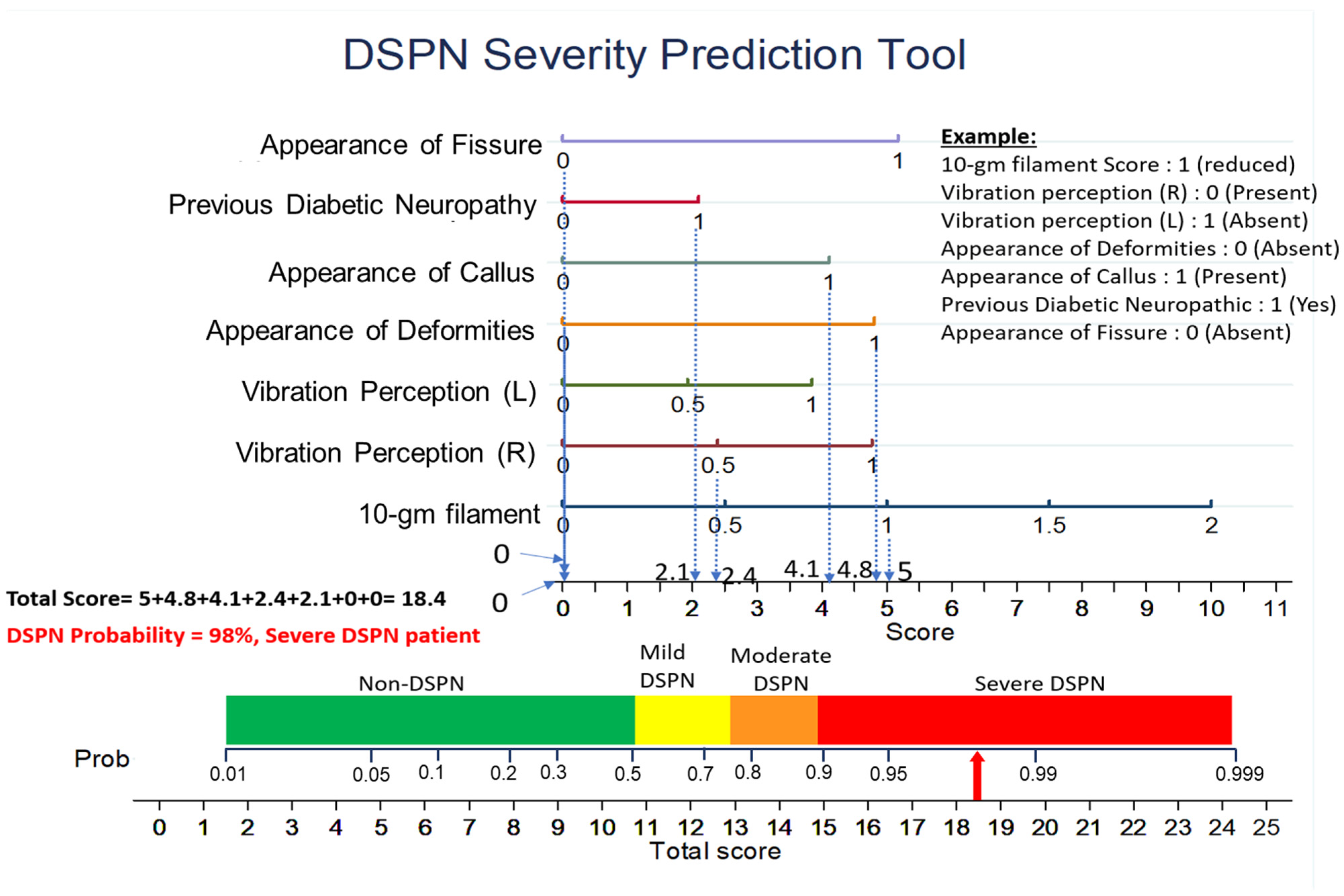
3.3. Development and Evaluation of a Nomogram to Predict DSPN


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Group | Absent | Mild | Moderate | Severe | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MNSI Severity score | 0 | 1 | 6.2 | 10.5 | 10.6 | 11.4 | 11.8 | 12.3 | 12.7 | 12.8 | 13.3 | 14 | 15 | 15.1 | 16.5 | 19 | >28 |
| DSPN Severity probability | 0.5 | 1 | 10 | 49 | 50 | 60 | 65 | 70 | 74 | 75 | 80 | 85 | 90 | 91 | 95 | 99 | 99.99 |

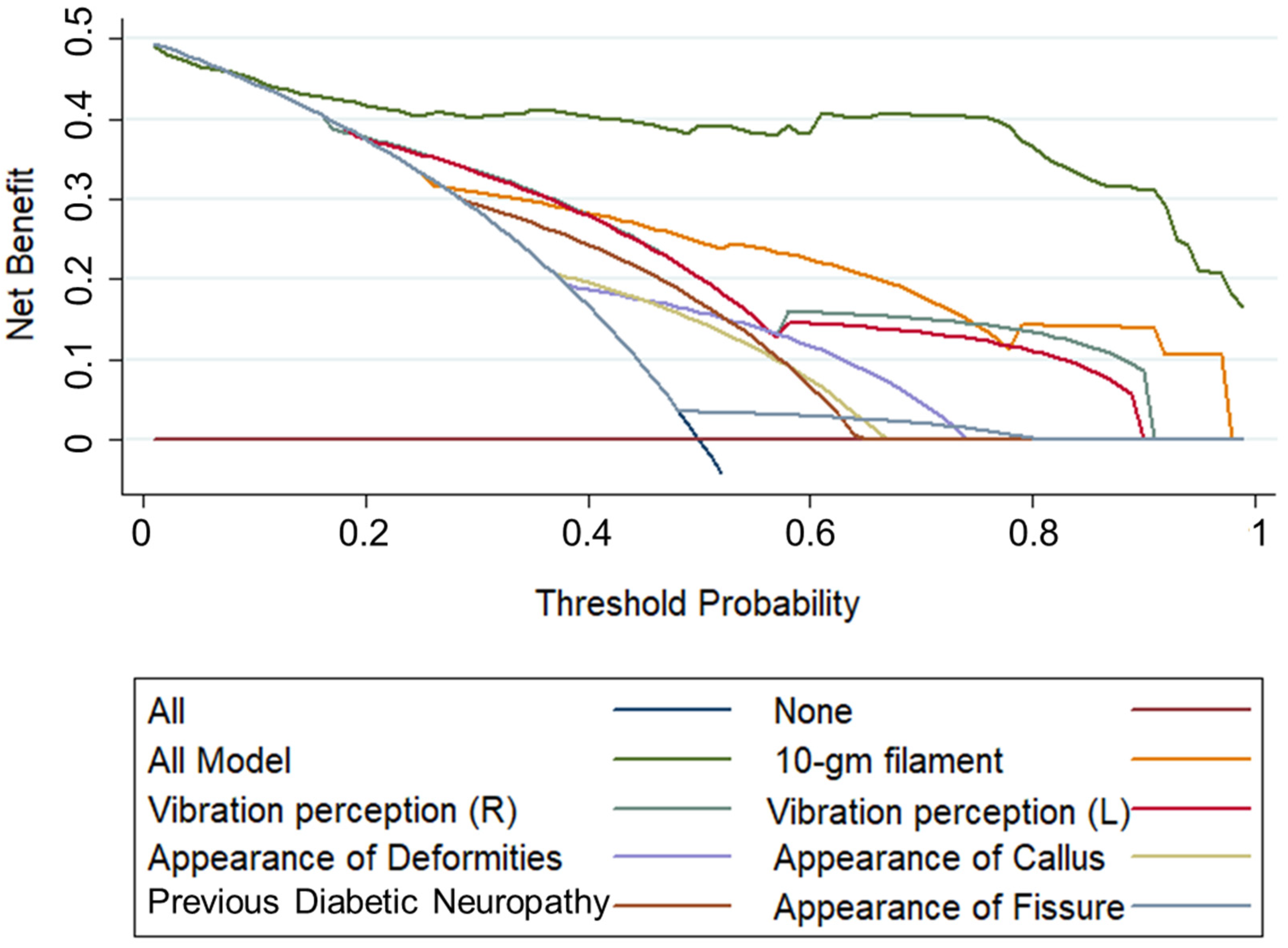
3.4. Evaluation of Performance of the Nomogram Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pop-Busui, R.; Boulton, A.J.M.; Feldman, E.L.; Bril, V.; Freeman, R.; Malik, R.A.; Sosenko, J.M.; Ziegler, D. Diabetic Neuropathy: A Position Statement by the American Diabetes Association. Diabetes Care 2017, 40, 136–154. [Google Scholar] [CrossRef] [Green Version]
- Malik, R.A. Which Test for Diagnosing Early Human Diabetic Neuropathy? Diabetes 2014, 63, 2206–2208. [Google Scholar] [CrossRef] [Green Version]
- Malik, R.A.; Williamson, S.; Abbott, C.; Carrington, A.L.; Iqbal, J.; Schady, W.; Boulton, A.J.M. Effect of Angiotensin-Converting-Enzyme (ACE) Inhibitor Trandolapril on Human Diabetic Neuropathy: Randomised Double-Blind Controlled Trial. Lancet 1998, 352, 1978–1981. [Google Scholar] [CrossRef] [PubMed]
- Malik, R.A.; Tesfaye, S.; Ziegler, D. Medical Strategies to Reduce Amputation in Patients with Type 2 Diabetes. Diabet. Med. 2013, 30, 893–900. [Google Scholar] [CrossRef]
- Haque, F.; Reaz, M.B.I.; Ali, S.H.; Arsad, N.; Enamul, M.; Chowdhury, H. Performance Analysis of Noninvasive Electrophysiological Methods for the Assessment of Diabetic Sensorimotor Polyneuropathy in Clinical Research: A Systematic Review and Meta-Analysis with Trial Sequential Analysis. Sci. Rep. 2020, 10, 21770. [Google Scholar] [CrossRef]
- Tesfaye, S.; Boulton, A.J.M.; Dyck, P.J.; Freeman, R.; Horowitz, M.; Kempler, P.; Lauria, G.; Malik, R.A.; Spallone, V.; Vinik, A.; et al. Diabetic Neuropathies: Update on Definitions, Diagnostic Criteria, Estimation of Severity, and Treatments. Diabetes Care 2010, 33, 2285–2293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taksandea, B.; Ansaria, S.; Jaikishana, A.; Karwasara, V. The Diagnostic Sensitivity, Specificity and Reproducibility of the Clinical Physical Examination Signs in Patients of Diabetes Mellitus for Making Diagnosis of Peripheral Neuropathy. J. Endocrinol. Metab. 2011, 1, 21–26. [Google Scholar] [CrossRef] [Green Version]
- Perkins, B.; Bril, V. Electrophysiologic Testing in Diabetic Neuropathy, 1st ed.; Elsevier B.V.: Amsterdam, The Netherlands, 2014; Volume 126. [Google Scholar]
- Ahmed, A.; Bril, V.; Orszag, A.; Paulson, J.; Yeung, E.; Ngo, M.; Orlov, S.; Perkins, B.A. Detection of Diabetic Sensorimotor Polyneuropathy by Corneal Confocal Microscopy in Type 1 Diabetes: A Concurrent Validity Study. Diabetes Care 2012, 35, 821–828. [Google Scholar] [CrossRef] [Green Version]
- Sacco, I.C.; Akashi, P.M.; Hennig, E.M. A Comparison of Lower Limb EMG and Ground Reaction Forces between Barefoot and Shod Gait in Participants with Diabetic Neuropathic and Healthy Controls. BMC Musculoskelet. Disord. 2010, 11, 24. [Google Scholar] [CrossRef]
- Won, J.C.; Park, T.S. Recent Advances in Diagnostic Strategies for Diabetic Peripheral Neuropathy. Endocrinol. Metab. 2016, 31, 230–238. [Google Scholar] [CrossRef]
- Atre, J.; Ganvir, S. Screening Instrument for Clinical Diagnosis of Peripheral Neuropathy in Diabetes—A Review. Indian J. Physiother. Occup. Ther.—Int. J. 2019, 13, 46. [Google Scholar] [CrossRef]
- Feldman, E.L.; Stevens, M.J.; Thomas, P.K.; Brown, M.B.; Canal, N.; Greene, D.A. A Practical Two-Step Quantitative Clinical and Electrophysiological Assessment for the Diagnosis and Staging of Diabetic Neuropathy. Diabetes Care 1994, 17, 1281–1289. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.L.; Albers, J.; Herman, W.H.; Cleary, P.; Waberski, B.; Greene, D.A.; Stevens, M.J.; Feldman, E.L. Neuropathy among the Diabetes Control and Complications Trial Cohort 8 Years after Trial Completion. Diabetes Care 2006, 29, 340–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qureshi, M.S.; Iqbal, M.; Zahoor, S.; Ali, J.; Javed, M.U. Ambulatory Screening of Diabetic Neuropathy and Predictors of Its Severity in Outpatient Settings. J. Endocrinol. Investig. 2017, 40, 425–430. [Google Scholar] [CrossRef]
- Andersen, S.T.; Witte, D.R.; Dalsgaard, E.M.; Andersen, H.; Nawroth, P.; Fleming, T.; Jensen, T.S.M.; Finnerup, N.B.; Jensen, T.S.M.; Lauritzen, T.; et al. Risk Factors for Incident Diabetic Polyneuropathy in a Cohort with Screen-Detected Type 2 Diabetes Followed for 13 Years: Addition-Denmark. Diabetes Care 2018, 41, 1068–1075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christensen, D.H.; Knudsen, S.T.; Gylfadottir, S.S.; Christensen, L.B.; Nielsen, J.S.; Beck-Nielsen, H.; Sørensen, H.T.; Andersen, H.; Callaghan, B.C.; Feldman, E.L.; et al. Metabolic Factors, Lifestyle Habits, and Possible Polyneuropathy in Early Type 2 Diabetes: A Nationwide Study of 5,249 Patients in the Danish Centre for Strategic Research in Type 2 Diabetes (Dd2) Cohort. Diabetes Care 2020, 43, 1266–1275. [Google Scholar] [CrossRef] [PubMed]
- Moghtaderi, A.; Bakhshipour, A.; Rashidi, H. Validation of Michigan Neuropathy Screening Instrument for Diabetic Peripheral Neuropathy. Clin. Neurol. Neurosurg. 2006, 108, 477–481. [Google Scholar] [CrossRef]
- Herman, W.H.; Pop-Busui, R.; Braffett, B.H.; Martin, C.L.; Cleary, P.A.; Albers, J.W.; Feldman, E.L. Use of the Michigan Neuropathy Screening Instrument as a Measure of Distal Symmetrical Peripheral Neuropathy in Type1 Diabetes: Results from the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications. Diabet. Med. 2012, 29, 937–944. [Google Scholar] [CrossRef] [Green Version]
- Pabellano-Tiongson, M.L.G.P.; Javelosa, G.F.J.; Tan, A.D.A. The Validity of the Filipino Version of the Michigan Neuropathy Screening Instrument as a Measure of Distal Symmetric Peripheral Neuropathy among Diabetic Patients at the Uermmmci Outpatient Deparment. Asian J. Res. Rep. Neurol. 2018, 58, S74. [Google Scholar]
- Park, J.H.; Kim, D.S. The Necessity of the Simple Tests for Diabetic Peripheral Neuropathy in Type 2 Diabetes Mellitus Patients without Neuropathic Symptoms in Clinical Practice. Diabetes Metab. J. 2018, 42, 442–446. [Google Scholar] [CrossRef]
- Haque, F.; Reaz, M.B.I.; Chowdhury, M.E.H.; Ezeddin, M.; Kiranyaz, S.; Alhatou, M.; Ali, S.H.M.; Bakar, A.A.A.; Srivastava, G. Machine Learning-Based Diabetic Neuropathy and Previous Foot Ulceration Patients Detection Using Electromyography and Ground Reaction Forces during Gait. Sensors 2022, 22, 3507. [Google Scholar] [CrossRef]
- Haque, F.; Reaz, M.B.I.; Chowdhury, M.E.H.; Kiranyaz, S.; Ali, S.H.M.; Alhatou, M.; Habib, R.; Bakar, A.A.A.; Arsad, N.; Srivastava, G. Performance Analysis of Conventional Machine Learning Algorithms for Diabetic Sensorimotor Polyneuropathy Severity Classification Using Nerve Conduction Studies. Comput. Intell. Neurosci. 2022, 2022, 9690940. [Google Scholar] [CrossRef] [PubMed]
- Haque, F.; Reaz, M.B.I.; Chowdhury, M.E.H.; Srivastava, G.; Ali, S.H.M.; Bakar, A.A.A.; Bhuiyan, M.A.S. Performance Analysis of Conventional Machine Learning Algorithms for Diabetic Sensorimotor Polyneuropathy Severity Classification. Diagnostics 2021, 11, 801. [Google Scholar] [CrossRef] [PubMed]
- Thorsen-Meyer, H.C.; Nielsen, A.B.; Nielsen, A.P.; Kaas-Hansen, B.S.; Toft, P.; Schierbeck, J.; Strøm, T.; Chmura, P.J.; Heimann, M.; Dybdahl, L.; et al. Dynamic and Explainable Machine Learning Prediction of Mortality in Patients in the Intensive Care Unit: A Retrospective Study of High-Frequency Data in Electronic Patient Records. Lancet Digit. Health 2020, 2, e179–e191. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Zhang, X.; Ran, X.; Xu, Z.; Ji, L. Simple-to-Use Nomogram for Evaluating the Incident Risk of Moderate-to-Severe LEAD in Adults with Type 2 Diabetes: A Cross-Sectional Study in a Chinese Population. Sci. Rep. 2020, 10, 3182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picon, A.A.P.; Ortega, N.R.S.N.; Watari, R.; Sartor, C.; Sacco, I.C.N.I. Classification of the Severity of Diabetic Neuropathy: A New Approach Taking Uncertainties into Account Using Fuzzy Logic. Clinics 2012, 67, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Watari, R.; Sartor, C.D.; Picon, A.P.; Butugan, M.K.; Amorim, C.F.; Ortega, N.R.S.; Sacco, I.C.N. Effect of Diabetic Neuropathy Severity Classified by a Fuzzy Model in Muscle Dynamics during Gait. J. NeuroEng. Rehabil. 2014, 11, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kazemi, M.; Moghimbeigi, A.; Kiani, J.; Mahjub, H.; Faradmal, J. Diabetic Peripheral Neuropathy Class Prediction by Multicategory Support Vector Machine Model: A Cross-Sectional Study. Epidemiol. Health 2016, 38, e2016011. [Google Scholar] [CrossRef]
- Haque, F.; Reaz, M.B.I.; Chowdhury, M.E.H.; Hashim, F.H.; Arsad, N.; Ali, S.H.M. Diabetic Sensorimotor Polyneuropathy Severity Classification Using Adaptive Neuro-Fuzzy Inference System. IEEE Access 2021, 9, 7618–7631. [Google Scholar] [CrossRef]
- Reddy, S.; Mahesh, G.; Preethi, N. Evolving A Neural Network to Predict Diabetic Neuropathy. ICST Trans. Scalable Inf. Syst. 2018, 8, 166765. [Google Scholar] [CrossRef]
- Chen, S.; Kang, L.; Lu, Y.; Wang, N.; Lu, Y.; Lo, B.; Yang, G.Z. Discriminative Information Added by Wearable Sensors for Early Screening—A Case Study on Diabetic Peripheral Neuropathy. In Proceedings of the 2019 IEEE 16th International Conference on Wearable and Implantable Body Sensor Networks, BSN 2019—Proceedings, Chicago, IL, USA, 19–22 May 2019; pp. 1–4. [Google Scholar]
- Epidemiology of Diabetes Interventions and Complications (EDIC) Research Group Epidemiology of Diabetes Interventions and Complications (EDIC): Design, Implementation, and Preliminary Results of a Long-Term Follow-up of the Diabetes Control and Complications Trial Cohort. Diabetes Care 1999, 22, 99–111. [CrossRef]
- Pop-Busui, R.; Herman, W.H.; Feldman, E.L.; Low, P.A.; Martin, C.L.; Cleary, P.A.; Waberski, B.H.; Lachin, J.M.; Albers, J.W. DCCT and EDIC Studies in Type 1 Diabetes: Lessons for Diabetic Neuropathy Regarding Metabolic Memory and Natural History. Curr. Diabetes Rep. 2010, 10, 276–282. [Google Scholar] [CrossRef] [Green Version]
- Martin, C.L.; Albers, J.W.; Pop-Busui, R. Neuropathy and Related Findings in the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Study. Diabetes Care 2014, 37, 31–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wulff, J.N.; Ejlskov, L. Multiple Imputation by Chained Equations in Praxis: Guidelines and Review. Electron. J. Bus. Res. Methods 2017, 15, 41–56. [Google Scholar]
- Austin, P.C.; White, I.R.; Lee, D.S.; van Buuren, S. Missing Data in Clinical Research: A Tutorial on Multiple Imputation. Can. J. Cardiol. 2020, 37, 1322–1331. [Google Scholar] [CrossRef]
- Hegde, H.; Shimpi, N.; Panny, A.; Glurich, I.; Christie, P.; Acharya, A. MICE vs PPCA: Missing Data Imputation in Healthcare. Inform. Med. Unlocked 2019, 17, 100275. [Google Scholar] [CrossRef]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Chen, T.; Guestrin, C. XGBoost: A Scalable Tree Boosting System. In Proceedings of the KDD ’16, San Francisco, CA, USA, 13–17 August 2016; Volume 42, pp. 785–794. [Google Scholar]
- Geurts, P.; Ernst, D.; Wehenkel, L. Extremely Randomized Trees. Mach. Learn. 2006, 63, 3–42. [Google Scholar] [CrossRef] [Green Version]
- Le Cessie, S.; van Houwelingen, J.C. Ridge Estimators in Logistic Regression. Appl. Stat. 1992, 41, 191–201. [Google Scholar] [CrossRef]
- Tolles, J.; Meurer, W.J. Logistic Regression Relating Patient Characteristics to Outcomes JAMA Guide to Statistics and Methods. JAMA 2016, 2, 533–534. [Google Scholar] [CrossRef]
- Zlotnik, A.; Abraira, V. A General-Purpose Nomogram Generator for Predictive Logistic Regression Models. Stata J. 2015, 15, 537–546. [Google Scholar] [CrossRef] [Green Version]
- Pop-Busui, R.; Evans, G.W.; Gerstein, H.C.; Fonseca, V.; Fleg, J.L.; Hoogwerf, B.J.; Genuth, S.; Grimm, R.H.; Corson, M.A.; Prineas, R.; et al. Effects of Cardiac Autonomic Dysfunction on Mortality Risk in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) Trial. Diabetes Care 2010, 33, 1578–1584. [Google Scholar] [CrossRef] [PubMed]




| N: 1341 M: 658 (52.39%) F: 598 (47.61%) | Mean | Std. Error of Mean | Minimum | Maximum |
|---|---|---|---|---|
| Age (years) | 35.98 ± 6.95 | 0.19 | 20.16 | 50.99 |
| HbA1C (%) | 8.23 ± 1.39 | 0.04 | 0.00 | 14.00 |
| BMI (kg/m2) | 26.24 ± 4.16 | 0.11 | 0.00 | 49.82 |
| Diabetes duration (years) | 14.55 ± 4.91 | 0.13 | 0.00 | 27.00 |
| HDL Cholesterol (mg/dL) | 52.69 ± 16.05 | 0.44 | 0.00 | 121.00 |
| LDL Cholesterol (mg/dL) | 110.75 ± 36.33 | 0.99 | 0.00 | 280.00 |
| Sensitivity (%) | Specificity (%) | Accuracy (%) | Precision (%) | F1 Score (%) | Non-DSPN | DSPN | |||
|---|---|---|---|---|---|---|---|---|---|
| TN | FP | FN | TP | ||||||
| Top 1 Feature | 72 ± 0.02 | 80 ± 0.04 | 76 ± 0.02 | 78 ± 0.03 | 75 ± 0.02 | 1732 | 445 | 619 | 1558 |
| Top 2 Features | 73 ± 0.05 | 85 ± 0.05 | 79 ± 0.02 | 83 ± 0.04 | 77 ± 0.02 | 1845 | 332 | 591 | 1586 |
| Top 3 Features | 75 ± 0.03 | 86 ± 0.04 | 80 ± 0.01 | 84 ± 0.03 | 79 ± 0.01 | 1869 | 308 | 548 | 1629 |
| Top 4 Features | 77 ± 0.04 | 86 ± 0.02 | 82 ± 0.03 | 85 ± 0.03 | 81 ± 0.03 | 1877 | 300 | 496 | 1681 |
| Top 5 Features | 86 ± 0.02 | 92 ± 0.03 | 89 ± 0.02 | 91 ± 0.03 | 88 ± 0.02 | 1994 | 183 | 315 | 1862 |
| Top 6 Features | 88 ± 0.03 | 86 ± 0.04 | 87 ± 0.03 | 87 ± 0.03 | 87 ± 0.03 | 1879 | 298 | 260 | 1917 |
| Top 7 Features | 90 ± 0.02 | 90 ± 0.03 | 90 ± 0.02 | 90 ± 0.02 | 90 ± 0.02 | 1954 | 223 | 220 | 1957 |
| Top 8 Features | 89 ± 0.02 | 92 ± 0.04 | 90 ± 0.02 | 91 ± 0.04 | 90 ± 0.02 | 1995 | 182 | 238 | 1939 |
| Top 9 Features | 89 ± 0.03 | 90 ± 0.07 | 89 ± 0.03 | 90 ± 0.06 | 89 ± 0.03 | 1949 | 228 | 233 | 1944 |
| Top 10 Features | 92 ± 0.01 | 93 ± 0.05 | 92 ± 0.02 | 93 ± 0.05 | 92 ± 0.02 | 2019 | 158 | 185 | 1992 |
| Top 11 Features | 91 ± 0.01 | 92 ± 0.05 | 92 ± 0.03 | 92 ± 0.05 | 91 ± 0.03 | 2001 | 176 | 194 | 1983 |
| Top 12 Features | 91 ± 0.02 | 92 ± 0.05 | 92 ± 0.03 | 92 ± 0.05 | 91 ± 0.03 | 2003 | 174 | 195 | 1982 |
| Top 13 Features | 91 ± 0.02 | 92 ± 0.04 | 92 ± 0.02 | 92 ± 0.03 | 91 ± 0.02 | 2012 | 165 | 204 | 1973 |
| Top 14 Features | 90 ± 0.02 | 92 ± 0.05 | 91 ± 0.03 | 92 ± 0.05 | 91 ± 0.02 | 2007 | 170 | 210 | 1967 |
| Top 15 Features | 90 ± 0.02 | 92 ± 0.06 | 91 ± 0.04 | 92 ± 0.06 | 91 ± 0.04 | 2008 | 169 | 209 | 1968 |
| Outcome | Coef. | Std. Err. | z | P > z | [95% Conf. Interval] | |
|---|---|---|---|---|---|---|
| 10-gm filament | 2.514831 | 0.137814 | 18.25 | 0.00 | 2.24472 | 2.784941 |
| Vibration perception (R) | 2.399316 | 0.249416 | 9.62 | 0.00 | 1.91047 | 2.888162 |
| Vibration perception (L) | 1.932473 | 0.247976 | 7.79 | 0.00 | 1.446448 | 2.418498 |
| Appearance of Deformities | 2.413763 | 0.142204 | 16.97 | 0.00 | 2.135049 | 2.692477 |
| Appearance of Callus | 2.064003 | 0.13319 | 15.5 | 0.00 | 1.802955 | 2.325051 |
| Previous Diabetic Neuropathy | 1.053302 | 0.125036 | 8.42 | 0.00 | 0.808235 | 1.298369 |
| Appearance of Fissure | 2.602008 | 0.272765 | 9.54 | 0.00 | 2.067398 | 3.136619 |
| _cons | −5.31948 | 0.207402 | −25.65 | 0.00 | −5.72598 | −4.91298 |
| Outcome | Coef. | Std. Err. | z | P > z | [95% Conf. Interval] | |
|---|---|---|---|---|---|---|
| 10-gm filament | 3.084504 | 0.1696 | 18.19 | 0.00 | 2.752094 | 3.416913 |
| Vibration perception (R) | 3.003988 | 0.285598 | 10.52 | 0.00 | 2.444225 | 3.56375 |
| Vibration perception (L) | 2.326558 | 0.282243 | 8.24 | 0.00 | 1.773372 | 2.879744 |
| Appearance of Deformities | 3.202711 | 0.176598 | 18.14 | 0.00 | 2.856585 | 3.548837 |
| Appearance of Callus | 2.886776 | 0.169801 | 17 | 0.00 | 2.553974 | 3.219579 |
| Previous Diabetic Neuropathy | 0.634693 | 0.140511 | 4.52 | 0.00 | 0.359297 | 0.910089 |
| Appearance of Fissure | 3.52151 | 0.309166 | 11.39 | 0.00 | 2.915556 | 4.127464 |
| Numb Leg | 0.941649 | 0.149556 | 6.3 | 0.00 | 0.648525 | 1.234772 |
| Burning Leg | 1.235312 | 0.153058 | 8.07 | 0.00 | 0.935324 | 1.535301 |
| Bed Cover Touch | 2.655393 | 0.244644 | 10.85 | 0.00 | 2.175899 | 3.134887 |
| _cons | −7.49854 | 0.306272 | −24.48 | 0.00 | −8.09883 | −6.89826 |
| Prediction Model | Test Sets | Sensitivity (%) | Specificity (%) | Accuracy (%) | Precision (%) | F1 Score (%) | Confusion Matrix | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Non-DSPN | DSPN | |||||||||
| TN | FP | FN | TP | |||||||
| Top 7 Variable model | EDIC Test Set | 91 | 89 | 90 | 86 | 88 | 583 | 71 | 44 | 429 |
| Independent Test Set | 91 | 92 | 91 | 89 | 90 | 54 | 5 | 4 | 39 | |
| Top 10 Variable model | EDIC Test Set | 91 | 92 | 91 | 89 | 90 | 598 | 56 | 42 | 431 |
| Independent Test Set | 93 | 81 | 86 | 78 | 85 | 48 | 11 | 3 | 40 | |
| DSPN Severity Class | Outcome | Total | |
|---|---|---|---|
| Non-DSPN | DSPN | ||
| Absent | 1361 (89.2%) | 165(10.8%) | 1526 (100%) |
| Mild | 162 (55.5%) | 130 (44.5%) | 292 (100%) |
| Moderate | 0 (0%) | 282 (100%) | 282 (100%) |
| Severe | 0 (0%) | 947 (100%) | 947 (100%) |
| Total | 1523 (50%) | 1524 (50%) | 3047 (100%) |
| DSPN Severity Class | Outcome | Total | |
|---|---|---|---|
| Non-DSPN | DSPN | ||
| Absent | 583 (91.8%) | 52 (8.2%) | 635 |
| Mild | 71(48.97%) | 74 (51.03%) | 145 |
| Moderate | 0 (0%) | 120 (100%) | 120 |
| Severe | 0 (0%) | 407 (100%) | 407 |
| Total | 654 (50%) | 653 (50%) | 1307 |
| DSPN Severity Class | Outcome | Total | |
|---|---|---|---|
| Non-DSPN | DSPN | ||
| Absent | 54 (93.1%) | 4 (6.9%) | 58 (100%) |
| Mild | 5 (50%) | 5 (50%) | 10 (100%) |
| Moderate | 0 (0%) | 9 (100%) | 9 (100%) |
| Severe | 0 (0%) | 25 (100%) | 25 (100%) |
| Total | 59 (57.8%) | 43 (42.2%) | 102 (100%) |
| DSPN Severity Grading by Our Model | DSPN Severity Grading by Watari et al., 2014 [28] | Total | |||
|---|---|---|---|---|---|
| Absent | Mild | Moderate | Severe | ||
| Absent | 28 | 18 | 12 | 0 | 59 |
| Mild | 0 | 2 | 5 | 3 | 10 |
| Moderate | 1 | 3 | 3 | 2 | 9 |
| Severe | 0 | 2 | 7 | 16 | 25 |
| Total | 29 | 25 | 27 | 21 | 102 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haque, F.; Reaz, M.B.I.; Chowdhury, M.E.H.; Shapiai, M.I.b.; Malik, R.A.; Alhatou, M.; Kobashi, S.; Ara, I.; Ali, S.H.M.; Bakar, A.A.A.; et al. A Machine Learning-Based Severity Prediction Tool for the Michigan Neuropathy Screening Instrument. Diagnostics 2023, 13, 264. https://doi.org/10.3390/diagnostics13020264
Haque F, Reaz MBI, Chowdhury MEH, Shapiai MIb, Malik RA, Alhatou M, Kobashi S, Ara I, Ali SHM, Bakar AAA, et al. A Machine Learning-Based Severity Prediction Tool for the Michigan Neuropathy Screening Instrument. Diagnostics. 2023; 13(2):264. https://doi.org/10.3390/diagnostics13020264
Chicago/Turabian StyleHaque, Fahmida, Mamun B. I. Reaz, Muhammad E. H. Chowdhury, Mohd Ibrahim bin Shapiai, Rayaz A. Malik, Mohammed Alhatou, Syoji Kobashi, Iffat Ara, Sawal H. M. Ali, Ahmad A. A. Bakar, and et al. 2023. "A Machine Learning-Based Severity Prediction Tool for the Michigan Neuropathy Screening Instrument" Diagnostics 13, no. 2: 264. https://doi.org/10.3390/diagnostics13020264