
Automated Diagnosis for Colon Cancer Diseases Using Stacking Transformer Models and Explainable Artificial Intelligence

 , , , ,
, , , , 
Abstract
:1. Introduction
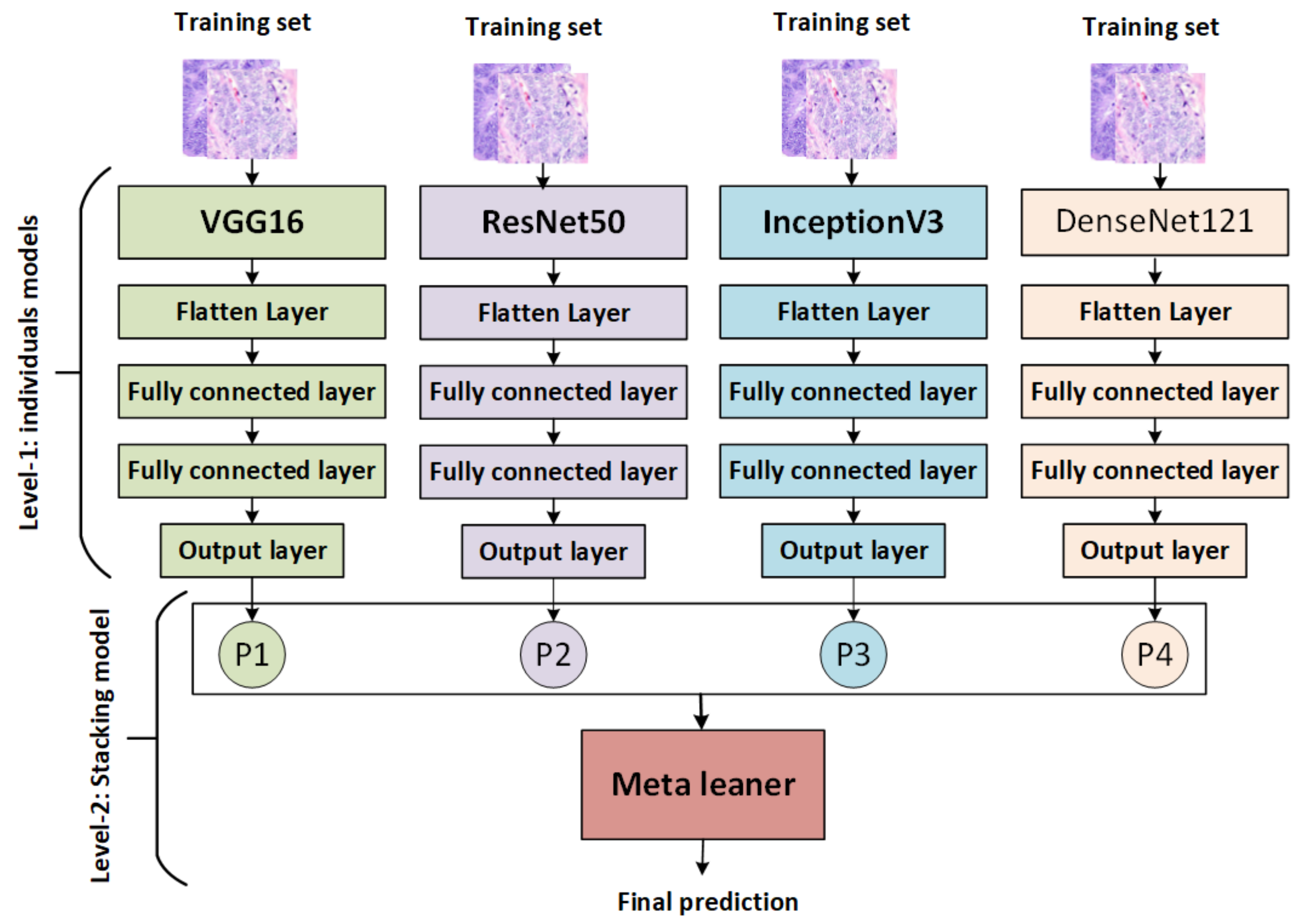
- A stacking model is developed based on integration of the output of pretrained base models (VGG16, InceptionV3, DenseNet121, and ResNet50) with a meta-learning (SVM) model to enhance performance;
- Stacking-SVM models are compared with VGG16, InceptionV3, DenseNet121, and ResNet50 using various evaluation methods and two image databases;
- Stacking-SVM achieves the best results compared to other models;
- Black-box deep learning models are represented using explainable AI (XAI).
2. Related Work
3. Methodology
3.1. Data Collection
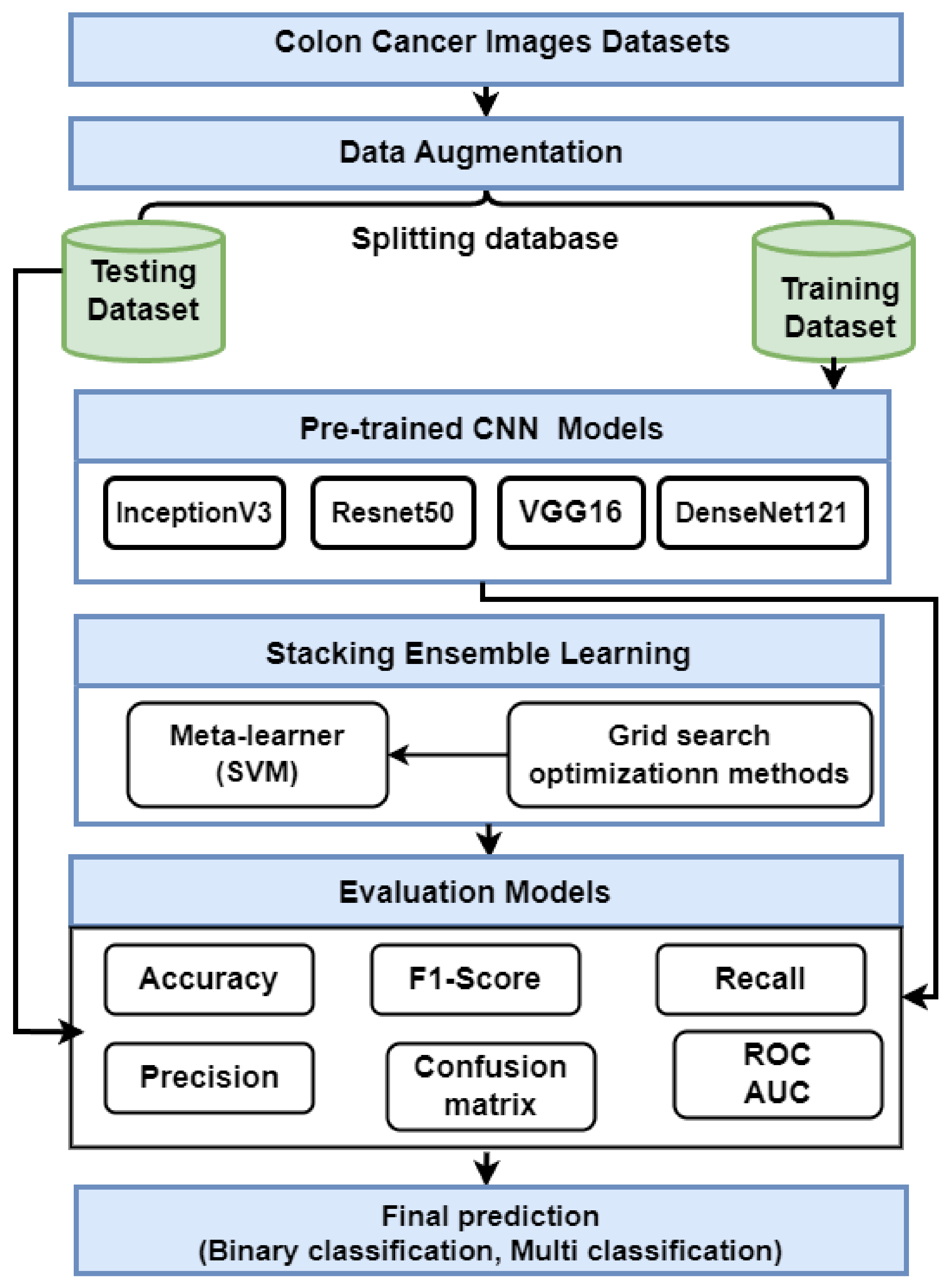
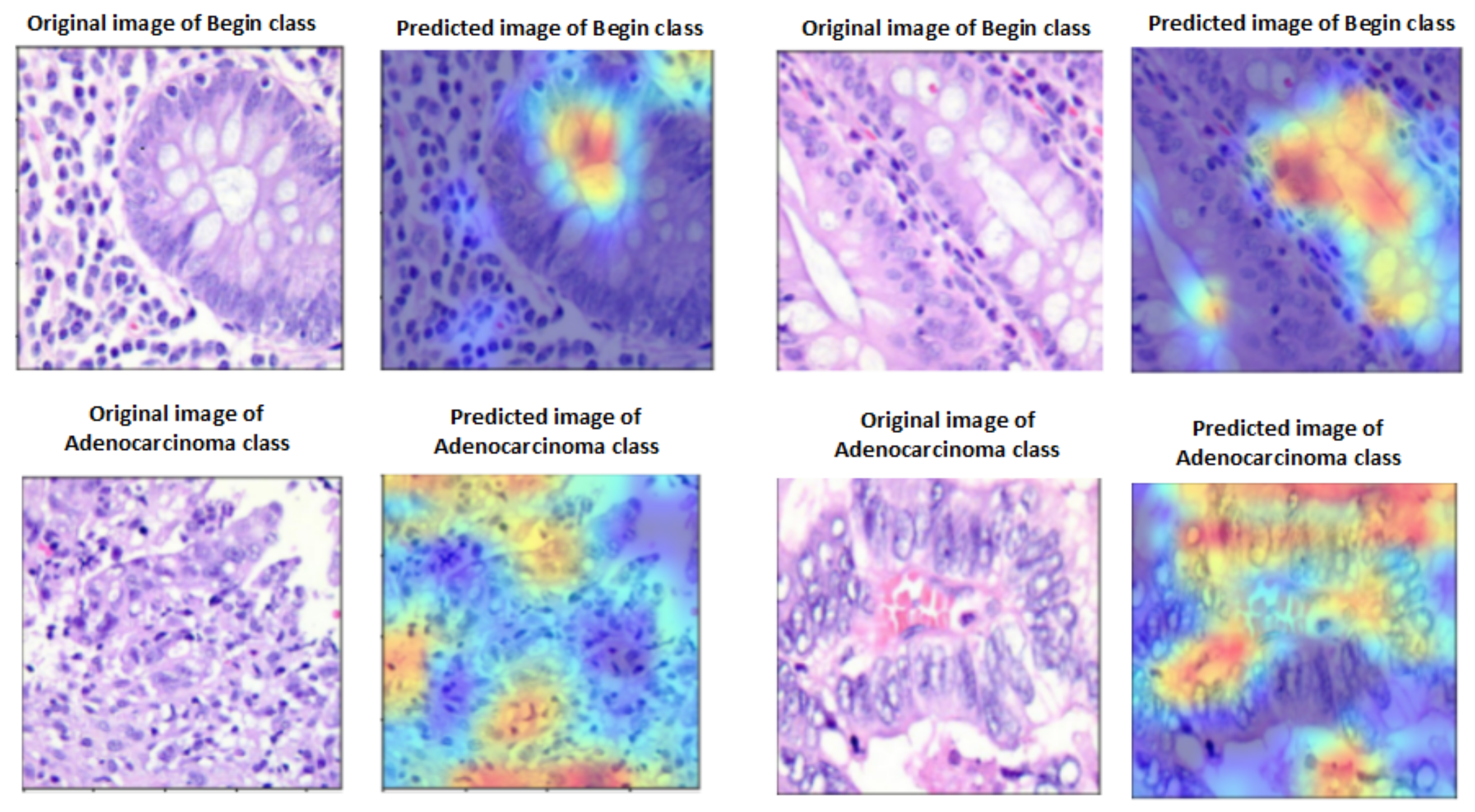
- We used a dataset known as LC25000, which contains histopathological images of colon cancer [45]. There are 5000 images for adenocarcinoma and 5000 images for benign colon cancers in the set. The dataset is split into 70% training (7000 images) and 30% testing (2000 images).
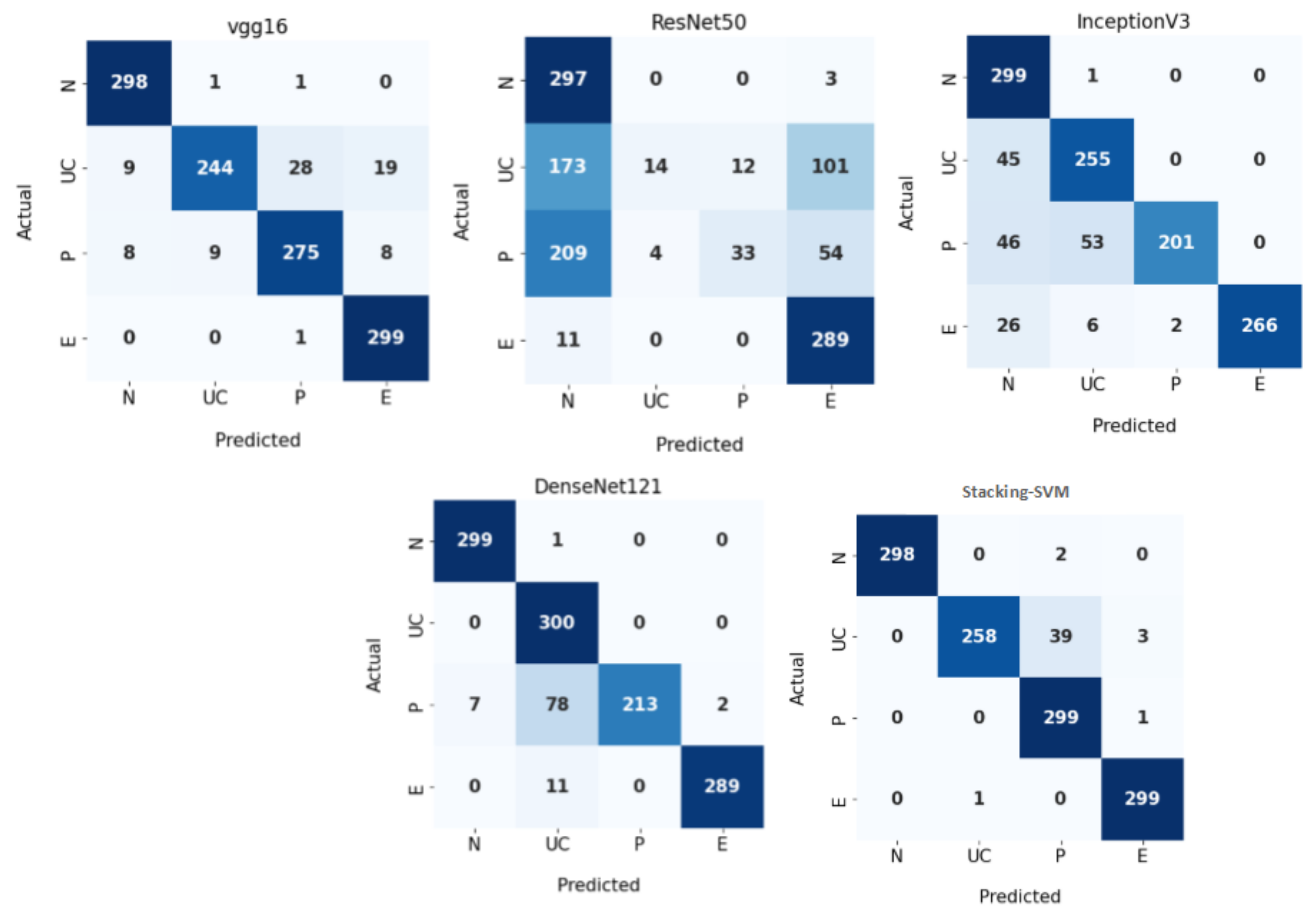
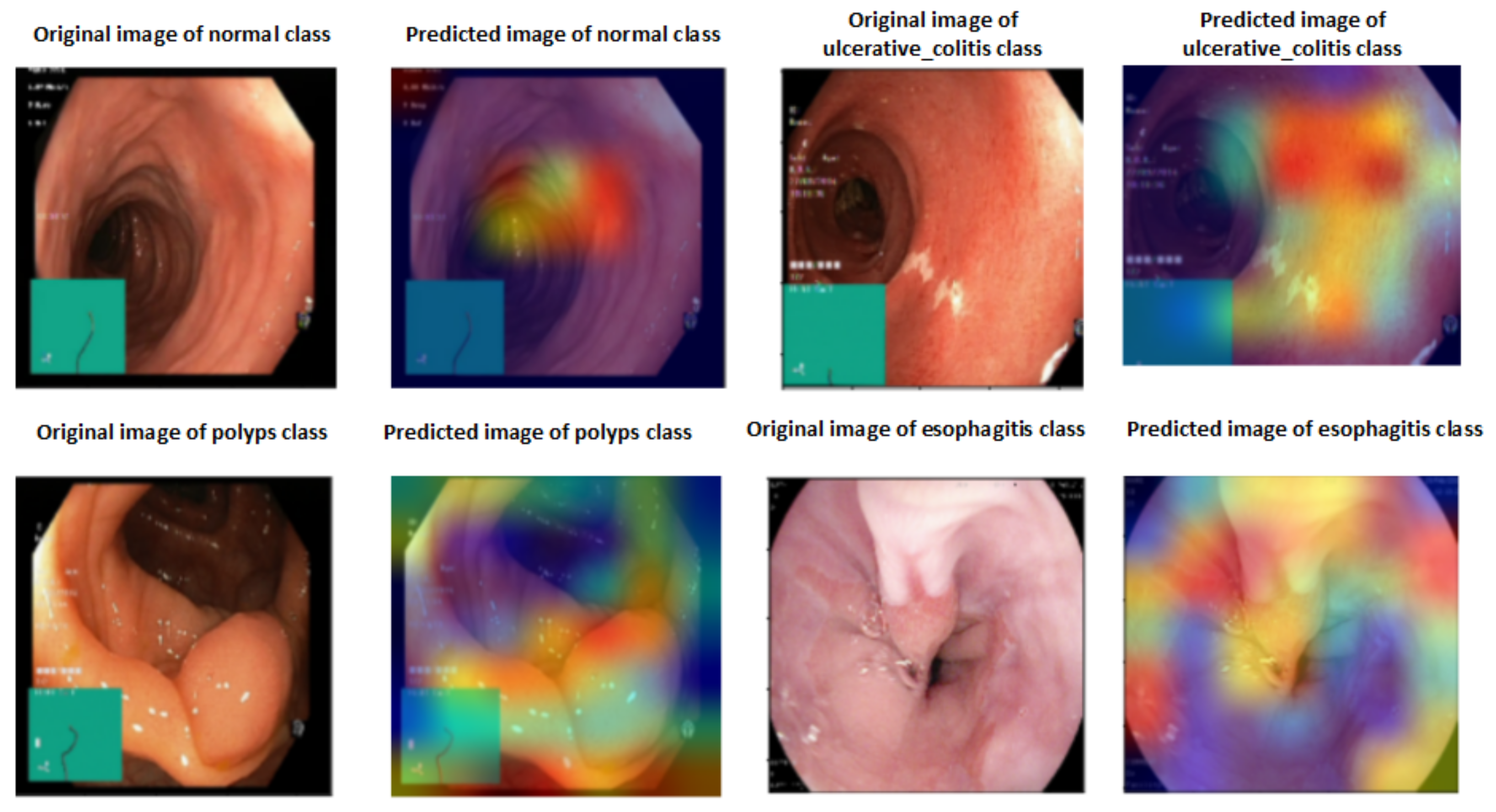
- The WCE colon image dataset collected from Bernal from the Universitat Autonoma de Barcelona [46] includes 6000 images with four classes: normal (N), ulcerative colitis (UC), polyps (P), and esophagitis (E). The dataset is split into 75% training (4500 images) and 25% testing (1200 images).
3.2. Data Augmentation
3.3. Pretrained CNN Models
- VGG16 is one of the first CNN models to achieve high accuracy on the ImageNet dataset, which contains over one million images divided into 1000 categories. VGG16 is made up of 16 layers (13 convolutional and 3 fully linked). Convolutional layers are organized into blocks, each with a predetermined number of layers (e.g., two or three) [49].
- InceptionV3 is an image categorization architecture based on CNN. InceptionV3 is made up of several convolutional layers, pooling layers, and fully connected layers. InceptionV3 includes a stack of convolutional layers, a global average pooling layer, numerous fully connected layers, and a Softmax output layer [50].
- Resnet50 comprises 50 convolutional layers and includes residual connections with shortcuts that help the model better manage the vanishing gradient problem and effectively train deeper architectures. The architecture is divided into stages, each containing a sequence of convolutional blocks and identity blocks. Each convolutional block contains three convolution layers, whereas each identity block only has one. The ResNet50 architecture’s last layer is a fully connected layer that performs classification [51].
- DenseNet121 is a CNN architecture consisting of four layers: the input layer, transition layer, dense block, and output layer. The input layer receives an image or data as input. The transition layers consist of multiple convolutional operations, which reduce the size of feature maps before entering densely connected blocks. Each dense block comprises several sets of batch normalization followed by Relu activation and then a series of 3×3 Conv2d with the same padding to preserve spatial resolution between two consecutive stages in the network, which helps to achieve faster convergence when training models on large datasets [52].
3.4. The Proposed Stacking Ensemble Model
- The pretrained models (VGG16, ResNet50, InceptionV3, and DenseNet121) are trained and saved, then loaded, and all model layers are frozen without the output layers.
- Training stacking combines the output predictions of the training set for each pretrained model. A metalearner (in this case, an SVM) is trained and optimized using stacking. A grid search is used to optimize SVMs as metalearners.
- Testing stacking combines the output predictions of each pretrained model. The metalearner (SVM) is then evaluated using accuracy, precision, recall, F1 score, and ROC analysis.
3.5. Evaluating Models
- Accuracy (ACC), precision (PRE), recall (REC), and F1 score (F1) are the most often-used metrics for classification performance. Equations (1) and (2) illustrate these measures (4).True negative (TN) indicates that an individual is healthy and the test is negative, in contrast to true positive (TP), which indicates that the person is ill and the test is positive. When a test shows positive although the subject is healthy, this is known as a false positive (FP). A false negative (FN) occurs when a person is sick but the test is negative
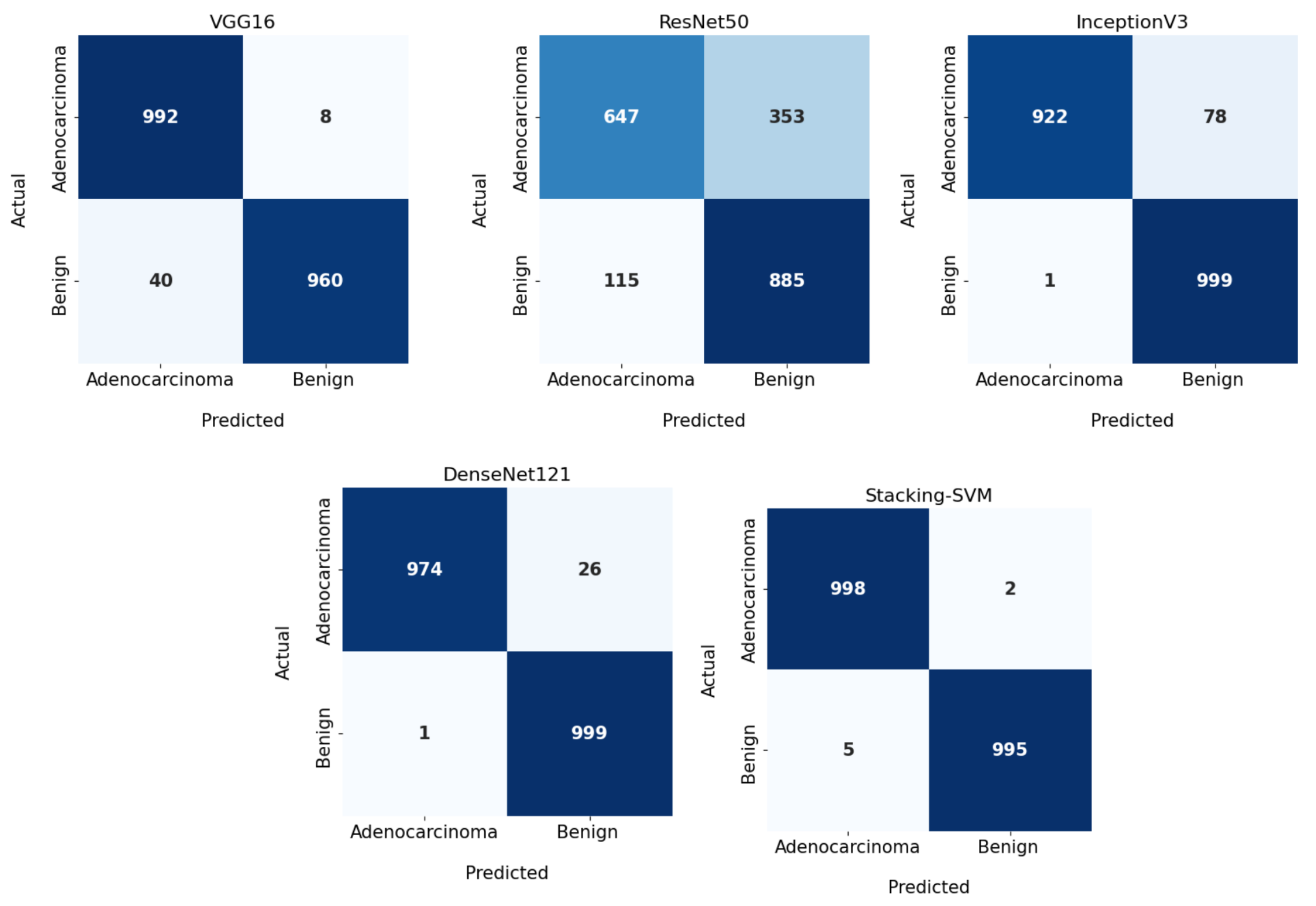
- A confusion matrix (CM) is used to evaluate the performance of models, comprising a table that summarizes an algorithm’s correct and incorrect predictions, with each row representing the actual class and each column representing the anticipated class [55].
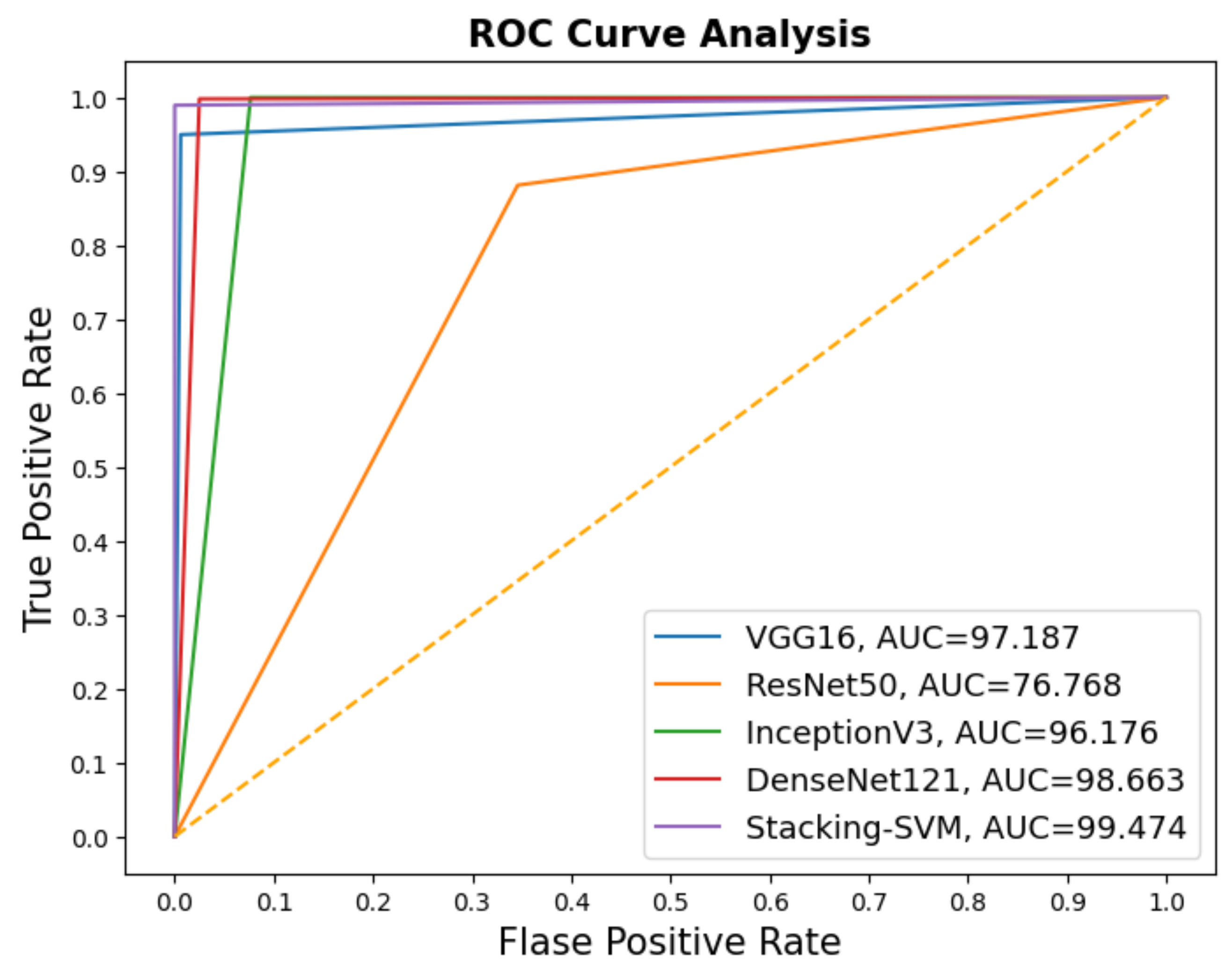
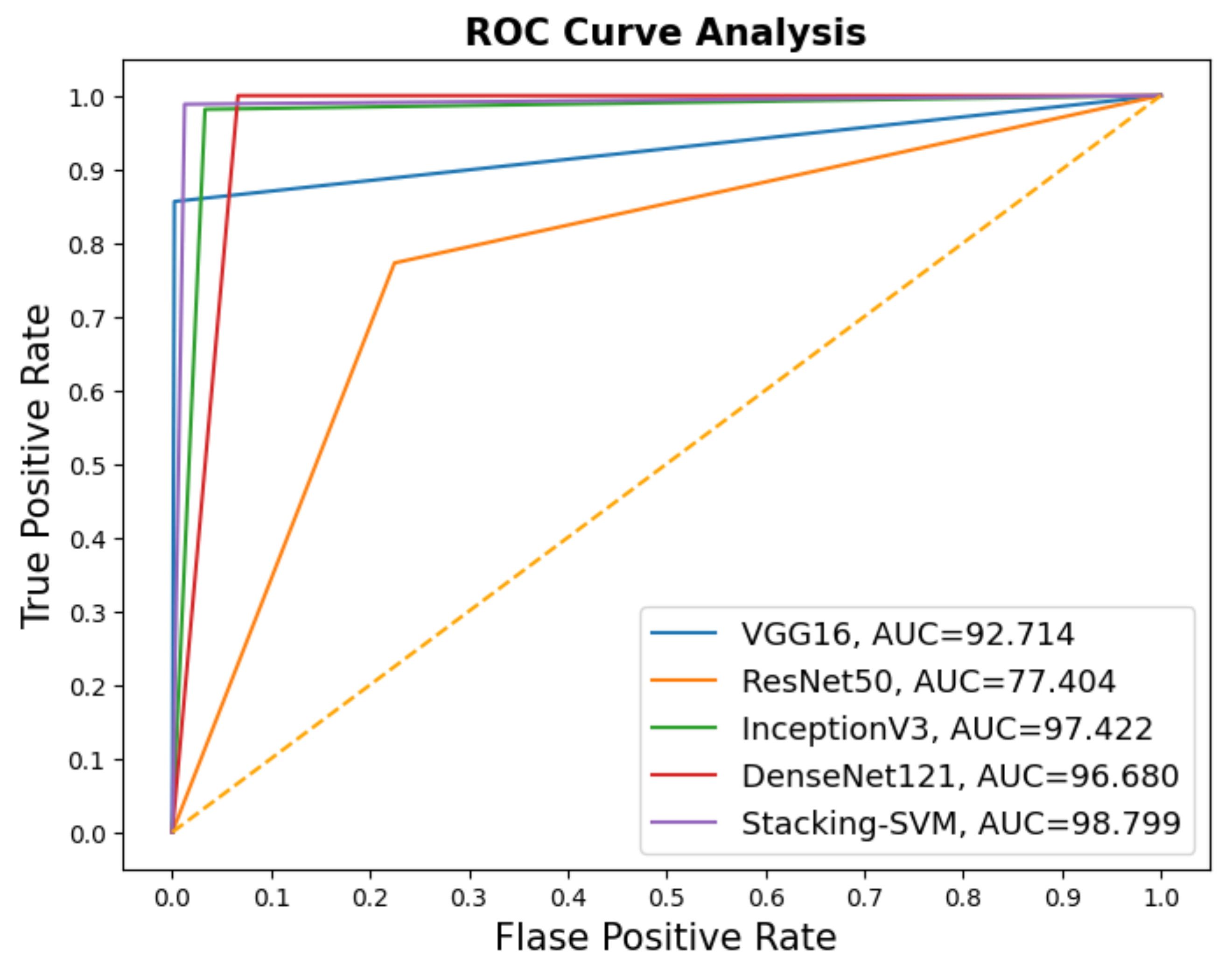
- Receiver operating characteristic (ROC) and area under the curve (AUC) are performance metrics for classification problems. ROC represents a probability curve, whereas AUC represents the degree of separability. By indicating the degree of separation between classes, the model is able to perform well. Models with higher AUCs predict better [56].
4. Experimental Results
4.1. Experimental Setup
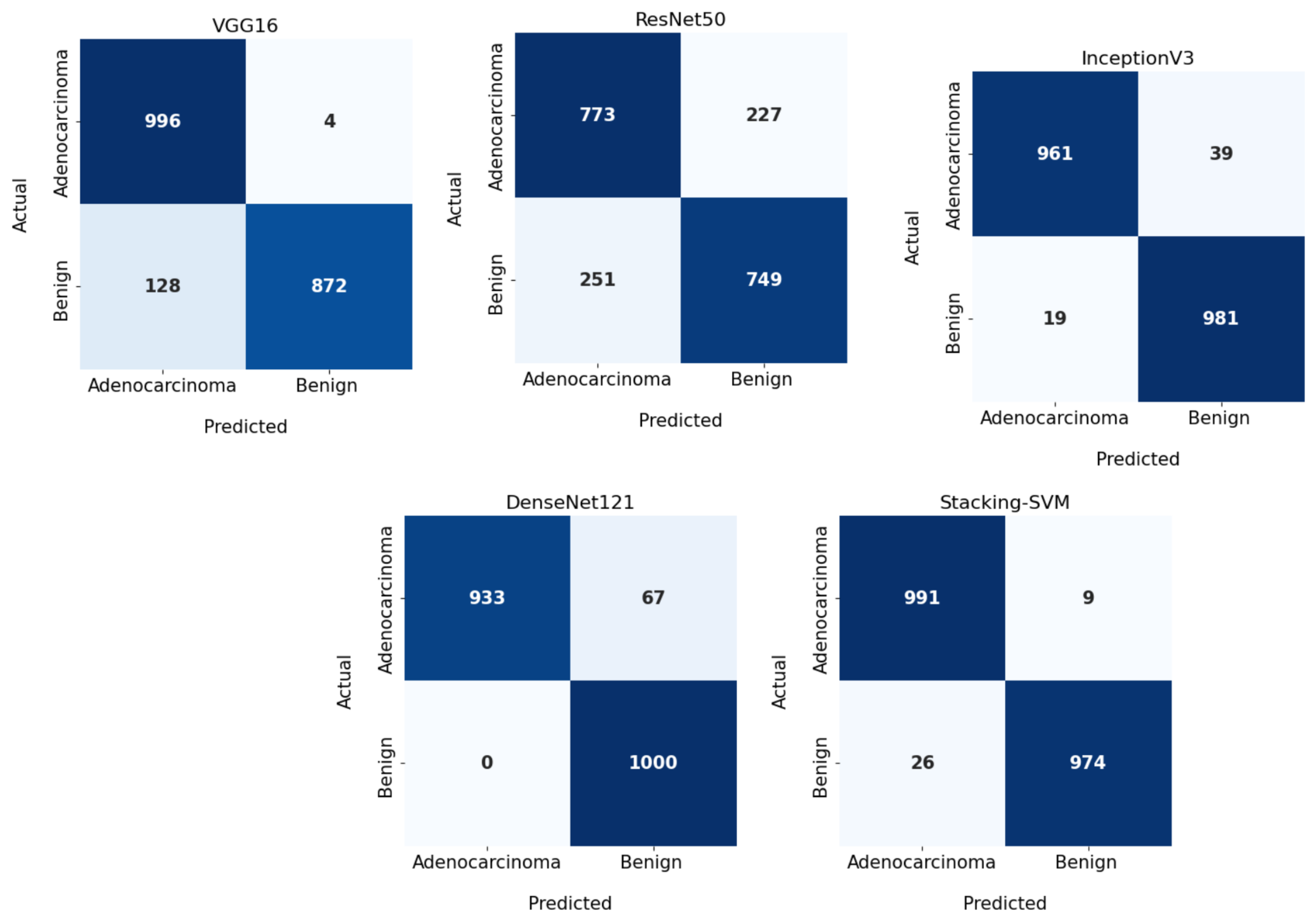
4.2. Performance Analysis of the Pre-Trained CNN and Stacking-SVM Models Using the LC25000 Dataset
4.2.1. Results of Fixed Learning Rate (LR)
4.2.2. Results of Dynamic Learning Rate (LR)
4.3. Performance Analysis of the Pretrained CNN and Stacking-SVM Models Using the WCE Dataset
4.3.1. Results of Fixed Learning Rate
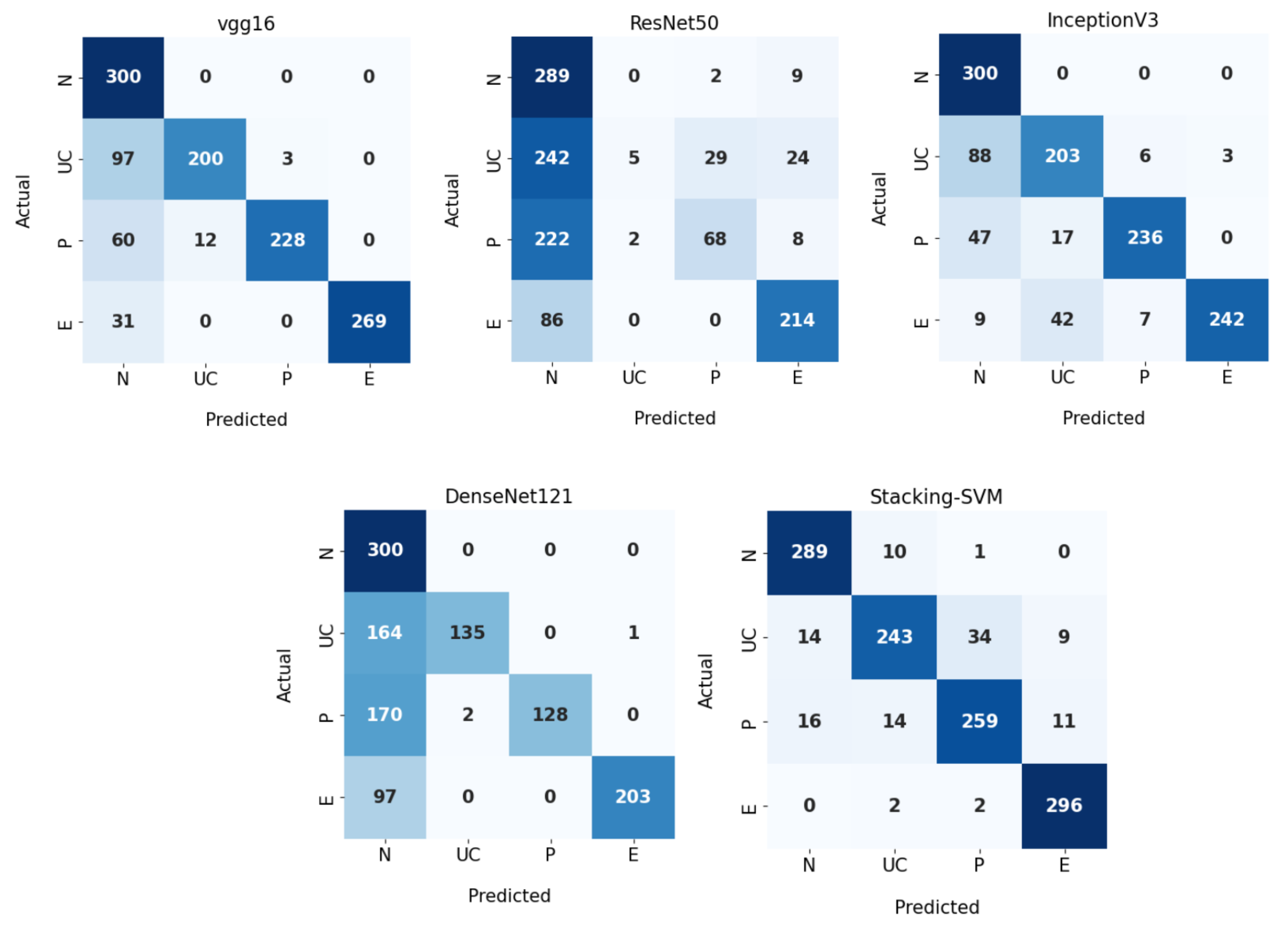
4.3.2. Results of Dynamic Learning Rate
4.4. Discussion
Rate of Model Results with Fixed and Dynamic Learning Rates Using Two Datasets
4.5. Explainable Artificial Intelligence
4.6. Comparison of Model Results with the Literature
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Colorectal Cancer. Available online: https://www.cancer.org (accessed on 5 August 2023).
- Yin, Z.; Yao, C.; Zhang, L.; Qi, S. Application of artificial intelligence in diagnosis and treatment of colorectal cancer: A novel Prospect. Front. Med. 2023, 10, 1128084. [Google Scholar] [CrossRef] [PubMed]
- Nemlander, E.; Ewing, M.; Abedi, E.; Hasselström, J.; Sjövall, A.; Carlsson, A.C.; Rosenblad, A. A machine learning tool for identifying non-metastatic colorectal cancer in primary care. Eur. J. Cancer 2023, 182, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Depciuch, J.; Jakubczyk, P.; Paja, W.; Pancerz, K.; Wosiak, A.; Kula-Maximenko, M.; Yaylım, İ.; Gültekin, G.İ.; Tarhan, N.; Hakan, M.T.; et al. Correlation between human colon cancer specific antigens and Raman spectra. Attempting to use Raman spectroscopy in the determination of tumor markers for colon cancer. Nanomed. Nanotechnol. Biol. Med. 2023, 48, 102657. [Google Scholar] [CrossRef] [PubMed]
- Colorectal Cancer. Available online: https://www.cdc.gov/cancer/uscs/about/data-briefs/no33-colorectal-cancer-incidence-2003-2019.htm (accessed on 5 August 2023).
- What Causes Colon Cancer. Available online: https://my.clevelandclinic.org/health/diseases/14501-colorectal-colon-cancer (accessed on 5 August 2023).
- Chen, Y.W.; Jain, L.C. Deep learning in healthcare. In Paradigms and Applications; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Saleh, H.; Alyami, H.; Alosaimi, W. Predicting breast cancer based on optimized deep learning approach. Comput. Intell. Neurosci. 2022, 2022, 1820777. [Google Scholar] [CrossRef] [PubMed]
- AlMohimeed, A.; Saleh, H.; El-Rashidy, N.; Saad, R.M.; El-Sappagh, S.; Mostafa, S. Diagnosis of COVID-19 Using Chest X-ray Images and Disease Symptoms Based on Stacking Ensemble Deep Learning. Diagnostics 2023, 13, 1968. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; Cheng, Q.; Lu, H.; Li, Q.; Zhang, X.; Qiu, S. Deep learning methods for medical image fusion: A review. In Computers in Biology and Medicine; Elsevier: Amsterdam, The Netherlands, 2023; p. 106959. [Google Scholar]
- Rex, D.K.; Boland, C.R.; Dominitz, J.A.; Giardiello, F.M.; Johnson, D.A.; Kaltenbach, T.; Levin, T.R.; Lieberman, D.; Robertson, D.J. Colorectal cancer screening: Recommendations for physicians and patients from the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology 2017, 153, 307–323. [Google Scholar] [CrossRef] [PubMed]
- Bosman, F.T.; Carneiro, F.; Hruban, R.H.; Theise, N.D. WHO Classification of Tumours of the DIGESTIVE System, 4th ed.; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Even-Sapir, E.; Parag, Y.; Lerman, H.; Gutman, M.; Levine, C.; Rabau, M.; Figer, A.; Metser, U. Detection of recurrence in patients with rectal cancer: PET/CT after abdominoperineal or anterior resection. Radiology 2004, 232, 815–822. [Google Scholar] [CrossRef]
- Saxena, S.; Gyanchandani, M. Machine learning methods for computer-aided breast cancer diagnosis using histopathology: A narrative review. J. Med. Imaging Radiat. Sci. 2020, 51, 182–193. [Google Scholar] [CrossRef]
- Hamida, A.B.; Devanne, M.; Weber, J.; Truntzer, C.; Derangère, V.; Ghiringhelli, F.; Forestier, G.; Wemmert, C. Deep learning for colon cancer histopathological images analysis. Comput. Biol. Med. 2021, 136, 104730. [Google Scholar] [CrossRef]
- Tasnim, Z.; Chakraborty, S.; Shamrat, F.; Chowdhury, A.N.; Nuha, H.A.; Karim, A.; Zahir, S.B.; Billah, M.M. Deep learning predictive model for colon cancer patient using CNN-based classification. Int. J. Adv. Comput. Sci. Appl. 2021, 12, 687–696. [Google Scholar] [CrossRef]
- Chen, Y. Convolutional Neural Network for Sentence Classification. Master’s Thesis, University of Waterloo, Waterloo, ON, Canada, 2015. [Google Scholar]
- Naranjo-Torres, J.; Mora, M.; Hernández-García, R.; Barrientos, R.J.; Fredes, C.; Valenzuela, A. A review of convolutional neural network applied to fruit image processing. Appl. Sci. 2020, 10, 3443. [Google Scholar] [CrossRef]
- Bhatt, D.; Patel, C.; Talsania, H.; Patel, J.; Vaghela, R.; Pandya, S.; Modi, K.; Ghayvat, H. CNN variants for computer vision: History, architecture, application, challenges and future scope. Electronics 2021, 10, 2470. [Google Scholar] [CrossRef]
- Ghaderzadeh, M.; Aria, M.; Hosseini, A.; Asadi, F.; Bashash, D.; Abolghasemi, H. A fast and efficient CNN model for B-ALL diagnosis and its subtypes classification using peripheral blood smear images. Int. J. Intell. Syst. 2022, 37, 5113–5133. [Google Scholar] [CrossRef]
- Ghaderzadeh, M.; Asadi, F.; Jafari, R.; Bashash, D.; Abolghasemi, H.; Aria, M. Deep convolutional neural network–based computer-aided detection system for COVID-19 using multiple lung scans: Design and implementation study. J. Med. Internet Res. 2021, 23, e27468. [Google Scholar] [CrossRef] [PubMed]
- Kugunavar, S.; Prabhakar, C. Convolutional neural networks for the diagnosis and prognosis of the coronavirus disease pandemic. Vis. Comput. Ind. Biomed. Art 2021, 4, 12. [Google Scholar] [CrossRef]
- Yadav, S.S.; Jadhav, S.M. Deep convolutional neural network based medical image classification for disease diagnosis. J. Big Data 2019, 6, 113. [Google Scholar] [CrossRef]
- Babu, T.; Singh, T.; Gupta, D.; Hameed, S. Colon cancer prediction on histological images using deep learning features and Bayesian optimized SVM. J. Intell. Fuzzy Syst. 2021, 41, 5275–5286. [Google Scholar] [CrossRef]
- Garg, S.; Garg, S. Prediction of lung and colon cancer through analysis of histopathological images by utilizing Pre-trained CNN models with visualization of class activation and saliency maps. In Proceedings of the 2020 3rd Artificial Intelligence and Cloud Computing Conference, Kyoto, Japan, 18–20 December 2020; pp. 38–45. [Google Scholar]
- Gheisari, M.; Ebrahimzadeh, F.; Rahimi, M.; Moazzamigodarzi, M.; Liu, Y.; Dutta Pramanik, P.K.; Heravi, M.A.; Mehbodniya, A.; Ghaderzadeh, M.; Feylizadeh, M.R.; et al. Deep learning: Applications, architectures, models, tools, and frameworks: A comprehensive survey. CAAI Trans. Intell. Technol. 2023. [Google Scholar] [CrossRef]
- Hastie, T.; Tibshirani, R.; Friedman, J.H.; Friedman, J.H. The Elements of Statistical Learning: Data Mining, Inference, and Prediction; Springer: Berlin/Heidelberg, Germany, 2009; Volume 2. [Google Scholar]
- Sagi, O.; Rokach, L. Ensemble learning: A survey. Wiley Interdiscip. Rev. Data Min. Knowl. Discov. 2018, 8, e1249. [Google Scholar] [CrossRef]
- Younas, F.; Usman, M.; Yan, W.Q. A deep ensemble learning method for colorectal polyp classification with optimized network parameters. Appl. Intell. 2023, 53, 2410–2433. [Google Scholar] [CrossRef]
- Häfner, M.; Tamaki, T.; Tanaka, S.; Uhl, A.; Wimmer, G.; Yoshida, S. Local fractal dimension based approaches for colonic polyp classification. Med. Image Anal. 2015, 26, 92–107. [Google Scholar] [CrossRef] [PubMed]
- Wimmer, G.; Tamaki, T.; Tischendorf, J.J.; Häfner, M.; Yoshida, S.; Tanaka, S.; Uhl, A. Directional wavelet based features for colonic polyp classification. Med. Image Anal. 2016, 31, 16–36. [Google Scholar] [CrossRef] [PubMed]
- Shin, Y.; Balasingham, I. Comparison of hand-craft feature based SVM and CNN based deep learning framework for automatic polyp classification. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju Island, Republic of Korea, 11–15 July 2017; pp. 3277–3280. [Google Scholar]
- Liew, W.S.; Tang, T.B.; Lin, C.H.; Lu, C.K. Automatic colonic polyp detection using integration of modified deep residual convolutional neural network and ensemble learning approaches. Comput. Methods Programs Biomed. 2021, 206, 106114. [Google Scholar] [CrossRef]
- Shaban, M.; Awan, R.; Fraz, M.M.; Azam, A.; Tsang, Y.W.; Snead, D.; Rajpoot, N.M. Context-aware convolutional neural network for grading of colorectal cancer histology images. IEEE Trans. Med. Imaging 2020, 39, 2395–2405. [Google Scholar] [CrossRef] [PubMed]
- Sikder, J.; Das, U.K.; Chakma, R.J. Supervised learning-based cancer detection. Int. J. Adv. Comput. Sci. Appl. 2021, 12, 863–869. [Google Scholar] [CrossRef]
- Hasan, I.; Ali, S.; Rahman, H.; Islam, K. Automated Detection and Characterization of Colon Cancer with Deep Convolutional Neural Networks. J. Healthc. Eng. 2022, 2022, 5269913. [Google Scholar] [CrossRef]
- Jansen-Winkeln, B.; Barberio, M.; Chalopin, C.; Schierle, K.; Diana, M.; Köhler, H.; Gockel, I.; Maktabi, M. Feedforward artificial neural network-based colorectal cancer detection using hyperspectral imaging: A step towards automatic optical biopsy. Cancers 2021, 13, 967. [Google Scholar] [CrossRef] [PubMed]
- Hage Chehade, A.; Abdallah, N.; Marion, J.M.; Oueidat, M.; Chauvet, P. Lung and colon cancer classification using medical imaging: A feature engineering approach. Phys. Eng. Sci. Med. 2022, 45, 729–746. [Google Scholar] [CrossRef]
- Masud, M.; Sikder, N.; Nahid, A.A.; Bairagi, A.K.; AlZain, M.A. A machine learning approach to diagnosing lung and colon cancer using a deep learning-based classification framework. Sensors 2021, 21, 748. [Google Scholar] [CrossRef]
- Raju, M.S.N.; Rao, B.S. Classification of Colon Cancer through analysis of histopathology images using Transfer Learning. In Proceedings of the 2022 IEEE 2nd International Symposium on Sustainable Energy, Signal Processing and Cyber Security (iSSSC), Gunupur, India, 15–17 December 2022; pp. 1–6. [Google Scholar]
- Dwivedi, A.K.; Srivastava, G.; Pradhan, N. NFF: A Novel Nested Feature Fusion Method for Efficient and Early Detection of Colorectal Carcinoma. In Proceedings of the 4th International Conference on Computer and Communication Technologies, Haldia, India, 1–3 March 2023; pp. 297–309. [Google Scholar]
- Yogapriya, J.; Chandran, V.; Sumithra, M.; Anitha, P.; Jenopaul, P.; Suresh Gnana Dhas, C. Gastrointestinal tract disease classification from wireless endoscopy images using pretrained deep learning model. Comput. Math. Methods Med. 2021, 2021, 5940433. [Google Scholar] [CrossRef]
- Sharma, P.; Balabantaray, B.K.; Bora, K.; Mallik, S.; Kasugai, K.; Zhao, Z. An ensemble-based deep convolutional neural network for computer-aided polyps identification from colonoscopy. Front. Genet. 2022, 13, 844391. [Google Scholar] [CrossRef] [PubMed]
- Albuquerque, C.; Henriques, R.; Castelli, M. A stacking-based artificial intelligence framework for an effective detection and localization of colon polyps. Sci. Rep. 2022, 12, 17678. [Google Scholar] [CrossRef] [PubMed]
- Borkowski, A.A.; Bui, M.M.; Thomas, L.B.; Wilson, C.P.; DeLand, L.A.; Mastorides, S.M. LC25000 Lung and colon histopathological image dataset. arXiv 2021, arXiv:1912.12142. [Google Scholar]
- Montalbo, F.J.P. Diagnosing gastrointestinal diseases from endoscopy images through a multi-fused CNN with auxiliary layers, alpha dropouts, and a fusion residual block. Biomed. Signal Process. Control 2022, 76, 103683. [Google Scholar] [CrossRef]
- Yang, S.; Xiao, W.; Zhang, M.; Guo, S.; Zhao, J.; Shen, F. Image data augmentation for deep learning: A survey. arXiv 2022, arXiv:2204.08610. [Google Scholar]
- Chlap, P.; Min, H.; Vandenberg, N.; Dowling, J.; Holloway, L.; Haworth, A. A review of medical image data augmentation techniques for deep learning applications. J. Med. Imaging Radiat. Oncol. 2021, 65, 545–563. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the inception architecture for computer vision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Radwan, N. Leveraging Sparse and Dense Features for Reliable STATE Estimation in Urban Environments. Ph.D. Thesis, University of Freiburg, Freiburg im Breisgau, Germany, 2019. [Google Scholar]
- Dietterich, T.G. Ensemble methods in machine learning. In Proceedings of the Multiple Classifier Systems: First International Workshop, MCS 2000, Cagliari, Italy, 21–23 June 2000; pp. 1–15. [Google Scholar]
- Rajagopal, S.; Kundapur, P.P.; Hareesha, K.S. A stacking ensemble for network intrusion detection using heterogeneous datasets. Secur. Commun. Netw. 2020, 2020, 4586875. [Google Scholar] [CrossRef]
- Liang, J. Confusion matrix: Machine learning. POGIL Act. Clgh. 2022, 3. [Google Scholar]
- Narkhede, S. Understanding auc-roc curve. Towards Data Sci. 2018, 26, 220–227. [Google Scholar]
- Tenserflow. Available online: https://www.tensorflow.org/ (accessed on 5 August 2023).
- Keras. Available online: https://keras.io/ (accessed on 5 August 2023).
- Anaconda. Available online: https://www.anaconda.com/ (accessed on 5 August 2023).
- Selvaraju, R.R.; Das, A.; Vedantam, R.; Cogswell, M.; Parikh, D.; Batra, D. Grad-CAM: Why did you say that? arXiv 2016, arXiv:1611.07450. [Google Scholar]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model | Class | PRE | REC | F1 |
|---|---|---|---|---|
| VGG16 | Benign | 96 | 99 | 98 |
| Adenocarcinomas | 99 | 96 | 98 | |
| Average | 98 | 98 | 98 | |
| ResNet50 | Benign | 85 | 65 | 73 |
| Adenocarcinomas | 71 | 89 | 79 | |
| Average | 78 | 77 | 76 | |
| InceptionV3 | Benign | 100 | 92 | 96 |
| Adenocarcinomas | 93 | 100 | 96 | |
| Average | 96 | 96 | 96 | |
| DenseNet121 | Benign | 100 | 97 | 99 |
| Adenocarcinomas | 97 | 100 | 99 | |
| Average | 99 | 99 | 99 | |
| Stacking-SVM | Benign | 100 | 100 | 100 |
| Adenocarcinomas | 100 | 100 | 100 | |
| Average | 100 | 100 | 100 |
| Model | Class | PRC | REC | F1 |
|---|---|---|---|---|
| VGG16 | Benign | 89 | 100 | 94 |
| Adenocarcinomas | 100 | 87 | 93 | |
| Average | 94 | 93 | 93 | |
| ResNet50 | Benign | 75 | 77 | 76 |
| Adenocarcinomas | 77 | 75 | 76 | |
| Average | 76 | 76 | 76 | |
| InceptionV3 | Benign | 98 | 96 | 97 |
| Adenocarcinomas | 96 | 98 | 97 | |
| Average | 97 | 97 | 97 | |
| DenseNet121 | Benign | 100 | 93 | 97 |
| Adenocarcinomas | 94 | 100 | 97 | |
| Average | 97 | 97 | 97 | |
| Stacking-SVM | Benign | 97 | 99 | 98 |
| Adenocarcinomas | 99 | 97 | 98 | |
| Average | 98 | 98 | 98 |
| Model | Class | PRE | REC | F1 |
|---|---|---|---|---|
| VGG16 | N | 95 | 99 | 97 |
| UC | 96 | 81 | 88 | |
| P | 90 | 92 | 91 | |
| E | 92 | 100 | 96 | |
| Average | 93 | 93 | 93 | |
| ResNet50 | N | 43 | 99 | 60 |
| UC | 78 | 05 | 09 | |
| P | 73 | 11 | 19 | |
| E | 65 | 96 | 77 | |
| Average | 65 | 53 | 41 | |
| InceptionV3 | N | 72 | 100 | 84 |
| UC | 81 | 85 | 83 | |
| P | 99 | 67 | 80 | |
| E | 100 | 89 | 94 | |
| Average | 88 | 85 | 85 | |
| DenseNet121 | N | 98 | 100 | 99 |
| UC | 77 | 100 | 87 | |
| P | 100 | 71 | 83 | |
| E | 99 | 96 | 98 | |
| Average | 93 | 92 | 92 | |
| Stacking-SVM | N | 100 | 99 | 100 |
| UC | 100 | 86 | 92 | |
| P | 88 | 100 | 93 | |
| E | 99 | 100 | 99 | |
| Average | 97 | 96 | 96 |
| Model | Class | PRE | REC | F1 |
|---|---|---|---|---|
| VGG16 | N | 61 | 100 | 76 |
| UC | 94 | 67 | 78 | |
| P | 99 | 76 | 86 | |
| E | 100 | 90 | 95 | |
| Average | 89 | 83 | 84 | |
| ResNet50 | N | 34 | 95 | 51 |
| UC | 71 | 02 | 03 | |
| P | 69 | 23 | 34 | |
| E | 84 | 71 | 77 | |
| Average | 65 | 48 | 41 | |
| InceptionV3 | N | 68 | 100 | 81 |
| UC | 77 | 68 | 72 | |
| P | 95 | 79 | 86 | |
| E | 99 | 81 | 89 | |
| Average | 85 | 82 | 82 | |
| DenseNet121 | N | 41 | 100 | 58 |
| UC | 99 | 45 | 62 | |
| P | 100 | 43 | 60 | |
| E | 100 | 68 | 81 | |
| Average | 85 | 64 | 65 | |
| Stacking-SVM | N | 91 | 96 | 93 |
| UC | 90 | 81 | 85 | |
| P | 88 | 86 | 87 | |
| E | 94 | 99 | 96 | |
| Average | 91 | 91 | 91 |
| Ref. | DL Architecture | Dataset(s) | Results (%) |
|---|---|---|---|
| [35] | VGG-16, Resnet-50, SVM | LC25000 | ACC = 93 |
| [36] | DeepCNN | LC25000 | ACC = 99.80, REC = 99.87, F1 = 99.87 |
| [38] | XGBoost | LC25000 | ACC = 99 |
| [16] | MobileNetV2 | LC25000 | ACC = 99 |
| [39] | CNN | LC25000 | ACC = 96.33 |
| [40] | CNN | LC25000 | ACC = 99.98 |
| [25] | NASNetMobile | LC25000 | ACC = 98, PRE = 98, REC = 98, and F1 = 98 |
| [41] | EfficientNet | WCE dataset | ACC = 94.11 |
| [42] | VGG16 | WCE dataset | ACC = 96.33 |
| [29] | the weighted ensemble model | UCI and PICCOLO | ACC = 96.3, PRE = 95.5, REC = 97.2, F1 = 96.3 |
| Our work | Stacking-SVM | LC25000 | ACC = 100, PRE = 100, REC = 100, F1 = 100 |
| Our work | Stacking-SVM | WCE | ACC = 98, PRE = 98, REC = 98, F1 = 98 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gabralla, L.A.; Hussien, A.M.; AlMohimeed, A.; Saleh, H.; Alsekait, D.M.; El-Sappagh, S.; Ali, A.A.; Refaat Hassan, M. Automated Diagnosis for Colon Cancer Diseases Using Stacking Transformer Models and Explainable Artificial Intelligence. Diagnostics 2023, 13, 2939. https://doi.org/10.3390/diagnostics13182939
Gabralla LA, Hussien AM, AlMohimeed A, Saleh H, Alsekait DM, El-Sappagh S, Ali AA, Refaat Hassan M. Automated Diagnosis for Colon Cancer Diseases Using Stacking Transformer Models and Explainable Artificial Intelligence. Diagnostics. 2023; 13(18):2939. https://doi.org/10.3390/diagnostics13182939
Chicago/Turabian StyleGabralla, Lubna Abdelkareim, Ali Mohamed Hussien, Abdulaziz AlMohimeed, Hager Saleh, Deema Mohammed Alsekait, Shaker El-Sappagh, Abdelmgeid A. Ali, and Moatamad Refaat Hassan. 2023. "Automated Diagnosis for Colon Cancer Diseases Using Stacking Transformer Models and Explainable Artificial Intelligence" Diagnostics 13, no. 18: 2939. https://doi.org/10.3390/diagnostics13182939