1. Introduction
Nasopharyngeal cancer is a malignant tumor originating from nasopharyngeal mucosal epithelial cells. It is prevalent in southern China and Southeast Asia, and its incidence rate is 20–30/10,000/year [
1]. Nasopharyngeal cancer has a hidden onset, and the early symptoms are not obvious. When apparent symptoms appear, it is already in the middle and late stages, and most patients only want to come to the hospital for the first time when they have touched the noticeable neck lumps [
2]. It is essential to determine whether cervical lymph nodes are metastatic for nasopharyngeal cancer patients to clarify clinical staging, formulate treatment plans, and evaluate prognosis. Unlike other head and neck malignant tumors, nasopharyngeal cancer mainly adopts a comprehensive treatment plan based on radiation therapy, with local recurrence being the leading cause of treatment failure. Among them, 14–18% are cervical lymph node recurrence [
3], mainly because the missed false negative lymph nodes were classified as low-dose areas during the planning process.
Previous studies have reported that
18F-fluorodeoxyglucose positron emission tomography-computed tomography (
18F-FDG PET-CT) has shown significant functionality in detecting distant metastasis of nasopharyngeal cancer [
4,
5].
18F-FDG PET-CT scanning is the most commonly used imaging method in clinical practice, which can reflect prognostic factors directly related to clinical outcomes, including maximum standardized uptake value (SUV-Max), metabolic tumor volume, and total lesion glycolysis [
6].
18FDG PET-CT combines the anatomical accuracy of CT and the details of PET molecular metabolism and has become an imaging method for molecular targets, providing an important basis for differential diagnosis and therapeutic evaluation of tumors [
7]. However, static
18F-FDG PET-CT only displays the cumulative results after 60 min of tracer injection, ignoring the intermediate processes, including the transport of the tracer through blood flow, its exchange between blood vessels and tissues, and its binding and separation with the target [
8]. SUV is an important diagnostic indicator for static PET imaging, a standard for given drug activity and weight, and a relative measurement value [
9,
10] and is influenced by many factors related to physical effects, hardware and software system specifications, tracer kinetics, motion, scanning protocol design, and limitations of current image derived PET indicators [
11]. Meanwhile, the average SUV value changes due to voxel levels, making it sensitive to the definition of ROI (region of interest) and influenced by changes within and between observers [
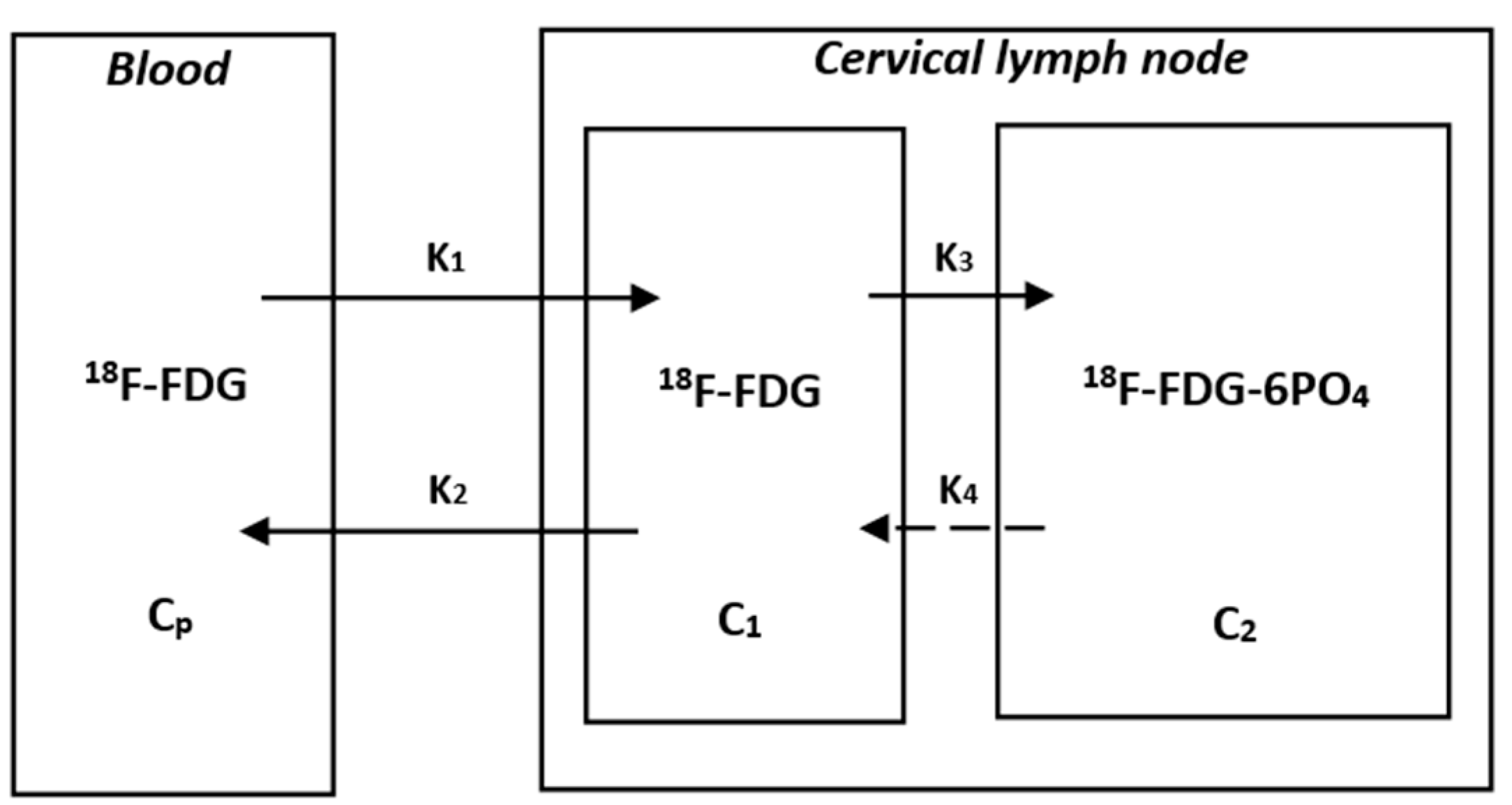
12]. Dynamic PET-CT scanning refers to starting data collection immediately after injection of a tracer, generating a time-activity-curve (TAC) based on the framing during the scanning process, and extracting parameters such as K
1-K
4, K
i, and glucose metabolism rate through dynamic modeling. It can avoid the influence of factors such as uptake kinetics, injection imaging time, and BMI, has better accuracy than SUVs, and can achieve a quantitative evaluation of tumor metabolism. In addition, dynamic studies have found that K
i can more sensitively identify early metastatic lymph nodes than SUVs [
13]. For suspected metastases that SUVs cannot accurately identify, dynamic PET-CT scans can provide more information.
Recently, multiple studies have confirmed the important role of dynamic PET-CT in determining lymph node metastasis. Sun [
14] et al. conducted a prospective cohort study on patients with non-small cell lung cancer and obtained some characteristic dynamic parameters such as V_Median, K
3_Entropy, VB_Entropy, K
1_Uniformity, and K
i_Uniformity. The results showed significant differences between benign and malignant lymph nodes, which were pathologically confirmed. The results showed significant differences in K
3_Entropy, VB_Entropy, K
1_Uniformity, and K
i_Uniformity. The K
i, VB, and K
3 regression models could make good predictions for distinguishing between benign and malignant lymph nodes. Wumner [
15] et al. analyzed 135 mediastinal and hilar lymph nodes from 29 lung cancer patients and confirmed pathologically that 49 were non-metastatic and 86 were metastatic. All patients completed dynamic PET-CT and obtained characteristic parameters. In addition to K
3, dynamic metabolic parameters K
1, K
2, K
i, and K
i/K
1 also performed well in the differential diagnosis of metastatic and non-metastatic lymph nodes (
p < 0.05). However, the predictive role of dynamic PET-CT in cervical lymph node metastasis of nasopharyngeal carcinoma has not been reported.
Therefore, the primary purpose of this study is to clarify whether the Ki value in dynamic PET-CT can replace the SUV value in distinguishing cervical lymph node metastasis of nasopharyngeal cancer, which can be used as a reference for radiation oncologists when delineating the target area, and can improve tumor control rate, reduce recurrence rate, and obtain better efficacy and prognosis in clinical treatment.
4. Discussion
In the first diagnosis, 70~80% of nasopharyngeal cancer patients have enlarged cervical lymph nodes [
30]. The location of metastatic lymph nodes is related to the lymphatic drainage area of the primary tumor. The cervical lymph node metastasis of nasopharyngeal cancer mainly occurs bilaterally, commonly around the jugular vein chain. Currently, the treatment of nasopharyngeal cancer mainly relies on radiation therapy as a comprehensive treatment. With the development of radiation therapy technology, although intensity-modulated radiation therapy (IMRT) can provide excellent dose coverage for tumors, better protect surrounding normal tissues, improve local control, and long-term survival [
31,
32], 7% to 18% of patients still have residual or recurrent cervical lymph nodes after the first round of radiation therapy [
33,
34]. Therefore, determining whether neck lymph nodes are metastatic is crucial for accurate staging, selection of treatment plans, delineation of radiotherapy targets, and evaluation of the prognosis of nasopharyngeal cancer.
PET imaging for cancer metabolic assessment has been widely used in clinical medicine. The commonly used method is to evaluate the energy consumption of tumors by injecting
18F-fluorodeoxyglucose and detecting the maximum glucose metabolism (SUV-Max) [
35]. However, many factors, such as uptake kinetics, body mass index, or post-injection time, can affect the results of SUV values [
36]. As a new imaging technology in nuclear medicine, dynamic PET-CT images collect continuous frames through long-term scanning compared with static PET-CT images. Therefore, the degree of drug metabolism and histopathological activity is dynamically reflected [
35]. The diagnostic value of dynamic PET-CT has been supported by data in non-small cell lung cancer and primary tumors of nasopharyngeal cancer [
13,
37], but there is no research report on whether it can differentiate cervical lymph node metastasis in nasopharyngeal cancer.
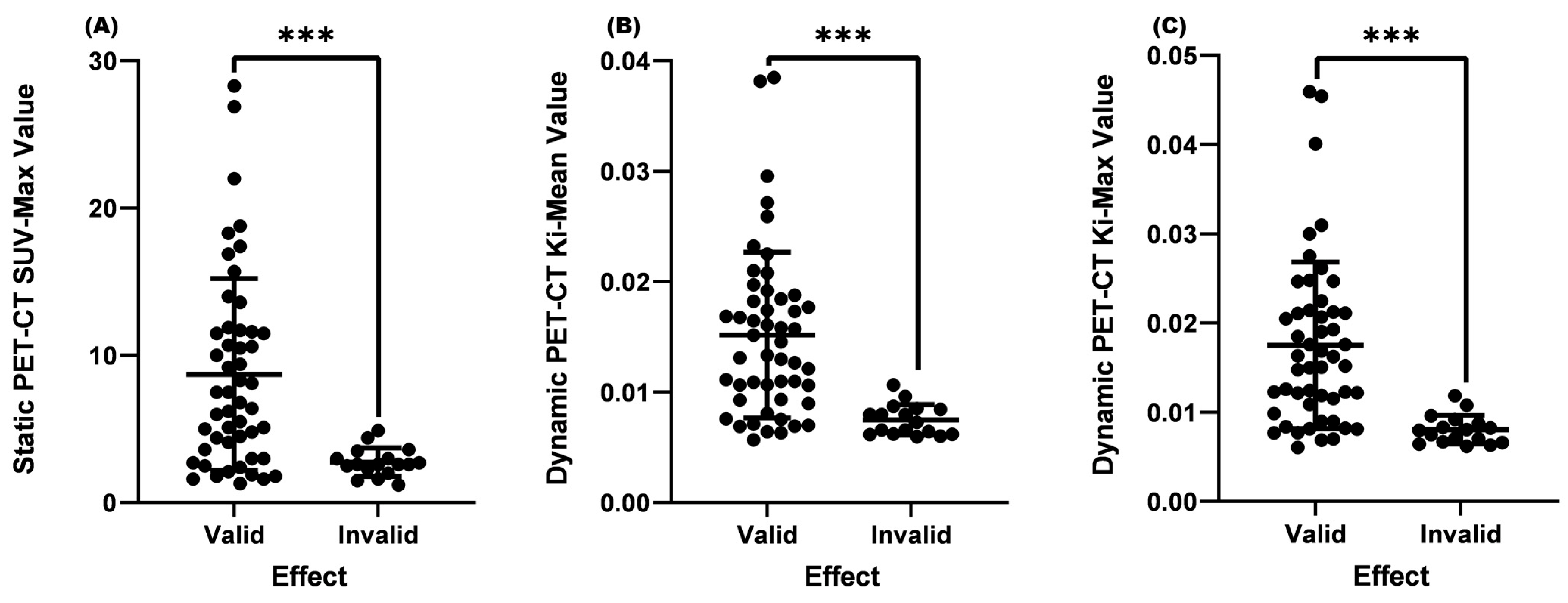
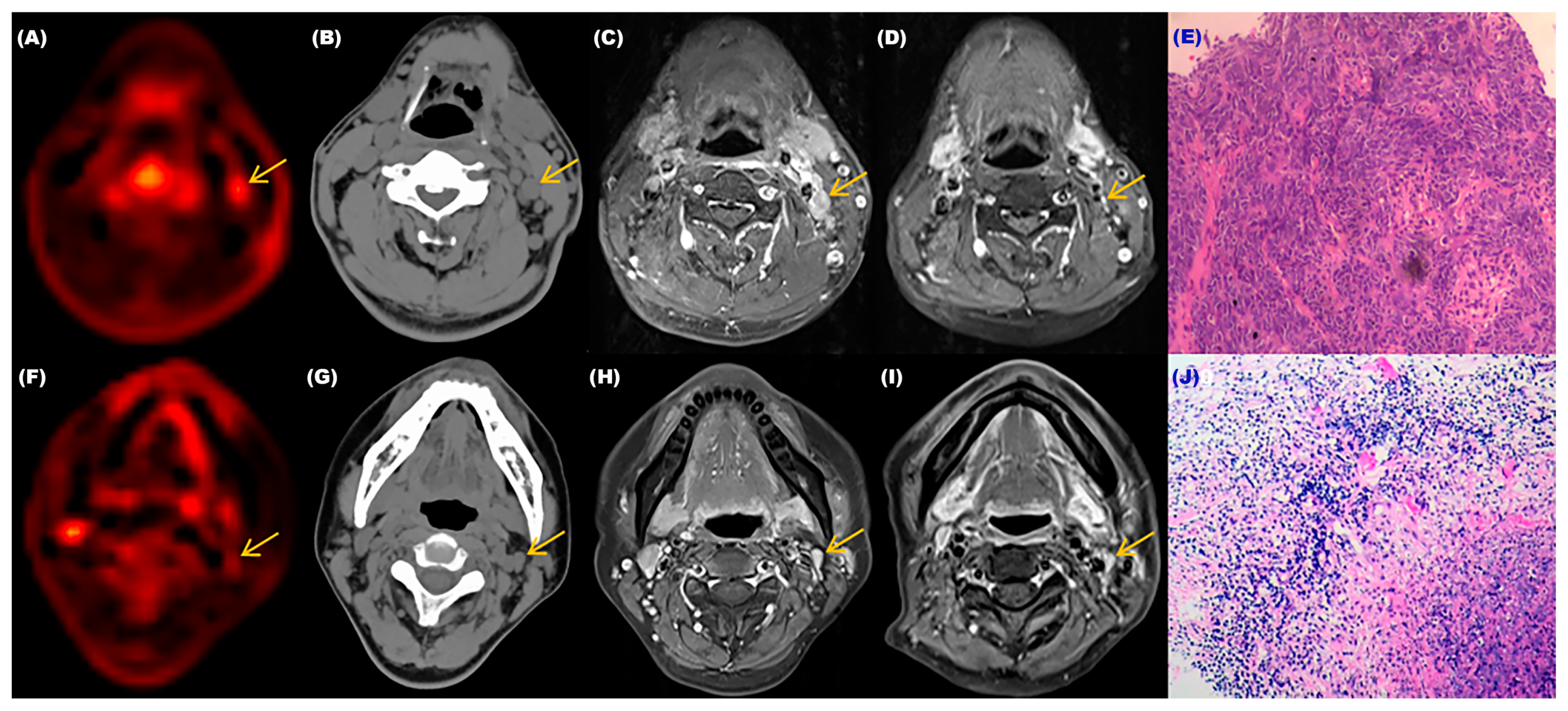
In our study, we first searched for cervical lymph nodes of interest on PET-CT images and then found the corresponding lymph nodes on magnetic resonance images. Then, according to the latest version of WHO solid tumor evaluation standards, we measured the maximum diameters and maximum vertical transverse diameters of lymph nodes before and after treatment and calculated the product size of the two. If the change before and after treatment exceeded 50%, it was included in the valid group; if it was less than 50%, it was included in the invalid group. Due to the inability to perform a needle biopsy on each cervical lymph node to determine its nature, we could only speculate on its potential for malignancy based on changes before and after treatment. It would likely be malignant if the change was greater than 50%. If the change was less than 50%, it was considered more likely to be benign. Through analysis, we found that the SUV-Max, Ki-Mean, and Ki-Max of the valid group were significantly higher than those of the invalid group (p < 0.001). This result might indicate that glucose metabolism’s degree and metabolic rate in general metastatic lymph nodes are significantly higher than in benign lymph nodes.
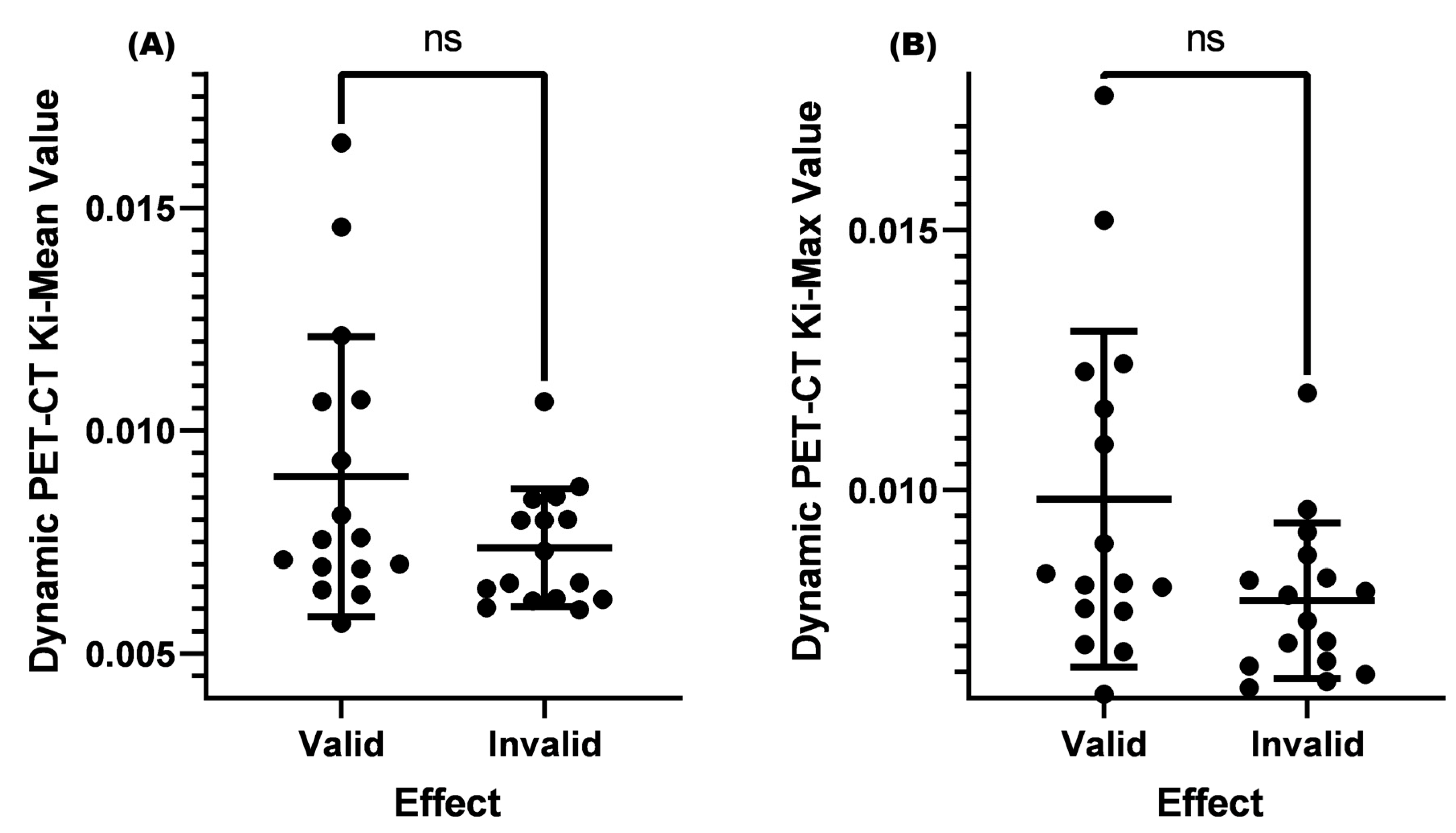
Previous studies have shown that when the SUV value of the lymph node is greater than 4.5, pathological biopsy confirms it as metastasis. However, for SUV values ≤ 4.5, it is difficult to distinguish between benign and malignant [
23,
38]. Given this result, we also set the same conditions in this study and found no significant difference in the K
i-Mean and K
i-Max between the two groups (
p > 0.05). However, it could be seen from the results that the
p-value of the K
i-Max was very close to 0.05. Due to the small sample size of this study, no positive results were obtained. Increasing the sample size further might result in better research results. According to the current results, when the SUV-Max was ≤4.5, the K
i-Mean and K
i-Max could not effectively distinguish between metastatic or benign lymph nodes.
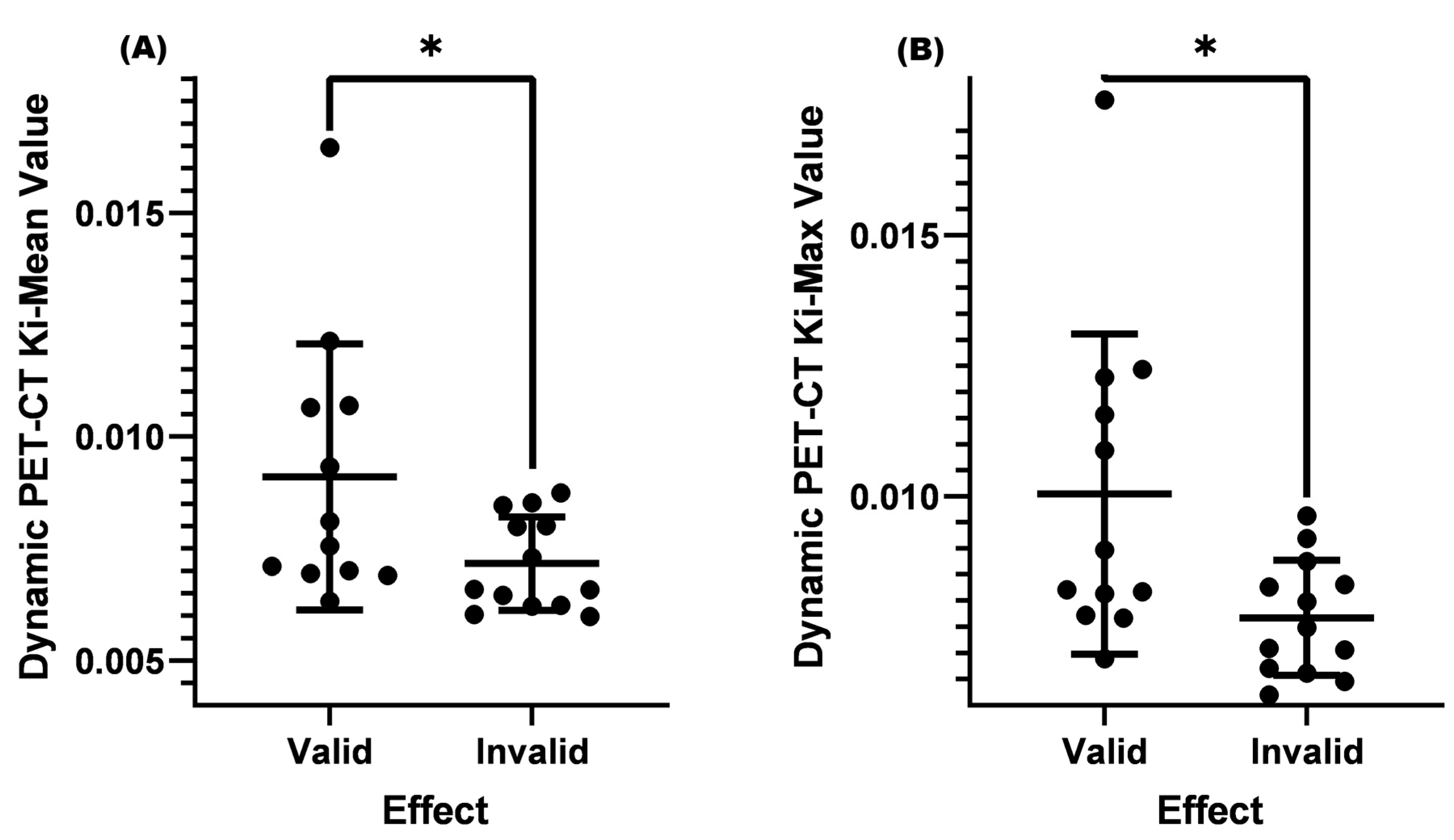
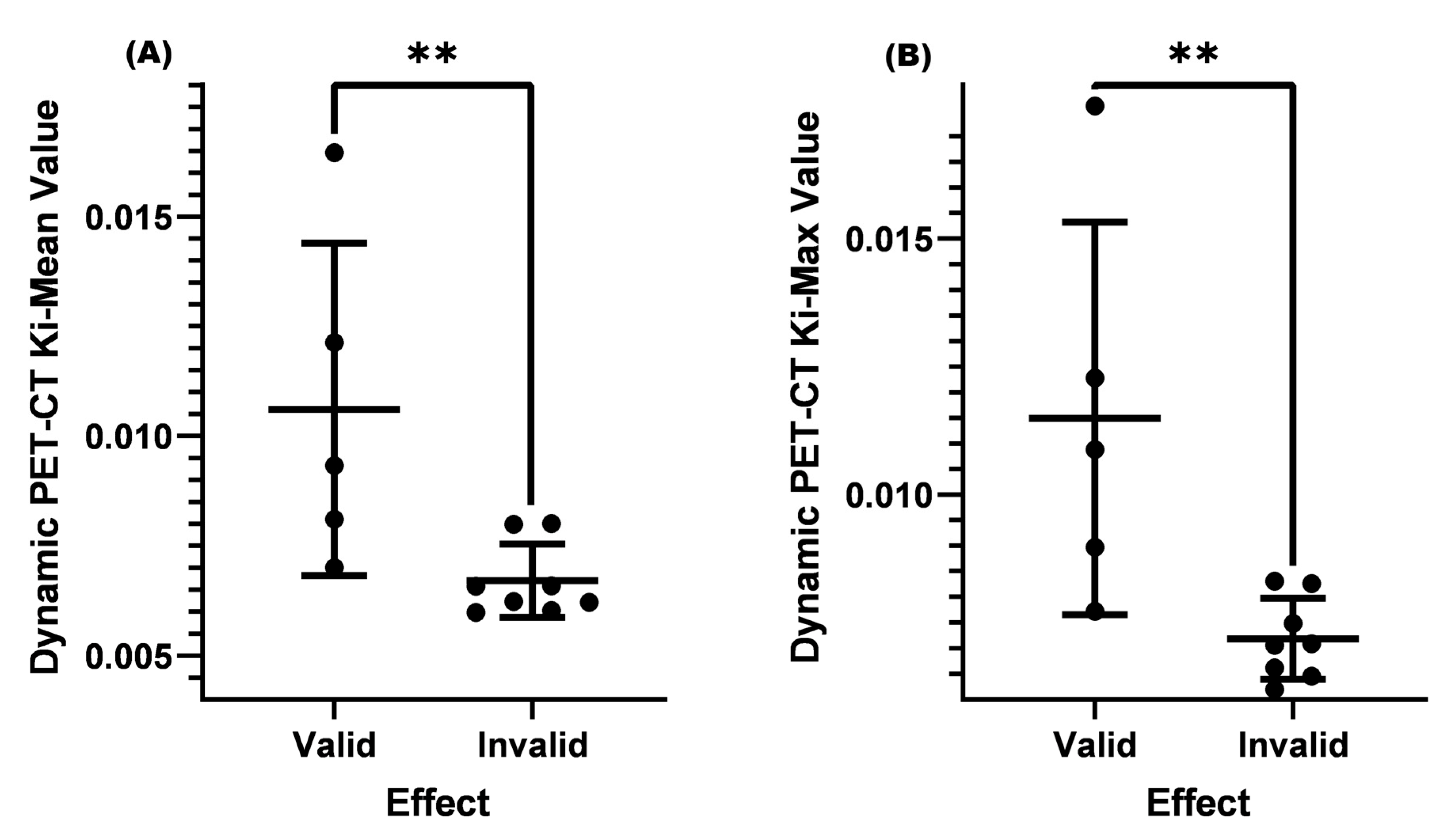
The lymph node size is often an important indicator for diagnosing metastasis. In clinical practice, a cervical lymph node size ≥ 1.0 cm is an important criterion for cervical lymph node metastasis. For lymph nodes < 1.0 cm, it is often necessary to consider specific situations, such as whether there is central necrosis, cluster distribution, obvious enhancement, and so on. In our study, it was found that when the SUV-Max was ≤4.5, and the cervical lymph node < 1.0 cm before treatment, it could be seen that the Ki-Mean and Ki-Max of the valid group were greater than those of the invalid group (p < 0.05). The average Ki-Mean and Ki-Max values of the valid group were 0.00910 and 0.01004, and both were close to 0.01. This result indicates that dynamic PET-CT can often distinguish between benign and malignant lymph nodes when the SUV-Max is small and the cervical lymph node size does not meet the standards.
Epstein–Barr (EB) is the γ herpesvirus [
39] and is closely related to the occurrence and development of nasopharyngeal cancer. In recent years, research has found that EB virus DNA (EBV-DNA) plays an important role in the efficacy monitoring and prognosis evaluation of nasopharyngeal cancer patients, especially in the clinical significance of changes in EBV-DNA concentration before and after treatment for distant metastasis and local recurrence in nasopharyngeal cancer patients [
40]. Current research shows a positive correlation between EBV-DNA content in the blood of nasopharyngeal cancer patients and the volume of cervical lymph node metastasis [
41], and EBV is closely associated with lymph node metastasis in nasopharyngeal cancer [
28]. To further explore whether dynamic PET-CT can identify cervical lymph node metastasis when the level of EBV-DNA replication was normal, we analyzed it. The results showed that when the SUV-Max was ≤4.5, the pre-treatment lymph node < 1.0 cm, and EBV-DNA replication was normal the K
i-Mean and K
i-Max in the valid group were significantly higher than those in the invalid group (
p < 0.05). Moreover, the valid group’s K
i-Mean and K
i-Max were greater than 0.01. Dynamic PET-CT can identify metastatic cervical lymph nodes when the EBV-DNA replication is normal, meanwhile, the SUV-Max is small and the lymph nodes do not meet the standards.
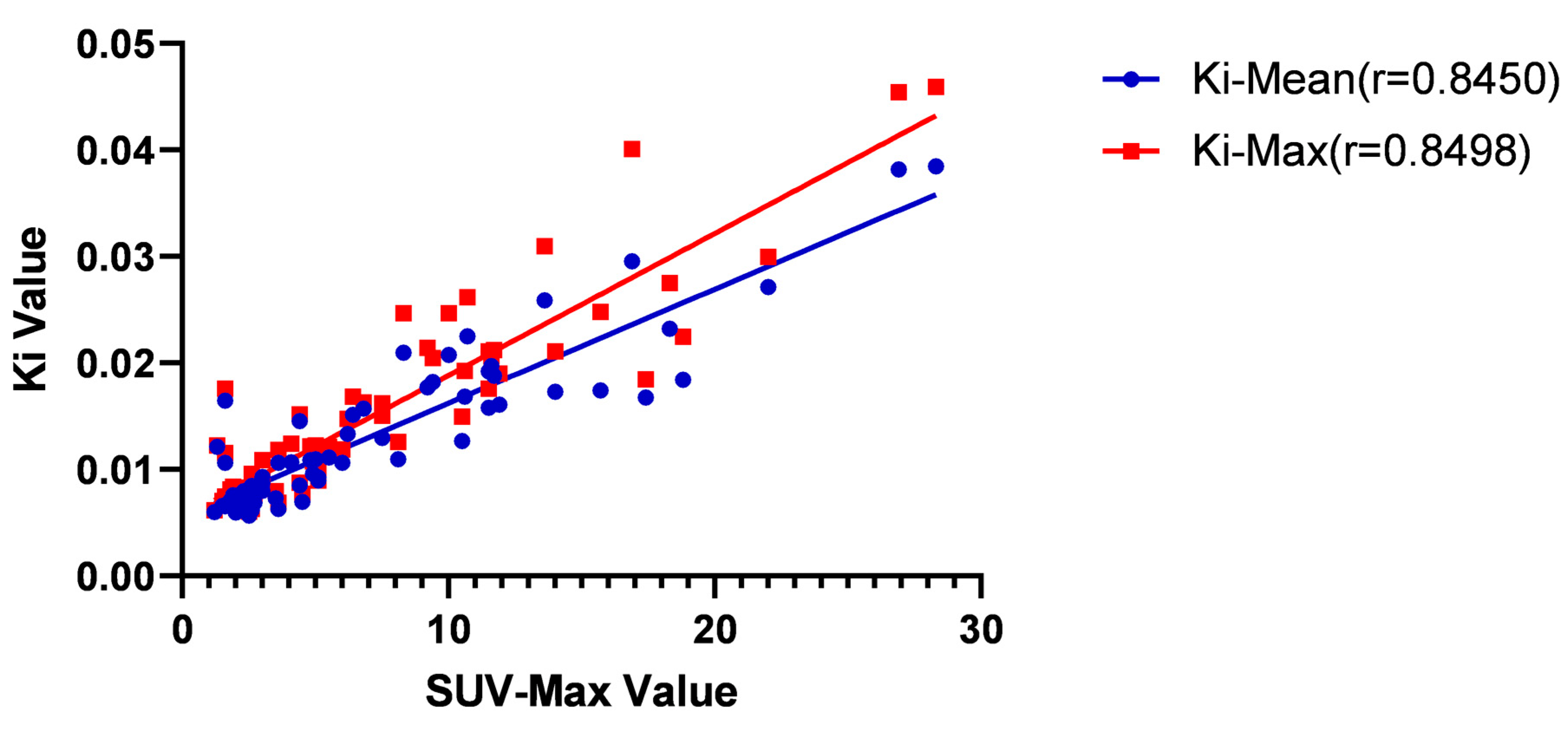
Many factors, such as age, T-stage, and SUV-Max, are related to parameters in dynamic PET-CT. Through analysis, it was found that SUV-Max and pre-treatment lymph nodes < 1.0 cm were associated with K
i-Mean and K
i-Max. A strong linear correlation existed between SUV-Max and K
i-Mean and K
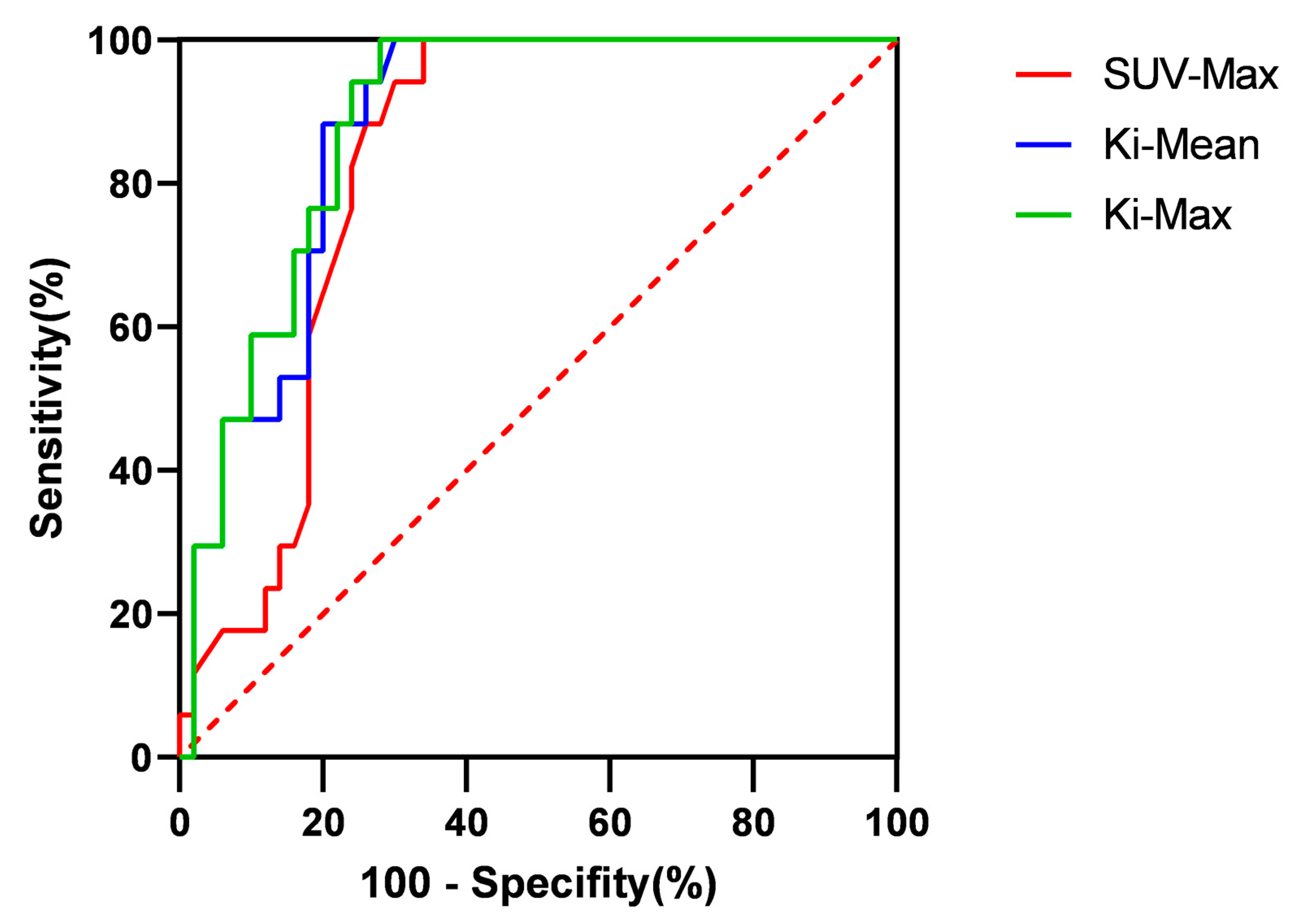
i-Max. After further diagnostic testing, it was found that the AUC value of both the K
i-Mean and K
i-Max were greater than those of the SUV-Max. Generally speaking, the larger the AUC value, the higher its diagnostic or exclusion value [
42]. However, in our study, it was found that there was no significant difference in AUC values between K
i-Mean and SUV-Max (
p = 0.220 > 0.05), and there was also no significant difference in AUC values between K
i-Max and SUV-Max (
p = 0.159 > 0.05). In terms of sensitivity, the sensitivity of SUV-Max, K
i-Mean, and K
i-Max could all reach 100%. However, regarding specificity, there was no significant difference between K
i-Mean and K
i-Max compared to SUV-Max (
p > 0.05). The above results may indicate that dynamic PET-CT has the more accurate tendency, and due to sample size limitations, no positive conclusion has been drawn. This positive conclusion may be confirmed in large sample data in the future.
Some issues need to be addressed in our research. (1) We could only speculate on the possibility of cervical lymph node metastasis based on the changes in MRI before and after treatment, without pathological results to support it. There might be misdiagnoses and errors in the conclusions. (2) Some studies yielded nearly positive results, but a positive conclusion could not be reached due to insufficient sample size and could only be treated as negative. (3) In our study, some nasopharyngeal cancer patients only received partial treatment, and the follow-up time after treatment was insufficient. Some cervical lymph nodes might not have shown significant changes and had been included in the invalid group. (4) The sample difference between the valid and invalid groups was large, and the data did not conform to the normal distribution, affecting the results’ authenticity.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}