
Application of Machine Learning Algorithm in Predicting Axillary Lymph Node Metastasis from Breast Cancer on Preoperative Chest CT
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
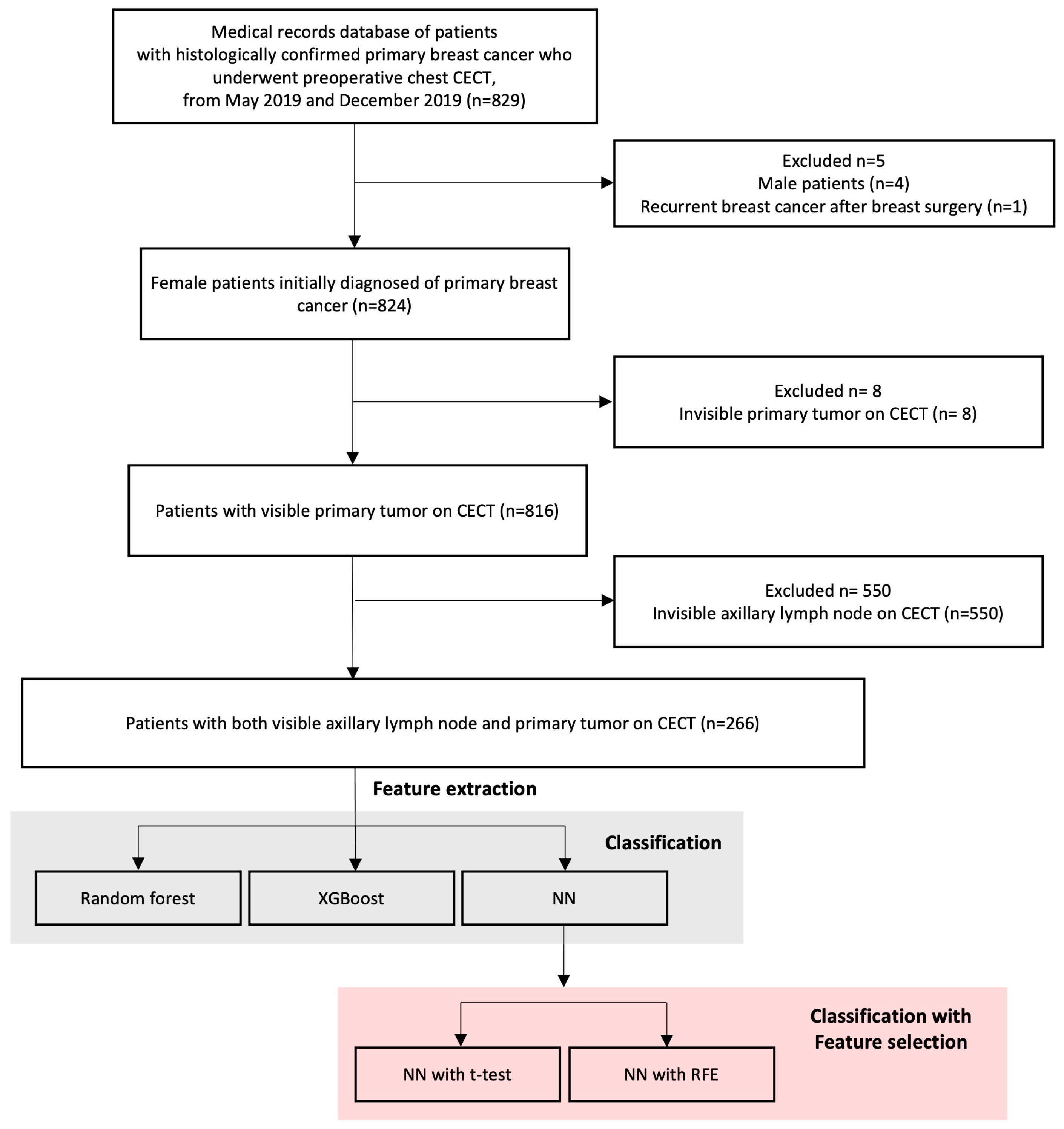
2.1. Data Collection
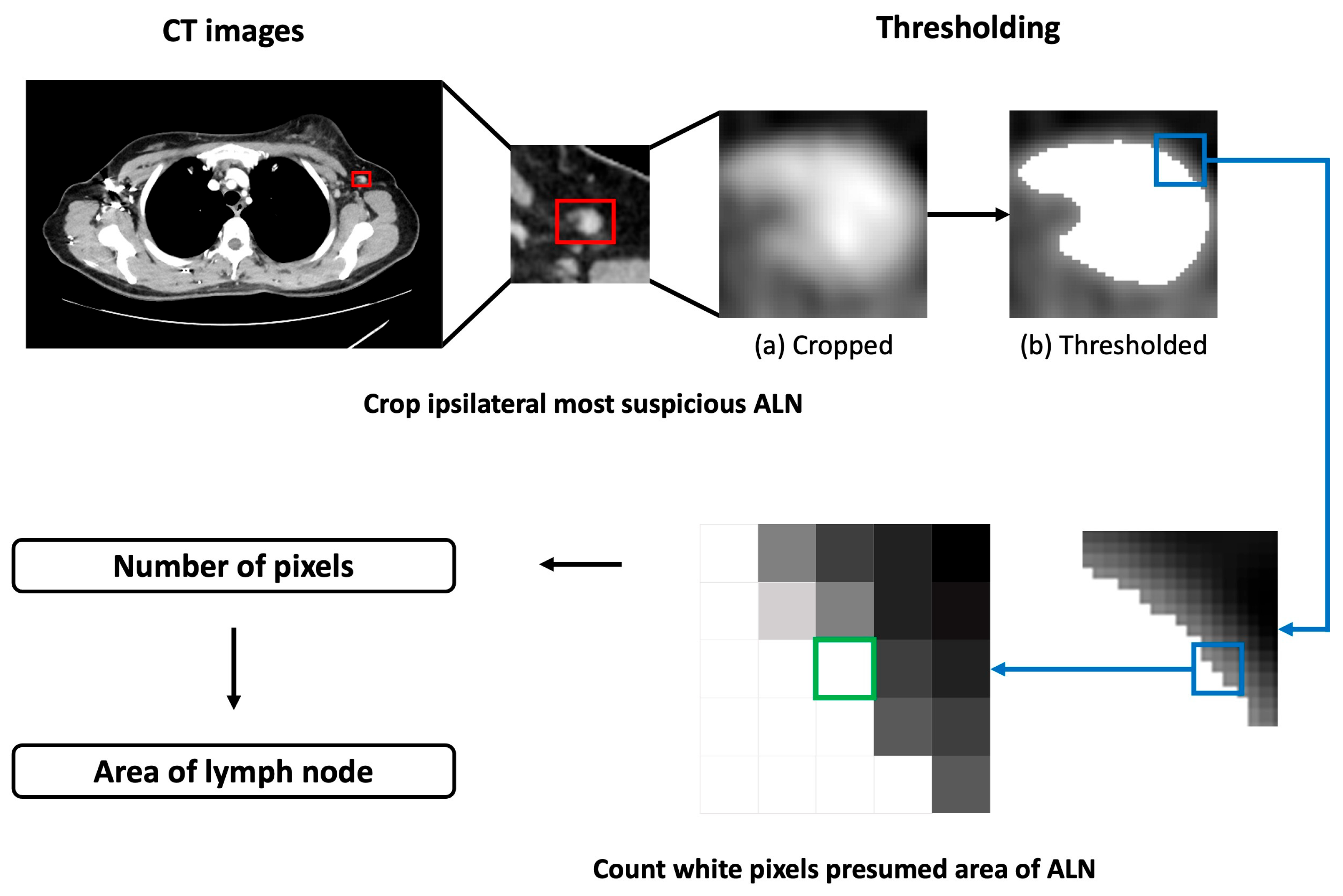
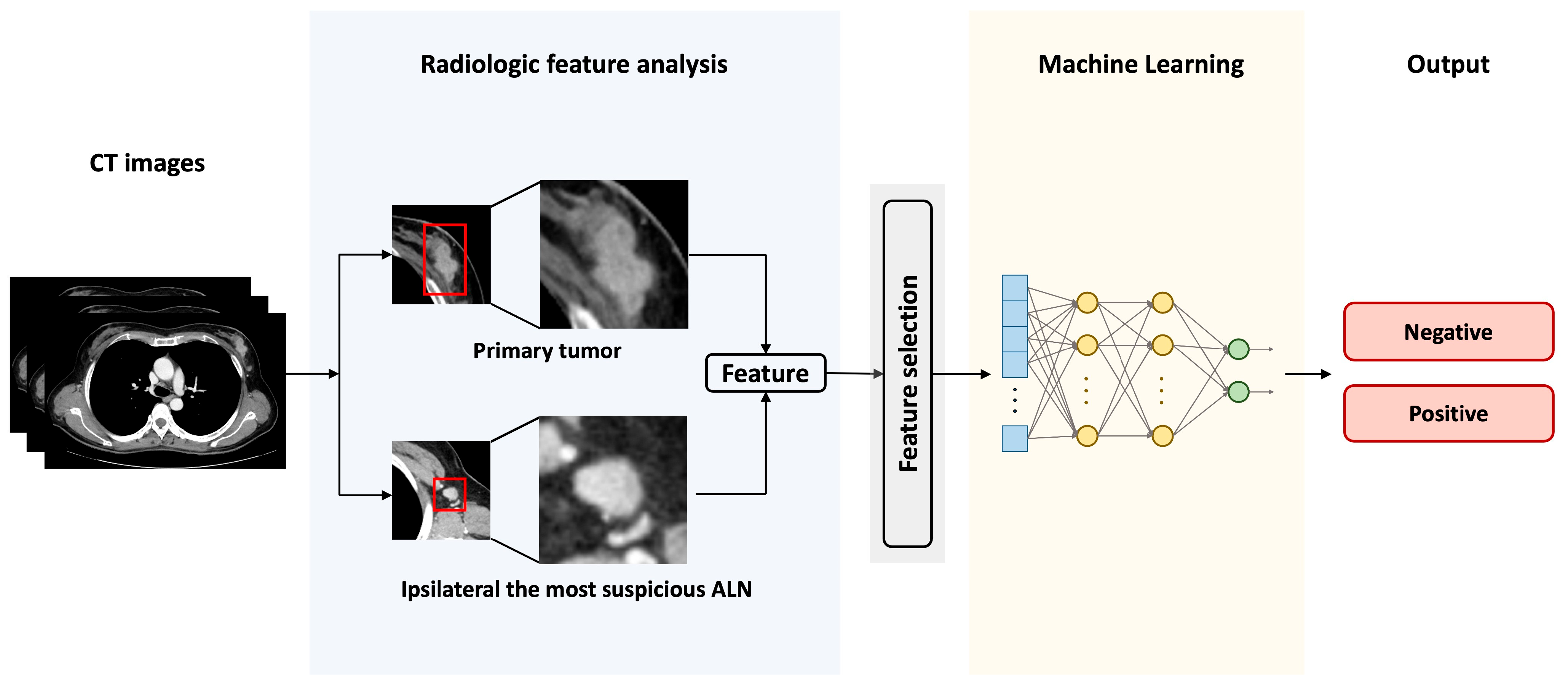
2.2. Feature Extraction
2.3. Feature Selection Methods
2.4. Machine Learning Algorithms
2.5. Evaluation of Machine Learning Models
3. Results
3.1. Data Collection and Feature Engineering
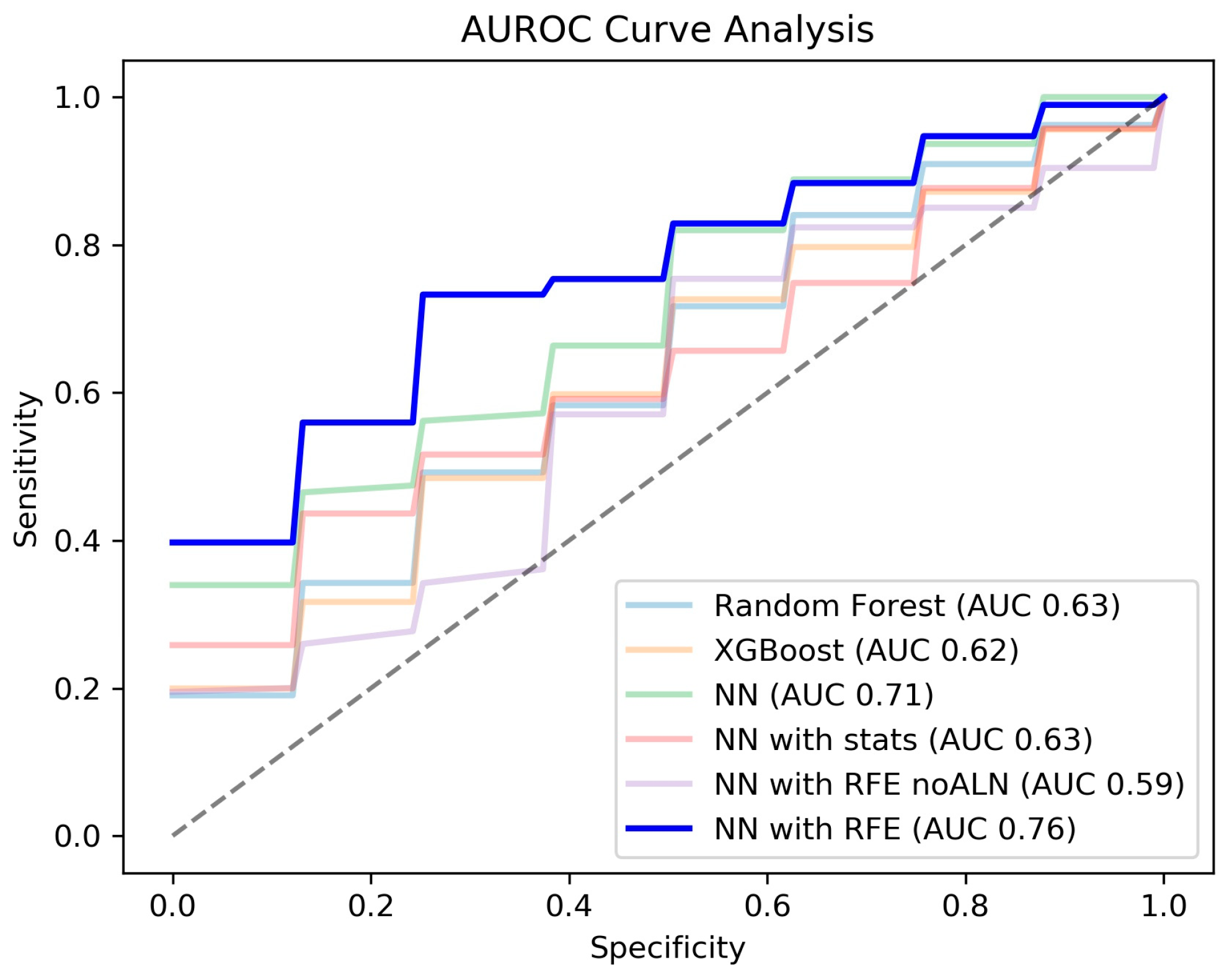
3.2. Performance Comparisons of ML Models for Detecting ALN Metastasis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA A Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Quiet, C.A.; Ferguson, D.J.; Weichselbaum, R.R.; Hellman, S. Natural history of node-negative breast cancer: A study of 826 patients with long-term follow-up. J. Clin. Oncol. 1995, 13, 1144–1151. [Google Scholar] [CrossRef] [PubMed]
- Tafreshi, N.K.; Kumar, V.; Morse, D.L.; Gatenby, R.A. Molecular and Functional Imaging of Breast Cancer. Cancer Control 2010, 17, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Dong, J.; Liu, Z.; Guo, Q.; Nie, Y.; Huang, D.; Qin, N.; Shu, J. Prediction of Metastasis in the Axillary Lymph Nodes of Patients With Breast Cancer: A Radiomics Method Based on Contrast-Enhanced Computed Tomography. Front. Oncol. 2021, 11, 726240. [Google Scholar] [CrossRef] [PubMed]
- Ashiba, H.; Nakayama, R. Computerized evaluation scheme to detect metastasis in sentinel lymph nodes using contrast-enhanced computed tomography before breast cancer surgery. Radiol. Phys. Technol. 2019, 12, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Urata, M.; Kijima, Y.; Hirata, M.; Shinden, Y.; Arima, H.; Nakajo, A.; Koriyama, C.; Arigami, T.; Uenosono, Y.; Okumura, H.; et al. Computed tomography Hounsfield units can predict breast cancer metastasis to axillary lymph nodes. BMC Cancer 2014, 14, 730. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zhang, Y.; Zhang, W.; Gao, Y.; Jia, S.; Guo, J. Contrast enhanced computed tomography is indicative for angiogenesis pattern and display prognostic significance in breast cancer. BMC Cancer 2014, 14, 672. [Google Scholar] [CrossRef]
- Torabi, M.; Aquino, S.L.; Harisinghani, M.G. Current concepts in lymph node imaging. J. Nucl. Med. 2004, 45, 1509–1518. [Google Scholar]
- Samiei, S.; Granzier, R.W.Y.; Ibrahim, A.; Primakov, S.; Lobbes, M.B.I.; Beets-Tan, R.G.H.; van Nijnatten, T.J.A.; Engelen, S.M.E.; Woodruff, H.C.; Smidt, M.L. Dedicated Axillary MRI-Based Radiomics Analysis for the Prediction of Axillary Lymph Node Metastasis in Breast Cancer. Cancers 2021, 13, 757. [Google Scholar] [CrossRef]
- Zhou, L.-Q.; Wu, X.-L.; Huang, S.-Y.; Wu, G.-G.; Ye, H.-R.; Wei, Q.; Bao, L.-Y.; Deng, Y.-B.; Li, X.-R.; Cui, X.-W.; et al. Lymph Node Metastasis Prediction from Primary Breast Cancer US Images Using Deep Learning. Radiology 2019, 294, 19–28. [Google Scholar] [CrossRef]
- Chen, M.; Kong, C.; Lin, G.; Chen, W.; Guo, X.; Chen, Y.; Cheng, X.; Chen, M.; Shi, C.; Xu, M.; et al. Development and validation of convolutional neural network-based model to predict the risk of sentinel or non-sentinel lymph node metastasis in patients with breast cancer: A machine learning study. eClinicalMedicine 2023, 63, 102176. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Wu, L.; Ye, W.; Zhao, K.; Wang, Y.; Liu, W.; Li, J.; Li, H.; Liu, Z.; Liang, C. Deep Learning Signature Based on Staging CT for Preoperative Prediction of Sentinel Lymph Node Metastasis in Breast Cancer. Acad. Radiol. 2020, 27, 1226–1233. [Google Scholar] [CrossRef] [PubMed]
- Barranger, E.; Coutant, C.; Flahault, A.; Delpech, Y.; Darai, E.; Uzan, S. An axilla scoring system to predict non-sentinel lymph node status in breast cancer patients with sentinel lymph node involvement. Breast Cancer Res. Treat. 2005, 91, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Degnim, A.C.; Reynolds, C.; Pantvaidya, G.; Zakaria, S.; Hoskin, T.; Barnes, S.; Roberts, M.V.; Lucas, P.C.; Oh, K.; Koker, M.; et al. Nonsentinel node metastasis in breast cancer patients: Assessment of an existing and a new predictive nomogram. Am. J. Surg. 2005, 190, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Hwang, R.F.; Krishnamurthy, S.; Hunt, K.K.; Mirza, N.; Ames, F.C.; Feig, B.; Kuerer, H.M.; Singletary, S.E.; Babiera, G.; Meric, F.; et al. Clinicopathologic factors predicting involvement of nonsentinel axillary nodes in women with breast cancer. Ann. Surg. Oncol. 2003, 10, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Kohrt, H.E.; Olshen, R.A.; Bermas, H.R.; Goodson, W.H.; Wood, D.J.; Henry, S.; Rouse, R.V.; Bailey, L.; Philben, V.J.; Dirbas, F.M.; et al. New models and online calculator for predicting non-sentinel lymph node status in sentinel lymph node positive breast cancer patients. BMC Cancer 2008, 8, 66. [Google Scholar] [CrossRef] [PubMed]
- Pal, A.; Provenzano, E.; Duffy, S.W.; Pinder, S.E.; Purushotham, A.D. A model for predicting non-sentinel lymph node metastatic disease when the sentinel lymph node is positive. Br. J. Surg. 2008, 95, 302–309. [Google Scholar] [CrossRef]
- Saidi, R.F.; Dudrick, P.S.; Remine, S.G.; Mittal, V.K. Nonsentinel lymph node status after positive sentinel lymph node biopsy in early breast cancer. Am. Surg. 2004, 70, 101–105; discussion 105, discussion 105. [Google Scholar] [CrossRef]
- Van Zee, K.J.; Manasseh, D.M.; Bevilacqua, J.L.; Boolbol, S.K.; Fey, J.V.; Tan, L.K.; Borgen, P.I.; Cody, H.S., 3rd; Kattan, M.W. A nomogram for predicting the likelihood of additional nodal metastases in breast cancer patients with a positive sentinel node biopsy. Ann. Surg. Oncol. 2003, 10, 1140–1151. [Google Scholar] [CrossRef]
- Chang, J.M.; Leung, J.W.T.; Moy, L.; Ha, S.M.; Moon, W.K. Axillary Nodal Evaluation in Breast Cancer: State of the Art. Radiology 2020, 295, 500–515. [Google Scholar] [CrossRef]
- Sickles, E.A.; D’Orsi, C.J.; Bassett, L.W.; Appleton, C.M.; Berg, W.A.; Burnside, E.S. ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System; American College of Radiology: Reston, VA, USA, 2013; pp. 39–48. [Google Scholar]
- Muller, N.L. Computed tomography and magnetic resonance imaging: Past, present and future. Eur. Respir. J. 2002, 19, 3S–12S. [Google Scholar] [CrossRef]
- Choi, Y.J.; Kim, T.H.; Cha, Y.J.; Son, E.J.; Gweon, H.M.; Park, C.H. Incidental Breast Lesions on Chest CT: Clinical Significance and Differential Features Requiring Referral. J. Korean Soc. Radiol. 2018, 79, 303–310. [Google Scholar] [CrossRef]
- Park, J.; Kim, C.; Cha, Y.K.; Chung, M.J. Missed and Detected Incidental Breast Cancers on Contrast Enhanced Chest CT: Detection Rates and CT Features. Diagnostics 2023, 13, 1522. [Google Scholar] [CrossRef] [PubMed]
- Ruppert-Kohlmayr, A.J.; Uggowitzer, M.; Meissnitzer, T.; Ruppert, G. Differentiation of Renal Clear Cell Carcinoma and Renal Papillary Carcinoma Using Quantitative CT Enhancement Parameters. Am. J. Roentgenol. 2004, 183, 1387–1391. [Google Scholar] [CrossRef] [PubMed]
- Cho, B.H.; Yu, H.; Kim, K.-W.; Kim, T.H.; Kim, I.Y.; Kim, S.I. Application of irregular and unbalanced data to predict diabetic nephropathy using visualization and feature selection methods. Artif. Intell. Med. 2008, 42, 37–53. [Google Scholar] [CrossRef]
- Vasantha, M.S.; Bharathi, D.V.S.; Dhamodharan, R.K. Medical Image Feature, Extraction, Selection and Classification. Int. J. Eng. Sci. Technol. 2010, 2, 2071–2076. [Google Scholar]
- Zhang, Y.; Ling, C. A strategy to apply machine learning to small datasets in materials science. Npj Comput. Mater. 2018, 4, 25. [Google Scholar] [CrossRef]
- Zhang, X.; Yu, L.; Yin, H.; Lai, K.K. Integrating data augmentation and hybrid feature selection for small sample credit risk assessment with high dimensionality. Comput. Oper. Res. 2022, 146, 105937. [Google Scholar] [CrossRef]
- Cho, B.H.; Yu, H.; Lee, J.; Chee, Y.J.; Kim, I.Y.; Kim, S.I. Nonlinear support vector machine visualization for risk factor analysis using nomograms and localized radial basis function kernels. IEEE Trans. Inf. Technol. Biomed. 2008, 12, 247–256. [Google Scholar] [CrossRef]
- Cho, B.H.; Lee, D.Y.; Park, K.A.; Oh, S.Y.; Moon, J.H.; Lee, G.I.; Noh, H.; Chung, J.K.; Kang, M.C.; Chung, M.J. Computer-aided recognition of myopic tilted optic disc using deep learning algorithms in fundus photography. BMC Ophthalmol. 2020, 20, 407. [Google Scholar] [CrossRef]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef]
- Chen, T.; Guestrin, C. Xgboost: A scalable tree boosting system. In Proceedings of the 22nd ACM Sigkdd International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; pp. 785–794. [Google Scholar]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Larochelle, H.; Erhan, D.; Courville, A.; Bergstra, J.; Bengio, Y. An empirical evaluation of deep architectures on problems with many factors of variation. In Proceedings of the 24th International Conference on Machine Learning—ICML’07, Corvallis, OR, USA, 20–24 June 2007. [Google Scholar]
- Yang, L.; Shami, A. On hyperparameter optimization of machine learning algorithms: Theory and practice. Neurocomputing 2020, 415, 295–316. [Google Scholar] [CrossRef]
- Diederik; Ba, J. Adam: A Method for Stochastic Optimization. arXiv 2017, arXiv:1412.6980. [Google Scholar]
- Santos, M.S.; Soares, J.P.; Abreu, P.H.; Araujo, H.; Santos, J. Cross-Validation for Imbalanced Datasets: Avoiding Overoptimistic and Overfitting Approaches [Research Frontier]. IEEE Comput. Intell. Mag. 2018, 13, 59–76. [Google Scholar] [CrossRef]
- Kau, R.J.; Alexiou, C.; Laubenbacher, C.; Werner, M.; Schwaiger, M.; Arnold, W. Lymph node detection of head and neck squamous cell carcinomas by positron emission tomography with fluorodeoxyglucose F 18 in a routine clinical setting. Arch. Otorhinolaryngol.-Head Neck Surg. 1999, 125, 1322–1328. [Google Scholar] [CrossRef] [PubMed]
- Dwamena, B.A.; Sonnad, S.S.; Angobaldo, J.O.; Wahl, R.L. Metastases from non-small cell lung cancer: Mediastinal staging in the 1990s—Meta-analytic comparison of PET and CT. Radiology 1999, 213, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Fischbein, N.J.; Noworolski, S.M.; Henry, R.G.; Kaplan, M.J.; Dillon, W.P.; Nelson, S.J. Assessment of metastatic cervical adenopathy using dynamic contrast-enhanced MR imaging. AJNR Am. J. Neuroradiol. 2003, 24, 301–311. [Google Scholar]
- Laissy, J.P.; Gay-Depassier, P.; Soyer, P.; Dombret, M.C.; Murciano, G.; Sautet, A.; Aubier, M.; Menu, Y. Enlarged mediastinal lymph nodes in bronchogenic carcinoma: Assessment with dynamic contrast-enhanced MR imaging. Work in progress. Radiology 1994, 191, 263–267. [Google Scholar] [CrossRef]
- Szabó, B.K.; Aspelin, P.; Kristoffersen Wiberg, M.; Tot, T.; Boné, B. Invasive breast cancer: Correlation of dynamic MR features with prognostic factors. Eur. Radiol. 2003, 13, 2425–2435. [Google Scholar] [CrossRef]
- Zheng, X.; Yao, Z.; Huang, Y.; Yu, Y.; Wang, Y.; Liu, Y.; Mao, R.; Li, F.; Xiao, Y.; Wang, Y.; et al. Deep learning radiomics can predict axillary lymph node status in early-stage breast cancer. Nat. Commun. 2020, 11, 1236. [Google Scholar] [CrossRef] [PubMed]
- Song, B.-I. A machine learning-based radiomics model for the prediction of axillary lymph-node metastasis in breast cancer. Breast Cancer 2021, 28, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Liu, M.; Ren, W.; Sun, J.; Wang, K.; Xi, X.; Zhang, G. Predicting of axillary lymph node metastasis in invasive breast cancer using multiparametric MRI dataset based on CNN model. Front. Oncol. 2022, 12, 1069733. [Google Scholar] [CrossRef] [PubMed]
- Piao, Y.; Piao, M.; Park, K.; Ryu, K.H. An ensemble correlation-based gene selection algorithm for cancer classification with gene expression data. Bioinformatics 2012, 28, 3306–3315. [Google Scholar] [CrossRef] [PubMed]
- Bolón-Canedo, V.; Sánchez-Maroño, N.; Alonso-Betanzos, A. A review of feature selection methods on synthetic data. Knowl. Inf. Syst. 2013, 34, 483–519. [Google Scholar] [CrossRef]
- O’Toole, J.; Miller, C.L.; Specht, M.C.; Skolny, M.N.; Jammallo, L.S.; Horick, N.; Elliott, K.; Niemierko, A.; Taghian, A.G. Cording following treatment for breast cancer. Breast Cancer Res. Treat. 2013, 140, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Nieves Maldonado, S.M.; Pubul Núñez, V.; Argibay Vázquez, S.; Macías Cortiñas, M.; Ruibal Morell, Á. Axillary web syndrome following sentinel node biopsy for breast cancer. Rev. Esp. Med. Nucl. Imagen Mol. (Engl. Ed.) 2016, 35, 325–328. [Google Scholar] [CrossRef]
- Kim, E.J.; Kim, S.H.; Kang, B.J.; Choi, B.G.; Song, B.J.; Choi, J.J. Diagnostic value of breast MRI for predicting metastatic axillary lymph nodes in breast cancer patients: Diffusion-weighted MRI and conventional MRI. Magn. Reson. Imaging 2014, 32, 1230–1236. [Google Scholar] [CrossRef]
- Joo, S.; Ko, E.S.; Kwon, S.; Jeon, E.; Jung, H.; Kim, J.-Y.; Chung, M.J.; Im, Y.-H. Multimodal deep learning models for the prediction of pathologic response to neoadjuvant chemotherapy in breast cancer. Sci. Rep. 2021, 11, 18800. [Google Scholar] [CrossRef]
- Lai, Z.; Deng, H. Medical Image Classification Based on Deep Features Extracted by Deep Model and Statistic Feature Fusion with Multilayer Perceptron. Comput. Intell. Neurosci. 2018, 2018, 2061516. [Google Scholar] [CrossRef]
- Wang, S.; Li, C.; Wang, R.; Liu, Z.; Wang, M.; Tan, H.; Wu, Y.; Liu, X.; Sun, H.; Yang, R.; et al. Annotation-efficient deep learning for automatic medical image segmentation. Nat. Commun. 2021, 12, 5915. [Google Scholar] [CrossRef]
- Khan, B.; Fatima, H.; Qureshi, A.; Kumar, S.; Hanan, A.; Hussain, J.; Abdullah, S. Drawbacks of Artificial Intelligence and Their Potential Solutions in the Healthcare Sector. Biomed. Mater. Devices 2023, 1–8. [Google Scholar] [CrossRef]
- Ansari, A.A.; Mishra, B.; Gera, P.; Khan, M.K.; Chakraborty, C.; Mishra, D. Privacy-Enabling Framework for Cloud-Assisted Digital Healthcare Industry. IEEE Trans. Ind. Inform. 2022, 18, 8316–8325. [Google Scholar] [CrossRef]
- Cao, Y.; Zhou, Z.; Chakraborty, C.; Wang, M.; Wu, Q.M.J.; Sun, X.; Yu, K. Generative Steganography Based on Long Readable Text Generation. IEEE Trans. Comput. Soc. Syst. 2022, 1–11. [Google Scholar] [CrossRef]
- Tang, M.; Gandhi, P.; Md; Zou, C.; Blakey, J.; Luo, X. Progress Notes Classification and Keyword Extraction using Attention-based Deep Learning Models with BERT. arXiv 2019, arXiv:1910.05786. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients | ALN Metastasis (−) | ALN Metastasis (+) | p-Value | |||
|---|---|---|---|---|---|---|
| Age (years) | 50 (23–81) | 49.5 (23–77) | 50 (32–81) | - | ||
| Primary tumor | ||||||
| T_site (left/right) | 133:133 | 38:42 | 95:91 | - | ||
| T_size (mm) | 18.72 ± 10.03 | 21.27 ± 13.54 | 17.62 ± 7.85 | <0.05 | ||
| Enhancement pattern | ||||||
| T_homogeneous a (E1:E2:E3:E4) | 234 (87.97%) (3:33:115:83) | 65 (81.25%) (1:13:30:21) | 169 (90.86%) (2:20:85:62) | <0.05 | ||
| T_heterogeneous | 8 (3.01%) | 3 (3.75%) | 5 (2.69%) | - | ||
| T_non-mass | 24 (9.02%) | 12 (15.00%) | 12 (6.45%) | <0.05 | ||
| Enhancement degree (HU) | ||||||
| T_average | 85.96 ± 22.02 | 88.78 ± 24.64 | 84.75 ± 20.74 | - | ||
| T_SD | 11.71 ± 5.84 | 11.26 ± 5.79 | 11.90 ± 5.87 | - | ||
| Lymph node | ||||||
| N_average | 81.44 ± 21.31 | 83.68 ± 21.46 | 80.48 ± 21.23 | - | ||
| N_area | 884.01 ± 282.24 | 940.35 ± 243.31 | 859.78 ± 294.73 | <0.05 | ||
| Aorta | ||||||
| A_average | 174.39 ± 21.46 | 173.17 ± 19.24 | 174.92 ± 22.38 | - | ||
| A_SD | 8.65 ± 2.32 | 8.33 ± 2.10 | 8.78 ± 2.40 | - | ||
| Calibrated enhancement degree b | ||||||
| (Aorta − Tumor) | 88.43 ± 26.34 | 84.39 ± 27.11 | 90.17 ± 25.89 | - | ||
| (Aorta − Node) | 92.95 ± 26.13 | 89.49 ± 22.09 | 94.44 ± 27.60 | - | ||
| (Tumor − Node) | 4.52 ± 27.16 | 5.11 ± 28.87 | 4.27 ± 26.48 | - | ||
| Classification | Classification with Feature Selection | ||||
|---|---|---|---|---|---|
| RF | XGBoost | NN | NN with Stats a | NN with RFE * | |
| AUROC | 0.63 ± 0.11 (0.47–0.84) | 0.62 ± 0.08 (0.51–0.74) | 0.71 ± 0.13 (0.49–0.84) | 0.63 ± 0.12 (0.49–0.87) | 0.76 ± 0.11 (0.61–0.97) |
| Accuracy | 0.70 ± 0.07 (0.56–0.81) | 0.66 ± 0.06 (0.56–0.74) | 0.72 ± 0.12 (0.44–0.85) | 0.61 ± 0.13 (0.44–0.85) | 0.74 ± 0.12 (0.56–0.92) |
| PPV | 0.72 ± 0.04 | 0.73 ± 0.04 | 0.90 ± 0.09 | 0.92 ± 0.07 | 0.93 ± 0.06 |
| NPV | 0.48 ± 0.35 | 0.45 ± 0.23 | 0.61 ± 0.20 | 0.45 ± 0.11 | 0.59 ± 0.19 |
| Sensitivity | 0.91 ± 0.08 | 0.82 ± 0.08 | 0.71 ± 0.24 | 0.49 ± 0.21 | 0.69 ± 0.29 |
| Specificity | 0.18 ± 0.13 | 0.28 ± 0.13 | 0.75 ± 0.24 | 0.88 ± 0.12 | 0.88 ± 0.12 |
| RFE without Lymph Features | RFE with Lymph Features * | |
|---|---|---|
| AUROC | 0.59 ± 0.17 (0.34–0.96) | 0.76 ± 0.11 (0.61–0.97) |
| Accuracy | 0.66 ± 0.18 (0.37–0.88) | 0.74 ± 0.12 (0.56–0.92) |
| PPV | 0.88 ± 0.11 | 0.93 ± 0.06 |
| NPV | 0.53 ± 0.17 | 0.59 ± 0.19 |
| Sensitivity | 0.63 ± 0.32 | 0.69 ± 0.29 |
| Specificity | 0.71 ± 0.25 | 0.88 ± 0.12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.; Kim, J.H.; Cha, Y.K.; Chung, M.J.; Woo, J.H.; Park, S. Application of Machine Learning Algorithm in Predicting Axillary Lymph Node Metastasis from Breast Cancer on Preoperative Chest CT. Diagnostics 2023, 13, 2953. https://doi.org/10.3390/diagnostics13182953
Park S, Kim JH, Cha YK, Chung MJ, Woo JH, Park S. Application of Machine Learning Algorithm in Predicting Axillary Lymph Node Metastasis from Breast Cancer on Preoperative Chest CT. Diagnostics. 2023; 13(18):2953. https://doi.org/10.3390/diagnostics13182953
Chicago/Turabian StylePark, Soyoung, Jong Hee Kim, Yoon Ki Cha, Myung Jin Chung, Jung Han Woo, and Subin Park. 2023. "Application of Machine Learning Algorithm in Predicting Axillary Lymph Node Metastasis from Breast Cancer on Preoperative Chest CT" Diagnostics 13, no. 18: 2953. https://doi.org/10.3390/diagnostics13182953