

Percutaneous CT-Guided Bone Biopsies: Indications, Feasibility and Diagnostic Yield in the Different Skeletal Sites—From the Skull to the Toe

Abstract
:1. Introduction
1.1. Biopsy: General Concepts
1.2. History
1.3. Image Guidance
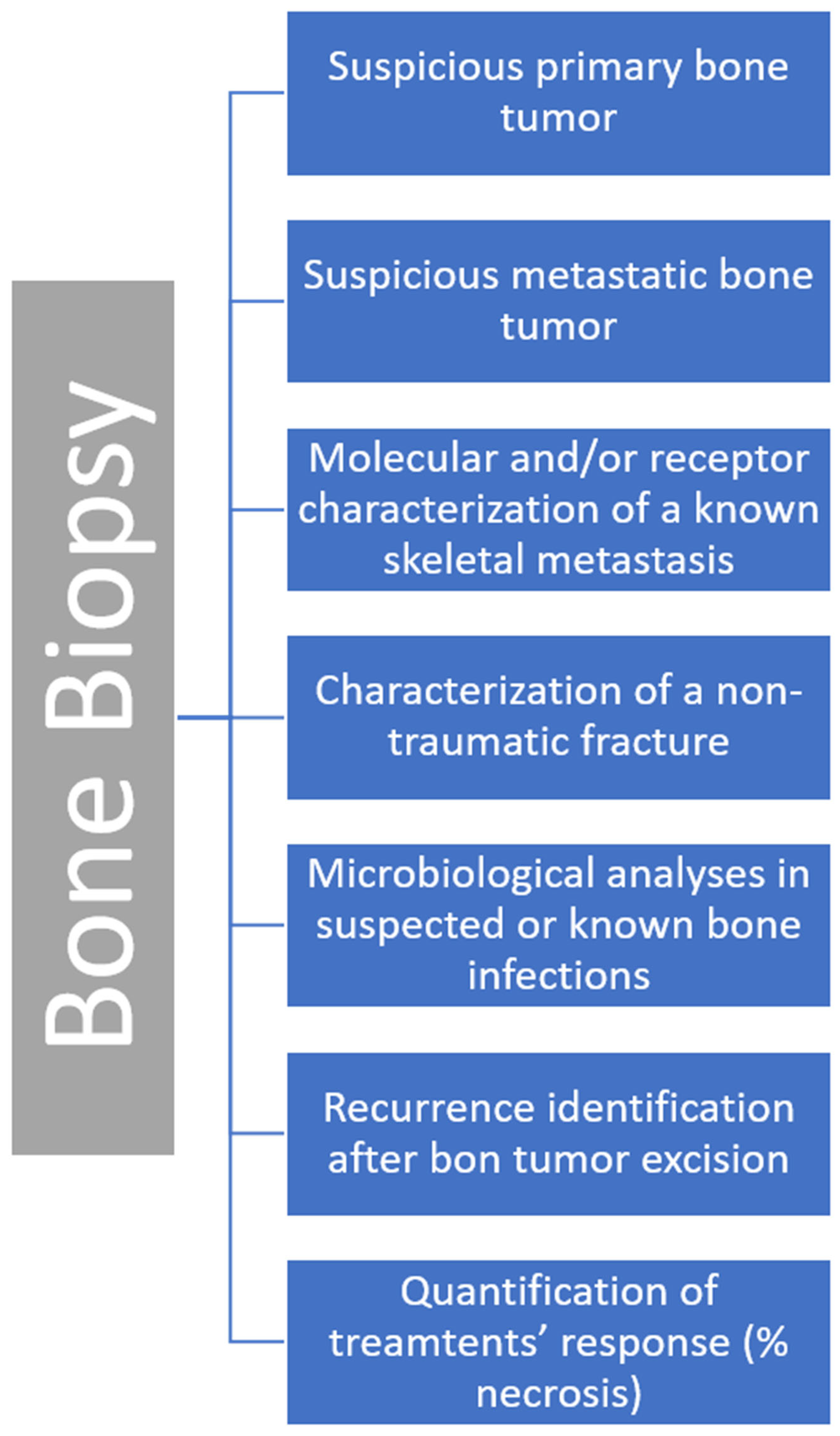
1.4. Clinical Indications
1.5. Contraindications and Complications
2. CT-Guided Skeletal Biopsy: Feasibility and Diagnostic Yield in Different Skeletal Sites
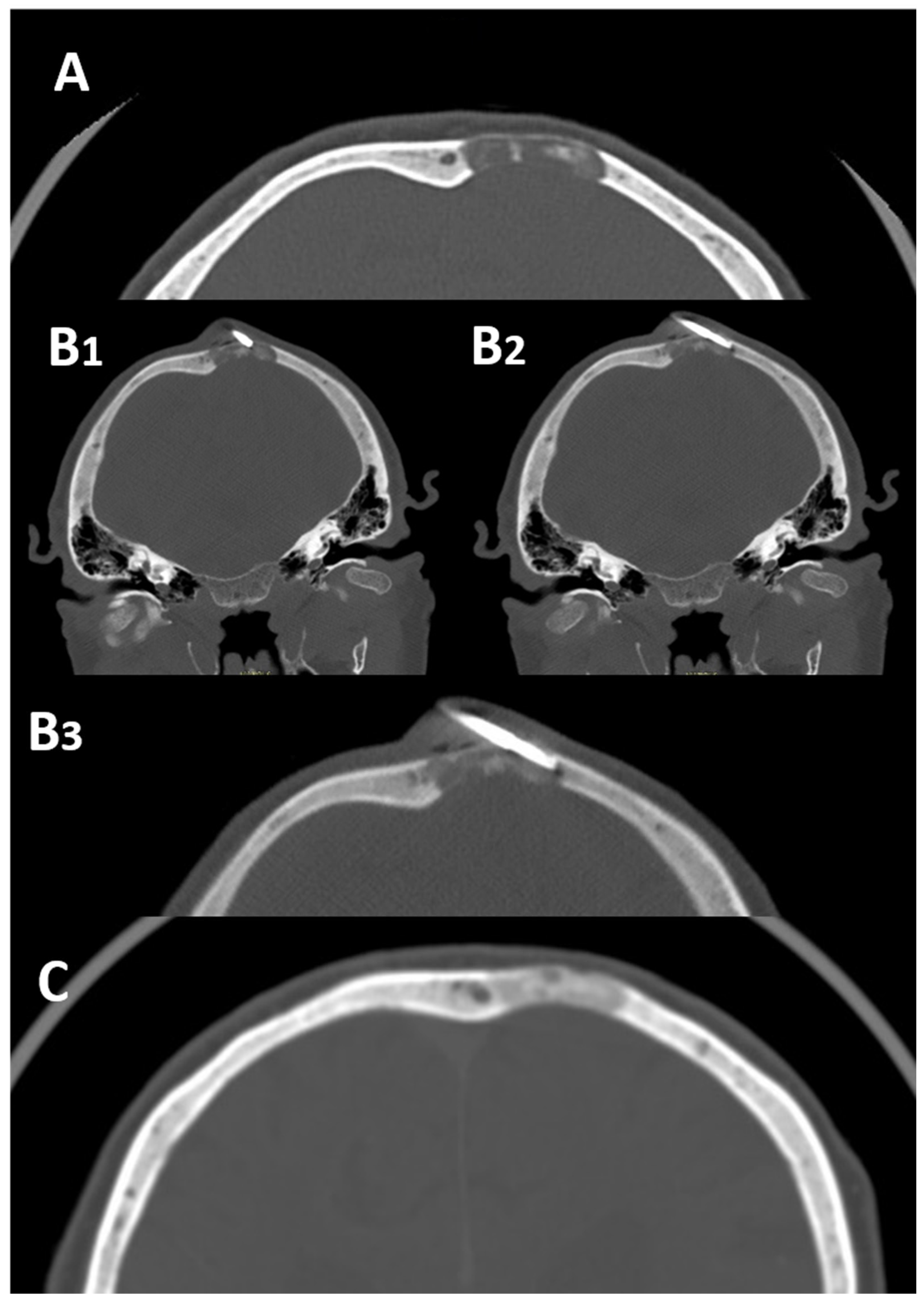
2.1. Skull
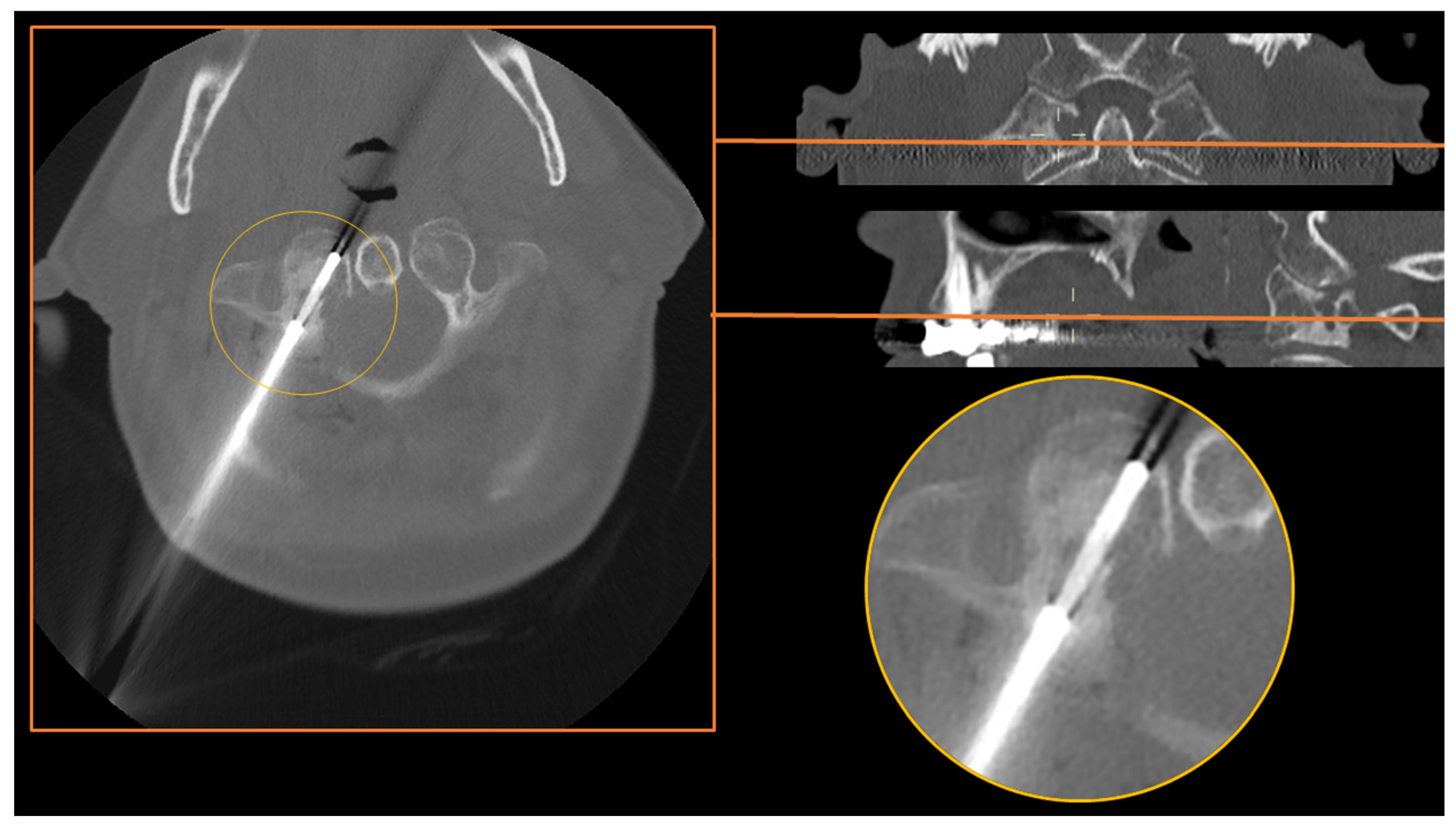
2.2. Skull Base and Craniovertebral Junction (C0–C2)
2.3. The Spine
2.4. Ribs and Sternum
2.5. The Pelvis
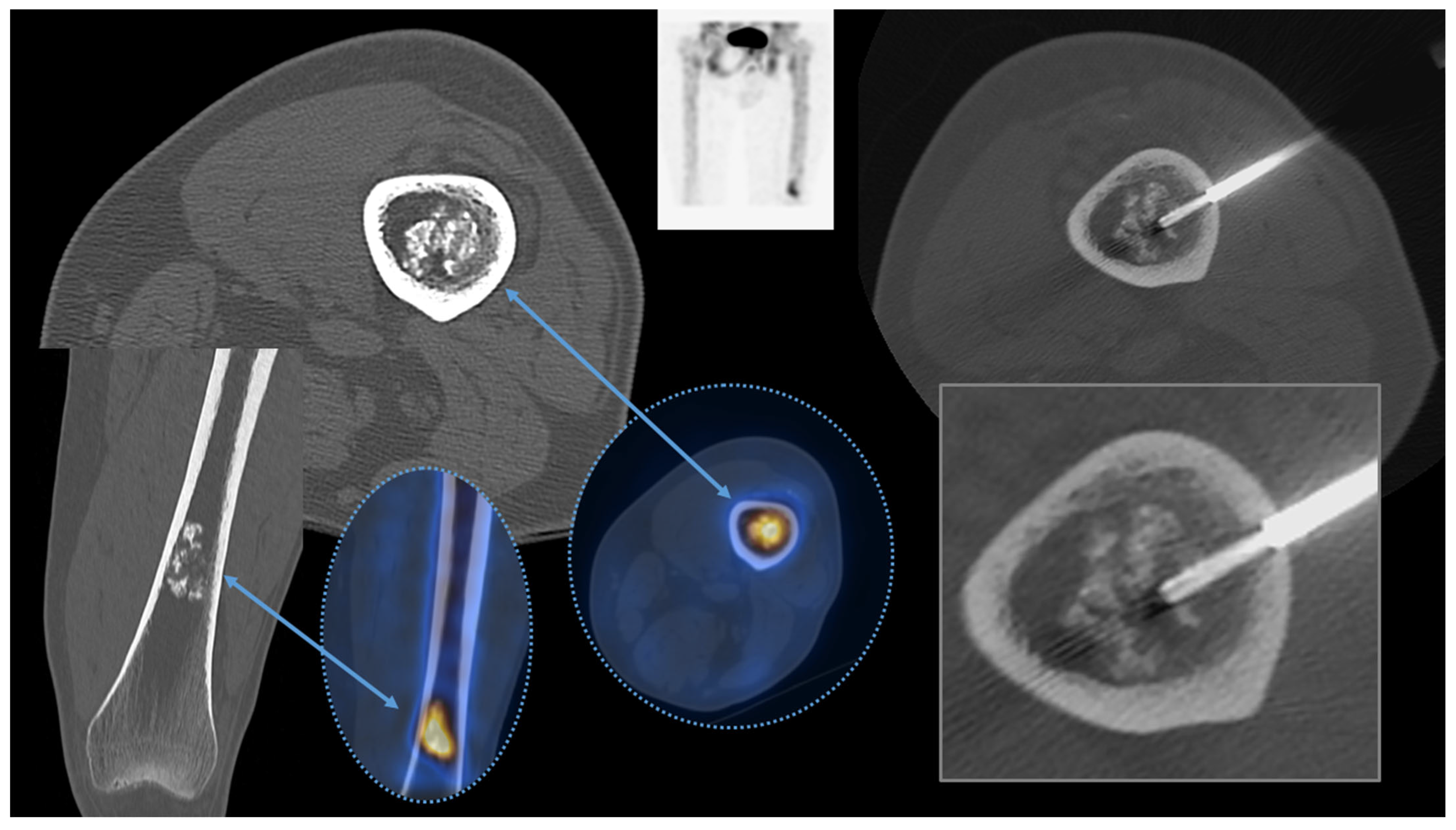
2.6. Appendicular Skeleton
Hands and Feet
3. Factors Influencing the Diagnostic Yield
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, A.J.; Kattapuram, S.V. Musculoskeletal Neoplasms: Biopsy and Intervention. Radiol. Clin. N. Am. 2011, 49, 1287–1305. [Google Scholar] [CrossRef] [PubMed]
- Traina, F.; Errani, C.; Toscano, A.; Pungetti, C.; Fabbri, D.; Mazzotti, A.; Donati, D.; Faldini, C. Current concepts in the biopsy of musculoskeletal tumors. J. Bone Joint Surg. Am. 2015, 97, e7. [Google Scholar] [CrossRef] [Green Version]
- Martin, H.E.; Ellis, E.B. Biopsy by needle puncture and aspiration. Ann. Surg. 1930, 92, 169–181. [Google Scholar] [CrossRef]
- Coley, B.L.; Sharp, G.S.; Ellis, E.B. Diagnosis of bone tumors by aspiration. Am. J. Surg. 1931, 13, 215–224. [Google Scholar] [CrossRef]
- Murphy, W.A.; Destouet, J.M.; Gilula, L.A. Percutaneous skeletal biopsy 1981: A procedure for radiologists—Results, review, and recommendations. Radiology 1981, 139, 545–549. [Google Scholar] [CrossRef] [PubMed]
- Chira, R.I.; Chira, A.; Manzat-Saplacan, R.M.; Nagy, G.; Bintintan, A.; Mircea, P.A.; Valean, S. Ultrasound-guided bone lesions biopsies—A systematic review. Med. Ultrason. 2017, 19, 302–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, J.W.; Souza, C.; Jibri, Z.; Rakhra, K.S. Ultrasound-guided percutaneous rib biopsy: A safe procedure with high diagnostic yield. Clin. Radiol. 2019, 74, 650.e1–650.e6. [Google Scholar] [CrossRef] [PubMed]
- Ponti, F.; Arioli, A.; Longo, C.; Miceli, M.; Colangeli, M.; Papalexis, N.; Spinnato, P. Ultrasound-Guided Percutaneous Bone Biopsy: Feasibility, Diagnostic Yield and Technical Notes. Diagnostics 2023, 13, 1773. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Sequeiros, R.B.; Xu, Y.; He, X.; Zhu, T.; Li, L.; Lu, Y.; Huang, J.; Li, C. MRI-guided percutaneous transpedicular biopsy of thoracic and lumbar spine using a 0.23t scanner with optical instrument tracking. J. Magn. Reson. Imaging 2015, 42, 1740–1746. [Google Scholar] [CrossRef] [PubMed]
- Kovacevic, L.; Cavka, M.; Marusic, Z.; Kresic, E.; Stajduhar, A.; Grbanovic, L.; Dumic-Cule, I.; Prutki, M. Percutaneous CT-Guided Bone Lesion Biopsy for Confirmation of Bone Metastases in Patients with Breast Cancer. Diagnostics 2022, 12, 2094. [Google Scholar] [CrossRef]
- Filippiadis, D.; Mazioti, A.; Kelekis, A. Percutaneous, Imaging-Guided Biopsy of Bone Metastases. Diagnostics 2018, 8, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spinnato, P.; Bazzocchi, A.; Facchini, G.; Filonzi, G.; Nanni, C.; Rambaldi, I.; Rimondi, E.; Fanti, S.; Albisinni, U. Vertebral Fractures of Unknown Origin: Role of Computed Tomography-Guided Biopsy. Int. J. Spine Surg. 2018, 12, 673–679. [Google Scholar] [CrossRef]
- Saifuddin, A.; Palloni, V.; du Preez, H.; Junaid, S.E. Review article: The current status of CT-guided needle biopsy of the spine. Skelet. Radiol. 2021, 50, 281–299. [Google Scholar] [CrossRef]
- Sambri, A.; Spinnato, P.; Tedeschi, S.; Zamparini, E.; Fiore, M.; Zucchini, R.; Giannini, C.; Caldari, E.; Crombé, A.; Viale, P.; et al. Bone and Joint Infections: The Role of Imaging in Tailoring Diagnosis to Improve Patients’ Care. J. Pers. Med. 2021, 11, 1317. [Google Scholar] [CrossRef]
- Spinnato, P.; Patel, D.B.; Di Carlo, M.; Bartoloni, A.; Cevolani, L.; Matcuk, G.R.; Crombé, A. Imaging of Musculoskeletal Soft-Tissue Infections in Clinical Practice: A Comprehensive Updated Review. Microorganisms 2022, 10, 2329. [Google Scholar] [CrossRef]
- Naselli, N.; Facchini, G.; Lima, G.M.; Evangelisti, G.; Ponti, F.; Miceli, M.; Spinnato, P. MRI in differential diagnosis between tuberculous and pyogenic spondylodiscitis. Eur. Spine J. 2022, 31, 431–441. [Google Scholar] [CrossRef] [PubMed]
- Nanni, P.; Landuzzi, L.; Manara, M.C.; Righi, A.; Nicoletti, G.; Cristalli, C.; Pasello, M.; Parra, A.; Carrabotta, M.; Ferracin, M.; et al. Bone sarcoma patient-derived xenografts are faithful and stable preclinical models for molecular and therapeutic investigations. Sci. Rep. 2019, 9, 12174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crombé, A.; Kind, M.; Fadli, D.; Miceli, M.; Linck, P.-A.; Bianchi, G.; Sambri, A.; Spinnato, P. Soft-tissue sarcoma in adults: Imaging appearances, pitfalls and diagnostic algorithms. Diagn. Interv. Imaging 2023, 104, 207–220. [Google Scholar] [CrossRef] [PubMed]
- Spinnato, P.; Sambri, A.; Fujiwara, T.; Ceccarelli, L.; Clinca, R.; Medellin, M.R.; Paolis, M.; Donati, D.M.; Bianchi, G. Myxofibrosarcoma: Clinical and Prognostic Value of MRI Features. Curr. Med. Imaging 2021, 17, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Patel, I.J.; Rahim, S.; Davidson, J.C.; Hanks, S.E.; Tam, A.L.; Walker, T.G.; Wilkins, L.R.; Sarode, R.; Weinberg, I. Society of Interventional Radiology Consensus Guidelines for the Periprocedural Management of Thrombotic and Bleeding Risk in Patients Undergoing Percutaneous Image-Guided Interventions—Part II: Recommendations: Endorsed by the Canadian Association for Interventional Radiology and the Cardiovascular and Interventional Radiological Society of Europe. J. Vasc. Interv. Radiol. 2019, 30, 1168–1184.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rimondi, E.; Rossi, G.; Bartalena, T.; Ciminari, R.; Alberghini, M.; Ruggieri, P.; Errani, C.; Angelini, A.; Calabrò, T.; Abati, C.N.; et al. Percutaneous CT-guided biopsy of the musculoskeletal system: Results of 2027 cases. Eur. J. Radiol. 2011, 77, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Tomasian, A.; Hillen, T.; Jennings, J. Percutaneous CT-Guided Skull Biopsy: Feasibility, Safety, and Diagnostic Yield. Am. J. Neuroradiol. 2019, 40, 309–312. [Google Scholar] [CrossRef] [Green Version]
- Sundararajan, S.H.; Cox, M.; Sedora-Roman, N.; Ranganathan, S.; Hurst, R.; Pukenas, B. Image-Guided Percutaneous Calvarial Biopsy with Low-Dose CT-Fluoroscopy: Technique, Safety, and Utility in 12 Patients. Cardiovasc. Interv. Radiol. 2022, 45, 134–136. [Google Scholar] [CrossRef]
- Pileggi, M.; Ventura, E.; Di Napoli, A.; Piantanida, R.; Muto, M.; Cardia, A.; Cianfoni, A. Gantry-needle-target alignment technique for CT-guided needle approaches to the skull base and cranio-cervical junction. Neuroradiology 2022, 64, 2039–2047. [Google Scholar] [CrossRef]
- Abrahams, J.J. Mandibular sigmoid notch: A window for CT-guided biopsies of lesions in the peripharyngeal and skull base regions. Radiology 1998, 208, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Kelley, T.F.; Stankiewicz, J.A.; Chow, J.M.; Origitano, T.C. Endoscopic Transsphenoidal Biopsy of the Sphenoid and Clival Mass. Am. J. Rhinol. 1999, 13, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Yamazawa, E.; Takahashi, S.; Shin, M.; Tanaka, S.; Takahashi, W.; Nakamoto, T.; Suzuki, Y.; Takami, H.; Saito, N. MRI-Based Radiomics Differentiates Skull Base Chordoma and Chondrosarcoma: A Preliminary Study. Cancers 2022, 14, 3264. [Google Scholar] [CrossRef] [PubMed]
- Spinnato, P.; Rimondi, E.; Facchini, G. Percutaneous CT-Guided Biopsy of the Craniovertebral Junction: Safety, Diagnostic Yield, and Technical Notes. Diagnostics 2022, 12, 168. [Google Scholar] [CrossRef] [PubMed]
- D’Ortenzio, R.; Tolhurst, S.; Harvey, M.; Ghag, R.; Heran, M.K. The CT guided transoral approach: A biopsy technique for a poorly differentiated chordoma in a 5 year old. J. Radiol. Case Rep. 2021, 15, 1–8. [Google Scholar] [CrossRef]
- Reddy, A.S.; Dinobile, D.; Orgeta, J.E.; Peri, N. Transoral approach to CT-guided C2 interventions. Pain Physician 2009, 12, 253–258. [Google Scholar] [PubMed]
- Singh, D.K.; Kumar, N.; Nayak, B.K.; Jaiswal, B.; Tomar, S.; Mittal, M.K.; Bajaj, S.K. Approach-based techniques of CT-guided percutaneous vertebral biopsy. Diagn. Interv. Radiol. 2020, 26, 143–146. [Google Scholar] [CrossRef]
- Rimondi, E.; Staals, E.L.; Errani, C.; Bianchi, G.; Casadei, R.; Alberghini, M.; Malaguti, M.C.; Rossi, G.; Durante, S.; Mercuri, M. Percutaneous CT-guided biopsy of the spine: Results of 430 biopsies. Eur. Spine J. 2008, 17, 975–981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lis, E.; Bilsky, M.H.; Pisinski, L.; Boland, P.; Healey, J.H.; O’malley, B.; Krol, G. Percutaneous CT-Guided Biopsy of Osseous Lesion of the Spine in Patients with Known or Suspected Malignancy. Am. J. Neuroradiol. 2004, 25, 1583–1588. [Google Scholar]
- Huang, A.J.; Halpern, E.F.; Rosenthal, D.I. Incidence of delayed complications following percutaneous CT-guided biopsy of bone and soft tissue lesions of the spine and extremities: A 2-year prospective study and analysis of risk factors. Skelet. Radiol. 2013, 42, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Baffour, F.I.; Moynagh, M.R.; Eiken, P.W.; Welch, B.T.; Kurup, A.N.; Atwell, T.D.; Schmit, G.D. Effectiveness and Safety of Percutaneous CT-Guided Rib Biopsy. J. Vasc. Interv. Radiol. 2019, 30, 82–86. [Google Scholar] [CrossRef]
- Song, Y.; Kwon, J.W. Percutaneous CT-guided sternal biopsy: Factors affecting the diagnostic yield. Acta Radiol. 2017, 58, 825–833. [Google Scholar] [CrossRef] [PubMed]
- Sundaram, S.; Jizzini, M.; Lamonica, D.; Attwood, K.; Gravina, M.; Hernandez-Ilizaliturri, F.; Torka, P. Utility of bone marrow aspirate and biopsy in staging of patients with T-cell lymphoma in the PET-Era—Tissue remains the issue. Leuk. Lymphoma 2020, 61, 3226–3233. [Google Scholar] [CrossRef]
- Cesari, M.; Righi, A.; Colangeli, M.; Gambarotti, M.; Spinnato, P.; Ferraro, A.; Longhi, A.; Abate, M.E.; Palmerini, E.; Paioli, A.; et al. Bone marrow biopsy in the initial staging of Ewing sarcoma: Experience from a single institution. Pediatr. Blood Cancer 2019, 66, e27653. [Google Scholar] [CrossRef]
- Chang, C.Y.; Husseini, J.S.; Moreira, A.; Simeone, F.J.; Yee, A.J.; Bredella, M.A.; Hasserjian, R. CT-guided bone marrow aspirations and biopsies: Retrospective study and comparison with blind procedures. Skelet. Radiol. 2020, 49, 1285–1294. [Google Scholar] [CrossRef]
- Li, Y.; Du, Y.; Luo, T.Y.; Yang, H.F.; Yu, J.H.; Xu, X.X.; Zheng, H.J.; Li, B. Factors influencing diagnostic yield of CT-guided percutaneous core needle biopsy for bone lesions. Clin. Radiol. 2014, 69, e43–e47. [Google Scholar] [CrossRef]
- Donners, R.; Fotiadis, N.; Figueiredo, I.; Blackledge, M.; Westaby, D.; Guo, C.; de la Maza, M.d.l.D.F.; Koh, D.-M.; Tunariu, N. Optimising CT-guided biopsies of sclerotic bone lesions in cancer patients. Eur. Radiol. 2022, 32, 6820–6829. [Google Scholar] [CrossRef]
- Yoon, G.H.; Gavilá, E.R.; Wei, J.; Burke, C.J.; Walter, W.R. Analysis of Factors Potentially Influencing Diagnostic Yield Among Computed Tomography-Guided Biopsies for Bone Lesions. J. Comput. Assist. Tomogr. 2022, 46, 762–769. [Google Scholar] [CrossRef]
- Wu, J.S.; Goldsmith, J.D.; Horwich, P.J.; Shetty, S.K.; Hochman, M.G. Bone and Soft-Tissue Lesions: What Factors Affect Diagnostic Yield of Image-guided Core-Needle Biopsy? Radiology 2008, 248, 962–970. [Google Scholar] [CrossRef]
- Husseini, J.S.; Habibollahi, S.; Nelson, S.B.; Rosenthal, D.I.; Chang, C.Y. Best Practices: CT-Guided Percutaneous Sampling of Vertebral Discitis-Osteomyelitis and Technical Factors Maximizing Biopsy Yield. Am. J. Roentgenol. 2021, 217, 1057–1068. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.S.; Gorbachova, T.; Morrison, W.B.; Haims, A.H. Imaging-Guided Bone Biopsy for Osteomyelitis: Are There Factors Associated with Positive or Negative Cultures? Am. J. Roentgenol. 2007, 188, 1529–1534. [Google Scholar] [CrossRef] [PubMed]
- McNamara, A.L.; Dickerson, E.C.; Gomez-Hassan, D.M.; Cinti, S.K.; Srinivasan, A. Yield of Image-Guided Needle Biopsy for Infectious Discitis: A Systematic Review and Meta-Analysis. Am. J. Neuroradiol. 2017, 38, 2021–2027. [Google Scholar] [CrossRef]
- Kim, W.; Sun, K.; Kung, J.W.; Wu, J.S. CT-Guided Core Needle Biopsy of Nonspinal Bone Lesions: Comparison of Occult and Visible Bone Lesions. Am. J. Roentgenol. 2023, 220, 104–114. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Frassica, F.J.; Fayad, L.; Clark, D.P.; Weber, K.L. Analysis of Nondiagnostic Results after Image-guided Needle Biopsies of Musculoskeletal Lesions. Clin. Orthop. Relat. Res. 2010, 468, 3103–3111. [Google Scholar] [CrossRef] [Green Version]
- Maciel, M.J.S.; Tyng, C.J.; Barbosa, P.N.V.P.; Bitencourt, A.G.V.; Júnior, J.P.K.M.; Zurstrassen, C.E.; Chung, W.T.; Chojniak, R. Computed tomography-guided percutaneous biopsy of bone lesions: Rate of diagnostic success and complications. Radiol. Bras. 2014, 47, 269–274. [Google Scholar] [CrossRef]
- Gross, J.S.; Yaeger, A.; Tchelepi, H.; Matcuk, G.R., Jr. Ultrasound Fusion: Applications in Musculoskeletal Imaging. Life 2023, 13, 1278. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Affected Skeletal Region | Radiologic Pattern | Imaging Guidance |
|---|---|---|
| Appendicular skeleton | Sclerotic pattern, osteolytic or mixed pattern without cortical disruption or intramedullary only involvement | CT, Fluoroscopy |
| Appendicular Skeleton | Osteolytic or mixed pattern with cortical disruption or cortical thinning | Ultrasound, CT, Fluoroscopy |
| Pelvic bones | Lesions without large extra-skeletal soft tissue involvement | CT |
| Pelvic bones | Osteolytic or mixed with large soft tissue extra-skeletal involvement | CT, Ultrasound |
| Spine | All | CT |
| Spine | Large lesions of the vertebral body | CT, Fluoroscopy |
| Spine | Large lesions with posterior extra-osseous involvement | CT, Ultrasound |
| Ribs | Osteolytic or mixed pattern with cortical disruption or cortical thinning | CT, Ultrasound |
| Ribs | Sclerotic pattern, osteolytic or mixed pattern without cortical disruption or intramedullary only involvement | CT |
| Sternum | All | CT |
| Sternum | Anterior extra-skeletal soft tissue involvement | CT, Ultrasound |
| Skull and Craniovertebral junction | All | CT |
| Factors Associated with a Lower Diagnostic Rate | Factors Associated with a Higher Diagnostic Rate |
|---|---|
| Sclerotic radiologic pattern | Lytic or mixed radiologic pattern |
| Location in the appendicular skeleton | Location in the axial skeleton |
| Small lesion size | Large lesion size |
| Single bone sample | Multiple bone samples |
| Short sample (short needle penetration in the tumor/perpendicular needle trajectory) | Large sample (long needle penetration in the tumor/oblique needle trajectory) |
| (Spondylodiscitis/Osteomyelitis) Targeting the bone only | (Spondylodiscitis/Osteomyelitis) Targeting soft tissue involvement and/or fluid collection aspiration. |
| Target lesion not visible in CT | Target lesion visible in CT |
| Benign final diagnosis | Malignant final diagnosis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spinnato, P.; Colangeli, M.; Rinaldi, R.; Ponti, F. Percutaneous CT-Guided Bone Biopsies: Indications, Feasibility and Diagnostic Yield in the Different Skeletal Sites—From the Skull to the Toe. Diagnostics 2023, 13, 2350. https://doi.org/10.3390/diagnostics13142350
Spinnato P, Colangeli M, Rinaldi R, Ponti F. Percutaneous CT-Guided Bone Biopsies: Indications, Feasibility and Diagnostic Yield in the Different Skeletal Sites—From the Skull to the Toe. Diagnostics. 2023; 13(14):2350. https://doi.org/10.3390/diagnostics13142350
Chicago/Turabian StyleSpinnato, Paolo, Marco Colangeli, Raffaella Rinaldi, and Federico Ponti. 2023. "Percutaneous CT-Guided Bone Biopsies: Indications, Feasibility and Diagnostic Yield in the Different Skeletal Sites—From the Skull to the Toe" Diagnostics 13, no. 14: 2350. https://doi.org/10.3390/diagnostics13142350