
Deep Learning-Based Classification of Chest Diseases Using X-rays, CT Scans, and Cough Sound Images
 , ,
, ,  ,
,  , and
, and 
Abstract
:1. Introduction
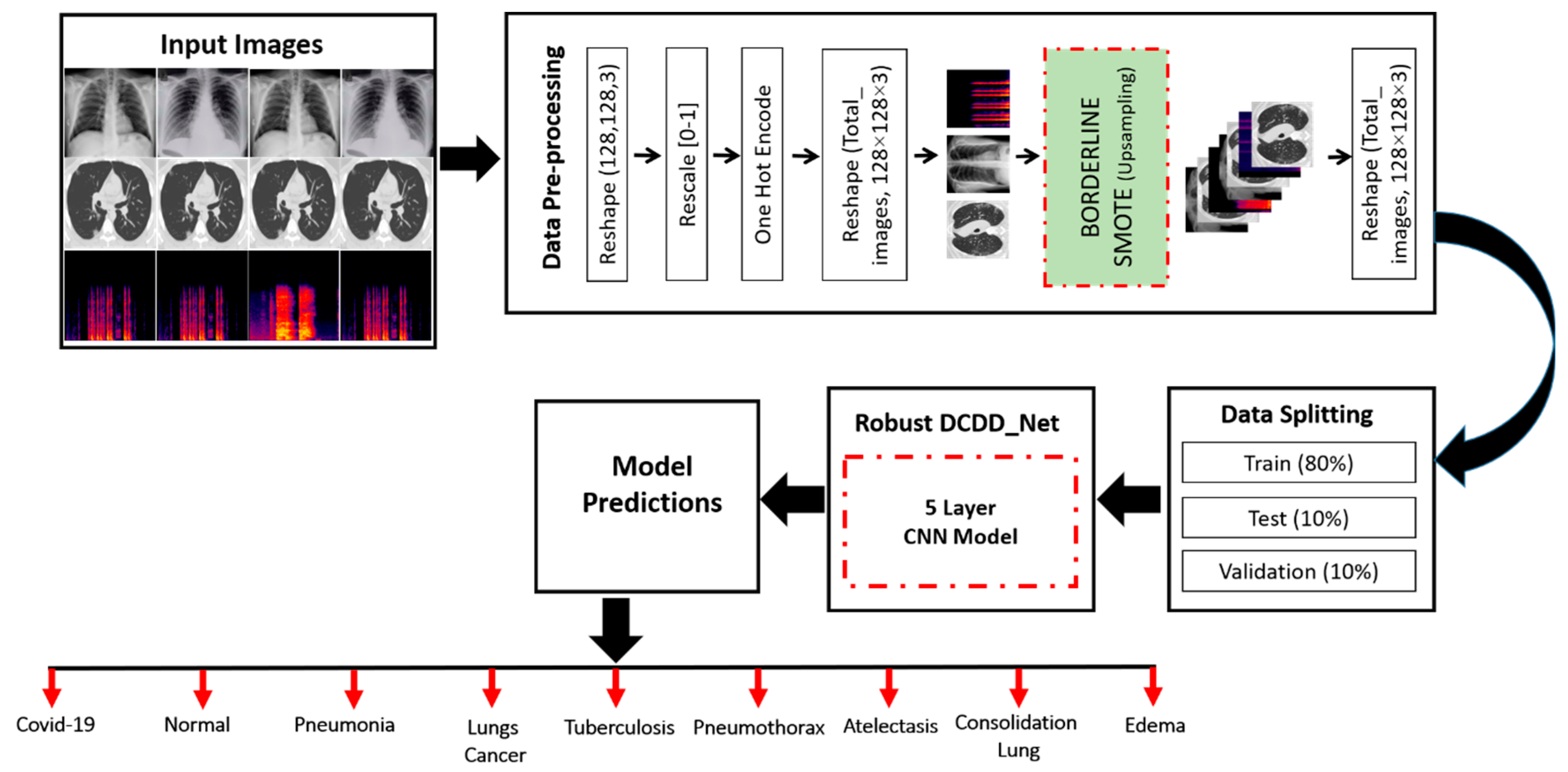
- The novel DCDD_Net model that is suggested is intended to diagnose each of the nine distinct forms of chest disease. The model that is proposed can extract dominating features from CXT, CT scans, and cough sound images, which can be of assistance in providing an accurate diagnosis of chest diseases.
- The scalogram method was used to convert the cough sounds into an image.
- For this work, we simplified the model by cutting down on the total number of trainable parameters to produce a reliable classifier.
- As a result of the issue of class imbalance that exists in CXT, CT scans, and cough sound image datasets, the accuracy of the DCDD_Net model was significantly reduced. We circumvented this problem by employing an upsampling strategy known as BL-SMOTE, which allowed us to collect mixture samples of the image at each class to achieve greater accuracy.
- The suggested DCDD_Net model achieved superior results in comparison to four baseline classifiers, namely, InceptionResNet-V2, EfficientNet-B0, DenseNet-201, and Xception, in terms of numerous assessment measures, including accuracy, area under the curve (AUC), precision, recall, loss, and F1 score.
- Additionally, when compared to the most recent state-of-the-art (SOTA) classifiers, the suggested DCDD_Net model provided results that were both significant and notable.
2. Literature Review
2.1. Deep Learning Models for Chest Disease Classification Using Chest X-rays and CT Scans
2.2. Deep Learning Models for Chest Disease Classification Using Cough Sounds

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Year | Models | Diseases | Types | Accuracy | Strength | Weakness |
|---|---|---|---|---|---|---|---|
| [15] | 2023 | CBAMWDnet | TB and normal | CXR | 98.80% | The model was suitable for TB and normal case classification using CXR. | The model was trained and tested on imbalanced datasets. |
| [16] | 2023 | COVID-CheXNET | COVID-19 and normal | CXR | 92.99% | The model was trained on the chest X-ray dataset and achieved remarkable results in classifying COVID-19 patients. | No augmentation method was used and datasets required an image enhancement process due to the poor quality of CXR. |
| [17] | 2023 | CDC_Net | COVID-19, PNEUTH, PNEU, LC, and TB | CXR | 90.39% | The model could classify five different chest diseases. | There was a gradient-boosting issue. |
| [19] | 2023 | CNN | COVID-19, fibrosis, and TB | CXR | 93.85% | The model was appropriate for classifying COVID-19, TB, and fibrosis using CXR. | Pre-processing of the dataset was not performed. |
| [20] | 2023 | ResNet-50, ResNet-101, ResNet-121, DenseNet-169, and Inception-V3 | COVID-19, non- COVID-19 (viral and bacterial PNE) and normal | CXR | 96.6% | Different pre-trained models were used for evaluating the COVID-19 cases. | Even having a very extensive ResNet did not ensure that all residual blocks would be included in the operations. |
| [21] | 2023 | VGG-19, ResNet-50, MobileNet-V2, Inception-V3, Xception, DenseNet-121, Dark COVIDNet, and COVID-Net | COVID-19, non- COVID-19, and PNEU | CXR | 86.13% | Several transfer learning models were used to identify COVID-19 and pneumonia-infected CXR. | The datasets were imbalanced. |
| [23] | 2023 | DCNN | COVID-19 and normal | CXR | 99.10% | A deep-layer network model was designed for COVID-19 classification. | The model was trained and tested on very few image samples. |
| [30] | 2023 | ResNet-50 and DNN | COVID-19 and healthy | Cough Sound | 96.00% | A neural network and a pre-trained model were used to identify COVID-19 using cough sound images. | No noise removal method was applied. |
| [36] | 2023 | DAvoU-Net + ResNet-50 | TB and normal | CT scan | 81.19% | Ensembling of DavoU-Net + ResNet-50 was used for image segmentation and classification of TB and normal. | The study did not focus on the CT scan slices. |
| [42] | 2023 | GoogleNet, AlexNet, ResNet, and DCNN | PNEU, TB, and COVID-19 | CT scan | 96.6% | Several well-renowned models were tested for the identification of pneumonia, TB, and COVID-19. | The datasets were imbalanced. |
| [13] | 2022 | TBXNet | COVID-19, normal, PNEU, and TB | CXR | 95.10% | A significant TBXNet was developed for TB case classification. | The datasets were imbalanced. |
| [29] | 2022 | CNN, LSTM, and ResNet-50 | TB, COVID-19, and healthy | Cough Sound | 92.59% | A concoction of CNN with LSTM and a pre-trained model were used to find TB and COVID-19 disease classification. | LSTMs are prone to overfitting and it was difficult to apply the dropout algorithm to curb this issue. |
| [31] | 2022 | DNN | COVID-19 and healthy | Cough Sound | 97.5% | A deep neural network model was used for COVID-19 using cough sounds. | There was a gradient-boosting issue. |
| [34] | 2022 | CNN | COVID-19 and non-COVID-19 | Cough Sound | 98.50% | A CNN-based model was designed for COVID-19 cases. | There was an increasing gradient and overfitting problem. |
| [35] | 2022 | DL + CBIR | LC and TB | CT scan | 94.7% | A combination of DL with CBIR was used to extract significant information from CT scans for LC and TB case classification. | A semantic gap existed that may have affected the classification performance. |
| [38] | 2022 | GoogleNet + ResNet-50 | COVID-19, PNEU, and normal | CT scan | 99.9% | A combination of two transfer learning models was used for COVID-19, PNEU, and normal cases. | Data validation was not performed. |
| [39] | 2022 | P-DenseCOVNet | COVID-19, PNEU, and normal | CT scan | 87.51% | A dense network was developed for COVID-19, PNEU, and normal classification. | There was a gradient-boosting issue. |
| [40] | 2022 | Federate Learning VGG-16 | COVID-19, LC, and normal | CT scan | 79.32% | A secure model was designed for data sharing. | Disease classification was not focused on. |
| [12] | 2021 | EfficientNet, GoogleNet, and XceptionNet | COVID-19, PNEU, and TB | CXR | 99.21% | Pre-trained models were used for lung disease classification. | There was a lack of interpretability. |
| [18] | 2021 | DenseNet-101, VGG-16, and ResNet-18 | COVID-19, PNEU, normal, and TB | CXR | 98.90% | A deep-layered model was designed for COVID-19 cases. | The models were trained and tested on a limited dataset. |
| [22] | 2021 | AlexNet | COVID-19, non- COVID-19 (viral and bacterial PNE), and healthy | CXR | 93.42% | The proposed model was designed for bacterial and viral pneumonia. | The datasets were imbalanced. |
| [32] | 2021 | ResNet-18, GoogleNet, ResNet-50, ResNet-101, MobileNetV2, and NasNetMobile | COVID-19 and healthy | Cough Sound | 94.90% | Several pre-trained models were tested to discover COVID-19 cases using cough sounds. | No noise removal methods were used. The time frame of the cough sounds was not considered. |
| [33] | 2021 | CNN | COVID-19 vs. non-COVID-19 | Cough Sound | 74.9% | A simple CNN model was used for COVID-19 classification using sounds. | No pre-processing methods were used. |
| [43] | 2021 | DCNN | COVID-positive and COVID-negative | CT scan | 93.24% | A deep network was developed for COVID-19 cases. | A very limited dataset was used. |
| [45] | 2021 | VGG-16 and ResNet-50 | COVID-19, PNEU, and normal | CT scan | 88.52% | VGG-16 and ResNet-50 were integrated for COVID-19 using CT scan. | CT scan images were not pre-processed before being applied to training the model. |
| [46] | 2021 | CNN | COVID-19 vs. non-COVID-19 | CT scan | 96% | A 6-layer CNN model was developed for lung disease classification. | Few image samples were used. |
| [37] | 2020 | AlexNet + KNN | LC and normal | CT scan | 98.74% | The proposed model was combined with KNN for lung cancer classification. | The normal class had more images than the LC class, which affected the model performance. |
| [41] | 2020 | AI | COVID-19, PNEU, TB, and normal | CT scan | 99.4% | A computer-assisted model was developed for several chest diseases. | There was a lack of training data, imbalanced data, and interpretability of data. |
3. Materials and Methods
3.1. Proposed Model for the Diagnosis of Chest Diseases
3.2. Dataset Description
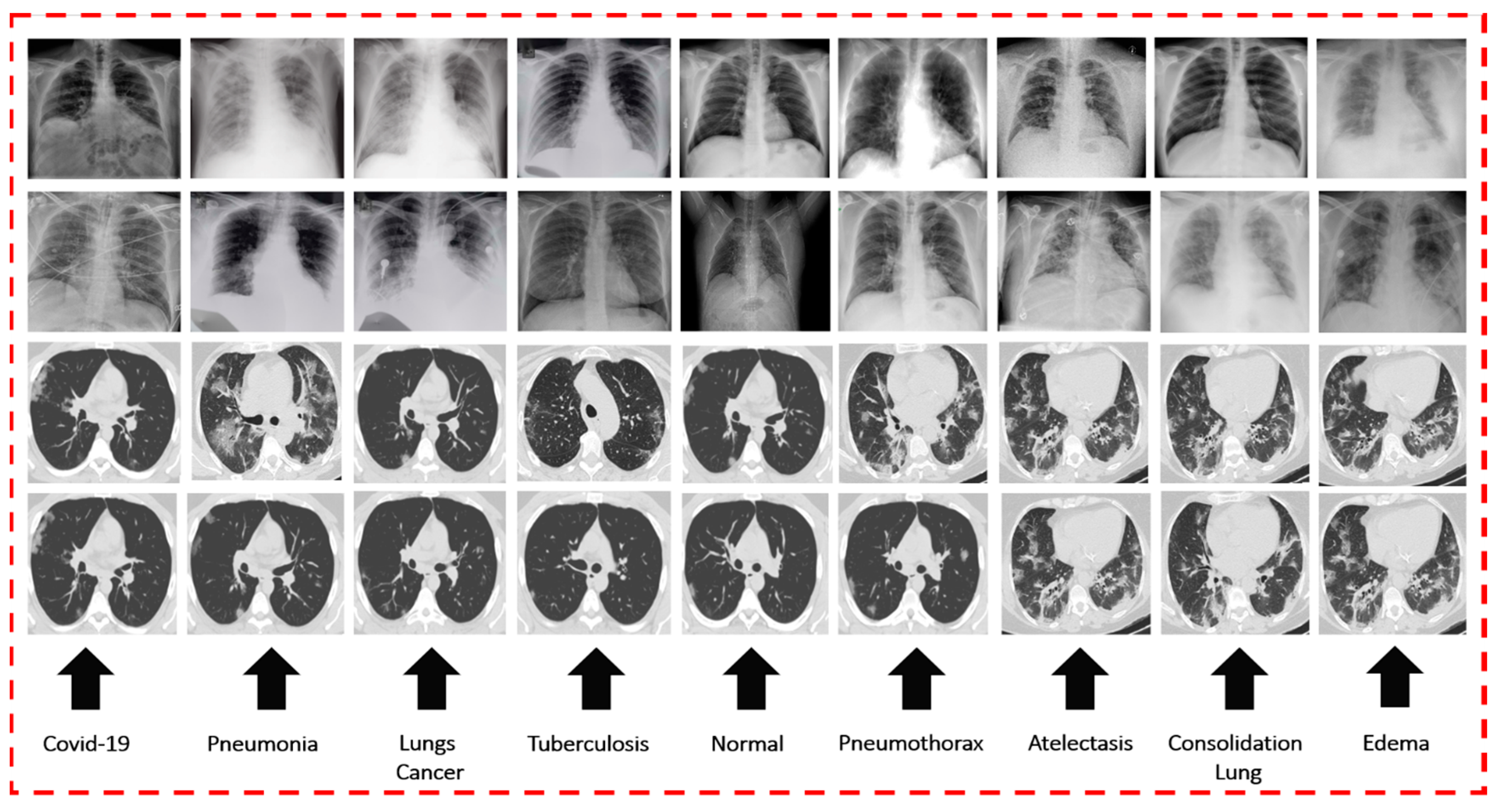
3.2.1. Dataset of CXR and CT Scan Images for Chest Diseases
3.2.2. Dataset of Cough Sounds for Chest Diseases
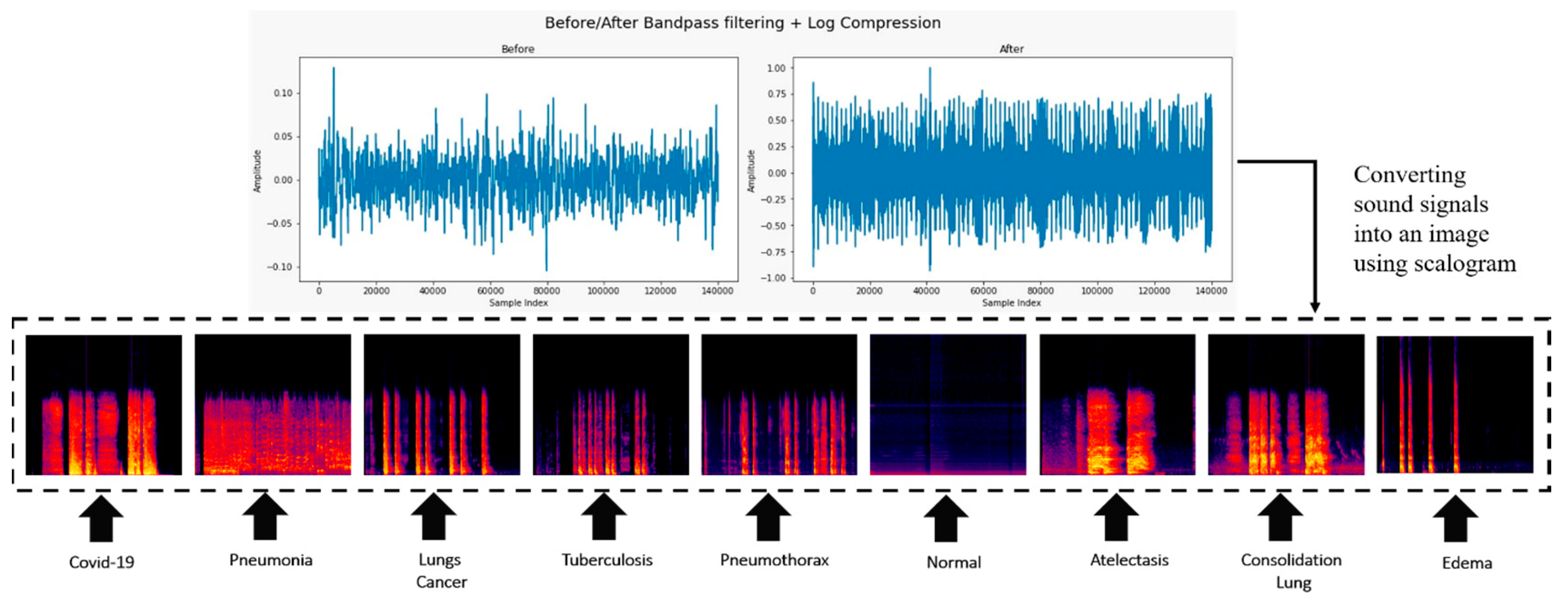
3.3. Conversion of Cough Audio to an Image
- We collected several different types of cough sound image databases.
- All cough sound recordings had the same sampling rate, such as 44.1 kHz.
- A low-band pass filter method was used to remove the unwanted background noise.
- The CWT method was applied to convert a cough sound signal into its frequency domain representation over time.
- In a scalogram, the scale of the frequency axis changes with time.
- The scalogram transformation is a 2D matrix, where one axis represents time and another axis represents frequency.
- We mapped the intensity values to colors by using a heatmap color map and created an image-like representation of the cough sound signal’s frequency content over time.
3.4. Using BL-SMOTE to Balance the Class’s Samples
3.5. Proposed Model
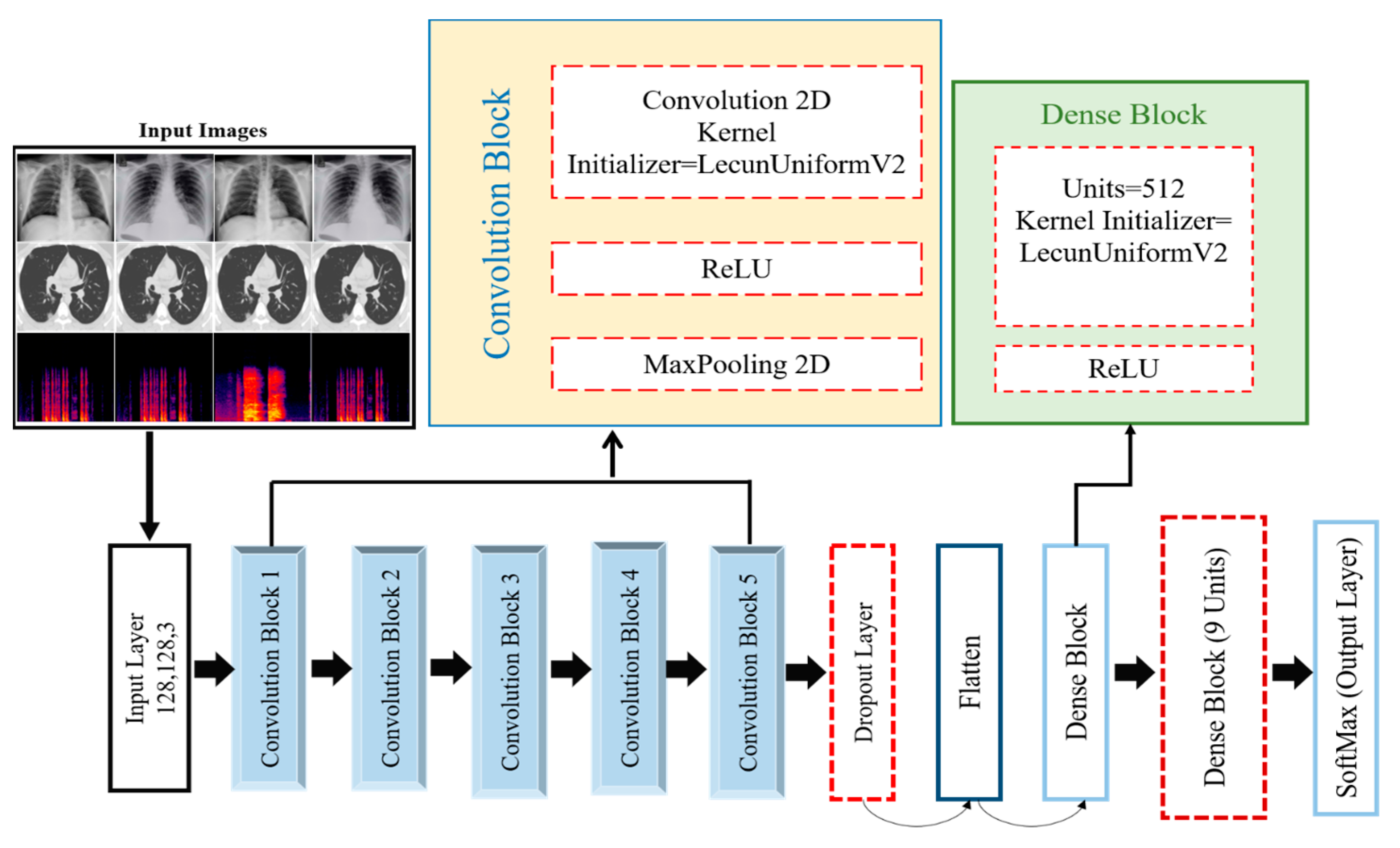
3.5.1. Detailed Structure of the Proposed DCDD_Net
3.5.2. Proposed DCDD_Net Convolutional Blocks
3.5.3. Dropout Layer
3.5.4. Flatten Layer
3.6. Dense Blocks
3.6.1. ReLU Activation
3.6.2. Dense Layer
3.7. Evaluation of the Proposed DCDD_Net
4. Results and Discussion
4.1. Experimental Setup and Fine-Tuning of Hyperparameters
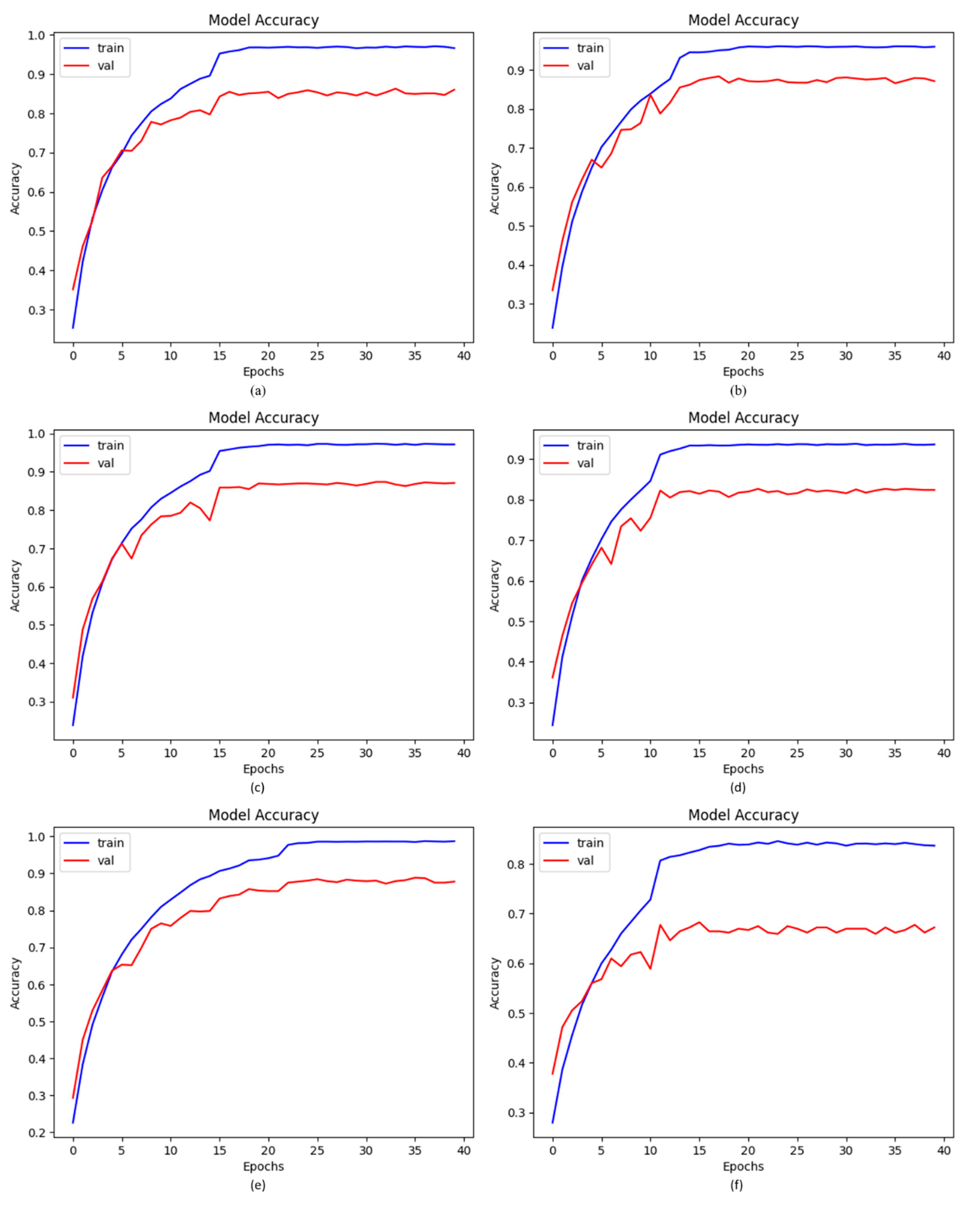
4.2. Accuracy of Proposed DCDD_Net with Baseline Models
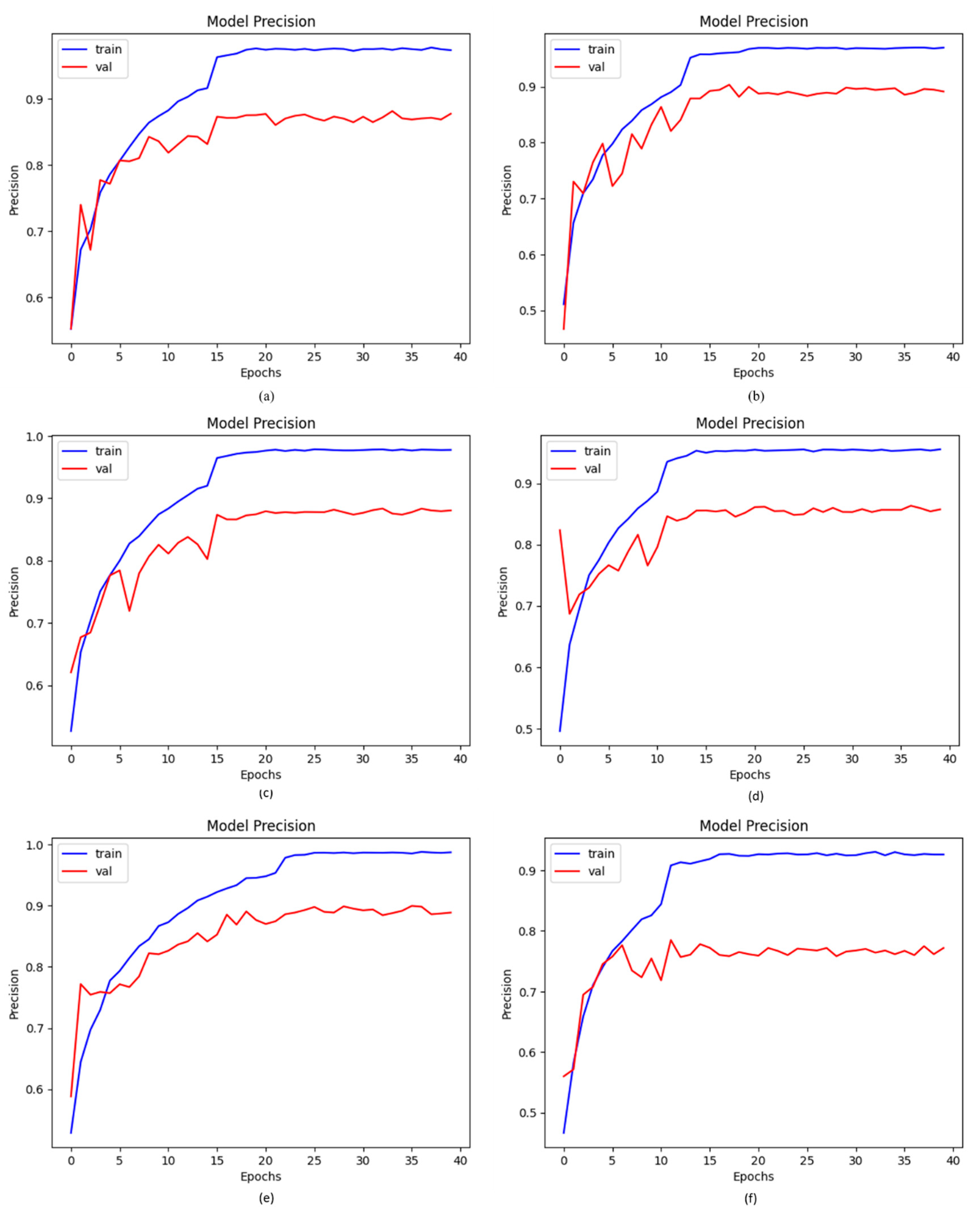
4.3. Precision of Proposed DCDD_Net with Baseline Models
4.4. AUC of Proposed DCDD_Net with Other Networks
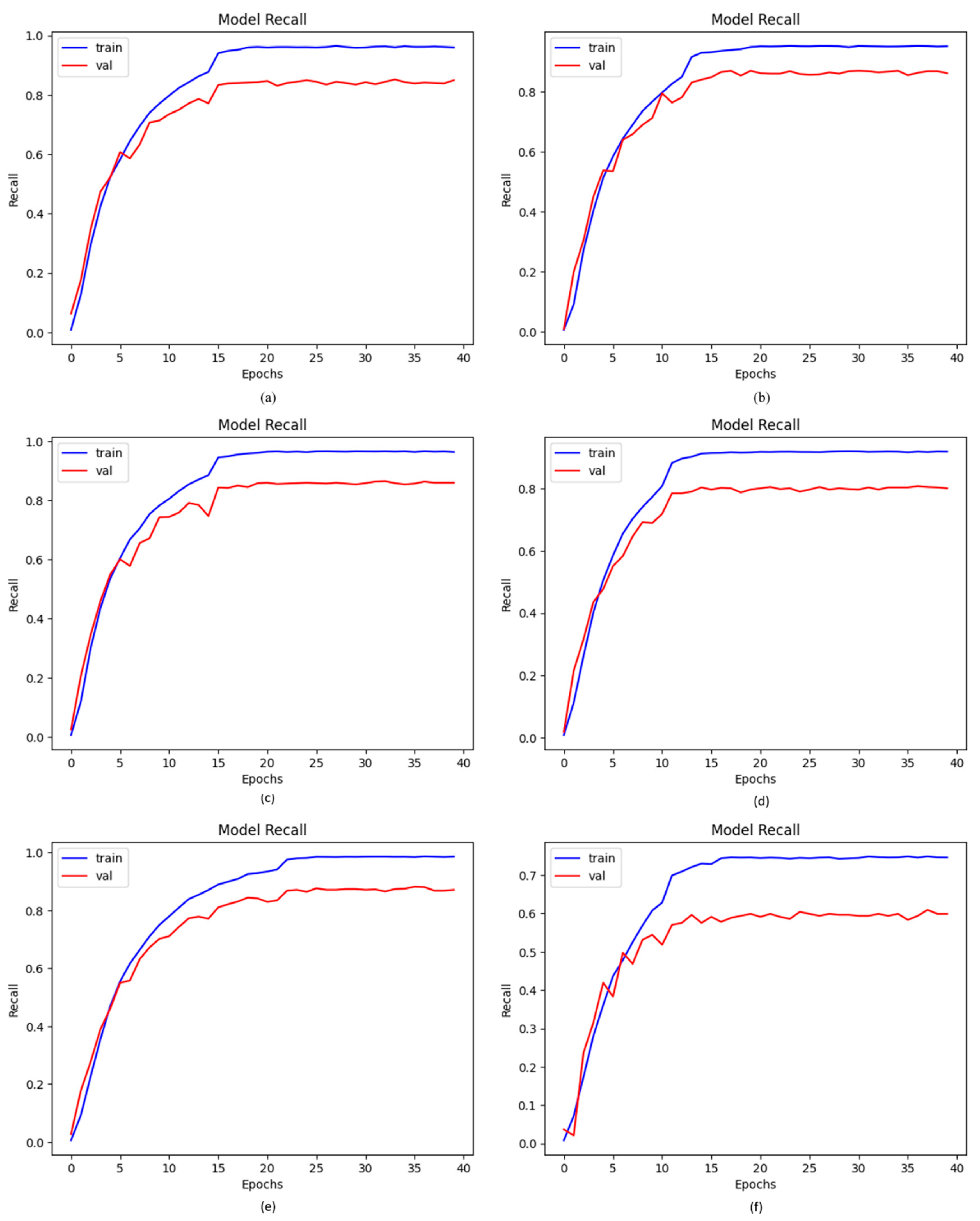
4.5. Recall of Proposed DCDD_Net with Other Networks
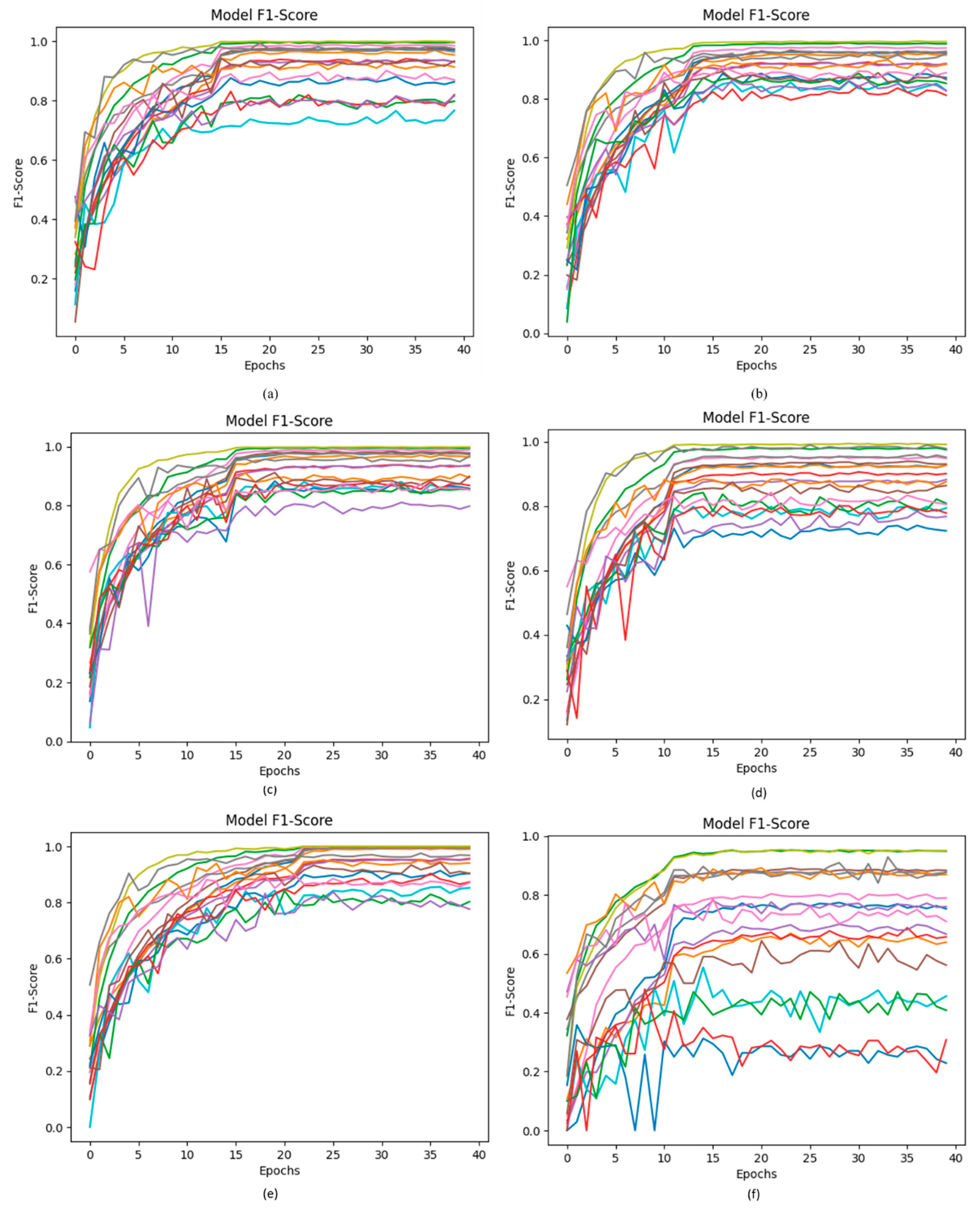
4.6. F1-Score of Proposed DCDD_Net with Other Networks
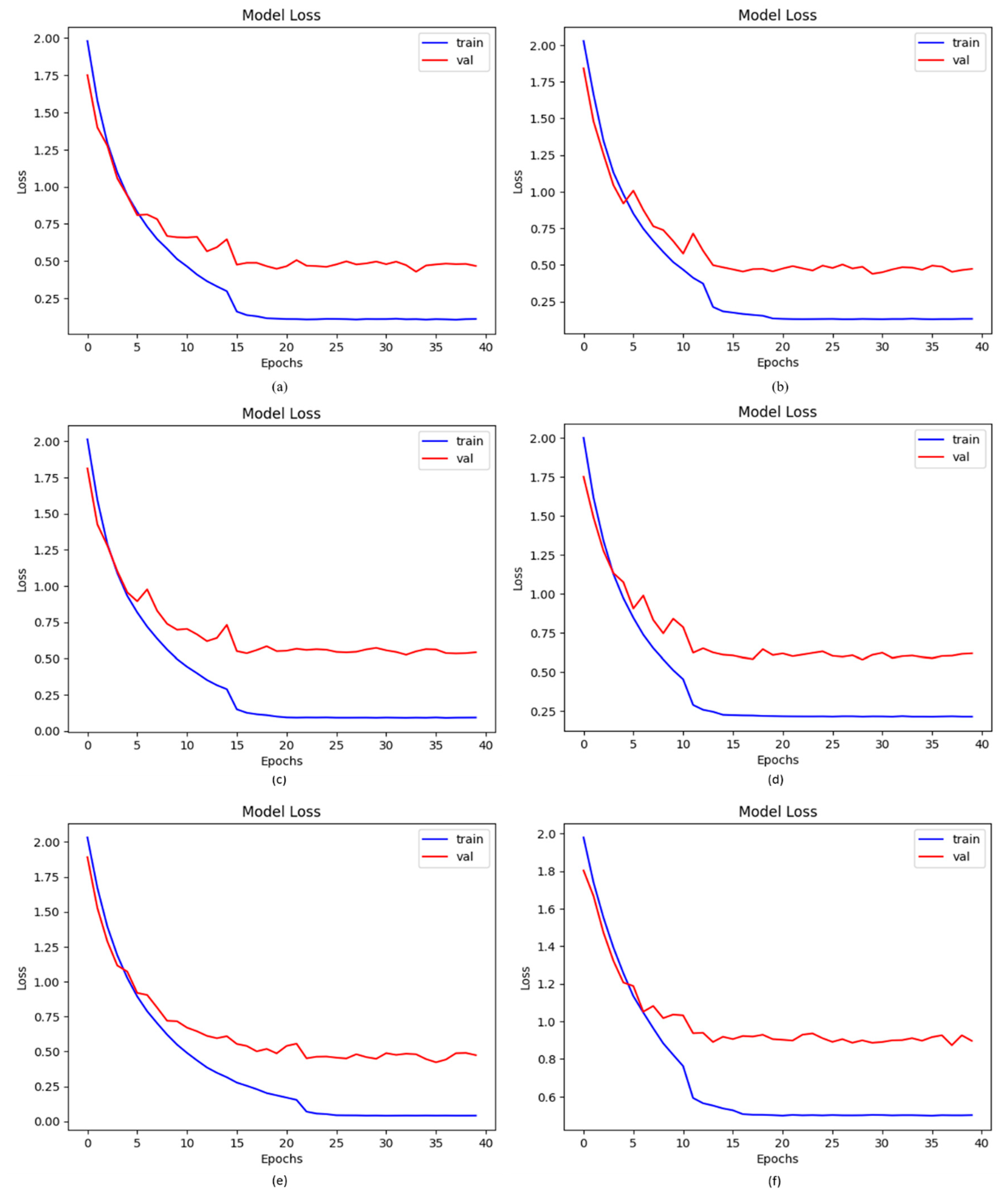
4.7. Loss of Proposed DCDD_Net with Other Networks
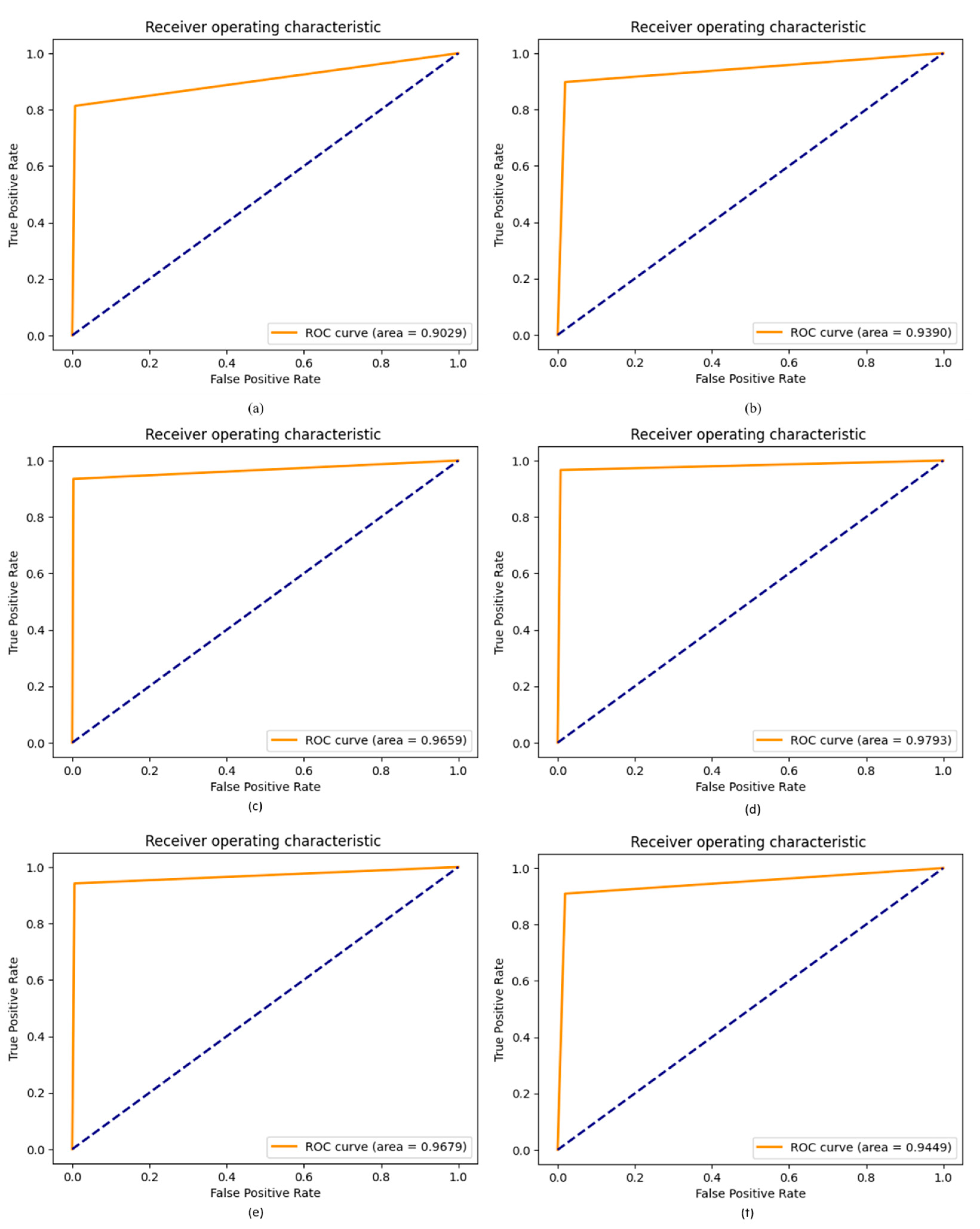
4.8. ROC of Proposed DCDD_Net with Other Networks
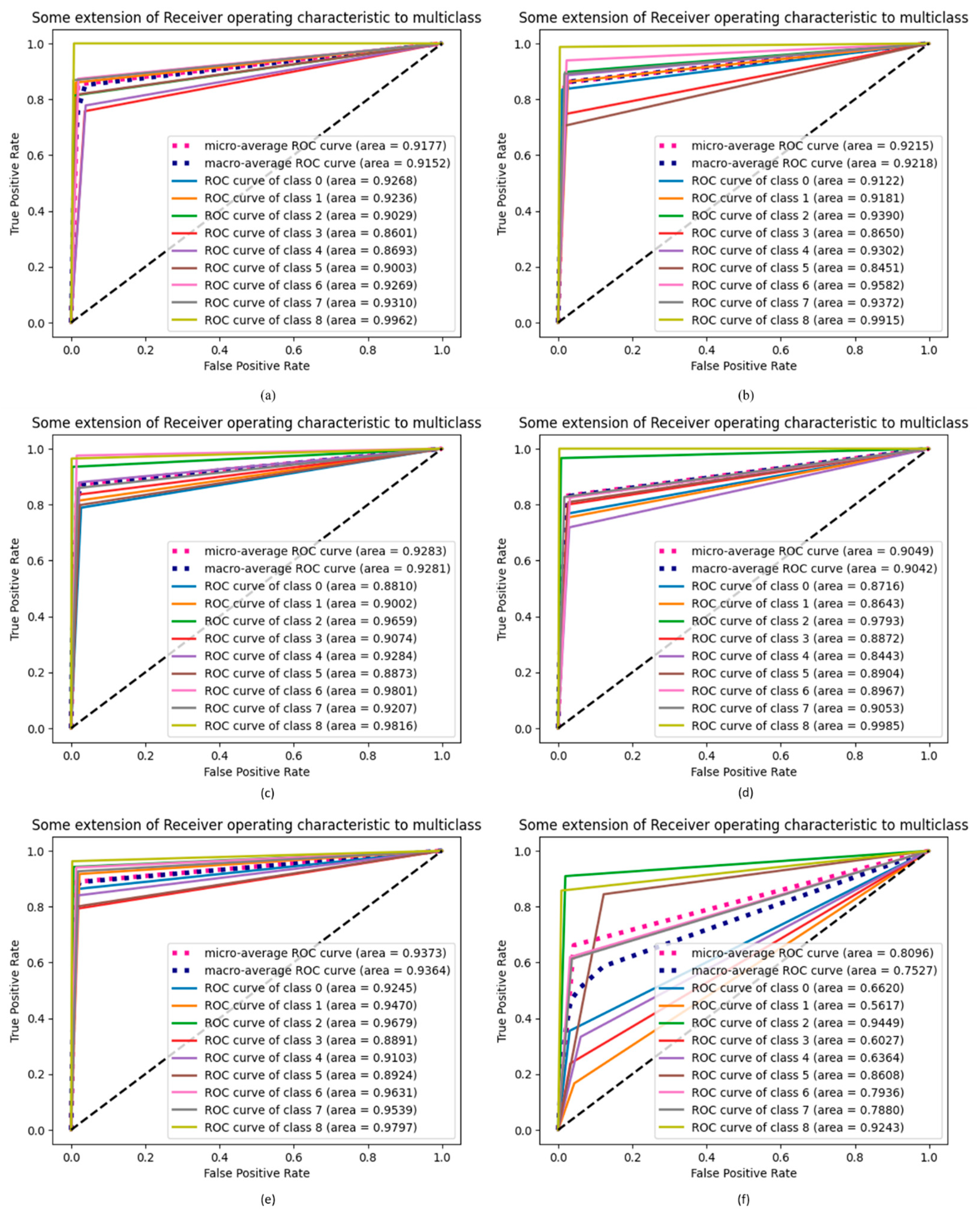
4.9. ROC Extension of Proposed DCDD_Net with Other Networks
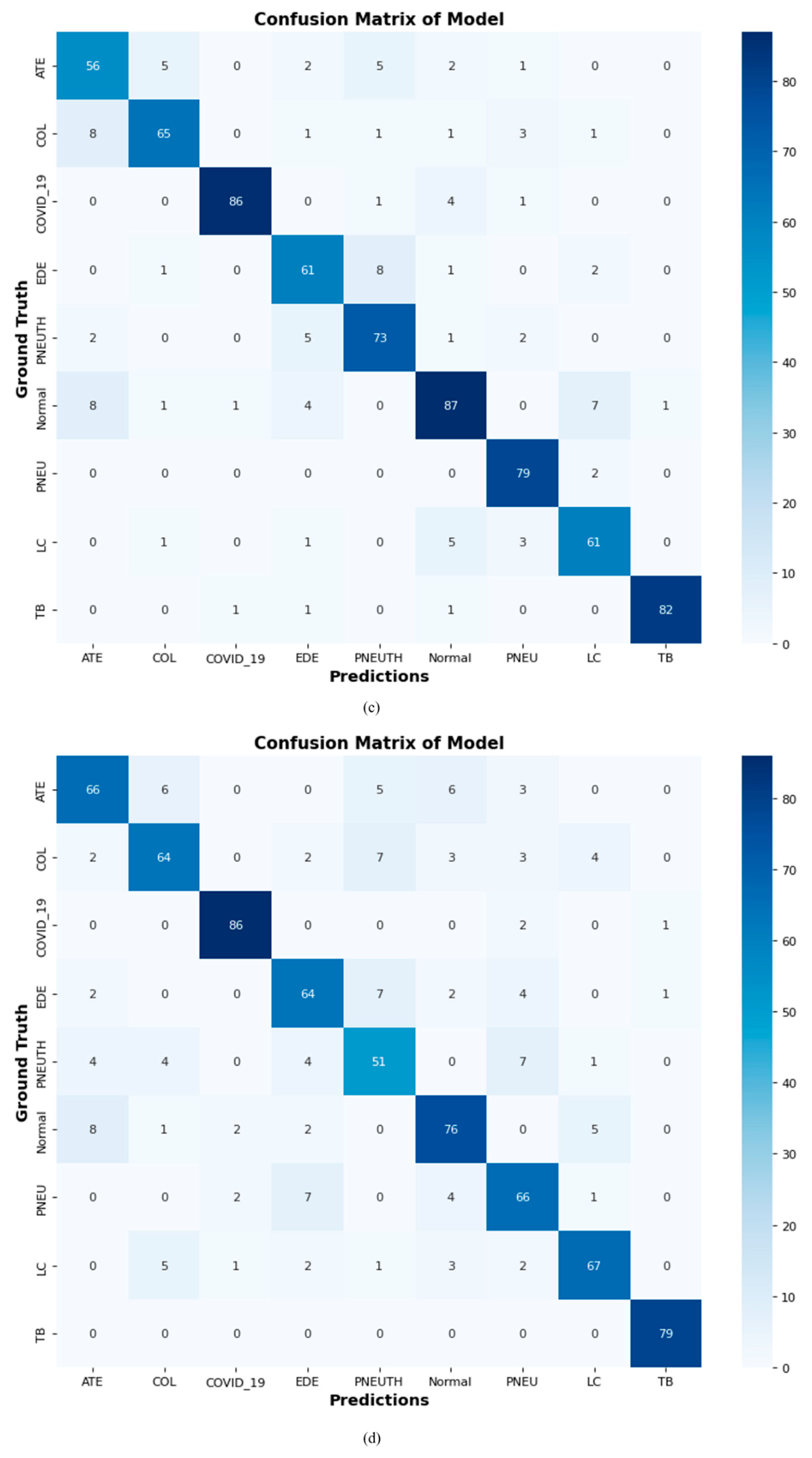
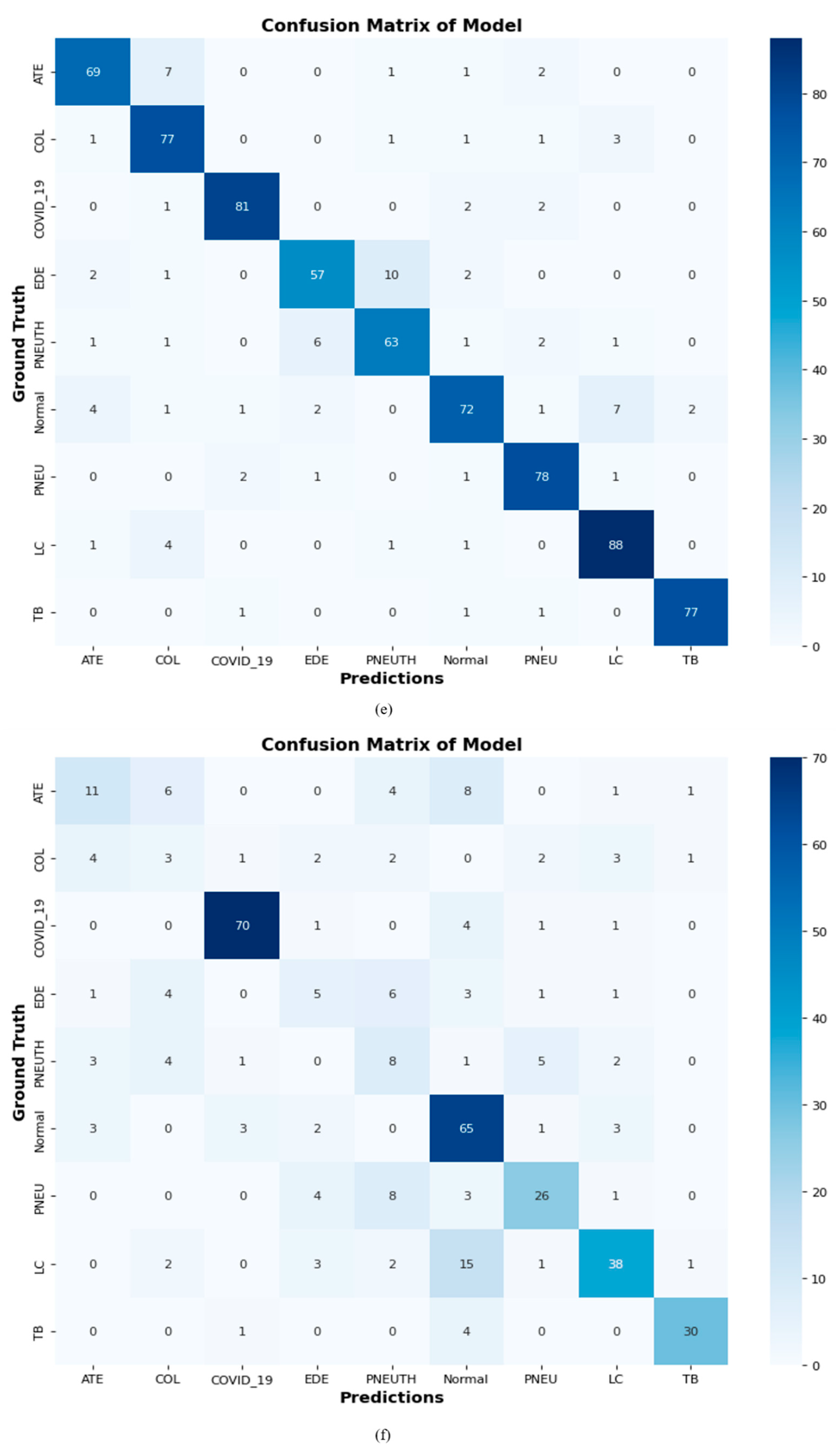
4.10. Confusion Matrix of Proposed DCDD_Net with Baseline Models
4.11. Statistical Analysis
4.12. Comparison of the Proposed DCDD_NET Using State-of-the-Art
4.13. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aslani, S.; Jacob, J. Utilisation of deep learning for COVID-19 diagnosis. Clin. Radiol. 2023, 78, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Hertel, R.; Benlamri, R. Deep Learning Techniques for COVID-19 Diagnosis and Prognosis Based on Radiological Imaging. ACM Comput. Surv. 2023, 55, 1–39. [Google Scholar] [CrossRef]
- Khan, A.; Khan, S.H.; Saif, M.; Batool, A.; Sohail, A.; Khan, M.W. A Survey of Deep Learning Techniques for the Analysis of COVID-19 and their usability for Detecting Omicron. J. Exp. Theor. Artif. Intell. 2023, 1–43. [Google Scholar] [CrossRef]
- Mercaldo, F.; Belfiore, M.P.; Reginelli, A.; Brunese, L.; Santone, A. Coronavirus covid-19 detection by means of explainable deep learning. Sci. Rep. 2023, 13, 462. [Google Scholar] [CrossRef]
- Bassiouni, M.M.; Chakrabortty, R.K.; Hussain, O.K.; Rahman, H.F. Advanced deep learning approaches to predict supply chain risks under COVID-19 restrictions. Expert Syst. Appl. 2023, 211, 118604. [Google Scholar] [CrossRef]
- Constantinou, M.; Exarchos, T.; Vrahatis, A.G.; Vlamos, P. COVID-19 Classification on Chest X-ray Images Using Deep Learning Methods. Int. J. Environ. Res. Public Health 2023, 20, 2035. [Google Scholar] [CrossRef]
- Vinod, D.N.; Prabaharan, S.R.S. COVID-19-The Role of Artificial Intelligence, Machine Learning, and Deep Learning: A Newfangled. Arch. Comput. Methods Eng. 2023, 30, 2667–2682. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.; Bajaj, V. Deep learning models-based CT-scan image classification for automated screening of COVID-19. Biomed. Signal Process. Control. 2023, 80, 104268. [Google Scholar] [CrossRef]
- Zhao, Z.; Wu, J.; Cai, F.; Zhang, S.; Wang, Y.-G. A hybrid deep learning framework for air quality prediction with spatial autocorrelation during the COVID-19 pandemic. Sci. Rep. 2023, 13, 1015. [Google Scholar] [CrossRef] [PubMed]
- Du, H.; Dong, E.; Badr, H.S.; Petrone, M.E.; Grubaugh, N.D.; Gardner, L.M. Incorporating variant frequencies data into short-term forecasting for COVID-19 cases and deaths in the USA: A deep learning approach. Ebiomedicine 2023, 89, 104482. [Google Scholar] [CrossRef]
- Choudhary, T.; Gujar, S.; Goswami, A.; Mishra, V.; Badal, T. Deep learning-based important weights-only transfer learning approach for COVID-19 CT-scan classification. Appl. Intell. 2023, 53, 7201–7215. [Google Scholar] [CrossRef]
- Chen, M.-Y.; Lai, Y.-W.; Lian, J.-W. Using Deep Learning Models to Detect Fake News about COVID-19. ACM Trans. Internet Technol. 2023, 23, 1–23. [Google Scholar] [CrossRef]
- Iqbal, A.; Usman, M.; Ahmed, Z. An efficient deep learning-based framework for tuberculosis detection using chest X-ray images. Tuberculosis 2022, 136, 102234. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Gupta, M.; Gupta, D.; Tiwari, S. Novel deep transfer learning model for COVID-19 patient detection using X-ray chest images. J. Ambient. Intell. Humaniz. Comput. 2023, 14, 469–478. [Google Scholar] [CrossRef]
- Huy, V.T.Q.; Lin, C.-M. An Improved Densenet Deep Neural Network Model for Tuberculosis Detection Using Chest X-ray Images. IEEE Access 2023, 11, 42839–42849. [Google Scholar] [CrossRef]
- Al-Waisy, A.S.; Al-Fahdawi, S.; Mohammed, M.A.; Abdulkareem, K.H.; Mostafa, S.A.; Maashi, M.S.; Arif, M.; Garcia-Zapirain, B. COVID-CheXNet: Hybrid deep learning framework for identifying COVID-19 virus in chest X-rays images. Soft Comput. 2023, 27, 2657–2672. [Google Scholar] [CrossRef] [PubMed]
- Malik, H.; Anees, T.; Din, M.; Naeem, A. CDC_Net: Multi-classification convolutional neural network model for detection of COVID-19, pneumothorax, pneumonia, lung Cancer, and tuberculosis using chest X-rays. Multimed. Tools Appl. 2023, 82, 13855–13880. [Google Scholar] [CrossRef] [PubMed]
- Shelke, A.; Inamdar, M.; Shah, V.; Tiwari, A.; Hussain, A.; Chafekar, T.; Mehendale, N. Chest X-ray Classification Using Deep Learning for Automated COVID-19 Screening. SN Comput. Sci. 2021, 2, 300. [Google Scholar] [CrossRef]
- Ali, M.U.; Kallu, K.D.; Masood, H.; Tahir, U.; Gopi, C.V.V.M.; Zafar, A.; Lee, S.W. A CNN-Based Chest Infection Diagnostic Model: A Multistage Multiclass Isolated and Developed Transfer Learning Framework. Int. J. Intell. Syst. 2023, 2023, 1–12. [Google Scholar] [CrossRef]
- Agrawal, S.; Honnakasturi, V.; Nara, M.; Patil, N. Utilizing Deep Learning Models and Transfer Learning for COVID-19 Detection from X-ray Images. SN Comput. Sci. 2023, 4, 326. [Google Scholar] [CrossRef]
- Ibrahim, A.U.; Ozsoz, M.; Serte, S.; Al-Turjman, F.; Yakoi, P.S. Pneumonia Classification Using Deep Learning from Chest X-ray Images During COVID-19. Cogn. Comput. 2021, 1–13. [Google Scholar] [CrossRef]
- Ayalew, A.M.; Salau, A.O.; Tamyalew, Y.; Abeje, B.T.; Woreta, N. X-ray image-based COVID-19 detection using deep learning. Multimed. Tools Appl. 2023, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Jennifer, J.S.; Sharmila, T.S. A Neutrosophic Set Approach on Chest X-rays for Automatic Lung Infection Detection. Inf. Technol. Control 2023, 52, 37–52. [Google Scholar] [CrossRef]
- Jaszcz, A.; Połap, D.; Damaševičius, R. Lung X-ray Image Segmentation Using Heuristic Red Fox Optimization Algorithm. Sci. Program. 2022, 2022, 1–8. [Google Scholar] [CrossRef]
- Karthik, R.; Menaka, R.; Hariharan, M.; Kathiresan, G.S. Ai for COVID-19 detection from radiographs: Incisive analysis of state of the art techniques, key challenges and future directions. IRBM 2022, 43, 486–510. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Shen, L.; Guan, Q.; Li, X.; Zhou, Q.; Ruan, S. Deep co-supervision and attention fusion strategy for automatic COVID-19 lung infection segmentation on CT images. Pattern Recognit. 2022, 124, 108452. [Google Scholar] [CrossRef]
- Li, Z.; Zhao, S.; Chen, Y.; Luo, F.; Kang, Z.; Cai, S.; Zhao, W.; Liu, J.; Zhao, D.; Li, Y. A deep-learning-based framework for severity assessment of COVID-19 with CT images. Expert Syst. Appl. 2021, 185, 115616. [Google Scholar] [CrossRef]
- Pahar, M.; Klopper, M.; Reeve, B.; Warren, R.; Theron, G.; Diacon, A.; Niesler, T. Automatic Tuberculosis and COVID-19 cough classification using deep learning. In Proceedings of the 2022 International Conference on Electrical, Computer and Energy Technologies (ICECET), Prague, Czech Republic, 20–22 July 2022; pp. 1–9. [Google Scholar] [CrossRef]
- Kim, S.; Baek, J.-Y.; Lee, S.-P. COVID-19 Detection Model with Acoustic Features from Cough Sound and Its Application. Appl. Sci. 2023, 13, 2378. [Google Scholar] [CrossRef]
- Islam, R.; Abdel-Raheem, E.; Tarique, M. A study of using cough sounds and deep neural networks for the early detection of Covid-19. Biomed. Eng. Adv. 2022, 3, 100025. [Google Scholar] [CrossRef]
- Loey, M.; Mirjalili, S. COVID-19 cough sound symptoms classification from scalogram image representation using deep learning models. Comput. Biol. Med. 2021, 139, 105020. [Google Scholar] [CrossRef]
- Nessiem, M.A.; Mohamed, M.M.; Coppock, H.; Gaskell, A.; Schuller, B.W. Detecting COVID-19 from breathing and coughing sounds using deep neural networks. In Proceedings of the 2021 IEEE 34th international symposium on computer-based medical systems (CBMS), Aveiro, Portugal, 7–9 June 2021; pp. 183–188. [Google Scholar]
- Tawfik, M.; Nimbhore, S.; Al-Zidi, N.M.; Ahmed, Z.A.; Almadani, A.M. Multi-features extraction for automating COVID-19 detection from cough sound using deep neural networks. In Proceedings of the 2022 4th International Conference on Smart Systems and Inventive Technology (ICSSIT), Tirunelveli, India, 20–22 January 2022; pp. 944–950. [Google Scholar]
- Zhang, K.; Qi, S.; Cai, J.; Zhao, D.; Yu, T.; Yue, Y.; Yao, Y.; Qian, W. Content-based image retrieval with a Convolutional Siamese Neural Network: Distinguishing lung cancer and tuberculosis in CT images. Comput. Biol. Med. 2022, 140, 105096. [Google Scholar] [CrossRef] [PubMed]
- Alebiosu, D.O.; Dharmaratne, A.; Lim, C.H. Improving tuberculosis severity assessment in computed tomography images using novel DAvoU-Net segmentation and deep learning framework. Expert Syst. Appl. 2023, 213, 119287. [Google Scholar] [CrossRef]
- Toğaçar, M.; Ergen, B.; Cömert, Z. Detection of lung cancer on chest CT images using minimum redundancy maximum relevance feature selection method with convolutional neural networks. Biocybern. Biomed. Eng. 2020, 40, 23–39. [Google Scholar] [CrossRef]
- Latif, G.; Morsy, H.; Hassan, A.; Alghazo, J. Novel Coronavirus and Common Pneumonia Detection from CT Scans Using Deep Learning-Based Extracted Features. Viruses 2022, 14, 1667. [Google Scholar] [CrossRef]
- Sadik, F.; Dastider, A.G.; Subah, M.R.; Mahmud, T.; Fattah, S.A. A dual-stage deep convolutional neural network for au-tomatic diagnosis of COVID-19 and pneumonia from chest CT images. Comput. Biol. Med. 2022, 149, 105806. [Google Scholar] [CrossRef]
- Florescu, L.M.; Streba, C.T.; Şerbănescu, M.-S.; Mămuleanu, M.; Florescu, D.N.; Teică, R.V.; Nica, R.E.; Gheonea, I.A. Federated Learning Approach with Pre-Trained Deep Learning Models for COVID-19 Detection from Unsegmented CT images. Life 2022, 12, 958. [Google Scholar] [CrossRef] [PubMed]
- Fu, M.; Yi, S.L.; Zeng, Y.; Ye, F.; Li, Y.; Dong, X.; Ren, Y.-D.; Luo, L.; Pan, J.-S.; Zhang, Q. Deep learning-based recognizing covid-19 and other common infectious diseases of the lung by chest ct scan images. medRxiv 2020. [Google Scholar] [CrossRef]
- Kaewlek, T.; Tanyong, K.; Chakkaeo, J.; Kladpree, S.; Chusin, T.; Yabsantia, S.; Udee, N. Classification of Pneumonia, Tuberculosis, and COVID-19 on Computed Tomography Images Using Deep Learning. 2023. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=4379837 (accessed on 10 July 2023).
- Polat, H.; Özerdem, M.S.; Ekici, F.; Akpolat, V. Automatic detection and localization of COVID-19 pneumonia using axial computed tomography images and deep convolutional neural networks. Int. J. Imaging Syst. Technol. 2021, 31, 509–524. [Google Scholar] [CrossRef]
- Abayomi-Alli, O.O.; Damaševičius, R.; Abbasi, A.A.; Maskeliūnas, R. Detection of COVID-19 from Deep Breathing Sounds Using Sound Spectrum with Image Augmentation and Deep Learning Techniques. Electronics 2022, 11, 2520. [Google Scholar] [CrossRef]
- Mishra, N.K.; Singh, P.; Joshi, S.D. Automated detection of COVID-19 from CT scan using convolutional neural network. Biocybern. Biomed. Eng. 2021, 41, 572–588. [Google Scholar] [CrossRef] [PubMed]
- Masud, M.; Alshehri, M.D.; Alroobaea, R.; Shorfuzzaman, M. Leveraging Convolutional Neural Network for COVID-19 Disease Detection Using CT Scan Images. Intell. Autom. Soft Comput. 2021, 29, 1–13. [Google Scholar] [CrossRef]
- World Health Organization. Cancer. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 30 July 2023).
- Yogapriya, J.; Chandran, V.; Sumithra, M.G.; Anitha, P.; Jenopaul, P.; Dhas, C.S.G. Gastrointestinal Tract Disease Classification from Wireless Endoscopy Images Using Pretrained Deep Learning Model. Comput. Math. Methods Med. 2021, 2021, 5940433. [Google Scholar] [CrossRef] [PubMed]
- Alzubaidi, L.; Fadhel, M.A.; Al-Shamma, O.; Zhang, J.; Santamaría, J.; Duan, Y.; Oleiwi, S.R. Towards a Better Understanding of Transfer Learning for Medical Imaging: A Case Study. Appl. Sci. 2020, 10, 4523. [Google Scholar] [CrossRef]
- Igarashi, S.; Sasaki, Y.; Mikami, T.; Sakuraba, H.; Fukuda, S. Anatomical classification of upper gastrointestinal organs under various image capture conditions using AlexNet. Comput. Biol. Med. 2020, 124, 103950. [Google Scholar] [CrossRef]
- Charisis, V.; Tsiligiri, A.; Hadjileontiadis, L.J.; Liatsos, C.N.; Mavrogiannis, C.C.; Sergiadis, G.D. Ulcer detection in Wireless Capsule Endoscopy images using bidimensional nonlinear analysis. In Proceedings of the XII Mediterranean Conference on Medical and Biological Engineering and Computing, Chalkidiki, Greece, 27–30 May 2010; Springer: Berlin/Heidelberg, Ger-many, 2010; pp. 236–239. [Google Scholar]
- Mohapatra, S.; Nayak, J.; Mishra, M.; Pati, G.K.; Naik, B.; Swarnkar, T. Wavelet Transform and Deep Convolutional Neural Network-Based Smart Healthcare System for Gastrointestinal Disease Detection. Interdiscip. Sci. Comput. Life Sci. 2021, 13, 212–228. [Google Scholar] [CrossRef]
- Yuan, Y.; Li, B.; Meng, M.Q.-H. Bleeding Frame and Region Detection in the Wireless Capsule Endoscopy Video. IEEE J. Biomed. Health Inform. 2015, 20, 624–630. [Google Scholar] [CrossRef]
- Shamsudhin, N.; Zverev, V.I.; Keller, H.; Pane, S.; Egolf, P.W.; Nelson, B.J.; Tishin, A.M. Magnetically guided capsule endos-copy. Med. Phys. 2017, 44, e91–e111. [Google Scholar] [CrossRef]
- Stewart, B.J.; Ferdinand, J.R.; Clatworthy, M.R. Using single-cell technologies to map the human immune system—Implications for nephrology. Nat. Rev. Nephrol. 2020, 16, 112–128. [Google Scholar] [CrossRef] [PubMed]
- Alqudah, A.M.; Qazan, S. Augmented COVID-19 X-ray Images Dataset: 4. Mendeley Data. 2020. Available online: https://data.mendeley.com/datasets/2fxz4px6d8/4 (accessed on 10 July 2023).
- COVID 19 Chest X-ray. 2020. Available online: https://github.com/agchung (accessed on 10 July 2023).
- NIH Chest X-rays. Kaggle, 2018. Available online: https://www.kaggle.com/nih-chest-xrays/data (accessed on 9 July 2023).
- Kermany, D.; Zhang, K.; Goldbaum, M. Labeled Optical Coherence Tomography (OCT) and Chest X-ray Images for Classification Mendeley Data. Mendeley Data. 2018. Available online: https://data.mendeley.com/datasets/rscbjbr9sj/2 (accessed on 10 July 2023).
- Kermany, D.S.; Goldbaum, M.; Cai, W.; Valentim, C.C.S.; Liang, H.; Baxter, S.L.; McKeown, A.; Yang, G.; Wu, X.; Yan, F.; et al. Identifying Medical Diagnoses and Treatable Diseases by Image-Based Deep Learning. Cell 2018, 172, 1122–1131.e9. [Google Scholar] [CrossRef]
- Shiraishi, J.; Katsuragawa, S.; Ikezoe, J.; Matsumoto, T.; Kobayashi, T.; Komatsu, K.-I.; Matsui, M.; Fujita, H.; Kodera, Y.; Doi, K. Development of a digital image database for chest radiographs with and without a lung nodule: Receiver operating characteristic analysis of radiologists’ detection of pulmonary nodules. Am. J. Roentgenol. 2000, 174, 71–74. [Google Scholar] [CrossRef]
- Rahman, T.; Khandakar, A.; Kadir, M.A.; Islam, K.R.; Islam, K.F.; Mazhar, R.; Hamid, T.; Islam, M.T.; Kashem, S.; Bin Mahbub, Z.; et al. Reliable Tuberculosis Detection Using Chest X-ray with Deep Learning, Segmentation and Visualization. IEEE Access 2020, 8, 191586–191601. [Google Scholar] [CrossRef]
- Soares, E.; Angelov, P.; Biaso, S.; Froes, M.H.; Abe, D.K. SARS-CoV-2 CT-scan dataset: A large dataset of real patients CT scans for SARS-CoV-2 identification. medRxiv 2020. [Google Scholar] [CrossRef]
- Curation, D. The RSNA pulmonary embolism CT dataset. Radiology 2021, 3, e200254. [Google Scholar]
- Colak, E.; Kitamura, F.C.; Hobbs, S.B.; Wu, C.C.; Lungren, M.P.; Prevedello, L.M.; Kalpathy-Cramer, J.; Ball, R.L.; Shih, G.; Stein, A.; et al. The RSNA pulmonary embolism CT dataset. Radiol. Artif. Intell. 2021, 3, e200254. [Google Scholar] [CrossRef]
- Yan, J. COVID-19 and Common Pneumonia Chest CT Dataset. Mendeley Data. 2020. Available online: https://data.mendeley.com/datasets/3y55vgckg6/1 (accessed on 10 July 2023).
- Gao, X.W.; James-Reynolds, C.; Currie, E. Analysis of tuberculosis severity levels from CT pulmonary images based on en-hanced residual deep learning architecture. Neurocomputing 2020, 392, 233–244. [Google Scholar] [CrossRef]
- Ghaderzadeh, M.; Asadi, F.; Jafari, R.; Bashash, D.; Abolghasemi, H.; Aria, M. Deep Convolutional Neural Network–Based Computer-Aided Detection System for COVID-19 Using Multiple Lung Scans: Design and Implementation Study. J. Med. Internet Res. 2021, 23, e27468. [Google Scholar] [CrossRef]
- Sharma, N.; Krishnan, P.; Kumar, R.; Ramoji, S.; Chetupalli, S.R.; Nirmala, R.; Ghosh, P.K.; Ganapathy, S. Coswara—A Database of Breathing, Cough, and Voice Sounds for COVID-19 Diagnosis. arXiv 2020, arXiv:2005.10548. [Google Scholar]
- Pahar, M.; Klopper, M.; Warren, R.; Niesler, T. COVID-19 Cough Classification using Machine Learning and Global Smartphone Recordings. Comput. Biol. Med. 2021, 135, 104572. [Google Scholar] [CrossRef]
- Pahar, M.; Klopper, M.; Reeve, B.; Warren, R.; Theron, G.; Niesler, T. Automatic cough classification for tuberculosis screening in a real-world environment. Physiol. Meas. 2021, 42, 105014. [Google Scholar] [CrossRef]
- Rocha, B.M.; Filos, D.; Mendes, L.; Serbes, G.; Ulukaya, S.; Kahya, Y.P.; Jakovljevic, N.; Turukalo, T.L.; Vogiatzis, I.M.; Perantoni, E.; et al. An open access database for the evaluation of respiratory sound classification algorithms. Physiol. Meas. 2019, 40, 035001. [Google Scholar] [CrossRef]
- Harle, A.S.; Blackhall, F.H.; Molassiotis, A.; Yorke, J.; Dockry, R.; Holt, K.J.; Yuill, D.; Baker, K.; Smith, J.A. Cough in patients with lung cancer: A longitudinal observational study of characterization and clinical associations. Chest 2019, 155, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Byeon, Y.-H.; Pan, S.-B.; Kwak, K.-C. Intelligent Deep Models Based on Scalograms of Electrocardiogram Signals for Biometrics. Sensors 2019, 19, 935. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Zhou, M. ECG Classification Using Wavelet Packet Entropy and Random Forests. Entropy 2016, 18, 285. [Google Scholar] [CrossRef]
- Khorrami, H.; Moavenian, M. A comparative study of DWT, CWT and DCT transformations in ECG arrhythmias classification. Expert Syst. Appl. 2010, 37, 5751–5757. [Google Scholar] [CrossRef]
- Han, H.; Wang, W.Y.; Mao, B.H. Borderline-SMOTE: A new over-sampling method in imbalanced datasets learning. In Proceedings of the International Conference on Intelligent Computing, Hefei, China, 23–26 August 2005; Springer: Berlin/Heidelberg, Germany, 2005; pp. 878–887. [Google Scholar]
- Wen, F.; David, A. A genetic algorithm based method for bidding strategy coordination in energy and spinning reserve markets. Artif. Intell. Eng. 2001, 15, 71–79. [Google Scholar] [CrossRef]
- Dietterich, T.G. Approximate Statistical Tests for Comparing Supervised Classification Learning Algorithms. Neural Comput. 1998, 10, 1895–1923. [Google Scholar] [CrossRef]
- Cuevas, A.; Febrero, M.; Fraiman, R. An anova test for functional data. Comput. Stat. Data Anal. 2004, 47, 111–122. [Google Scholar] [CrossRef]
- Wang, L.; Wang, X.; Fu, J.; Zhen, L. A Novel Probability Binary Particle Swarm Optimization Algorithm and Its Application. J. Softw. 2008, 3, 28–35. [Google Scholar] [CrossRef]
- Albataineh, Z.; Aldrweesh, F.; Alzubaidi, M.A. COVID-19 CT-images diagnosis and severity assessment using machine learning algorithm. Clust. Comput. 2023, 1–16. [Google Scholar] [CrossRef]
- Ulukaya, S.; Sarıca, A.A.; Erdem, O.; Karaali, A. MSCCov19Net: Multi-branch deep learning model for COVID-19 detection from cough sounds. Med. Biol. Eng. Comput. 2023, 61, 1619–1629. [Google Scholar] [CrossRef] [PubMed]
- Nasser, A.A.; Akhloufi, M.A. A Review of Recent Advances in Deep Learning Models for Chest Disease Detection Using Radiography. Diagnostics 2023, 13, 159. [Google Scholar] [CrossRef]
- Anjugam, S.; Arul Leena Rose, P.J. Study of Deep Learning Approaches for Diagnosing COVID-19 Disease using Chest CT Images. In Proceedings of the 2023 7th International Conference on Computing Methodologies and Communication (ICCMC), Erode, India, 23–25 February 2023; pp. 263–269. [Google Scholar] [CrossRef]
- Malik, H.; Anees, T.; Chaudhry, M.U.; Gono, R.; Jasiński, M.; Leonowicz, Z.; Bernat, P. A Novel Fusion Model of Hand-Crafted Features with Deep Convolutional Neural Networks for Classification of Several Chest Diseases Using X-ray Images. IEEE Access 2023, 11, 39243–39268. [Google Scholar] [CrossRef]
- Saeed, N.; Malik, H.; Naeem, A.; Bashir, U. Incorporating big data and IoT in intelligent ecosystems: State-of-the-arts, challenges and opportunities, and future directions. Multimed. Tools Appl. 2023, 1–43. [Google Scholar] [CrossRef]
- Malik, H.; Anees, T.; Faheem, M.; Chaudhry, M.U.; Ali, A.; Asghar, M.N. Blockchain and Internet of Things in Smart Cities and Drug Supply Management: Open Issues, Opportunities, and Future Directions. Internet Things 2023, 23, 100860. [Google Scholar] [CrossRef]















| Chest Diseases | No. of Cough Audios for Each Class | Total Audio in Minutes (m) | Standard Sounds per Person in Seconds (s) | Standard Deviation |
|---|---|---|---|---|
| COVID-19 | 100 | 32 (m) | 2.77 (s) | 1.61 (s) |
| EDE | 39 | 32 (m) | 2.05 (s) | 1.04 (s) |
| Normal | 210 | 120 (m) | 3.92 (s) | 1.79 (s) |
| COL | 80 | 24 (m) | 2.61 (s) | 1.30 (s) |
| PNEU | 119 | 57 (m) | 2.02 (s) | 1.01 (s) |
| PNEUTH | 42 | 37 (m) | 2.11 (s) | 1.06 (s) |
| LC | 222 | 60 (m) | 2.15 (s) | 1.07 (s) |
| TB | 292 | 60(m) | 3.12 (s) | 1.61 (s) |
| ATE | 90 | 27 (m) | 2.52 (s) | 1.24 (s) |
| Total | 1194 | 449 (m) | 23.27 (s) | 11.73 (s) |
| No. of Classes | Class Name | CXR | CT Scan | Cough Sound | Total |
|---|---|---|---|---|---|
| 0 | COVID_19 | 423 | 426 | 100 | 949 |
| 1 | Normal | 247 | 672 | 210 | 1129 |
| 2 | TB | 259 | 112 | 292 | 663 |
| 3 | PNEU | 189 | 168 | 119 | 476 |
| 4 | LC | 174 | 118 | 222 | 515 |
| 5 | PNEUTH | 425 | 160 | 42 | 627 |
| 6 | ATE | 154 | 217 | 90 | 461 |
| 7 | COL | 154 | 112 | 80 | 346 |
| 8 | EDE | 198 | 91 | 39 | 328 |
| No. of Classes | Class Name | Total | Training (70%) | Validation (20%) | Testing (10%) |
|---|---|---|---|---|---|
| 0 | COVID_19 | 1129 | 790 | 225 | 114 |
| 1 | Normal | 1129 | 790 | 225 | 114 |
| 2 | TB | 1129 | 790 | 225 | 114 |
| 3 | PNEU | 1129 | 790 | 225 | 114 |
| 4 | LC | 1129 | 790 | 225 | 114 |
| 5 | PNEUTH | 1129 | 790 | 225 | 114 |
| 6 | ATE | 1129 | 790 | 225 | 114 |
| 7 | COL | 1129 | 790 | 225 | 114 |
| 8 | EDE | 1129 | 790 | 225 | 114 |
| Layer Type | Output Shape | Parameters |
|---|---|---|
| Input layer | (None, 128, 128, 3) | 0 |
| Block 1 | (None, 128, 128,8) | 224 |
| Block 2 | (None, 64, 64, 16) | 1168 |
| Block 3 | (None, 32, 32, 32) | 4640 |
| Block 4 | (None, 16, 16, 64) | 18,496 |
| Block 5 | (None, 8, 8, 128) | 73,856 |
| Dropout layer | (None, 4, 4, 128) | 0 |
| Flatten | (None, 2048) | 0 |
| Dense block 1 | (None, 512) | 1,049,088 |
| Dense layer | (None, 9) | 4617 |
| Output: SoftMax | (None, 9) | 0 |
| Total parameters: | 1,152,089 | |
| Trainable parameters: | 1,152,089 | |
| Non-trainable parameters: | 0 | |
| Classifiers | Accuracy | Precision | Recall | F1-Score | AUC | Trainable Parameters |
|---|---|---|---|---|---|---|
| DenseNet-201 | 85.37% | 87.85% | 84.42% | 84.88% | 98.22% | 5,431,999 |
| EfficientNet-B0 | 86.04% | 87.60% | 84.43% | 85.79% | 97.75% | 4,587,852 |
| InceptionResNet-V2 | 87.25% | 88.45% | 86.31% | 87.04% | 97.98% | 6,123,027 |
| Xception | 83.09% | 85.78% | 80.94% | 82.88% | 97.90% | 5,965,411 S |
| Proposed model (with BL-SMOTE) | 96.67% | 96.82% | 95.76% | 95.61% | 99.43% | 1,152,089 |
| Proposed model (without BL-SMOTE) | 66.15% | 75.17% | 58.66% | 55.48% | 95.31% | 2,263,190 |
| Sr# | Statistical Analyses | Outcomes |
|---|---|---|
| 1 | McNemar test | 0.0140 |
| 2 | ANOVA test | 0.0011 |
| Reference | Year | Model | Diagnostic Technique | Accuracy | Recall | F1-Score |
|---|---|---|---|---|---|---|
| [82] | 2021 | AlexNet | CXR | 94.00% | 91.30% | - |
| [83] | 2023 | ResNet101, DenseNet121, ResNet50, InceptionV3, and DenseNet169 | CXR | 92.00% | 91.00% | 90.00% |
| [84] | 2022 | CDC_Net | CXR | 90.39% | 90.13% | 92.26% |
| [85] | 2023 | DarkNet19 | CT scan | 94.91% | 93.96% | 94.52% |
| [86] | 2023 | SVM | CT scan | 95.90% | - | - |
| [87] | 2022 | MSCCov19Net | Cough sound | 90.40% | - | - |
| Ours | - | DCDD_Net with BL-SMOTE | CXR, CT scan, and cough sound/images | 96.67% | 95.61% | 99.43% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malik, H.; Anees, T.; Al-Shamaylehs, A.S.; Alharthi, S.Z.; Khalil, W.; Akhunzada, A. Deep Learning-Based Classification of Chest Diseases Using X-rays, CT Scans, and Cough Sound Images. Diagnostics 2023, 13, 2772. https://doi.org/10.3390/diagnostics13172772
Malik H, Anees T, Al-Shamaylehs AS, Alharthi SZ, Khalil W, Akhunzada A. Deep Learning-Based Classification of Chest Diseases Using X-rays, CT Scans, and Cough Sound Images. Diagnostics. 2023; 13(17):2772. https://doi.org/10.3390/diagnostics13172772
Chicago/Turabian StyleMalik, Hassaan, Tayyaba Anees, Ahmad Sami Al-Shamaylehs, Salman Z. Alharthi, Wajeeha Khalil, and Adnan Akhunzada. 2023. "Deep Learning-Based Classification of Chest Diseases Using X-rays, CT Scans, and Cough Sound Images" Diagnostics 13, no. 17: 2772. https://doi.org/10.3390/diagnostics13172772