
SARS-CoV-2 Testing of Emergency Department Patients Using cobas® Liat® and eazyplex® Rapid Molecular Assays

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
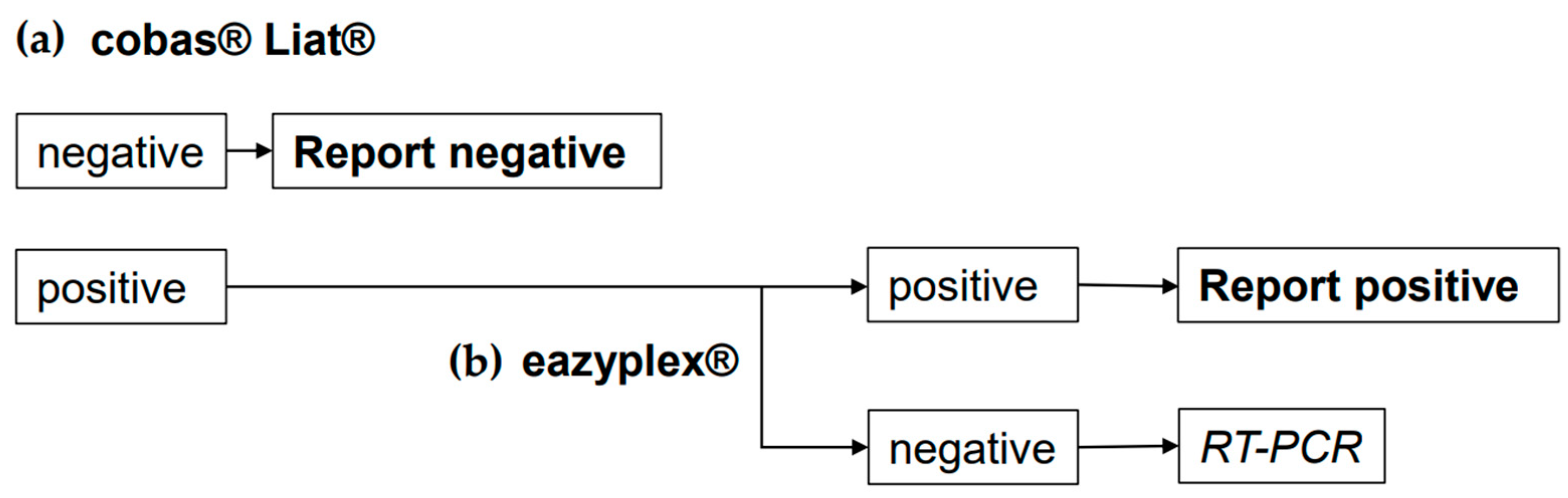
2.1. Clinical Specimens and Diagnostic Workflow
2.2. SARS-CoV-2 Assays
2.3. Data Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kepka, S.; Ohana, M.; Séverac, F.; Muller, J.; Bayle, E.; Ruch, Y.; Laugel, E.; Oberlin, M.; Soli, M.; Hansmann, Y.; et al. Rapid antigen test combined with chest computed tomography to rule out COVID-19 in patients admitted to the emergency department. J. Clin. Med. 2021, 10, 3455. [Google Scholar] [CrossRef]
- Möckel, M.; Corman, V.M.; Stegemann, M.S.; Hofmann, J.; Stein, A.; Jones, T.C.; Gastmeier, P.; Seybold, J.; Offermann, R.; Bachmann, U.; et al. SARS-CoV-2 antigen rapid immunoassay for diagnosis of COVID-19 in the emergency department. Biomarkers 2021, 26, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Bruno, A.; de Mora, D.; Freire-Paspuel, B.; Rodriguez, A.S.; Paredes-Espinosa, M.B.; Olmedo, M.; Sanchez, M.; Romero, J.; Paez, M.; Gonzalez, M.; et al. Analytical and clinical evaluation of a heat shock SARS-CoV-2 detection method without RNA extraction for N and E genes RT-qPCR. Int. J. Infect. Dis. 2021, 109, 315–320. [Google Scholar] [CrossRef]
- Hansen, G.; Marino, J.; Wang, Z.X.; Beavis, K.G.; Rodrigo, J.; Labog, K.; Westblade, L.F.; Jin, R.; Love, N.; Ding, K.; et al. Clinical performance of the point-of-care cobas Liat for detection of SARS-CoV-2 in 20 minutes: A multicenter study. J. Clin. Microbiol. 2021, 59, e02811-20. [Google Scholar] [CrossRef]
- NguyenVan, J.C.; Gerlier, C.; Pilmis, B.; Mizrahi, A.; Péan de Ponfilly, G.; Khaterchi, A.; Enouf, V.; Ganansia, O.; Le Monnier, A. Prospective evaluation of ID NOW COVID-19 assay used as point-of-care test in an emergency department. J. Clin. Virol. 2021, 145, 105021. [Google Scholar] [CrossRef] [PubMed]
- Egerer, R.; Edel, B.; Löffler, B.; Henke, A.; Rödel, J. Performance of the RT-LAMP-based eazyplex® SARS-CoV-2 as a novel rapid diagnostic test. J. Clin. Virol. 2021, 138, 104817. [Google Scholar] [CrossRef] [PubMed]
- Pu, R.; Liu, S.; Ren, X.; Shi, D.; Ba, Y.; Huo, Y.; Zhang, W.; Ma, L.; Liu, Y.; Yang, Y.; et al. The screening value of RT-LAMP and RT-PCR in the diagnosis of COVID-19: Systematic review and meta-analysis. J. Virol. Methods 2022, 300, 114392. [Google Scholar] [CrossRef]
- Schellenberg, J.J.; Ormond, M.; Keynan, Y. Extraction-free RT-LAMP to detect SARS-CoV-2 is less sensitive but highly specific compared to standard RT-PCR in 101 samples. J. Clin. Virol. 2021, 136, 104764. [Google Scholar] [CrossRef]
- Subsoontorn, P.; Lohitnavy, M.; Kongkaew, C. The diagnostic accuracy of isothermal nucleic acid point-of-care tests for human coronaviruses: A systematic review and meta-analysis. Sci. Rep. 2020, 10, 22349. [Google Scholar] [CrossRef]
- Berengua, C.; López, M.; Esteban, M.; Marín, P.; Ramos, P.; del Cuerpo, M.; Gich, I.; Navarro, F.; Miró, E.; Rabella, N. Viral culture and immunofluorescence for the detection of SARS-CoV-2 infectivity in RT-PCR positive respiratory samples. J. Clin. Virol. 2022, 152, 105167. [Google Scholar] [CrossRef]
- García-Fernández, S.; Pablo-Marcos, D.; de la Fuente, S.V.; Rodríguez, M.J.R.; Gozalo, M.; Rodríguez-Lozano, J.; Méndez-Legaza, J.M.; Calvo, J. Evaluation of the rapid antigen detection test STANDARD F COVID-19 Ag FIA for diagnosing SARS-CoV-2: Experience from an emergency department. Diagn. Microbiol. Infect. Dis. 2022, 103, 115683. [Google Scholar] [CrossRef]
- Hong, T.C.; Mai, Q.L.; Cuong, D.V.; Parida, M.; Minekawa, H.; Notomi, T.; Hasebe, F.; Morita, K. Development and evaluation of a novel loop-mediated isothermal amplification method for rapid detection of severe acute respiratory syndrome coronavirus. J. Clin. Microbiol. 2004, 42, 1956–1961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babic, N.; Garner, K.S.; Hirschhorn, J.W.; Zebian, R.; Nolte, F.S. Evaluation of Abbott ID NOW COVID-19 POC test performance characteristics and integration in the regional health network workflows to improve health care delivery. Clin. Biochem. 2021, 117, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Tanimoto, Y.; Mori, A.; Miyamoto, S.; Ito, E.; Arikawa, K.; Iwamoto, T. Comparison of RT-PCR, RT-LAMP, and antigen quantification assays for the detection of SARS-CoV-2. Jpn. J. Infect. Dis. 2022, 75, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.H.; Bui, N.N.; Chang, Y.C.; Hsu, L.Y.; Su, Y.D.; Chang, C.M.; Hong, W.A.; Le, U.N.P.; Huang, S.H.; Lin, C.W. Comparison between the analytical sensitivity and clinical performance of two cobas SARS-CoV-2 tests based on high-throughput and point-of-care systems. Biomedicine (Taipei) 2022, 12, 40–46. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration (FDA). Potential for False Results with Roche Molecular Systems, Inc. Cobas SARS-CoV-2 & Influenza Test for Use on Cobas Liat System-Letter to Clinical Laboratory Staff, Point-of-Care Facility Staff, and Health Care Providers. Available online: https://www.fda.gov/medical-devices/letters-health-care-providers/potential-false-results-roche-molecular-systems-inc-cobas-sars-cov-2-influenza-test-use-cobas-liat (accessed on 3 December 2021).
- Blackall, D.; Moreno, R.; Jin, J.; Plotinsky, R.; Dworkin, R.; Oethinger, M. Performance characteristics of the Roche Diagnostics cobas Liat PCR system as a COVID-19 screening tool for hospital admissions in a regional health care delivery system. J. Clin. Microbiol. 2021, 59, e0127821. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO COVID-19: Case Definitions. Available online: www.who.int/publications/i/item/WHO-2019-nCov-Surveillance_Case_Definition-2022.1 (accessed on 22 July 2022).
- Berg, M.G.; Zhen, W.; Lucic, D.; Degli-Angeli, E.J.; Anderson, M.; Forberg, K.; Olivo, A.; Sheikh, F.; Toolsie, D.; Greninger, A.L.; et al. Development of the RealTime SARS-CoV-2 quantitative laboratory developed test and correlation with viral culture as a measure of infectivity. J. Clin. Virol. 2021, 143, 104945. [Google Scholar] [CrossRef]
- Jajou, R.; Mutsaers-van Oudheusden, A.; Verweij, J.J.; Rietveld, J.J.; Mukrk, J.L. SARS-CoV-2 transmitters have more than three times higher viral loads than non-transmitters—Practical use of viral load for disease control. J. Clin. Virol. 2022, 150–151, 105131. [Google Scholar] [CrossRef]
- Mahmoud, S.A.; Ganesan, S.; Ibrahim, E.; Thakre, B.; Teddy, J.G.; Raheja, P.; Zaher, W.A. Evaluation of six different rapid methods for nucleic acid detection of SARS-COV-2 virus. J. Med. Virol. 2021, 93, 5538–5543. [Google Scholar] [CrossRef]
- Allsopp, R.C.; Cowley, C.M.; Barber, R.C.; Jones, C.; Holmes, C.W.; Bird, P.W.; Gohil, S.G.; Blackmore, C.; Tobin, M.D.; Brunskill, N.; et al. A rapid RT-LAMP SARS-CoV-2 screening assay for collapsing asymptomatic COVID-19 transmission. PLoS ONE 2022, 17, e0273912. [Google Scholar] [CrossRef]
- Pickering, S.; Batra, R.; Merrick, B.; Snell, L.B.; Nebbia, G.; Douthwaite, S.; Reid, F.; Patel, A.; Kia Ik, M.T.; Patel, B.; et al. Comparative performance of SARS-CoV-2 lateral flow antigen tests and association with detection of infectious virus in clinical specimens: A single-centre laboratory evaluation study. Lancet Microbe 2021, 2, e461–e471. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.C.; Malott, R.J.; Ward, L.; Kiplagat, L.; Pabbaraju, K.; Gill, K.; Berenger, B.M.; Hu, J.; Fonseca, K.; Noyce, R.S.; et al. Detection and quantification of infectious severe acute respiratory coronavirus-2 in diverse clinical and environmental samples. Sci. Rep. 2022, 12, 5418. [Google Scholar] [CrossRef] [PubMed]
- Scheiblauer, H.; Filomena, A.; Nitsche, A.; Puyskens, A.; Corman, V.M.; Drosten, C.; Zwirglmaier, K.; Lange, C.; Emmerich, P.; Müller, M.; et al. Comparative sensitivity evaluation for 122 CE-marked rapid diagnostic tests for SARS-CoV-2 antigen, Germany, September 2020 to April 2021. Euro Surveill. 2021, 26, 2100441. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patient Group | cobas® Liat®-Positive Samples (n) | Confirmatory Test | False-Positive Rate of cobas® Liat® (%) | |
|---|---|---|---|---|
| Positive | Negative | |||
| Asymptomatic | 157 | 115 a | 42 | 26.8 |
| Symptomatic | 221 | 213 a | 8 | 3.8 |
| Patient Group | RT-PCR Positive | eazyplex® RT-LAMP | PPA, % (CI a) | |
|---|---|---|---|---|
| Positive | Negative | |||
| Asymptomatic | 113 | 70 | 43 | 62 (52.3–70.9) |
| Symptomatic | 212 | 192 | 20 | 90.6 (85.8–94.1) |
| Patient Group | Ct | Sample Number (% of All Positive Samples) | eazyplex® RT-LAMP- Positive Results (%) |
|---|---|---|---|
| Asymptomatic | ≤25 | 42 (37.1) | 40 (95.2) |
| 25 < Ct < 30 | 28 (24.8) | 24 (85.7) | |
| ≥30 | 43 (38.1) | 5 (11.7) | |
| Symptomatic | ≤25 | 150 (70.8) | 150 (100) |
| 25 < Ct < 30 | 51 (24) | 42 (82.4) | |
| ≥30 | 11 (5.2) | 1 (9) |
| EQA Sample Number | Copies/mL b | cobas® Liat® | eazyplex® | NeuMoDx™ | cobas® | |||
|---|---|---|---|---|---|---|---|---|
| Qualitative Result | Threshold Time, Min | Ct Value | Ct Value | |||||
| N Gene | ORF8 Gene | N Gene | Nsp2 Gene | ORF1ab Gene | E Gene | |||
| 340,094 c | 1.14 × 105 | positive | 15.5 | 22.25 | 27.8 | 28.5 | 28.6 | 28.9 |
| 340,099 d | 1.11 × 105 | positive | 13.5 | - | 27.2 | 27.8 | 28.5 | 29 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Egerer, R.; Edel, B.; Hornung, F.; Deinhardt-Emmer, S.; Baier, M.; Lewejohann, J.-C.; Pfister, W.; Löffler, B.; Rödel, J. SARS-CoV-2 Testing of Emergency Department Patients Using cobas® Liat® and eazyplex® Rapid Molecular Assays. Diagnostics 2023, 13, 2245. https://doi.org/10.3390/diagnostics13132245
Egerer R, Edel B, Hornung F, Deinhardt-Emmer S, Baier M, Lewejohann J-C, Pfister W, Löffler B, Rödel J. SARS-CoV-2 Testing of Emergency Department Patients Using cobas® Liat® and eazyplex® Rapid Molecular Assays. Diagnostics. 2023; 13(13):2245. https://doi.org/10.3390/diagnostics13132245
Chicago/Turabian StyleEgerer, Renate, Birgit Edel, Franziska Hornung, Stefanie Deinhardt-Emmer, Michael Baier, Jan-Christoph Lewejohann, Wolfgang Pfister, Bettina Löffler, and Jürgen Rödel. 2023. "SARS-CoV-2 Testing of Emergency Department Patients Using cobas® Liat® and eazyplex® Rapid Molecular Assays" Diagnostics 13, no. 13: 2245. https://doi.org/10.3390/diagnostics13132245