1. Introduction
Cancer is a curse that threatens human life. It is characterized by the growth of abnormal cells, as well as their abnormal and out-of-control reproduction. Malignant cells invade and cause damage to neighboring organs. Any abnormal growth is a precursor to a tumor, whether benign or malignant. The benign tumor remains in its place and does not invade the adjacent normal tissues [
1], while the malignant tumors infiltrate the neighboring normal cells and destroy them [
2]. Cervical cancer is the fourth type of malignant tumor that threatens a woman’s life if detected late [
3]. Cervical cancer appears in the lower cervical tissues, which grow abnormally and out of control [
4]. According to World Health Organization reports [
5], 342,000 women died in 2020 due to cervical cancer [
6]. Human papillomavirus (HPV) is a virus of the genital tract and is the main cause of cervical cancer [
7]. HIV-positive women are more likely to develop cervical cancer at a younger age and with more advanced disease. This is because HIV infection can speed up the progression of HPV infection from precancerous to cancerous cells [
8]. Cervical cancer slowly grows and spreads, so no symptoms appear in the early stages [
9]. Therefore, regular screening is the best way to prevent cervical cancer. Squamous cell carcinoma is a type of cancer that begins in the squamous cells, which are the flat cells that line the outer part of the cervix. It is the most common type of cervical cancer, accounting for about 80% of all cases. Squamous cell carcinomas are often aggressive and can spread quickly to other parts of the body if not diagnosed and treated early [
10]. There are some symptoms that occur in the advanced stages, such as abnormal vaginal bleeding, hematuria, pelvic pain, bleeding, and dysuria. Cervical cancer begins at the bottom of the cervical tissue and progresses as it spreads to other places [
11]. In the second stage, the abnormal cells spread to the vagina, although the recovery rate remains high. In the third stage, the abnormal cells spread to the lymph nodes in the pelvis and vagina and cause kidney problems. At this stage, the chance of recovery becomes low. In the fourth stage, abnormal cells spread outside the pelvis and invade the bladder and other nearby organs. This stage is difficult to treat. At this stage, the patient only receives pain-relieving health care [
12]. There are several techniques for cervical cancer screening that have led to a lower mortality rate. There are consistent techniques for detecting abnormal cervical intraepithelial cells, such as smear techniques. There are also techniques for examining the cervix, such as liquid-based cytology (LBC), microscopy, digital colposcopy, and HPV testing [
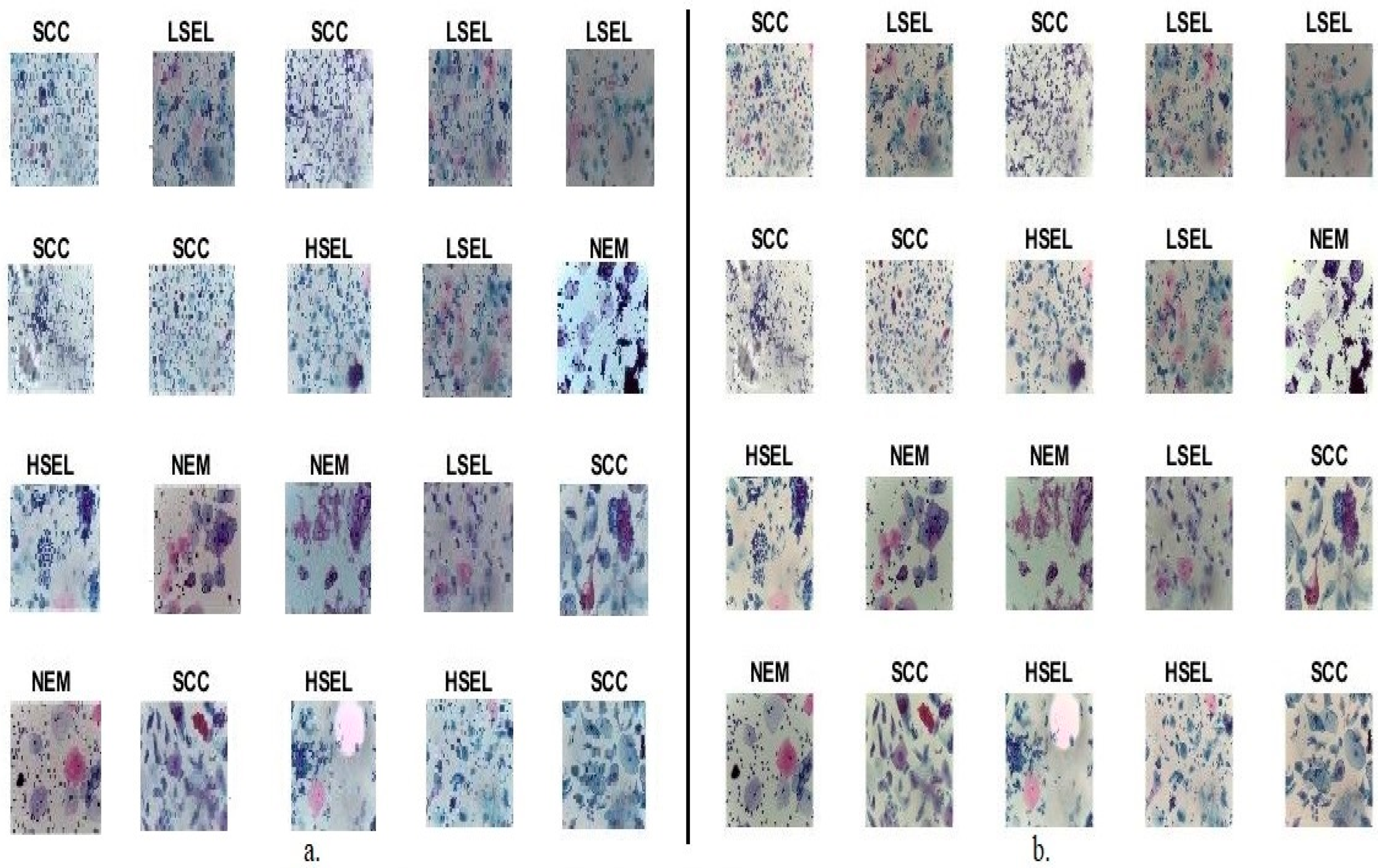
13]. The LBC is a method of collecting and preparing cervical cells for testing. It is a newer method than the traditional Pap smear, and it has several advantages. In a traditional Pap smear, a sample of cells is taken from the cervix and smeared onto a glass slide. The slide is then stained and examined under a microscope by a cytotechnologist or pathologist. In LBC, the cells are collected in a liquid preservative solution. The solution is then centrifuged, which separates the cells from the liquid. The cells are then spread onto a slide and stained. LBC has several advantages over traditional Pap smears. It is more sensitive, meaning that it is more likely to detect abnormal cells. It is also more specific, meaning that it is less likely to produce false-positive results. LBC is also less likely to be affected by blood or other debris, which can make it difficult to interpret traditional Pap smears. LBC is the preferred method of cervical cancer screening in many countries. It is more effective than traditional Pap smears, and it is less likely to be affected by blood or other debris. Thus, LBC technology played a key role in analyzing cervical smears and detecting the type of cervical cancer to help patients receive appropriate health care. The doctor magnifies the LBC slice under the microscope to different magnification factors such as 400×. Therefore, the doctor obtains thousands of cells, which must be carefully examined [
14]. In the initial stages, a few abnormal cells may appear that doctors may not focus on, causing a wrong diagnosis. The gap between the number of experienced doctors and patients is also one of the challenges facing health care. The examination of LBC slides is codified and time-consuming, and it is subject to differing doctors’ opinions about the diagnosis. Thus, automated computer-assisted techniques solve the challenges of manual diagnosis. The WSIs are a method of numbering glass slides obtained with WSI scanners [
15]. WSI allows for the digital viewing and analysis of tissue sections. Thus, the advent of WSI images led to the use of machine and deep learning (DL) to analyze images of cervical cells to assist doctors in analyzing WSI images, segmenting, and classifying cells, as well as predicting the type of cervical cancer.
Early diagnosis plays a crucial role in the effective management and treatment of cervical cancer. The WSI has emerged as a powerful tool in the field of pathology, allowing for the digitization and analysis of histopathological slides. However, the quality of WSI images can significantly impact the accuracy and reliability of diagnostic assessments. One fundamental aspect of improving WSI image quality is enhancing resolution. Higher-resolution images provide finer details and enable pathologists to better visualize cellular structures and tissue morphology. Various techniques can be employed for resolution enhancement. These techniques aim to reconstruct high-resolution images from low-resolution counterparts, thus enhancing WSI images’ overall quality and diagnostic potential. Noise, such as random variations in pixel values, can degrade the quality of WSI images and introduce artifacts that may hinder accurate diagnosis. Effective noise reduction techniques, such as spatial filtering and wavelet denoising, can be applied to minimize noise while preserving important image features. By reducing noise, the clarity and visibility of cellular structures and pathological characteristics are improved, aiding pathologists in making accurate assessments. WSI images may contain artifacts, including dust particles, stains, and tissue folds, which can obstruct the visibility of critical features. These artifacts can be removed using various techniques, such as morphological operations, adaptive filtering, and inpainting algorithms. By effectively eliminating artifacts, the clarity and accuracy of WSI images are enhanced, enabling pathologists to focus on relevant structures and abnormalities. Enhancing the contrast of WSI images can improve the visibility of subtle features and facilitate the identification of abnormal tissue patterns. Contrast enhancement techniques, such as histogram equalization, adaptive contrast stretching, and retinex-based methods, can be employed to amplify the differences in pixel intensity values across the image. This enhancement enables better discrimination between healthy and abnormal tissue regions, aiding in the early detection and diagnosis of cervical cancer. Improving the quality of WSI images is vital for early diagnosis and the accurate assessment of cervical cancer. By employing techniques such as resolution enhancement, noise reduction, color correction, artifact removal, contrast enhancement, and image registration, the overall quality and diagnostic utility of WSI images can be significantly improved. These candidates provide valuable avenues for research and development, aiming to advance the field of early detection and diagnosis of cervical cancer using WSI technology. DL networks play a vital role in analyzing WSI images to extract salient and hidden characteristics, as well as biomarkers, that cannot be detected by manual diagnosis. There is a similarity between the characteristics of the types of cervical cancer, especially in the early stages. Therefore, to receive the appropriate treatment, DL networks have the superior ability to extract the characteristics of each type of cervical cancer to help doctors distinguish between types of cervical cancer [
16]. In this study, to solve the challenge of the similarity of cervical cancer types, the focus was on extracting features from more than one CNN model, integrating them sequentially into vectors and classifying them using RF and SVM networks.
Here, previous studies on techniques were used to analyze the images of the cervical cancer dataset and the results that were reached.
Kavitha et al. [
17] applied a technique to improve cervical images by Dynamic Fuzzy Histogram Equalization and to identify regions of interest by fuzzy c-mean. The ant colony optimization method was applied to select and classify the traits by CNN and ANN. Badiea et al. [
18] applied a CNN hybrid method with SVM for the analysis of WSI images of the cervix. CNN layers extracted the features, and PCA selected the features. The SVM based on the GoogLeNet features achieved an accuracy of 96.8%. Hiam et al. [
19] used a method for integrating DL features with Shuffle Net to classify cervical cancer. PCA and canonical correlation (CCA) methods were applied to obtain discriminatory features for each class. The discriminatory features of the CCA method were classified by ML methods SVM, RF, and ANN, which reached an accuracy of 91.1%, 94.7%, and 94.9%, respectively. Jesse et al. [
20] analyzed cervical cancer risk factors using the decision tree algorithm. A recursive feature elimination (RFE) method was applied to select the predictive characteristics of cervical cancer. SMOTE Tomek was applied to collate the dataset. The decision tree reached an accuracy of 95.29%. Odai et al. [
21] presented a system for predicting cervical cancer using the Genetic Method (GM), PCA, and MLP Algorithm. The GM optimizes the parameters of the MLP, and the prediction is simulated within the GM by the MLP. The features were fed into several classifiers, where the RF achieved an accuracy of 92.16%, a specificity of 85.57%, and a precision of 87.22%. Mingmei et al. [
22] applied an unsupervised ML method for analyzing cervical cytology images. The images improved, and the PCA was applied to represent the features in a low-dimensional space. The method yielded a sensitivity of 81.8% and a specificity of 86.5%. Park et al. [
23] applied a DL and ML method for cervical cancer detection. The images were optimized, and 300 features were extracted and classified by XGB and SVM. Validated tests and ROC analysis yielded an AUC of 82% and 84% for both XGB and SVM. Yoon et al. [
24] used a CNN based on acetowhite for cervical cancer detection. A comparison was made between the method before and after improvement in the area of interest, where the method based on acetowhite reached an accuracy of 81.31%. Naif et al. [
25] developed several ML methods based on the previous stages: image optimization and selection of vital features for each class by predictive model selection (PMS). Phasit et al. [
26] developed an RF-based cervical cancer prediction model called iPMI. Features were extracted along with clinical characteristics with characteristics of cervical neighboring regions called iPMI-Econ. The iPMI–Power method showed a superiority of 86.2%, a sensitivity of 60%, and an AUC of 90.5%. Madhura et al. [
27] applied a hybrid method between machine learning and fuzzy min–max neural to analyze and extract features from cervical images. The method took advantage of fuzzy min–max neural features, as Resnet-50 reached an accuracy of 95.33%. Deborah et al. [
28] featured an analysis of the nuclei of cervical cells and their classification by a hierarchical method of ML algorithms. Quality results were obtained through a hierarchical classification with RF, which yielded an accuracy of 95.34%, a precision of 84.31%, and a sensitivity of 84%. Mohammed et al. [
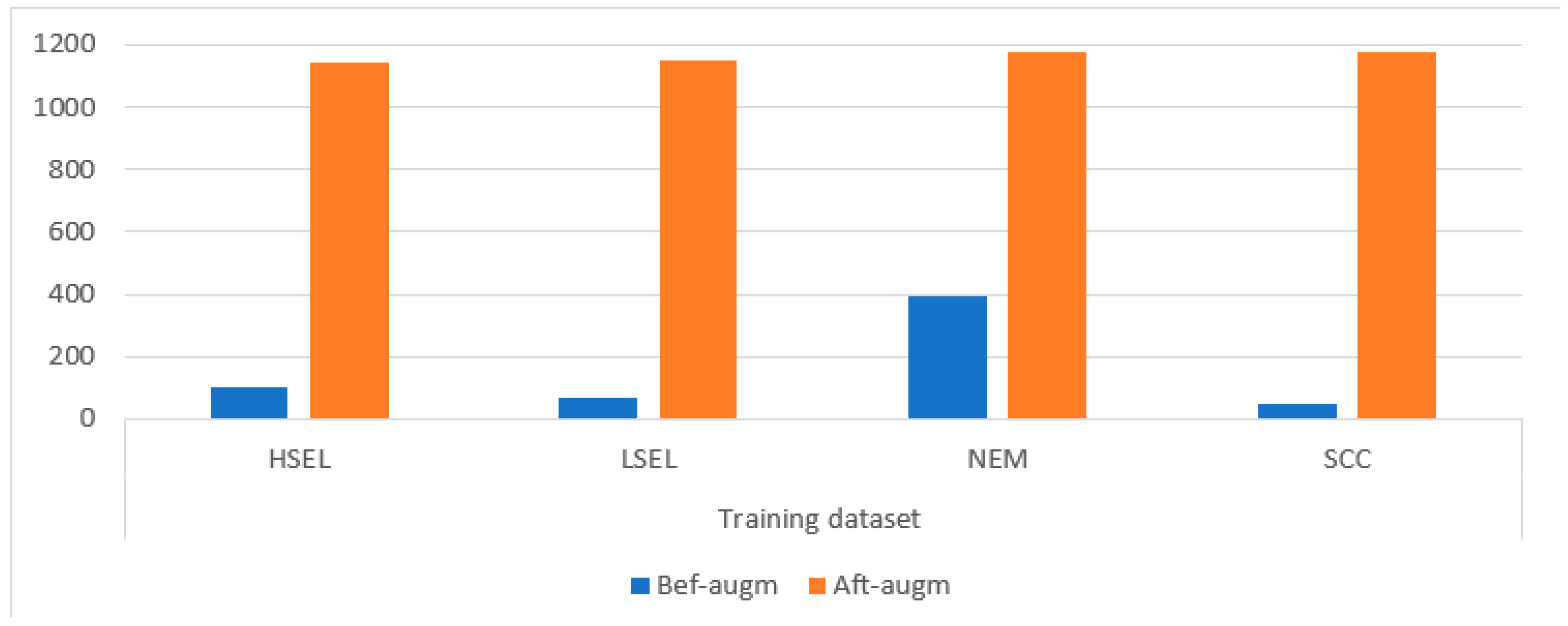
29] applied a DL network for the analysis of all-cell of WSI images of the cervix. A median filter has been applied to improve the images and augment the data to balance the classes. The systems performed better after the image improvement process. Débora et al. [
30] used DL models for analyzing cervical cells for cervical cancer detection. Deep features were extracted from the cervical cancer dataset and classified, where the XceptionNet model yielded an accuracy of 93%, sensitivity of 80%, and specificity of 80%. Shervan et al. at [
31] applied three deep networks to extract features and replace the classification layers with MLP, KNN, and RF networks. The MLP, KNN, and RF networks resulted in an accuracy of 96.53%, 94.43%, and 95.51%, respectively.
Nitin et al. [
32] proposed a hybrid deep feature concatenated network (HDFCN) for the detection of cervical cancer in WSI images. The network combined features from three deep-learning models. WSI images were enhanced to high resolution and resized to pixels to reduce computational costs and fit into deep-learning models. The performance of the proposed HDFCN model was compared to individual deep-learning models. The results showed that the HDFCN model outperformed the individual models in classifications, achieving an accuracy of 97.45%. Ishak et al.’s [
33] study employed state-of-the-art deep-learning techniques, specifically in two categories: CNN approaches and vision transformer (ViT) approaches. To make the models efficient, WSI images were optimized to high resolution and resized to a manageable number of pixels. The experimental results showed that the latest ViT-based models outperformed the CNN models, while the existing CNN models performed similarly to the ViT models. By leveraging data augmentation and ensemble-learning techniques in ViT-based models, the research achieved a level of success. Yuan et al. [
34] aimed to address the grade classification problem on segmented epithelium patches using conditional Generative Adversarial Networks (cGANs). The study introduced a synthetic-image filtering mechanism based on the divergence in feature space between the generated images and class centroids. This filtering process aimed to control the quality of selected synthetic images for data augmentation, ensuring that only meaningful features were included. The results demonstrated a significant improvement in classification accuracy. Specifically, the classification accuracy increased from 66.3% to 71.7% when utilizing the cGAN generated images with feature-based filtering.
It is noted that researchers devoted their efforts to designing techniques with various tools to reach satisfactory results. However, because of the similarity of cervical cancer cell types in their early stages, diagnostic accuracy is still the goal of every researcher. This study focuses on various techniques for extracting fused features by CNN models and replacing the classification layers of CNN with other algorithms. This study reached satisfactory results compared to previous related studies, which is due to the extraction of fused features between CNN models and the application of dimension reduction techniques to select important features only.
The main contributions of this study are as follows:
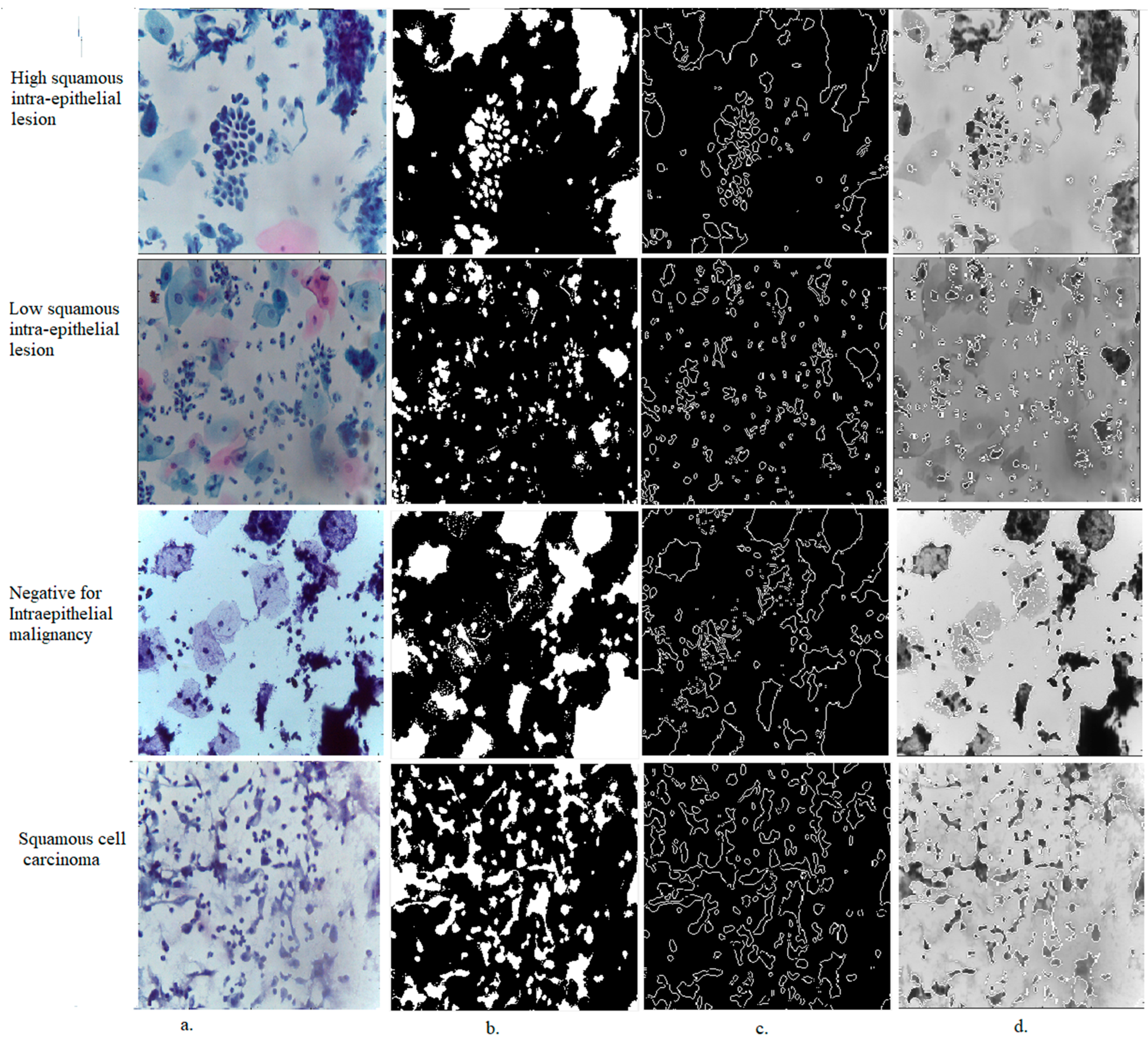
Applying two successive filters to improve the quality of WSI images and show the edges of low-contrast cells.
Applying the ACA algorithm to separate the cells to be analyzed, separating them from the rest of the image, and saving them in a new file to feed them into DL models.
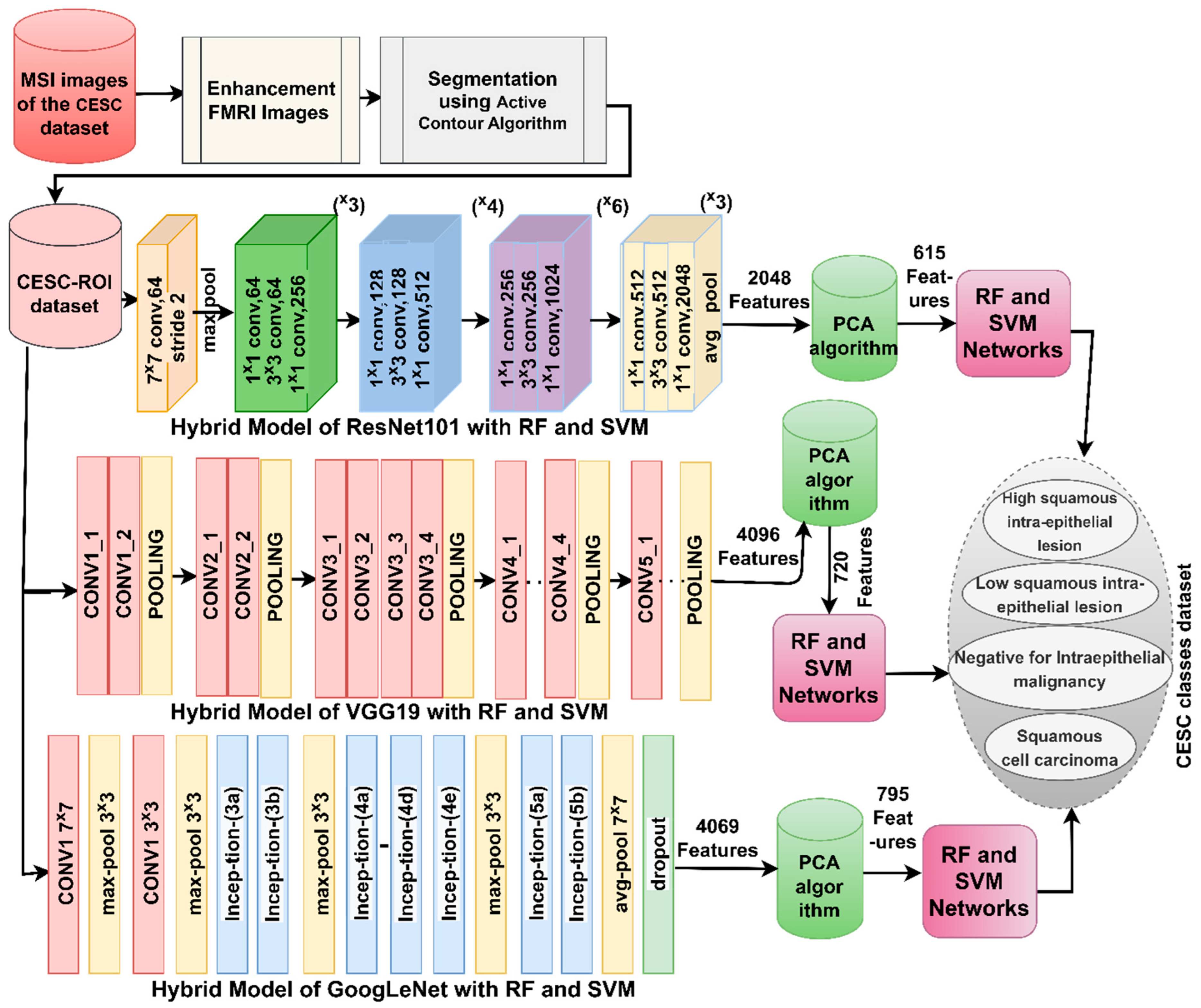
Developing a hybrid technique between machine-learning algorithms (RF and SVM) and ResNet50, VGG19, and GoogLeNet models for analyzing WSI images for cervical cancer diagnosis.
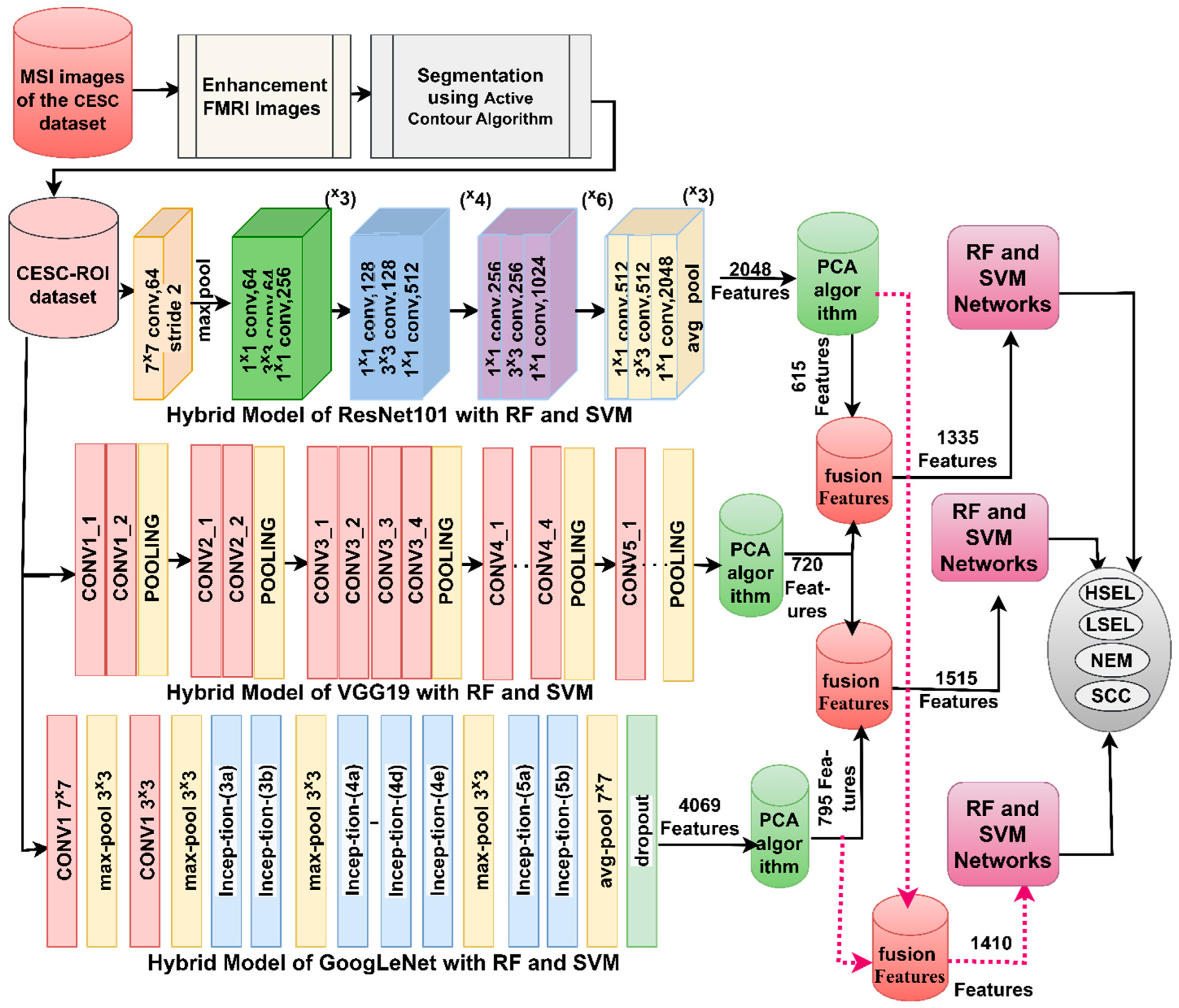
Developing a technique to extract the fused features of DL models (ResNet50-VGG19, VGG19-GoogLeNet and ResNet50-GoogLeNet) and classify them by RF and SVM algorithms.
The remainder of the study is arranged as follows:
Section 2 summarizes the methods and results of several previous studies.
Section 3 explains the various techniques and tools applied to analyze WSI images of abnormal cells of cervical cancer.
Section 4 presents the results of the proposed approaches in the study.
Section 5 compares the performance of the proposed approaches and concludes with the best performance compared to the studies mentioned in
Section 2.
Section 5 concludes the study.
4. Discussion of the Performance
Cervical cancer is one of the deadliest types of ailments for women. HPV is one of the main causes of cervical cancer. Early diagnosis of cervical cancer is the only means to receive appropriate treatment and recover. The similarity between the vital characteristics of the types of cervical cancer or the stages of cancer development makes it difficult for doctors to distinguish the stages. Thus, artificial intelligence techniques solve the shortcomings of manual diagnosis. Many researchers discussed various techniques and algorithms and their findings. It is noted from previous studies that there are shortcomings in terms of pathological accuracy. Therefore, due to the similarity of clinical characteristics between cancer stages, this study aimed to extract features from several DL models and combine them.
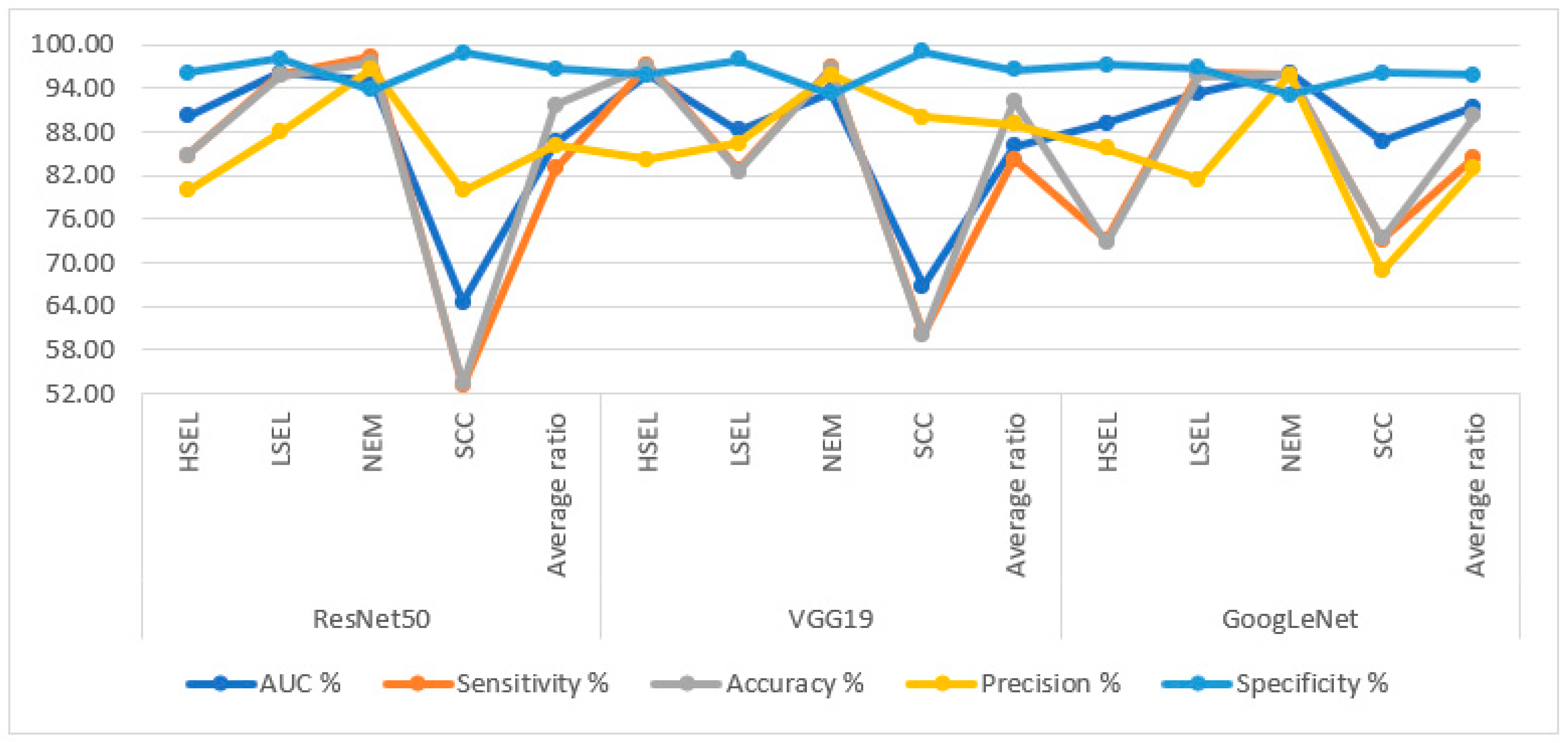
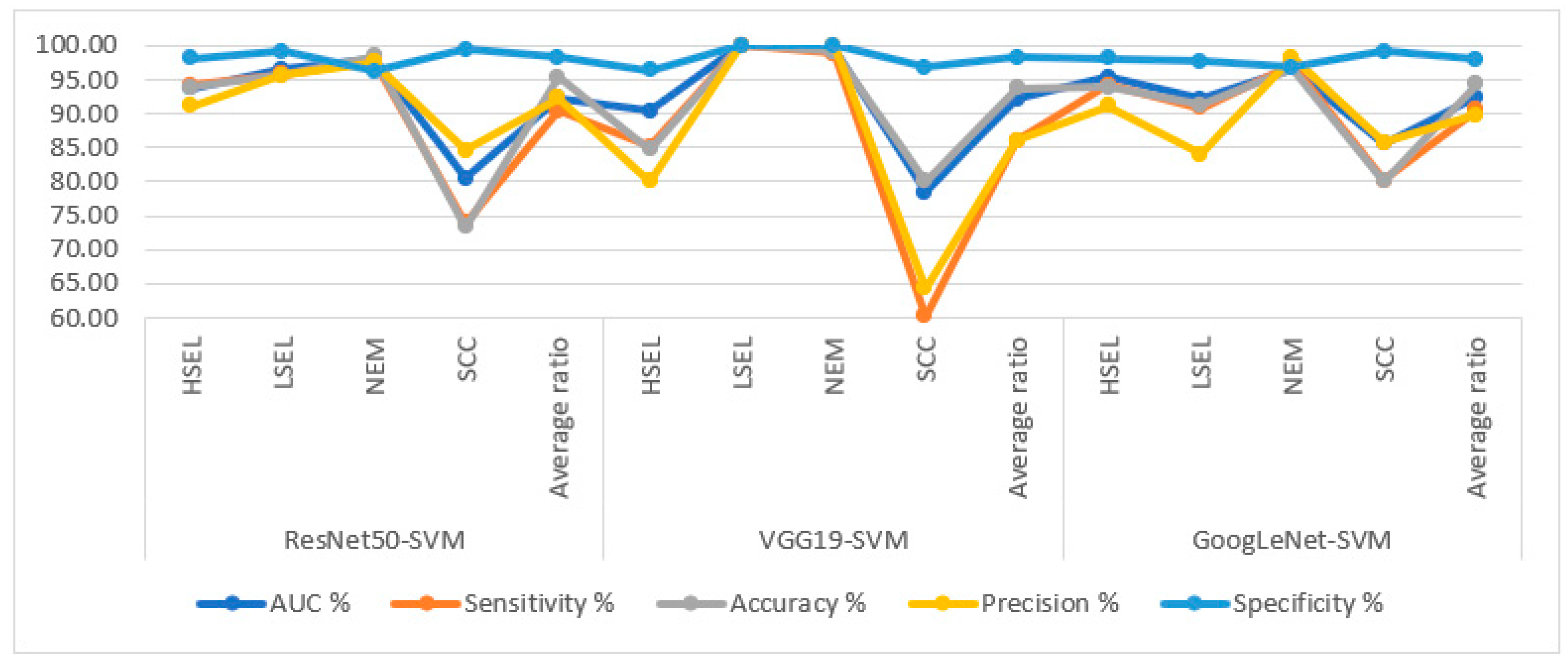
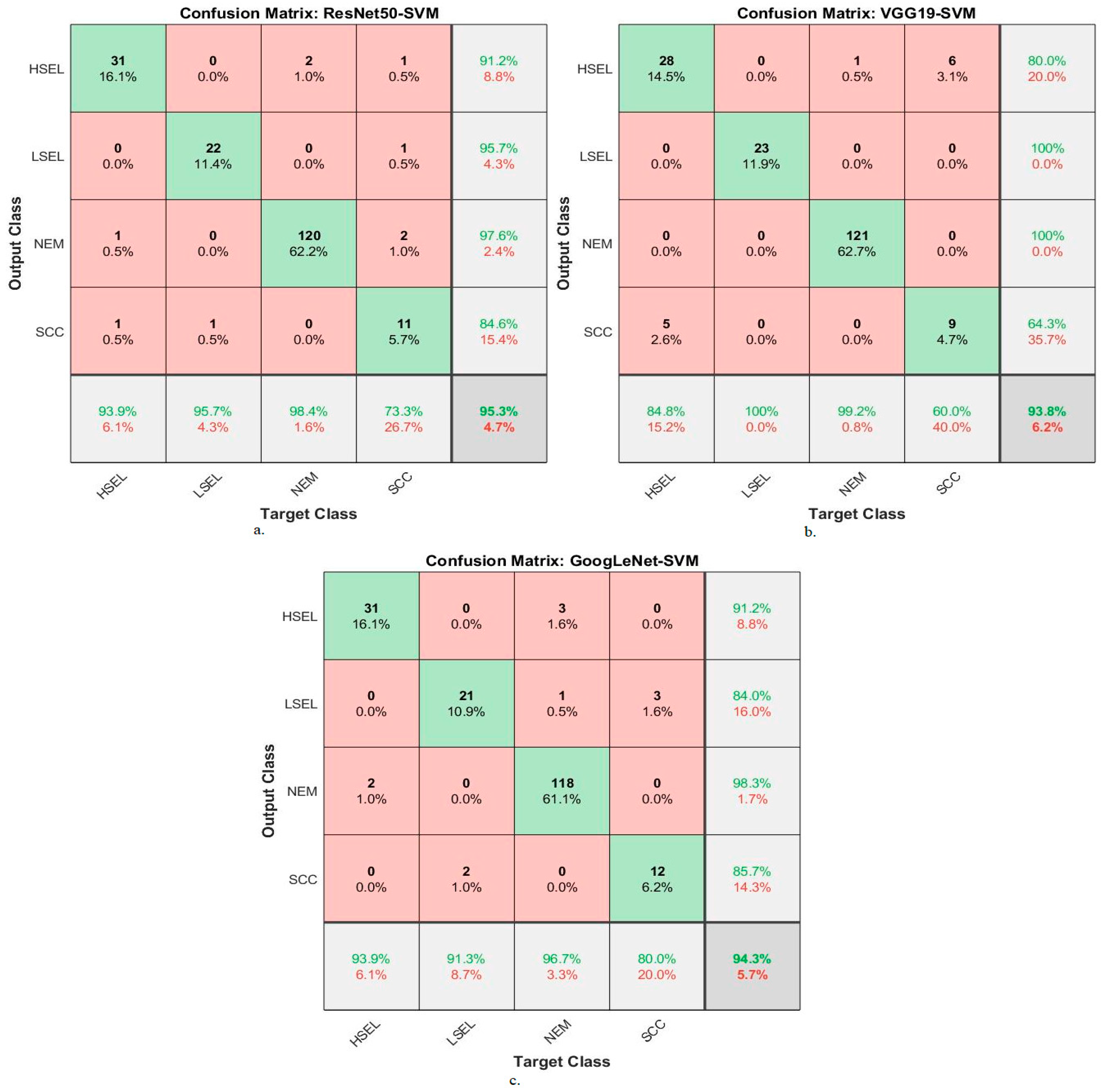
In this study, WSI images for diagnosing squamous cell carcinoma of the cervix were analyzed by several approaches. The first approach to analyze WSI images for cervical cancer diagnosis is through pre-trained ResNet50, VGG19, and GoogLeNet models. The ResNet50, VGG19, and GoogLeNet models achieved an accuracy of 91.7%, 92.2%, and 90.2%, respectively.
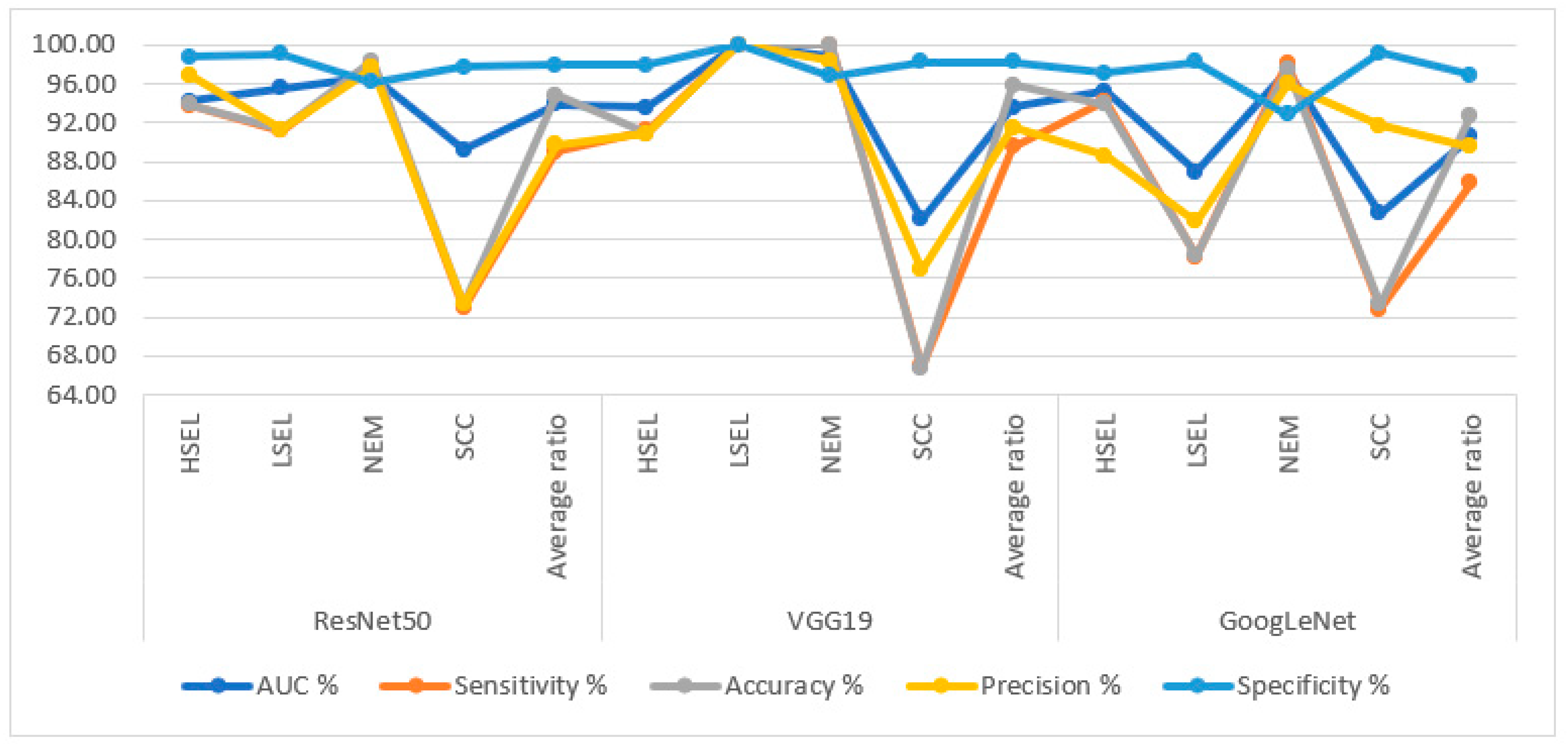
The second approach to analyze WSI images for cervical cancer diagnosis through ResNet50, VGG19, and GoogLeNet models was based on the ACA algorithm to segment and isolate regions of interest from non-significant regions. The second approach notes an improvement in the performance of ResNet50, VGG19, and GoogLeNet models thanks to the segmentation algorithm before feeding images to DL models. ResNet50, VGG19, and GoogLeNet models based on the ACA algorithm achieved an accuracy of 94.8%, 95.9%, and 92.7%.
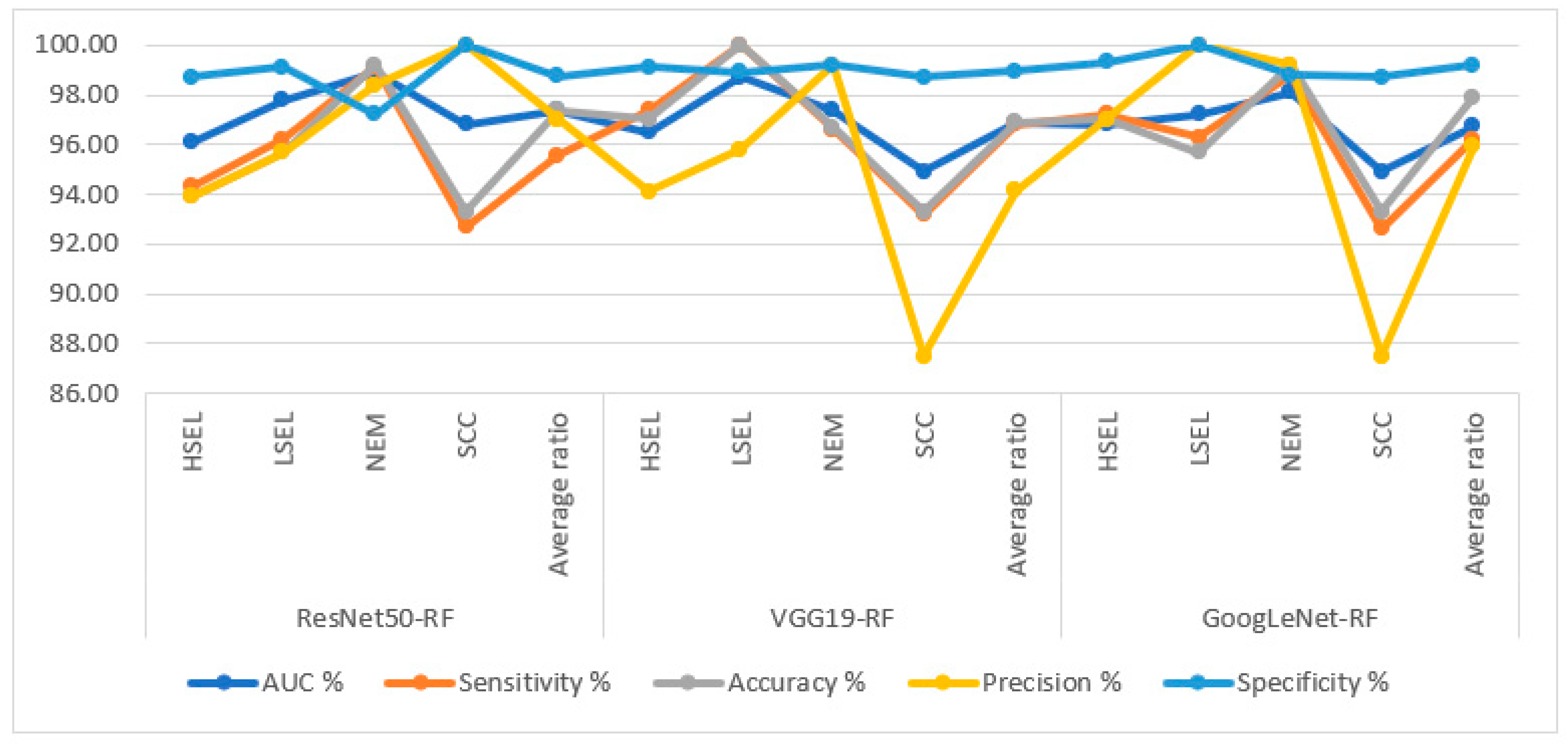
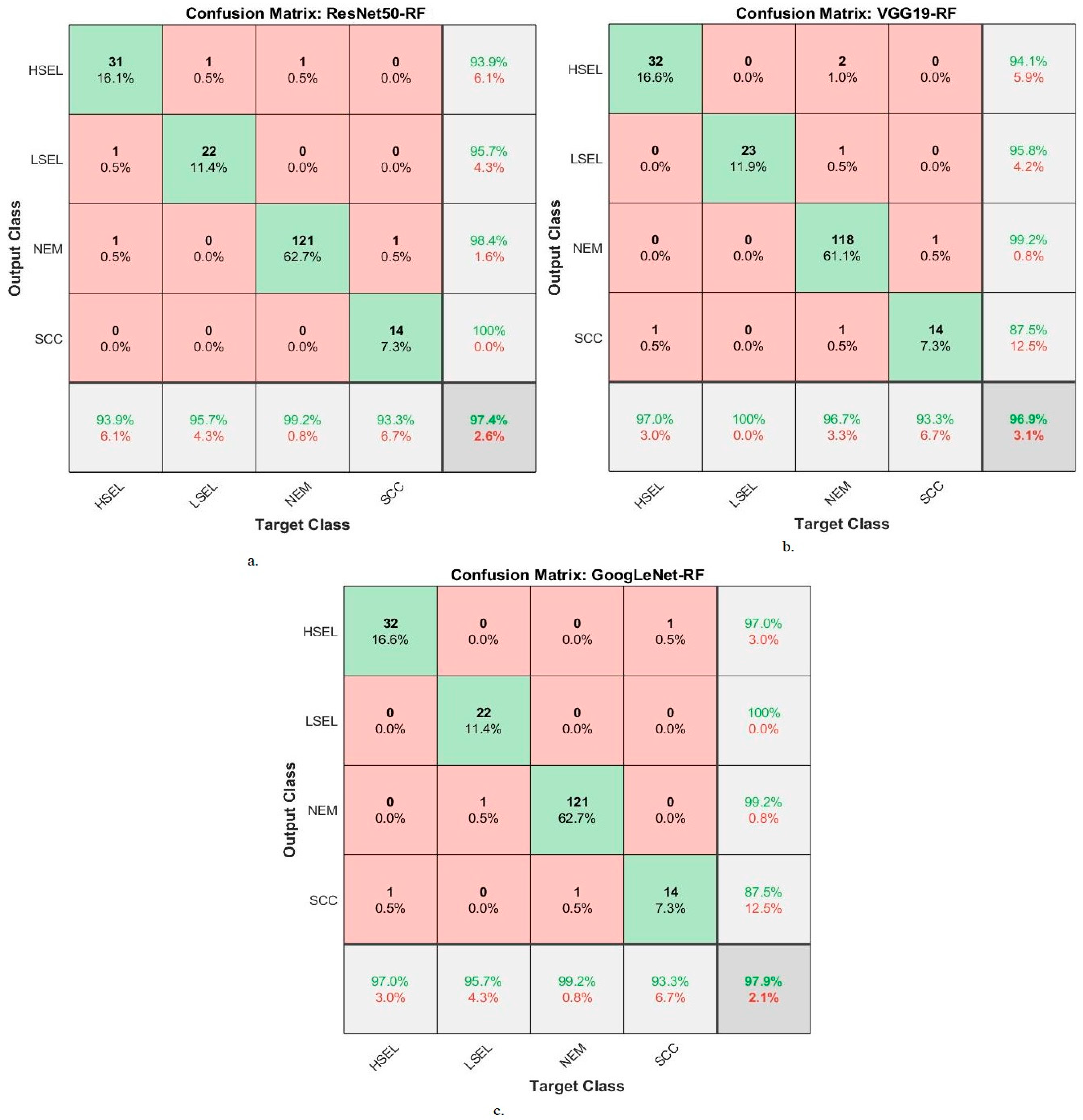
The third approach is based on a hybrid of DL models and RF and SVM algorithms. In this technique, ResNet50, VGG19, and GoogLeNet models were fed after applying the ACA algorithm, and the images were analyzed to extract the high-dimensional features. The PCA method receives high-dimensional features to select representative features and eliminate non-significant and redundant features. Finally, the RF and SVM algorithm receives representative features to classify each image into the appropriate class with high accuracy. It is noted that the results of the RF algorithm based on the characteristics of DL demonstrated greater improvement than the first and second approaches. The ResNet50-RF, VGG19-RF, and GoogLeNet-RF approaches achieved an accuracy of 97.4%, 96.9%, and 97.9%, respectively.
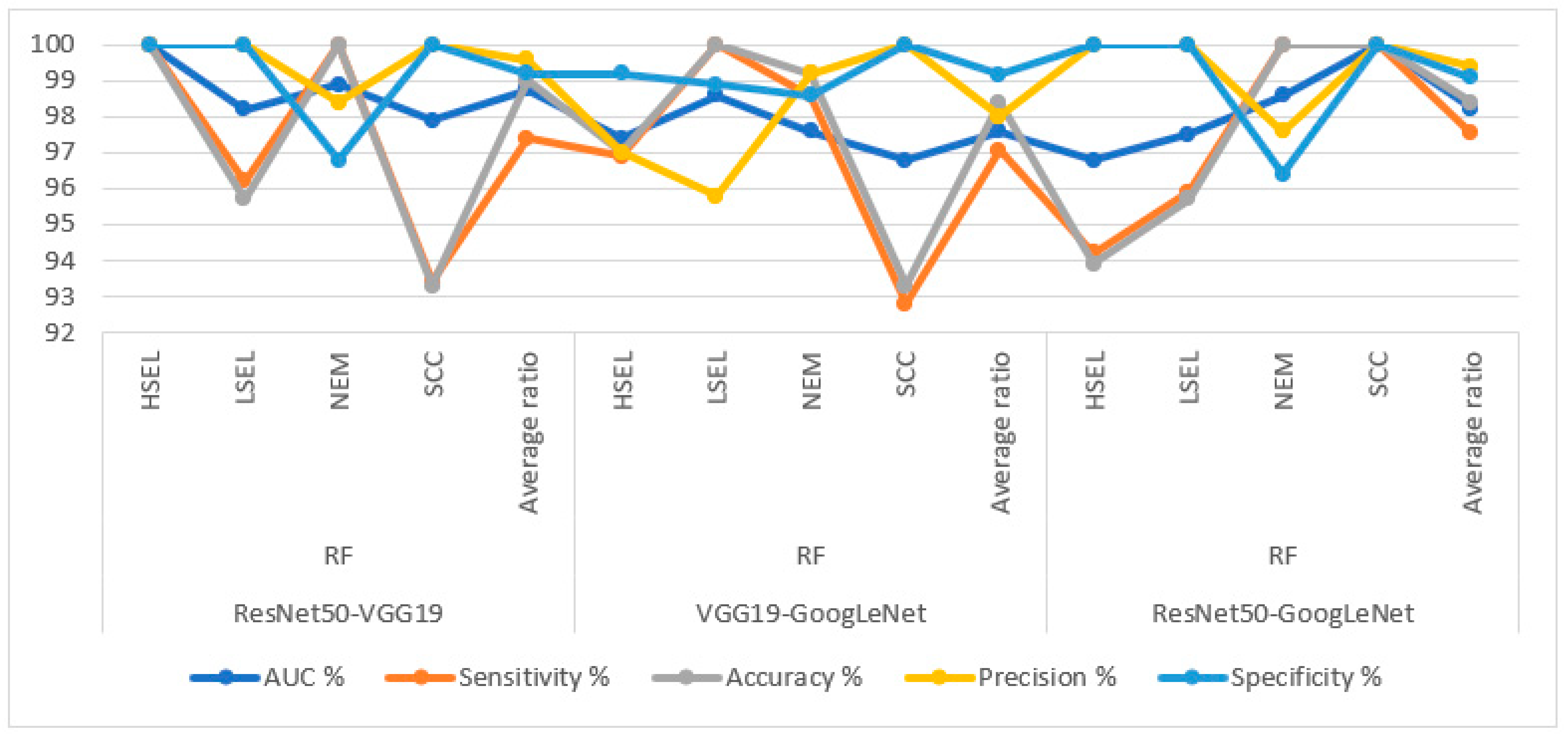
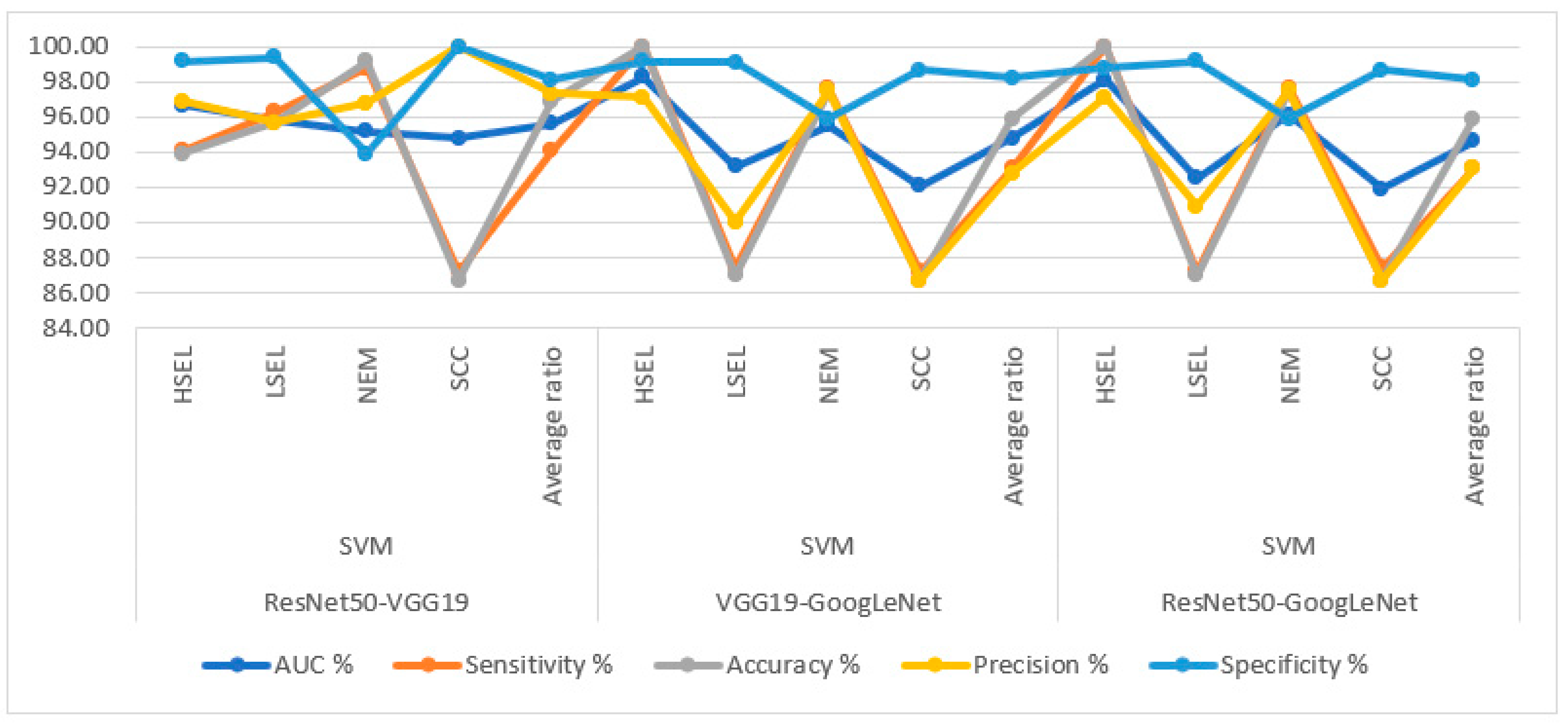
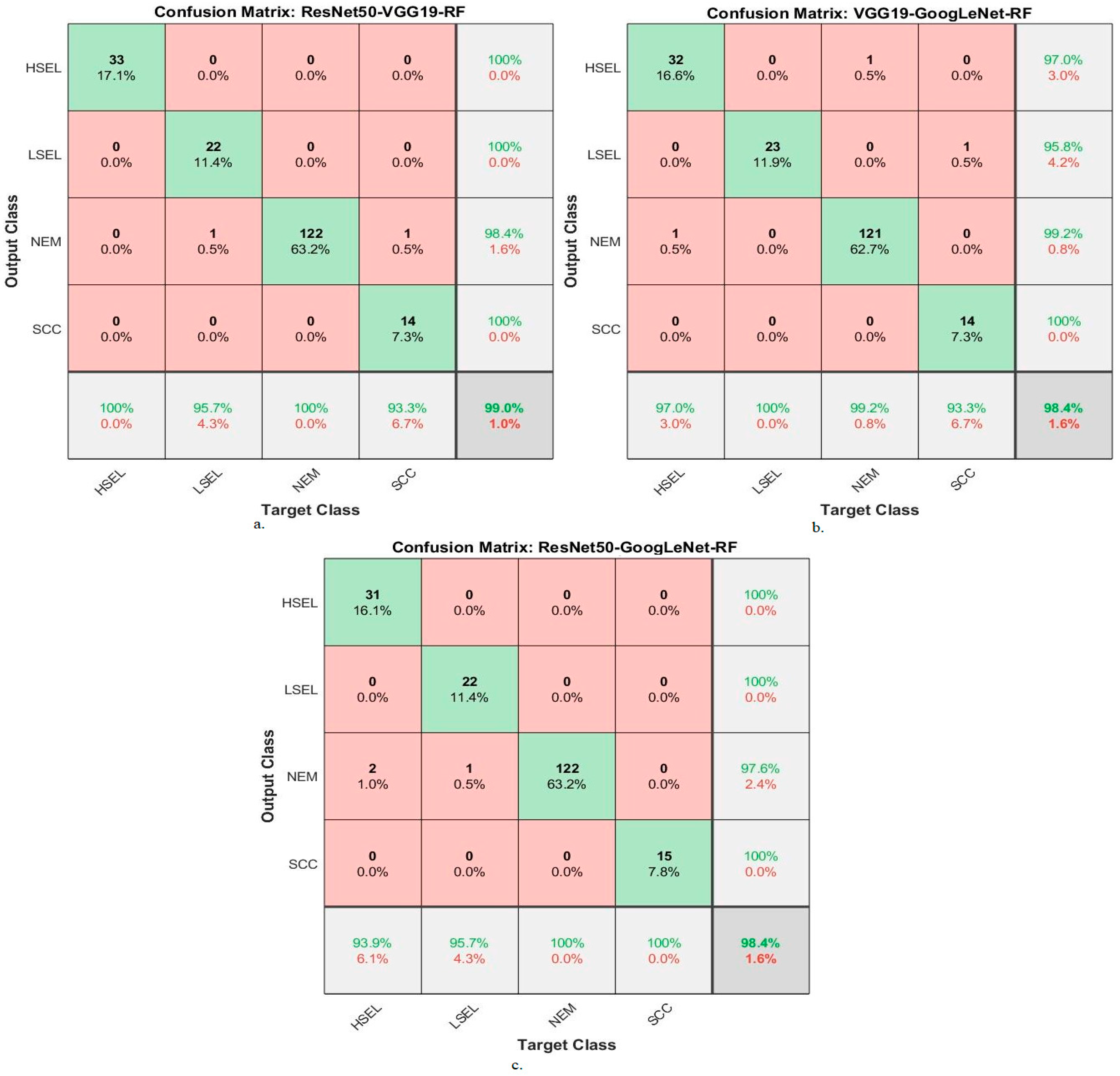
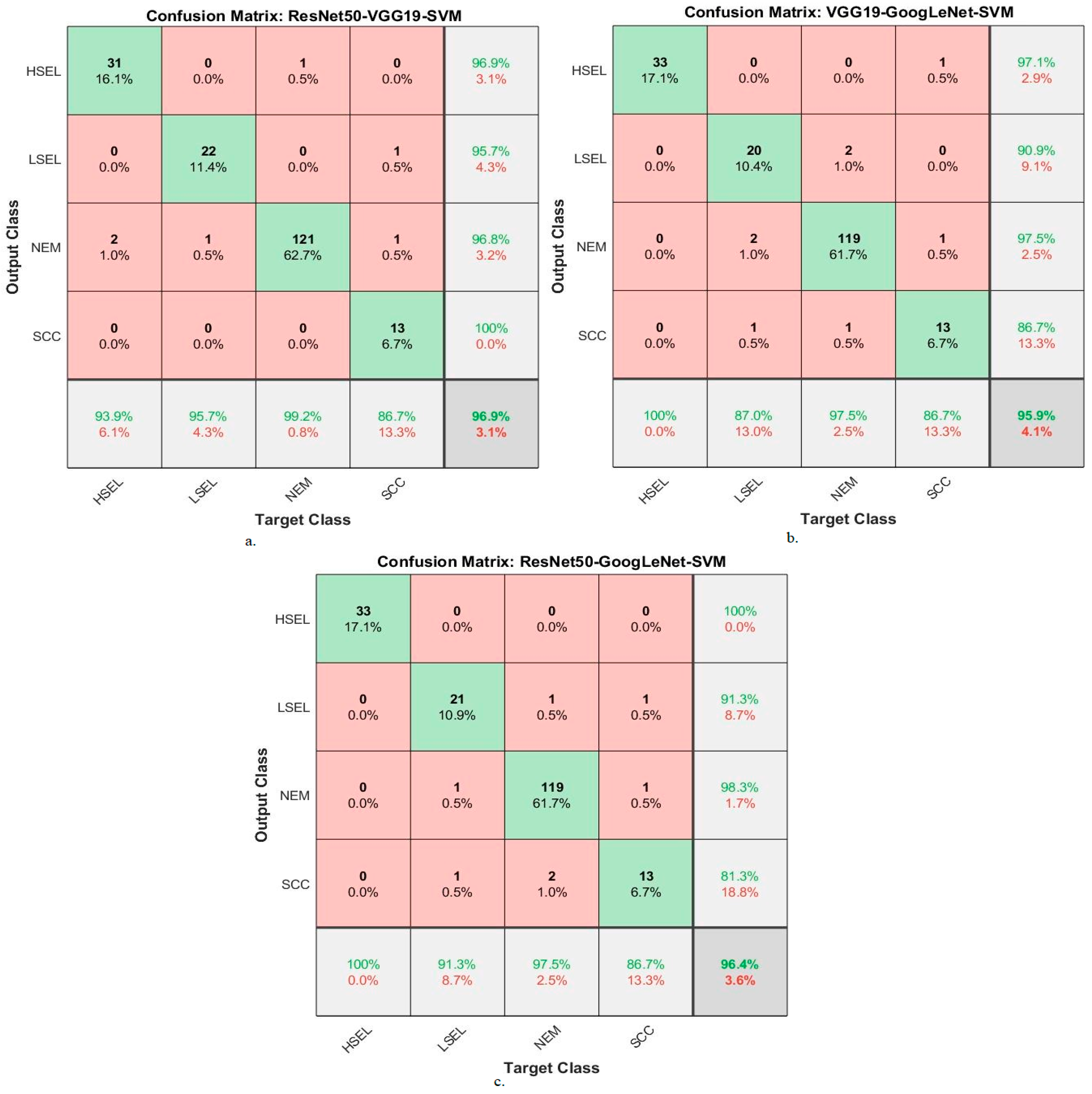
The fourth approach is based on analyzing WSI images for cervical cancer diagnosis by RF and SVM algorithms based on integrating the features of DL models. In this approach, WSI image cells are segmented and fed into ResNet50, VGG19, and GoogLeNet models, WSI image cells are analyzed, and high-level features are extracted. After that, the PCA method was applied to eliminate the repeated features and save the most important features. The features of the low-dimensional DL models are combined: ResNet50-VGG19, VGG19-GoogLeNet, and ResNet50-GoogLeNet. Finally, the RF and SVM algorithms receive the DL-fused features. Experiments with this approach have proven high performance compared to previous approaches thanks to the combination of the features of DL models. The RF algorithm with the features of the models ResNet50-VGG19, VGG19-GoogLeNet, and ResNet50-GoogLeNet reached an accuracy of 99%, 98.4%, and 98.5%, respectively.
The reason behind the improvement in results across the approaches lies in the combination of different techniques and algorithms. The first approach leverages pre-trained DL models to directly classify the WSI images, but without any specific preprocessing. The second approach introduces the ACA algorithm for segmentation, isolates the regions of interest, and reduces noise, which enhances the DL models’ performance. The third approach combines DL models with RF and SVM algorithms, allowing for better feature representation and classification. Finally, the fourth approach integrates the features from different DL models, further refining the representation of the images and achieving the highest accuracy. Each subsequent approach builds upon the strengths and limitations of the previous ones, resulting in incremental improvements in performance.
In our study, a system for cervical cancer diagnosis based on analyzing whole slide imaging (WSI) images was proposed. We compare our approach with several previous studies that employed different methods and achieved varying results. Here, we summarize the previous studies and their outcomes. Kavitha et al. [
18] used Dynamic Fuzzy Histogram Equalization for image enhancement and fuzzy c-mean for the region of interest identification. Ant colony optimization, CNN, and ANN were used for trait selection and classification. Badiea et al. [
19] applied a hybrid method using CNN and SVM for WSI image analysis. GoogLeNet features combined with SVM achieved an accuracy of 96.8%. Hiam et al. [
20] integrated DL features with Shuffle Net for cervical cancer classification. PCA and CCA were used for feature extraction, and SVM, RF, and ANN achieved accuracies of 91.1%, 94.7%, and 94.9%, respectively. Jesse et al. [
21] used a decision tree algorithm and RFE for feature selection in cervical cancer risk factor analysis. The decision tree achieved an accuracy of 95.29%. Odai et al. [
22] presented a system for predicting cervical cancer using GM, PCA, and MLP. RF achieved an accuracy of 92.16%, a specificity of 85.57%, and a precision of 87.22%. Mingmei et al. [
23] applied unsupervised ML for analyzing cervical cytology images. Their method achieved a sensitivity of 81.8% and specificity of 86.5%. Park et al. [
24] used DL and ML methods for cervical cancer detection. XGB and SVM achieved AUC values of 82% and 84%, respectively. Yoon et al. [
25] employed a CNN-based method for cervical cancer detection using acetowhite images. The accuracy of their method was reported as 81.31%. Naif et al. [
26] developed ML methods based on image optimization and feature selection using PMS. No specific accuracy results were provided. Phasit et al. [
27] developed an RF-based prediction model for cervical cancer using iPMI-Econ and iPMI-Power features. Their method achieved a superiority of 86.2%, sensitivity of 60%, and an AUC of 90.5%. Madhura et al. [
28] applied a hybrid method combining machine learning and fuzzy min–max neural networks. Their approach achieved an accuracy of 95.33% using ResNet-50. Deborah et al. [
29] performed feature analysis and hierarchical classification of cervical cells using ML algorithms. RF achieved an accuracy of 95.34%, a precision of 84.31%, and a sensitivity of 84%. Mohammed et al. [
30] used DL networks for analyzing WSI images of cervical cells. After image improvement, their systems showed better performance, but specific accuracy results were not provided. Débora et al. [
31] used DL models, specifically XceptionNet, for cervical cancer detection. The accuracy, sensitivity, and specificity achieved were 93%, 80%, and 80%, respectively. Shervan et al. [
32] employed deep networks (MLP, KNN, and RF) for feature extraction and classification. Accuracy results were reported as 96.53%, 94.43%, and 95.51% for MLP, KNN, and RF, respectively. In our proposed system, we analyze WSI images for cervical cancer diagnosis using RF and SVM algorithms. We integrate features from DL models, specifically ResNet50, VGG19, and GoogLeNet. The features are combined using PCA to eliminate redundant features. The fused features from ResNet50-VGG19, VGG19-GoogLeNet, and ResNet50-GoogLeNet are then fed into RF and SVM algorithms. Our experiments showed that our approach outperformed previous methods. The RF algorithm achieved accuracies of 99%, 98.4%, and 98.5% with ResNet50-VGG19, VGG19-GoogLeNet, and ResNet50-GoogLeNet features, respectively. Overall, our proposed system demonstrates improved performance compared to previous studies by leveraging the combination of features from DL models and utilizing RF and SVM algorithms for classification.
We conclude that the segmentation of WSI images of cervical cancer cells by the ACA algorithm was effective in improving performance. The DL-RF and DL-SVM hybrid models perform better than the pre-trained DL models. We also conclude that the performance of the two RF and SVM algorithms based on the merged DL models is better than its performance with DL features without merging the feature vectors.


 ,
, 















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}