
Electrical Stimulation for Preventing Skin Injuries in Denervated Gluteal Muscles—Promising Perspectives from a Case Series and Narrative Review


Abstract
:1. Introduction
2. Materials and Methods
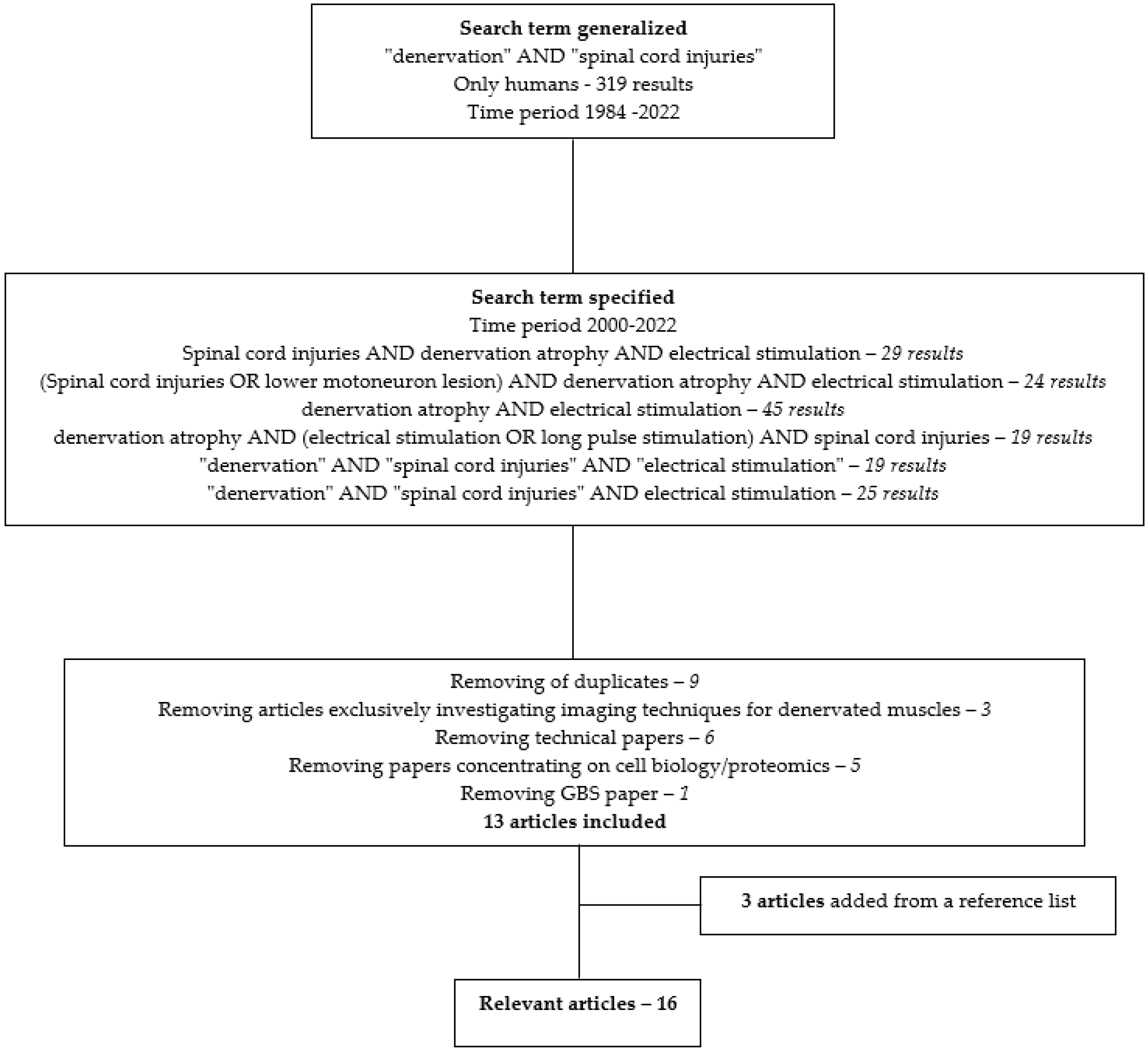
2.1. Narrative Literature Search
2.2. Case Series
2.2.1. Participant Eligibility
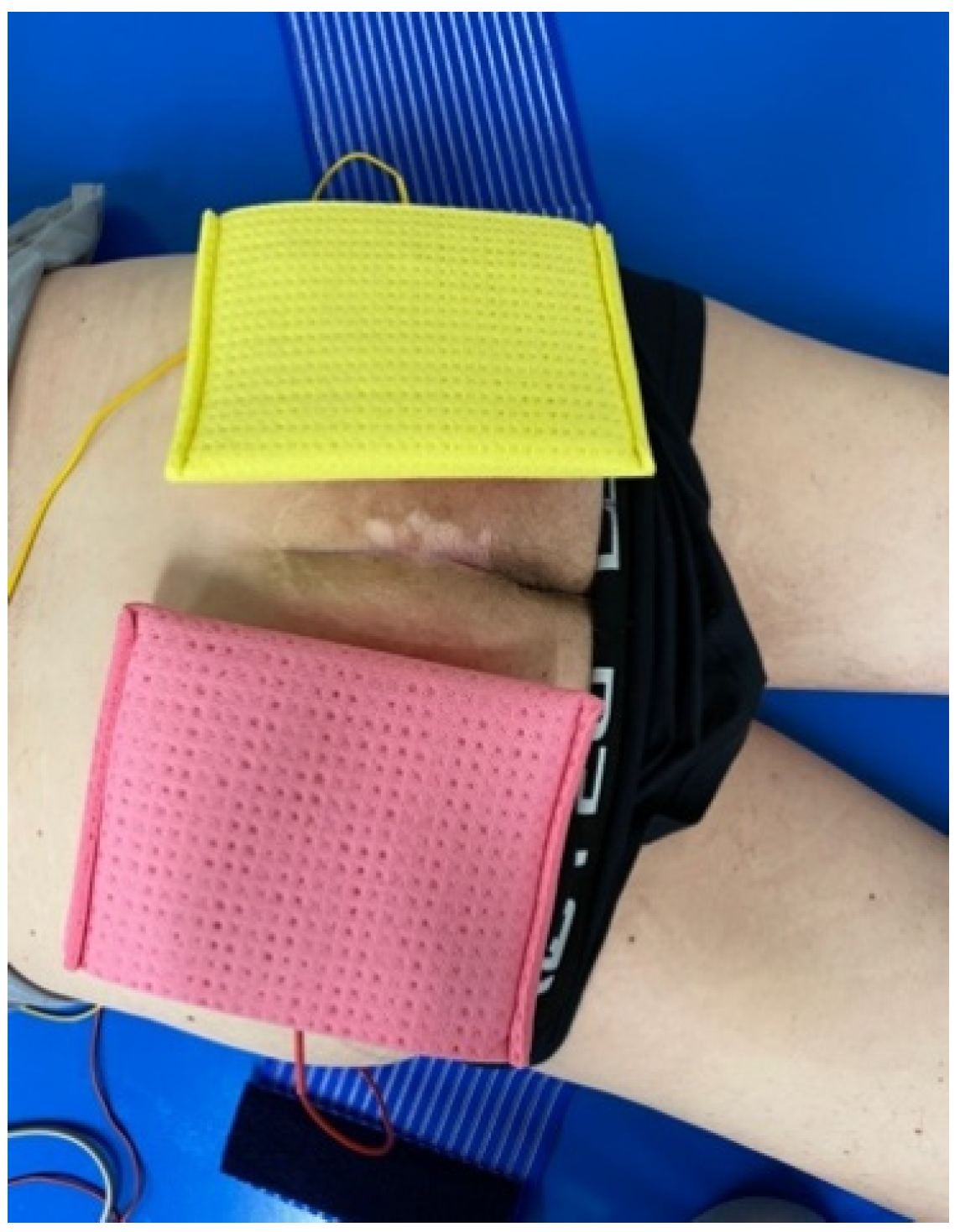
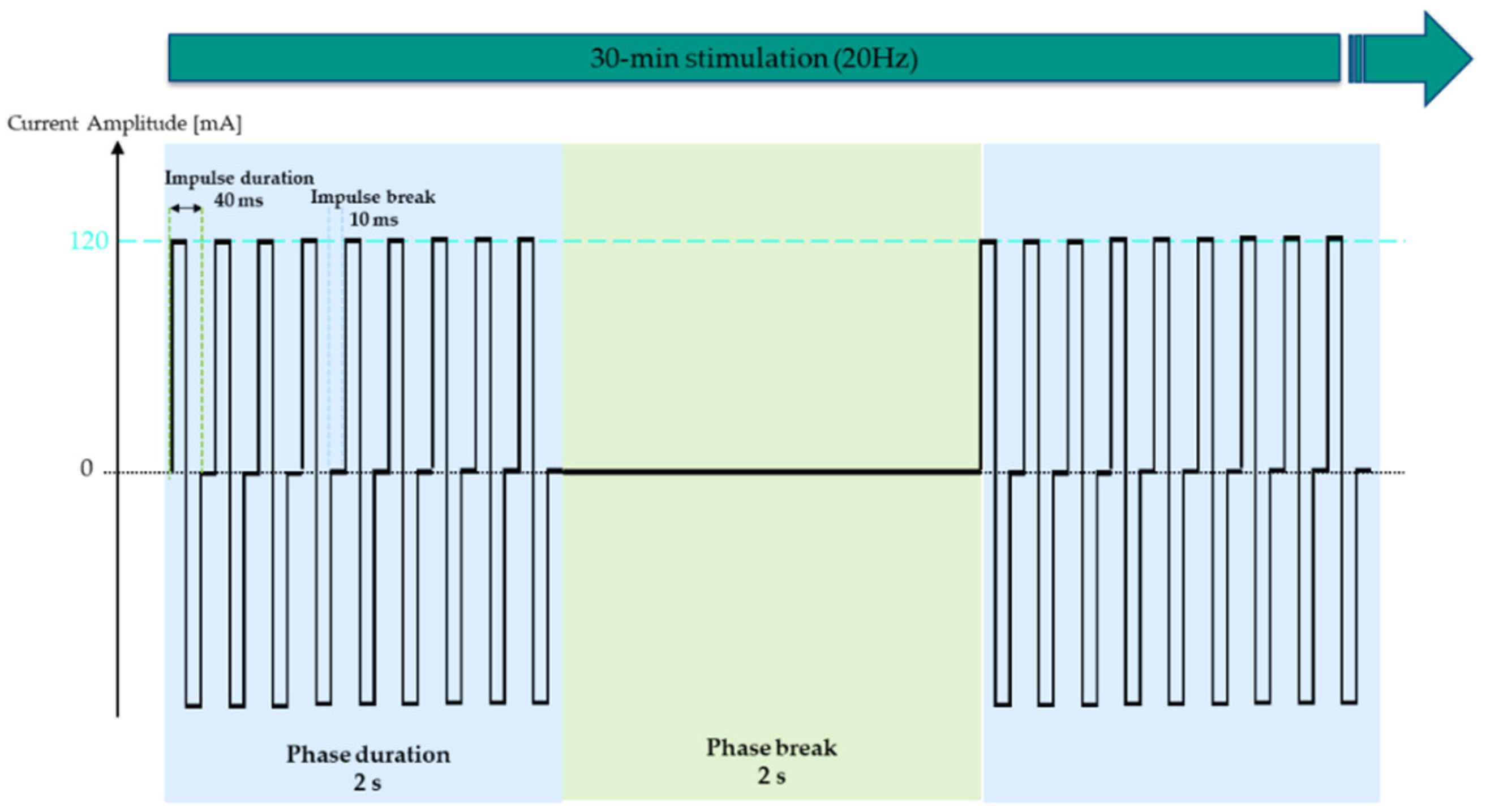
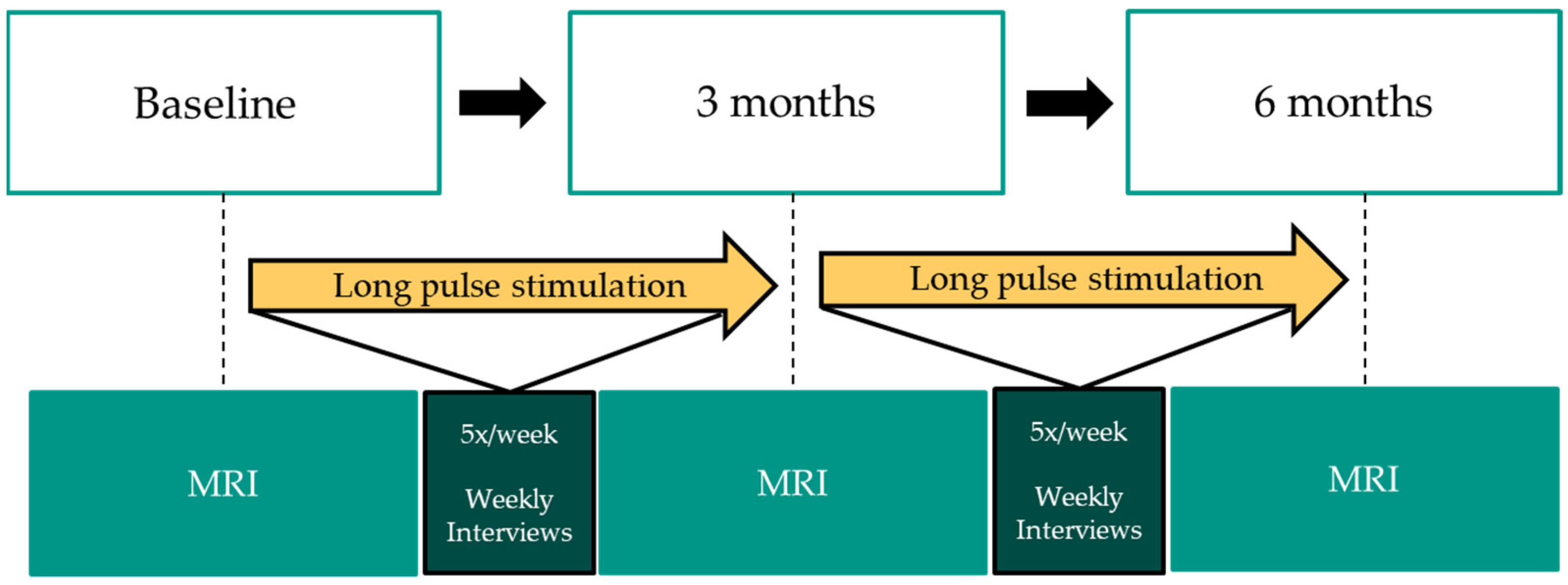
2.2.2. Intervention
2.2.3. Outcomes Measures
2.2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Limitations
4.2. Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Author Title | Year | Type | Population | Intervention | Methodology | Main Outcomes & Conclusion |
| Kern et al. [15] Functional electrical stimulation of long-term denervated muscles in humans: clinical observations and laboratory findings | 2002 | Article | Traumatic conus cauda lesion (>1.9 years) n = 14 | Progressive training program: (1) Single twitches with 120–150 ms pulses (f = 2 Hz) (2) With ↑muscle excitability after 3–6 months: 35–50 ms (f = 16–25 Hz) (3) Knee extensions (4) Strength endurance training (5) Standing exercise (6) Stepping |
|
High current intensities are needed for FES training of denervated muscles to improve structure and function |
| Kern et al. [25] Denervated muscles in humans: limitations and problems of currently used functional electrical stimulation protocols | 2002 | Review + EU RISE protocol | Complete conus cauda lesions | Start stimulation with single twitches using biphasic pulses of 120–150 ms Proceed with tetanic contractions using 30–50 ms (f = 16–25 Hz) up until 250 mA; 2 s on and 2–4 s off Later paired with knee extensions & ankle weights |
|
Standing training can be initiated after conclusion of 1 yr FES therapy |
| Mödlin et al. [2] Electrical stimulation of denervated muscles: first results of a clinical study | 2005 | Article | SCI (T11-L1) with denervated m. quadriceps (>6–12 months) n = 40 | 1 year of ES max 160 V Progressive protocol: (1) 120–150 ms pulses (f = 2 Hz); 5 s bursts and 2 s pauses; 15 min, increasing up to 20–30 min (2) After some months: 70 ms pulses (f = 5 Hz) (3) 40 ms pulses and 10 ms pauses (f = 20 Hz); 2 s bursts |
|
|
| Salmons et al. [34] Functional electrical stimulation of denervated muscles: basic issues | 2005 | Narrative review | N/A | N/A |
|
|
| Carraro et al. [26] Muscle fiber regeneration in human permanent lower motoneuron denervation: relevance to safety and effectiveness of FES-training, which induces muscle recovery in SCI subjects | 2005 | Article | Subjects with denervated degenerated muscle | No FES vs. FES | Needle biopsies |
|
| Kern et al. [13] Recovery of long-term denervated human muscles induced by electrical stimulation | 2005 | Case study | Traumatic cauda equina lesion at T12 n = 1, male, age: 47 | FES training onset after 18 months Biphasic rectangular current:
|
|
Severe atrophy and replacement of muscle tissue by fat was reversed by FES |
| Kern et al. [17] Muscle biopsies show that FES of denervated muscles reverses human muscle degeneration from permanent spinal motoneuron lesion | 2005 | Article | Traumatic conus cauda lesions n = 9 | 4-phase training protocol: biphasic rectangular current (1) Early twitch stimulation: 150–200 ms (f = 2 Hz); 4 s on-2 s off, 1–2 min rest (2) Late twitch stimulation: 80–100 ms for 3 months (3) Burst stimulation: 40 ms impulses - 10 ms pauses (f = 20 Hz) with 2 s bursts, 2×/day, 5×/week (4) Force/endurance stimulation with ankle weights |
|
|
| Hofer et al. [35] In vivo assessment of conduction velocity and refractory period of denervated muscle fibers | 2005 | Article | SCI with denervation of the thigh muscles n = 4 | 2 subjects included in the RISE training program (6 and 15 months) 2 untrained SCI subjects |
|
|
| Kern et al. [19] One year of home-based daily FES in complete lower motor neuron paraplegia: recovery of tetanic contractility drives the structural improvements of denervated muscles | 2010 | Comparative study | Chronic SCI n = 25 | 4-phase stimulation protocol conducted over 1 year on the quadriceps muscle against resistance | pre-post 1 yr FES:
|
|
| Kern et al. [20] Home-based functional electrical stimulation rescues permanently denervated muscles in paraplegic patients with complete lower motor neuron lesion | 2010 | Longitudinal prospective study | Complete SCI n = 25 | Biphasic stimulation 120–150 ms, 60–75 ms per phase, 250 mA |
|
|
| Pieber et al. [36] Optimizing stimulation parameters in functional electrical stimulation of denervated muscles: a cross-sectional study | 2015 | Cross-sectional study | Denervated EDC or TA n = 24/group | ES using triangular pulses with different electrode placements (anode&cathode) and different pulse durations |
|
|
| Kern et al. [16] Atrophy, ultra-structural disorders, severe atrophy and degeneration of denervated human muscl in SCI and ageing. Implications for their recovery by functional electrical stimulation, updated 2017 | 2017 | Review | N/A | / | Biopsies of m. quadriceps | Denervation consequences:
Training:
|
| Ravara et al. [37] Dermal papillae flattening of thigh skin in conus cauda syndrome | 2018 | Article | SCI n = 18 | N/A |
|
|
| Albertin et al. [21] Two years of functional electrical stimulation by large surface electrodes for denervated muscles improve skin epidermis in SCI | 2018 | Article - preliminary data | SCI n = 3 | 2 years of h-bFES | Skin biopsies analyzed through:
|
|
| Kern et al. [38] To reverse atrophy of human muscles in complete SCI lower motor neuron denervation by home-based functional electrical stimulation | 2018 | Book chapter | N/A | 2 years of h-bFES of m. quadriceps 5×/week |
| In 20 out of 25 patients:
Starting h-bFES even 3 years after denervation allows for recovery of muscle tissue ES with large electrodes on the m. quadriceps is unspecific, eliciting co-contraction of the hamstrings
|
| Bersch & Fridén [28] Electrical stimulation alters muscle morphological properties in denervated upper limb muscles | 2021 | Prospective interventional study | SCI (C3–C7) with denervated ECU and/or IOD1 n = 20 | 12 weeks of ES of IOD1 and/or ECU
|
| Direct muscle stimulation of denervated upper limb muscle increases MT and PA within 12 weeks Early onset of ES in denervated muscles of the upper limbs can preserve muscle contractility and quality for optimal preparation for possible nerve transfers |
References
- Carlson, B.M. The Biology of Long-Term Denervated Skeletal Muscle. Eur. J. Transl. Myol. 2014, 24, 3293. [Google Scholar] [CrossRef]
- Modlin, M.; Forstner, C.; Hofer, C.; Mayr, W.; Richter, W.; Carraro, U.; Protasi, F.; Kern, H. Electrical Stimulation of Denervated Muscles: First Results of a Clinical Study. Artif. Organs 2005, 29, 203–206. [Google Scholar] [CrossRef]
- Invernizzi, M.; de Sire, A.; Fusco, N. Rethinking the clinical management of volumetric muscle loss in patients with spinal cord injury: Synergy among nutritional supplementation, pharmacotherapy, and rehabilitation. Curr. Opin. Pharmacol. 2021, 57, 132–139. [Google Scholar] [CrossRef]
- Scheel-Sailer, A.; Wyss, A.; Boldt, C.; Post, M.W.; Lay, V. Prevalence, Location, Grade of Pressure Ulcers and Association with Specific Patient Characteristics in Adult Spinal Cord Injury Patients during the Hospital Stay: A Prospective Cohort Study. Spinal Cord 2013, 51, 828–833. [Google Scholar] [CrossRef] [Green Version]
- Shiferaw, W.S.; Akalu, T.Y.; Mulugeta, H.; Aynalem, Y.A. The global burden of pressure ulcers among patients with spinal cord injury: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2020, 21, 334. [Google Scholar] [CrossRef]
- Šín, P.; Hokynková, A.; Marie, N.; Andrea, P.; Krč, R.; Podroužek, J. Machine Learning-Based Pressure Ulcer Prediction in Modular Critical Care Data. Diagnostics 2022, 12, 850. [Google Scholar] [CrossRef]
- Bélanger, M.; Stein, R.B.; Wheeler, G.D.; Gordon, T.; Leduc, B. Electrical stimulation: Can it increase muscle strength and reverse osteopenia in spinal cord injured individuals? Arch. Phys. Med. Rehabil. 2000, 81, 1090–1098. [Google Scholar] [CrossRef]
- Chang, K.-V.; Hung, C.-Y.; Chen, W.-S.; Lai, M.-S.; Chien, K.-L.; Han, D.-S. Effectiveness of Bisphosphonate Analogues and Functional Electrical Stimulation on Attenuating Post-Injury Osteoporosis in Spinal Cord Injury Patients—A Systematic Review and Meta-Analysis. PLoS ONE 2013, 8, e81124. [Google Scholar] [CrossRef]
- Fornusek, C.; Gwinn, T.H.; Heard, R. Cardiorespiratory responses during functional electrical stimulation cycling and electrical stimulation isometric exercise. Spinal Cord 2014, 52, 635–639. [Google Scholar] [CrossRef] [Green Version]
- Carraro, U.; Kern, H. Severely Atrophic Human Muscle Fibers With Nuclear Misplacement Survive Many Years of Permanent Denervation. Eur. J. Transl. Myol. 2016, 26, 5894. [Google Scholar] [CrossRef]
- Kern, H.; Carraro, U. Home-Based Functional Electrical Stimulation for Long-Term Denervated Human Muscle: History, Basics, Results and Perspectives of the Vienna Rehabilitation Strategy. Eur. J. Transl. Myol. 2014, 24, 3296. [Google Scholar] [CrossRef]
- Boncompagni, S.; Kern, H.; Rossini, K.; Hofer, C.; Mayr, W.; Carraro, U.; Protasi, F. Structural differentiation of skeletal muscle fibers in the absence of innervation in humans. Proc. Natl. Acad. Sci. USA 2007, 104, 19339–19344. [Google Scholar] [CrossRef] [Green Version]
- Kern, H.; Salmons, S.; Mayr, W.; Rossini, K.; Carraro, U. Recovery of long-term denervated human muscles induced by electrical stimulation. Muscle Nerve 2005, 31, 98–101. [Google Scholar] [CrossRef]
- Carraro, U.; Boncompagni, S.; Gobbo, V.; Rossini, K.; Zampieri, S.; Mosole, S.; Ravara, B.; Nori, A.; Stramare, R.; Ambrosio, F.; et al. Persistent muscle fiber regeneration in long term denervation. Past, present, future. Eur. J. Transl. Myol. 2014, 25, 77–92. [Google Scholar] [CrossRef]
- Kern, H.; Hofer, C.; Mödlin, M.; Forstner, C.; Mayr, M.; Richter, W. Functional Electrical Stimulation (FES) of Long-Term Denervated Muscles in Humans: Clinical Observations and Laboratory. Basic Appl. Myol 2002, 6, 291–299. [Google Scholar]
- Kern, H.; Hofer, C.; Loefler, S.; Zampieri, S.; Gargiulo, P.; Baba, A.; Marcante, A.; Piccione, F.; Pond, A.; Carraro, U. Atrophy, ultra-structural disorders, severe atrophy and degeneration of denervated human muscle in SCI and Aging. Implications for their recovery by Functional Electrical Stimulation, updated 2017. Neurol. Res. 2017, 39, 660–666. [Google Scholar] [CrossRef]
- Kern, H.; Rossini, K.; Carraro, U.; Mayr, W.; Vogelauer, M.; Hoellwarth, U.; Hofer, C. Muscle biopsies show that FES of denervated muscles reverses human muscle degeneration from permanent spinal motoneuron lesion. J. Rehabil. Res. Dev. 2005, 42, 43–53. [Google Scholar] [CrossRef]
- Kern, H.; Boncompagni, S.; Rossini, K.; Mayr, W.; Fanò, G.; Zanin, M.E.; Podhorska-Okolow, M.; Protasi, F.; Carraro, U. Long-Term Denervation in Humans Causes Degeneration of Both Contractile and Excitation-Contraction Coupling Apparatus, Which Is Reversible by Functional Electrical Stimulation (FES): A Role for Myofiber Regeneration? J. Neuropathol. Exp. Neurol. 2004, 63, 919–931. [Google Scholar] [CrossRef] [Green Version]
- Kern, H.; Carraro, U.; Adami, N.; Hofer, C.; Löfler, S.; Vogelauer, M.; Mayr, W.; Rupp, R.; Zampieri, S. One year of home-based daily FES in complete lower motor neuron paraplegia: Recovery of tetanic contractility drives the structural improvements of denervated muscle. Neurol. Res. 2010, 32, 5–12. [Google Scholar] [CrossRef]
- Kern, H.; Carraro, U.; Adami, N.; Biral, D.; Hofer, C.; Forstner, C.; Mödlin, M.; Vogelauer, M.; Pond, A.; Boncompagni, S.; et al. Home-Based Functional Electrical Stimulation Rescues Permanently Denervated Muscles in Paraplegic Patients With Complete Lower Motor Neuron Lesion. Neurorehabilit. Neural Repair 2010, 24, 709–721. [Google Scholar] [CrossRef] [PubMed]
- Albertin, G.; Hofer, C.; Zampieri, S.; Vogelauer, M.; Löfler, S.; Ravara, B.; Guidolin, D.; Fede, C.; Incendi, D.; Porzionato, A.; et al. In complete SCI patients, long-term functional electrical stimulation of permanent denervated muscles increases epidermis thickness. Neurol. Res. 2018, 40, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Kern, H.; Carraro, U. Home-Based Functional Electrical Stimulation of Human Permanent Denervated Muscles: A Narrative Review on Diagnostics, Managements, Results and Byproducts Revisited 2020. Diagnostics 2020, 10, 529. [Google Scholar] [CrossRef] [PubMed]
- Inglis, J.G.; Howard, J.; McIntosh, K.; Gabriel, D.A.; Vandenboom, R. Decreased Motor Unit Discharge Rate in the Potenti-ated Human Tibialis Anterior Muscle. Acta Physiol. 2011, 201, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Bersch, I.; Fridén, J. Upper and Lower Motor Neuron Lesions in Tetraplegia: Implications for Surgical Nerve Transfer to Restore Hand Function. J. Appl. Physiol. 2020, 129, 1214–1219. [Google Scholar] [CrossRef] [PubMed]
- Kern, H.; Hofer, C.; Mödlin, M.; Forstner, C.; Raschka-Högler, D.; Mayr, W.; Stöhr, H. Denervated Muscles in Humans: Limitations and Problems of Currently Used Functional Electrical Stimulation Training Protocols. Artif. Organs 2002, 26, 216–218. [Google Scholar] [CrossRef] [PubMed]
- Carraro, U.; Rossini, K.; Mayr, W.; Kern, H. Muscle Fiber Regeneration in Human Permanent Lower Motoneuron Denerva-tion: Relevance to Safety and Effectiveness of FES-Training, Which Induces Muscle Recovery in SCI Subjects. Artif. Organs 2005, 29, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Kern, H.; Gargiulo, P.; Pond, A.; Albertin, G.; Marcante, A.; Carraro, U. Muscle Atrophy; Springer: Singapore, 2018. [Google Scholar]
- Bersch, I.; Fridén, J. Electrical stimulation alters muscle morphological properties in denervated upper limb muscles. Ebiomedicine 2021, 74, 103737. [Google Scholar] [CrossRef]
- Gargiulo, P.; Kern, H.; Carraro, U.; Ingvarsson, P.; Knútsdóttir, S.; Gudmundsdóttir, V.; Yngvason, S.; Vatnsdal, B.; Helgason, T. Quantitative color three-dimensional computer tomography imaging of human long-term denervated muscle. Neurol. Res. 2013, 32, 13–19. [Google Scholar] [CrossRef]
- Gargiulo, P.; Helgason, T.; Reynisson, P.J.; Helgason, B.; Kern, H.; Mayr, W.; Ingvarsson, P.; Carraro, U. Monitoring of Muscle and Bone Recovery in Spinal Cord Injury Patients Treated With Electrical Stimulation Using Three-Dimensional Imaging and Segmentation Techniques: Methodological Assessment. Artif. Organs 2011, 35, 275–281. [Google Scholar] [CrossRef]
- Gargiulo, P.; Reynisson, P.J.; Helgason, B.; Kern, H.; Mayr, W.; Ingvarsson, P.; Helgason, T.; Carraro, U. Muscle, tendons, and bone: Structural changes during denervation and FES treatment. Neurol. Res. 2011, 33, 750–758. [Google Scholar] [CrossRef]
- Gargiulo, P.; Vatnsdal, B.; Ingvarsson, P.; Knútsdóttir, S.; Gudmundsdóttir, V.; Yngvason, S.; Helgason, T. Restoration of Muscle Volume and Shape Induced by Electrical Stimulation of Denervated Degenerated Muscles: Qualitative and Quantitative Measurement of Changes in Rectus Femoris Using Computer Tomography and Image Segmentation. Artif. Organs 2008, 32, 609–613. [Google Scholar] [CrossRef]
- Helgason, T.; Gargiulo, P.; Johannesdottir, F.; Ingvarsson, P.; Knútsdóttir, S.; Gudmundsdóttir, V.; Yngvason, S. Monitoring Muscle Growth and Tissue Changes Induced by Electrical Stimulation of Denervated Degenerated Muscles With CT and Stereolithographic 3D Modeling. Artif. Organs 2005, 29, 440–443. [Google Scholar] [CrossRef]
- Salmons, S.; Ashley, Z.; Sutherland, H.; Russold, M.F.; Li, F.; Jarvis, J.C. Functional Electrical Stimulation of Denervated Muscles: Basic Issues. Artif. Organs 2005, 29, 199–202. [Google Scholar] [CrossRef]
- Hofer, C.; Forstner, C.; Mödlin, M.; Jäger, H.; Mayr, W.; Kern, H. In Vivo Assessment of Conduction Velocity and Refractory Period of Denervated Muscle Fibers. Artif. Organs 2005, 29, 436–439. [Google Scholar] [CrossRef]
- Pieber, K.; Herceg, M.; Paternostro-Sluga, T.; Schuhfried, O. Optimizing stimulation parameters in functional electrical stimulation of denervated muscles: A cross-sectional study. J. Neuroeng. Rehabil. 2015, 12, 51. [Google Scholar] [CrossRef] [Green Version]
- Ravara, B.; Hofer, C.; Kern, H.; Guidolin, D.; Porzionato, A.; De Caro, R.; Albertin, G. Dermal papillae flattening of thigh skin in Conus Cauda Syndrome. Eur. J. Transl. Myol. 2018, 28, 7914. [Google Scholar] [CrossRef]
- Kern, H.; Gargiulo, P.; Pond, A.; Albertin, G.; Marcante, A.; Carraro, U. To Reverse Atrophy of Human Muscles in Complete SCI Lower Motor Neuron Denervation by Home-Based Functional Electrical Stimulation. In Muscle Atrophy; Springer: Singapore, 2018. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant | Age | NLI | AIS Score | Time Since Injury (Years) | Previous Pressure Ulcers (Number, Location, Treatment) | Stimulation Period & Number of Sessions |
|---|---|---|---|---|---|---|
| 1 | 43 | T9 | A | 23 | Recuring, sacrum + tuber ischiadicum, conservative | 21 weeks, 92 sessions |
| 2 | 49 | L1 | C | 2 | 3, tuber ischiadicum, operative | 26 weeks, 129 sessions |
| 3 | 33 | T11 | A | 32 | 2, tuber ischiadicum, conservative | 26 weeks, 117 sessions |
| 4 | 65 | C4 | A | 27 | 2, tuber ischiadicum, conservative | 27 weeks, 129 sessions |
| 5 | 62 | T12 | A | 20 | No data | 27 weeks, 121 sessions |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alberty, M.; Mayr, W.; Bersch, I. Electrical Stimulation for Preventing Skin Injuries in Denervated Gluteal Muscles—Promising Perspectives from a Case Series and Narrative Review. Diagnostics 2023, 13, 219. https://doi.org/10.3390/diagnostics13020219
Alberty M, Mayr W, Bersch I. Electrical Stimulation for Preventing Skin Injuries in Denervated Gluteal Muscles—Promising Perspectives from a Case Series and Narrative Review. Diagnostics. 2023; 13(2):219. https://doi.org/10.3390/diagnostics13020219
Chicago/Turabian StyleAlberty, Marie, Winfried Mayr, and Ines Bersch. 2023. "Electrical Stimulation for Preventing Skin Injuries in Denervated Gluteal Muscles—Promising Perspectives from a Case Series and Narrative Review" Diagnostics 13, no. 2: 219. https://doi.org/10.3390/diagnostics13020219