
Positive Point-of-Care Influenza Test Significantly Decreases the Probability of Antibiotic Treatment during Respiratory Tract Infections in Primary Care

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Assessments
2.3. Treatment Approach
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Analysis of the Factors in the Group Treated with Antibiotics and Symptomatic Therapy
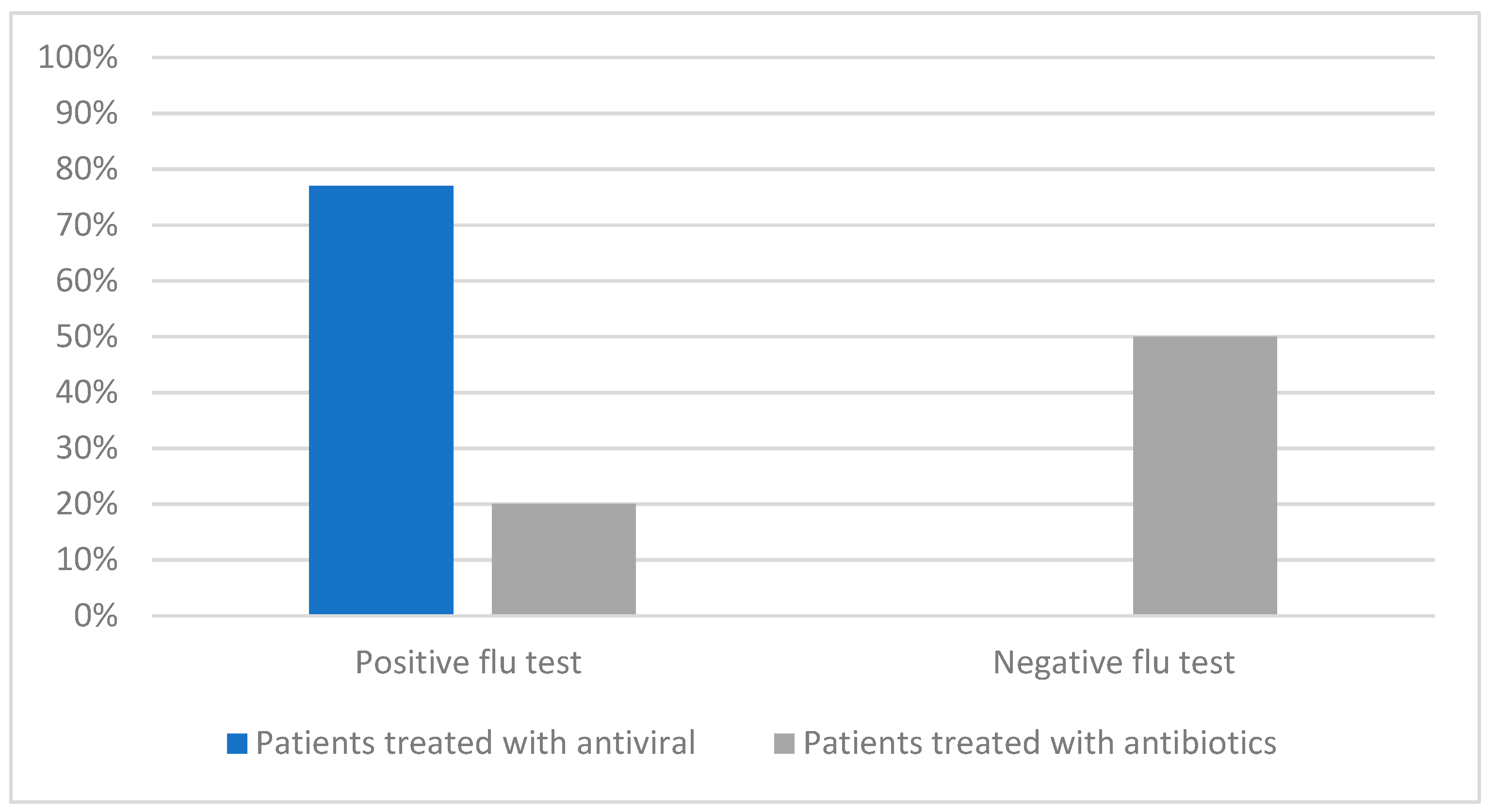
3.3. Point-of-Care Influenza Testing
3.4. Comorbidities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Finley, C.R.; Chan, D.S.; Garrison, S.; Korownyk, C.; Kolber, M.R.; Campbell, S.; Eurich, D.T.; Lindblad, A.J.; Vandermeer, B.; Allan, G.M. What are the most common conditions in primary care? Can. Fam. Physician 2018, 64, 832–840. [Google Scholar]
- Grief, S.N. Upper Respiratory Infections. Prim. Care 2013, 40, 757–770. [Google Scholar] [CrossRef]
- Cots, J.M.; Moragas, A.; García-Sangenís, A.; Morros, R.; Gomez-Lumbreras, A.; Ouchi, D.; Monfà, R.; Pera, H.; Pujol, J.; Bayona, C.; et al. Effectiveness of antitussives, anticholinergics or honey versus usual care in adults with uncomplicated acute bronchitis: A study protocol of an open randomised clinical trial in primary care. BMJ Open 2019, 9, e028159. [Google Scholar] [CrossRef] [Green Version]
- Thornton, H.V.; Turner, K.M.E.; Harrison, S.; Hammond, A.; Hawcroft, C.; Hay, A.D. Assessing the potential of upper respiratory tract point-of-care testing: A systematic review of the prognostic significance of upper respiratory tract microbes. Clin. Microbiol. Infect. 2019, 25, 1339–1346. [Google Scholar] [CrossRef]
- Cohen, J.F.; Bertille, N.; Cohen, R.; Chalumeau, M. Rapid antigen detection test for group A streptococcus in children with pharyngitis. Cochrane Database Syst. Rev. 2016, 7, CD010502. [Google Scholar] [CrossRef]
- Van Hecke, O.; Raymond, M.; Lee, J.J.; Turner, P.; Goyder, C.R.; Verbakel, J.Y.; Bruel, A.V.D.; Hayward, G. In-vitro diagnostic point-of-care tests in paediatric ambulatory care: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0235605. [Google Scholar] [CrossRef]
- Gaitonde, D.Y.; Moore, F.C.; Morgan, M.K. Influenza: Diagnosis and Treatment. Am. Fam. Physician 2019, 100, 751–758. [Google Scholar]
- Brody, H. Influenza. Nature 2019, 573, S49. [Google Scholar] [CrossRef] [Green Version]
- Rzepka, A.; Mania, A. The clinical picture of influenza against other respiratory tract infections in a general practitioner practice. Prz. Epidemiol. 2021, 75, 159–175. [Google Scholar] [CrossRef]
- Iuliano, A.D.; Roguski, K.M.; Chang, H.H.; Muscatello, D.J.; Palekar, R.; Tempia, S.; Cohen, C.; Gran, J.M.; Schanzer, D.; Cowling, B.J.; et al. Global Seasonal Influenza-associated Mortality Collaborator Network. Estimates of global seasonal influenza-associated respiratory mortality: A modelling study. Lancet 2018, 391, 1285–1300. [Google Scholar] [CrossRef]
- Chua, K.P.; Fischer, M.A.; Linder, J.A. Appropriateness of outpatient antibiotic prescribing among privately insured US patients: ICD-10-CM based cross sectional study. BMJ 2019, 16, k5092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Velden, A.W.; van de Pol, A.C.; Bongard, E.; Cianci, D.; Aabenhus, R.; Balan, A.; Böhmer, F.; Lang, V.B.; Bruno, P.; Chlabicz, S.; et al. Point-of-care testing, antibiotic prescribing, and prescribing confidence for respiratory tract infections in primary care: A prospective audit in 18 European countries. BJGP Open 2021, 6, BJGPO.2021.0212. [Google Scholar] [CrossRef] [PubMed]
- Petursson, P. GPs’ reasons for “non-pharmacological” prescribing of antibiotics A phenomenological study. Scand. J. Prim. Health Care 2005, 23, 120–125. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, R.; O’Doherty, J.; O’Regan, A.; Dunne, C. Antibiotic use for acute respiratory tract infections (ARTI) in primary care; what factors affect prescribing and why is it important? A narrative review. Ir. J. Med. Sci. 2018, 187, 969–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costelloe, C.; Metcalfe, C.; Lovering, A.; Mant, D.; Hay, A.D. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: Systematic review and meta-analysis. BMJ 2010, 340, c2096. [Google Scholar] [CrossRef] [Green Version]
- Antibiotic Expenditures by Medication, Class, and Healthcare Setting in the United States, 2010–2015 [Internet]. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9454312/ (accessed on 20 April 2023).
- McNulty, C.A.; Nichols, T.; French, D.P.; Joshi, P.; Butler, C.C. Expectations for consultations and antibiotics for respiratory tract infection in primary care: The RTI clinical iceberg. Br. J. Gen. Pract. 2013, 63, e429–e436. [Google Scholar] [CrossRef] [Green Version]
- Eudy, J.L.; Pallotta, A.M.; Neuner, E.A.; Brummel, G.L.; Postelnick, M.J.; Schulz, L.T.; Spivak, E.S.; Wrenn, R.H. Antimicrobial Stewardship Practice in the Ambulatory Setting from a National Cohort. Open Forum Infect. Dis. 2020, 7, ofaa513. [Google Scholar] [CrossRef]
- Dutcher, L.; Degnan, K.; Adu-Gyamfi, A.B.; Lautenbach, E.; Cressman, L.; David, M.Z.; Cluzet, V.; E Szymczak, J.; A Pegues, D.; Bilker, W.; et al. Improving Outpatient Antibiotic Prescribing for Respiratory Tract Infections in Primary Care: A Stepped-Wedge Cluster Randomized Trial. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 74, 947–956. [Google Scholar] [CrossRef]
- Köchling, A.; Löffler, C.; Reinsch, S.; Hornung, A.; Böhmer, F.; Altiner, A.; Chenot, J.-F. Reduction of antibiotic prescriptions for acute respiratory tract infections in primary care: A systematic review. Implement. Sci. IS 2018, 13, 47. [Google Scholar] [CrossRef]
- Chan, Y.Y.; Bin Ibrahim, M.A.; Wong, C.M.; Ooi, C.K.; Chow, A. Determinants of antibiotic prescribing for upper respiratory tract infections in an emergency department with good primary care access: A qualitative analysis. Epidemiol. Infect. 2019, 147, e111. [Google Scholar] [CrossRef] [Green Version]
- Yates, T.D.; Davis, M.E.; Taylor, Y.J.; Davidson, L.; Connor, C.D.; Buehler, K.; Spencer, M. Not a magic pill: A qualitative exploration of provider perspectives on antibiotic prescribing in the outpatient setting. BMC Fam. Pract. 2018, 19, 96. [Google Scholar] [CrossRef]
- Khalid, T.Y.; Duncan, L.J.; Thornton, H.V.; Lasseter, G.; Muir, P.; Toney, Z.A.; Hay, A.D. Novel multi-virus rapid respiratory microbiological point-of-care testing in primary care: A mixed-methods feasibility evaluation. Fam. Pract. 2021, 38, 598–605. [Google Scholar] [CrossRef]
- de Lusignan, S.; Hoang, U.; Liyanage, H.; Tripathy, M.; Yonova, I.; Byford, R.; Ferreira, F.; Diez-Domingo, J.; Clark, T. Integrating molecular point-of-care testing for influenza into primary care: A mixed-methods feasibility study. Br. J. Gen. Pract. 2020, 70, e555–e562. [Google Scholar] [CrossRef]
- Vicentini, C.; Vola, L.; Previti, C.; Brescia, V.; Dal Mas, F.; Zotti, C.M.; Bert, F. Antimicrobial Stewardship Strategies Including Point-of-Care Testing (POCT) for Pediatric Patients with Upper-Respiratory-Tract Infections in Primary Care: A Systematic Review of Economic Evaluations. Antibiotics 2022, 11, 1139. [Google Scholar] [CrossRef]
- Bruning, A.H.L.; de Kruijf, W.B.; van Weert, H.C.P.M.; Willems, W.L.M.; de Jong, M.D.; Pajkrt, D.; Wolthers, K.C. Diagnostic performance and clinical feasibility of a point-of-care test for respiratory viral infections in primary health care. Fam. Pract. 2017, 34, 558–563. [Google Scholar] [CrossRef] [Green Version]
- Loens, K.; Van Heirstraeten, L.; Malhotra-Kumar, S.; Goossens, H.; Ieven, M. Optimal sampling sites and methods for detection of pathogens possibly causing community-acquired lower respiratory tract infections. J. Clin. Microbiol. 2009, 47, 21–31. [Google Scholar] [CrossRef] [Green Version]
- Dekker, A.R.J.; Verheij, T.J.M.; van der Velden, A.W. Inappropriate antibiotic prescription for respiratory tract indications: Most prominent in adult patients. Fam. Pract. 2015, 32, 401–407. [Google Scholar] [CrossRef]
- Poss-Doering, R.; Kronsteiner, D.; Kamradt, M.; Andres, E.; Kaufmann-Kolle, P.; Wensing, M.; A Rena-Study Group; Szecsenyi, J. Antibiotic prescribing for acute, non-complicated infections in primary care in Germany: Baseline assessment in the cluster randomised trial ARena. BMC Infect. Dis. 2021, 21, 877. [Google Scholar] [CrossRef]
- Van Deursen, A.M.M.; Verheij, T.J.M.; Rovers, M.M.; Veenhoven, R.H.; Groenwold, R.H.H.; Bonten, M.J.M.; Sanders, E.A.M. Trends in primary-care consultations, comorbidities, and antibiotic prescriptions for respiratory infections in The Netherlands before implementation of pneumococcal vaccines for infants. Epidemiol. Infect. 2012, 140, 823–834. [Google Scholar] [CrossRef] [Green Version]
- Rzepka, A.; Mania, A. An analysis of the clinical picture of respiratory tract infections in primary care patients. Pediatr. Med. Rodz. 2020, 16, 382–388. [Google Scholar] [CrossRef]
- Dahlén, E.; Collin, J.; Hellman, J.; Norman, C.; Nauclér, P.; Ternhag, A. The effect of absent or deferred antibiotic treatment on complications of common infections in primary care. Int. J. Infect. Dis. 2022, 124, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Saliba-Gustafsson, E.A.; Röing, M.; Borg, M.A.; Rosales-Klintz, S.; Lundborg, C.S. General practitioners’ perceptions of delayed antibiotic prescription for respiratory tract infections: A phenomenographic study. PLoS ONE 2019, 14, e0225506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryves, R.; Eyles, C.; Moore, M.; McDermott, L.; Little, P.; Leydon, G.M. Understanding the delayed prescribing of antibiotics for respiratory tract infection in primary care: A qualitative analysis. BMJ Open 2016, 6, e011882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKay, R.; Mah, A.; Law, M.R.; McGrail, K.; Patrick, D.M. Systematic Review of Factors Associated with Antibiotic Prescribing for Respiratory Tract Infections. Antimicrob. Agents Chemother. 2016, 60, 4106–4118. [Google Scholar] [CrossRef] [Green Version]
- Rebnord, I.K.; Sandvik, H.; Mjelle, A.B.; Hunskaar, S. Factors predicting antibiotic prescription and referral to hospital for children with respiratory symptoms: Secondary analysis of a randomised controlled study at out-of-hours services in primary care. BMJ Open 2017, 7, e012992. [Google Scholar] [CrossRef] [Green Version]
- Tonkin-Crine, S.K.; Tan, P.S.; van Hecke, O.; Wang, K.; Roberts, N.W.; McCullough, A.; Hansen, M.P.; Butler, C.C.; Del Mar, C.B. Clinician-targeted interventions to influence antibiotic prescribing behaviour for acute respiratory infections in primary care: An overview of systematic reviews. Cochrane Database Syst. Rev. 2017, 9, CD012252. [Google Scholar] [CrossRef] [Green Version]
- Hardy, V.; Thompson, M.; Keppel, G.A.; Alto, W.; Dirac, M.A.; Neher, J.; Sanford, C.; Hornecker, J.; Cole, A. Qualitative study of primary care clinicians’ views on point-of-care testing for C-reactive protein for acute respiratory tract infections in family medicine. BMJ Open 2017, 7, e012503. [Google Scholar] [CrossRef]
- Cooke, J.; Llor, C.; Hopstaken, R.; Dryden, M.; Butler, C. Respiratory tract infections (RTIs) in primary care: Narrative review of C reactive protein (CRP) point-of-care testing (POCT) and antibacterial use in patients who present with symptoms of RTI. BMJ Open Respir. Res. 2020, 7, e000624. [Google Scholar] [CrossRef]
- Lhopitallier, L.; Kronenberg, A.; Meuwly, J.Y.; Locatelli, I.; Mueller, Y.; Senn, N.; D’acremont, V.; Boillat-Blanco, N. Procalcitonin and lung ultrasonography point-of-care testing to determine antibiotic prescription in patients with lower respiratory tract infection in primary care: Pragmatic cluster randomised trial. BMJ 2021, 374, n2132. [Google Scholar] [CrossRef]
- Schuetz, P.; Wirz, Y.; Sager, R.; Christ-Crain, M.; Stolz, D.; Tamm, M. Procalcitonin to initiate or discontinue antibiotics in acute respiratory tract infections. Cochrane Database Syst. Rev. 2017, 10, CD007498. [Google Scholar] [CrossRef] [Green Version]
- Sydenham, R.V.; Hansen, M.P.; Justesen, U.S.; Pedersen, L.B.; Aabenhus, R.M.; Wehberg, S.; Jarbøl, D.E. Factors associated with C-reactive protein testing when prescribing antibiotics in general practice: A register-based study. BMC Prim. Care 2022, 23, 17. [Google Scholar] [CrossRef]
- Martínez-González, N.A.; Keizer, E.; Plate, A.; Coenen, S.; Valeri, F.; Verbakel, J.Y.J.; Rosemann, T.; Neuner-Jehle, S.; Senn, O. Point-of-Care C-Reactive Protein Testing to Reduce Antibiotic Prescribing for Respiratory Tract Infections in Primary Care: Systematic Review and Meta-Analysis of Randomised Controlled Trials. Antibiotics 2020, 9, 610. [Google Scholar] [CrossRef]
- Boere, T.M.; El Alili, M.; van Buul, L.W.; Hopstaken, R.M.; Verheij, T.J.M.; Hertogh, C.M.P.M.; van Tulder, M.W.; E Bosmans, J. Cost-effectiveness and return-on-investment of C-reactive protein point-of-care testing in comparison with usual care to reduce antibiotic prescribing for lower respiratory tract infections in nursing homes: A cluster randomised trial. BMJ Open 2022, 12, e055234. [Google Scholar] [CrossRef]
- Tonkin-Crine, S.; Yardley, L.; Little, P. Antibiotic prescribing for acute respiratory tract infections in primary care: A systematic review and meta-ethnography. J. Antimicrob. Chemother. 2011, 66, 2215–2223. [Google Scholar] [CrossRef] [Green Version]
- Thompson, W.; McCormack, S. Interventions to Influence the Use of Antibiotics for Acute Upper Respiratory Tract Infections [Internet]; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2021. [Google Scholar]
- Schneider, J.E.; Boehme, C.; Borisch, B.; Dittrich, S. Application of a simple point-of-care test to reduce UK healthcare costs and adverse events in outpatient acute respiratory infections. J. Med. Econ. 2020, 23, 673–682. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Feature | Number of Patients | Median | IQR | 95%CI |
|---|---|---|---|---|
| Age (years) | 631 | 48 | 36–63 | 46–51 |
| Sex M/F | 264/367 | |||
| Fever Y/N | 333/298 | |||
| Flu-test P/N | 90/266 | |||
| Number of comorbidities | 631 | 3 | 2–5 | 3–3 |
| Comorbidities complexity Y/N | 148/484 | |||
| URTI Y/N | 492/139 | |||
| LRTI Y/N | 182/449 | |||
| Number of visits | 632 | 2 | 1–2 | 2–2 |
| WBC (G/L) | 333 | 7.1 | 5.4–8.8 | 5.89–7.80 |
| Neutrophils (G/L) | 333 | 3.8 | 2.85–5.81 | 3.28–4.30 |
| Lymphocytes (G/L) | 333 | 2.3 | 1.90–2.85 | 2.17–2.60 |
| CRP (mg/dL) | 261 | 19 | 11–30 | 15.0–21.81 |
| ESR (mm/h) | 261 | 20 | 12–28 | 15–22 |
| Feature | Patients Receiving Antibiotics | Patients Not Receiving Antibiotics | p | OR (95%CI) | ||||
|---|---|---|---|---|---|---|---|---|
| Number of Patients | Median | IQR | Number of Patients | Median | IQR | |||
| Age (years) | 269 | 51 | 38–66 | 362 | 47 | 35–62 | 0.008 * | 1.01 (1.01–1.04) |
| Sex M/F | 111/158 | 153/209 | 0.778 | - | ||||
| Fever Y/N | 208/61 | 90/272 | <0.0001 * | 10.31 (7.11–14.94) | ||||
| Flu test P/N | 18/132 | 72/134 | <0.0001 * | 0.26 (0.14–0.44) | ||||
| Number of comorbidities | 269 | 4 | 2–6 | 362 | 3 | 1–4 | <0.0001 * | 2.19 (1.51–3.19) |
| Comorbidities complexity Y/N | 85/184 | 63/299 | <0.0001 * | 2.19 (1.51–3.19) | ||||
| Number of visits | 269 | 2 | 1–3 | 362 | 1 | 1–2 | <0.0001 * | 2.15 (1.74–2.66) |
| URTI Y/N | 193/76 | 299/63 | 0.001 | 0.53 (0.36–0.78) | ||||
| LRTI Y/N | 98/171 | 84/278 | 0.0003 * | 1.89 (1.34–2.68) | ||||
| Cough Y/N | 169/100 | 111/151 | 0.0014 * | 1.69 (1.23–2.33) | ||||
| Throat pain Y/N | 154/115 | 201/161 | 0.67 | - | ||||
| Wheezing Y/N | 75/194 | 13/349 | <0.0001 * | 10.37 (5.61–19.18) | ||||
| Crackles Y/N | 23/246 | 1/361 | <0.0001 * | 33.75 (4.52–251.58) | ||||
| WBC (G/L) | 112 | 8.60 | 5.55–9.10 | 221 | 7.0 | 5.05–7.75 | 0.22 | - |
| Neutrophils (G/L) | 112 | 5.85 | 3.8–7.35 | 221 | 3.70 | 2.62–4.52 | 0.27 | - |
| Lymphocytes (G/L) | 112 | 2.35 | 2.01–2.60 | 221 | 2.30 | 1.80–2.95 | 0.97 | - |
| CRP (mg/dL) | 112 | 19 | 15.75–30.50 | 221 | 10 | 11.1–26.2 | 0.55 | - |
| ESR (mm/h) | 112 | 20 | 11.75–30.00 | 221 | 17.5 | 10.75–20.0 | 0.48 | - |
| Feature | Patients Receiving Antibiotics | Patients not Receiving Antibiotics | p | OR (95%CI) |
|---|---|---|---|---|
| Number of Patients N = 269 | Number of Patients N = 362 | |||
| Diabetes Y/N | 51/218 | 22/340 | <0.0001 * | 3.62 (2.13–6.13) |
| Obesity Y/N | 37/232 | 44/318 | <0.0001 * | 3.63 (2.13–6.16) |
| Inflammatory bowel disease Y/N | 27/242 | 19/343 | 0.022 * | 2.01 (1.09–3.70) |
| Hypertension Y/N | 126/143 | 123/239 | 0.001 * | 1.71 (1.24–2.37) |
| Cigarette smoking Y/N | 72/197 | 59/303 | 0.0014 * | 3.45 (1.07–11.14) |
| Hypercholesterolemia Y/N | 83/186 | 88/274 | 0.07 | - |
| Malignancy Y/N | 17/252 | 15/347 | 0.22 | - |
| Degenerative spine conditions Y/N | 110/159 | 102/260 | 0.0008 * | 1.76 (1.26–2.46) |
| Epilepsy Y/N | 10/259 | 4/358 | 0.027 * | 2.15 (1.74–2.66) |
| Headaches Y/N | 121/148 | 123/239 | 0.005 * | 1.58 (1.15–2.19) |
| Chronic ischemic heart disease Y/N | 20/249 | 8/354 | 0.0016 * | 3.55 (1.54–8.19) |
| Chronic obstructive pulmonary disease Y/N | 34/235 | 17/345 | 0.0003 * | 1.89 (1.00–3.57) |
| Asthma Y/N | 22/247 | 22/340 | 0.31 | - |
| Feature | aOR | 95%CI | p |
|---|---|---|---|
| Comorbidities complexity | 2.62 | 1.54–4.46 | 0.0004 |
| Fever | 32.59 | 19.15–55.47 | <0.0001 * |
| Positive flu-test | 0.0015 | 0.0001–0.0168 | <0.0001 * |
| Number of visits | 4.15 | 2.39–7.20 | <0.0001 * |
| Crackles | 26.35 | 2.77–250.81 | 0.044 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rzepka, A.; Mania, A. Positive Point-of-Care Influenza Test Significantly Decreases the Probability of Antibiotic Treatment during Respiratory Tract Infections in Primary Care. Diagnostics 2023, 13, 2031. https://doi.org/10.3390/diagnostics13122031
Rzepka A, Mania A. Positive Point-of-Care Influenza Test Significantly Decreases the Probability of Antibiotic Treatment during Respiratory Tract Infections in Primary Care. Diagnostics. 2023; 13(12):2031. https://doi.org/10.3390/diagnostics13122031
Chicago/Turabian StyleRzepka, Aneta, and Anna Mania. 2023. "Positive Point-of-Care Influenza Test Significantly Decreases the Probability of Antibiotic Treatment during Respiratory Tract Infections in Primary Care" Diagnostics 13, no. 12: 2031. https://doi.org/10.3390/diagnostics13122031