
Impact of Robotic-Assisted Gait Training in Subacute Spinal Cord Injury Patients on Outcome Measure

Abstract
:1. Introduction
2. Methods
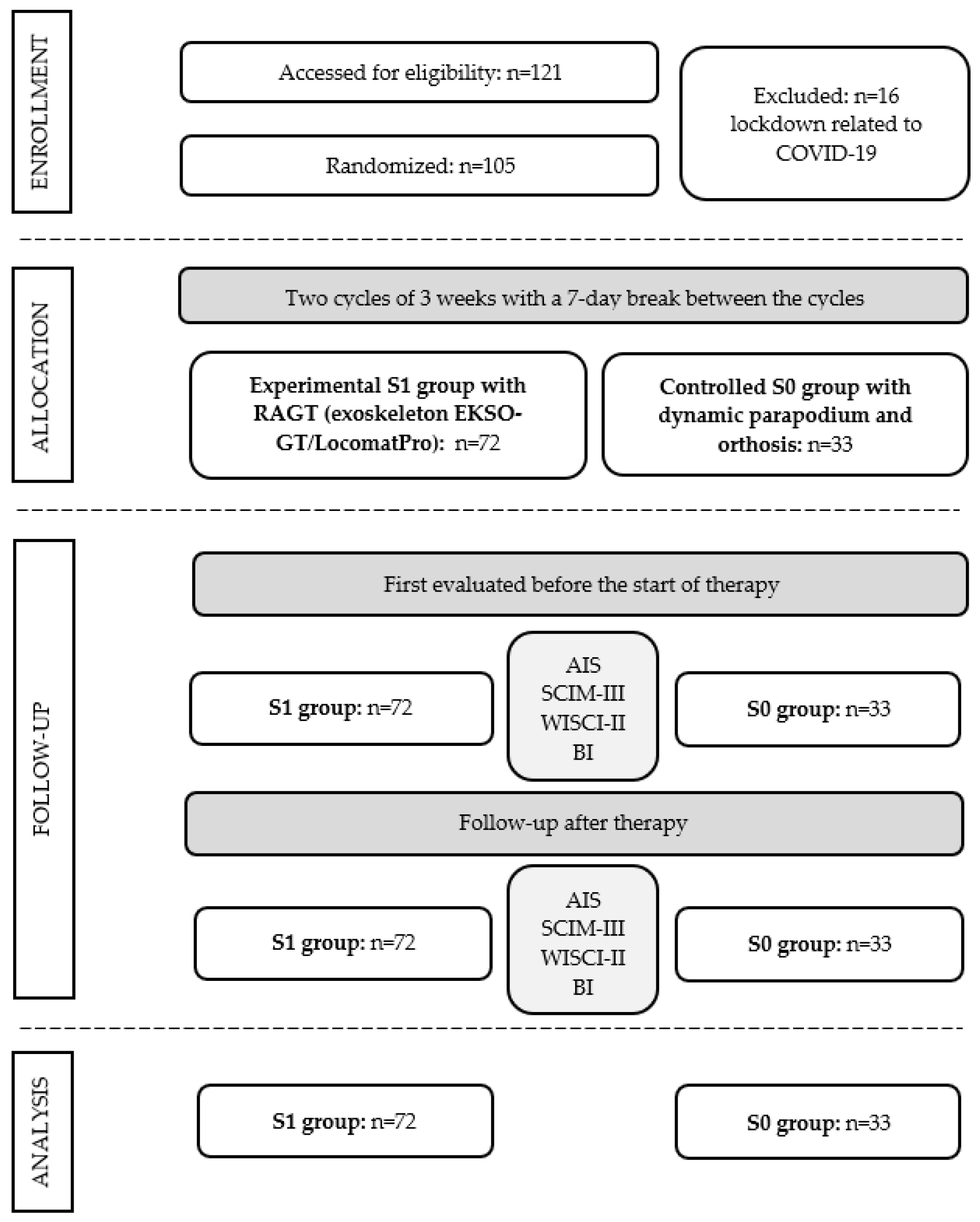
2.1. Data Source and Study Population
2.2. Statistical Methods
3. Results
3.1. Characteristics of the Investigated Group
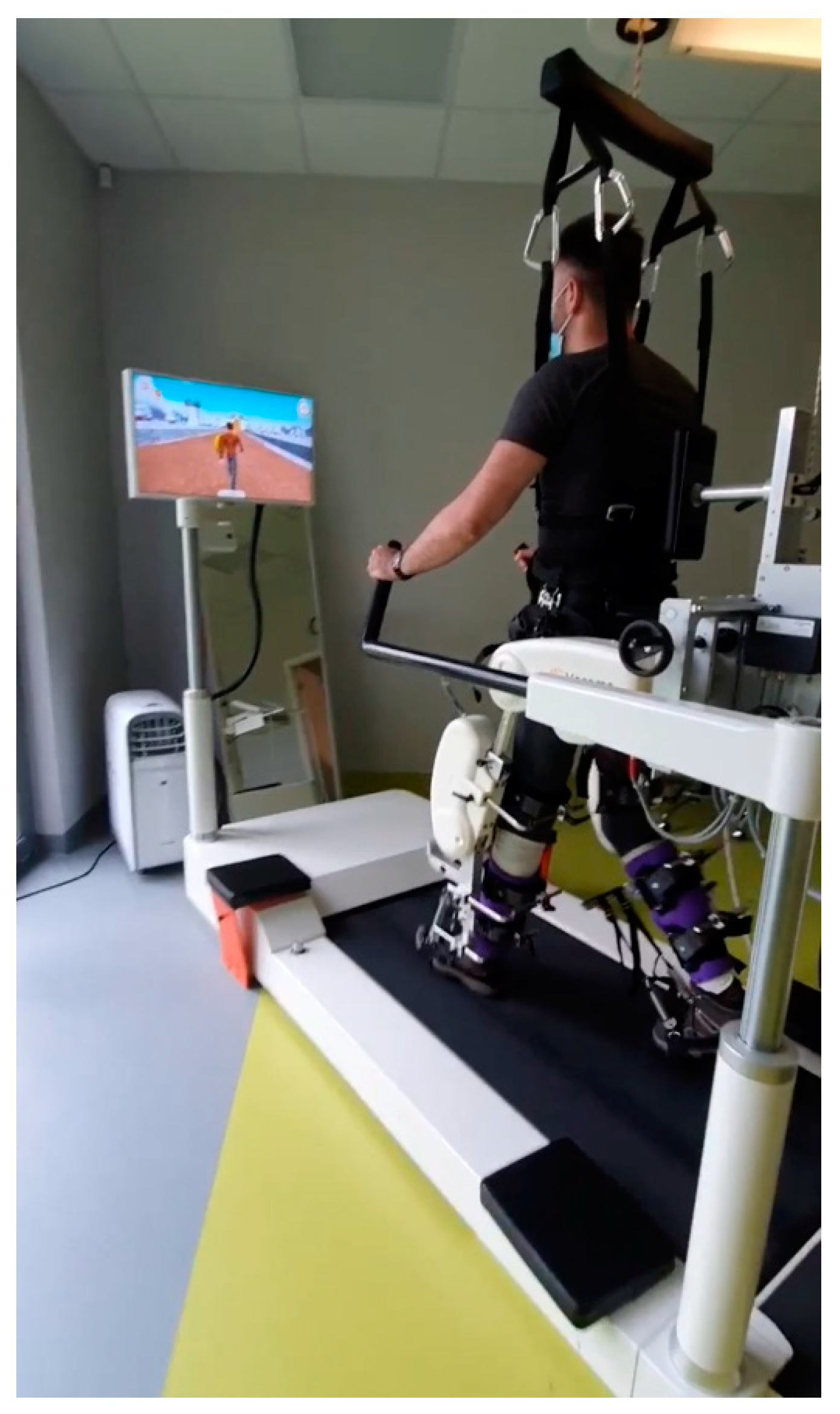
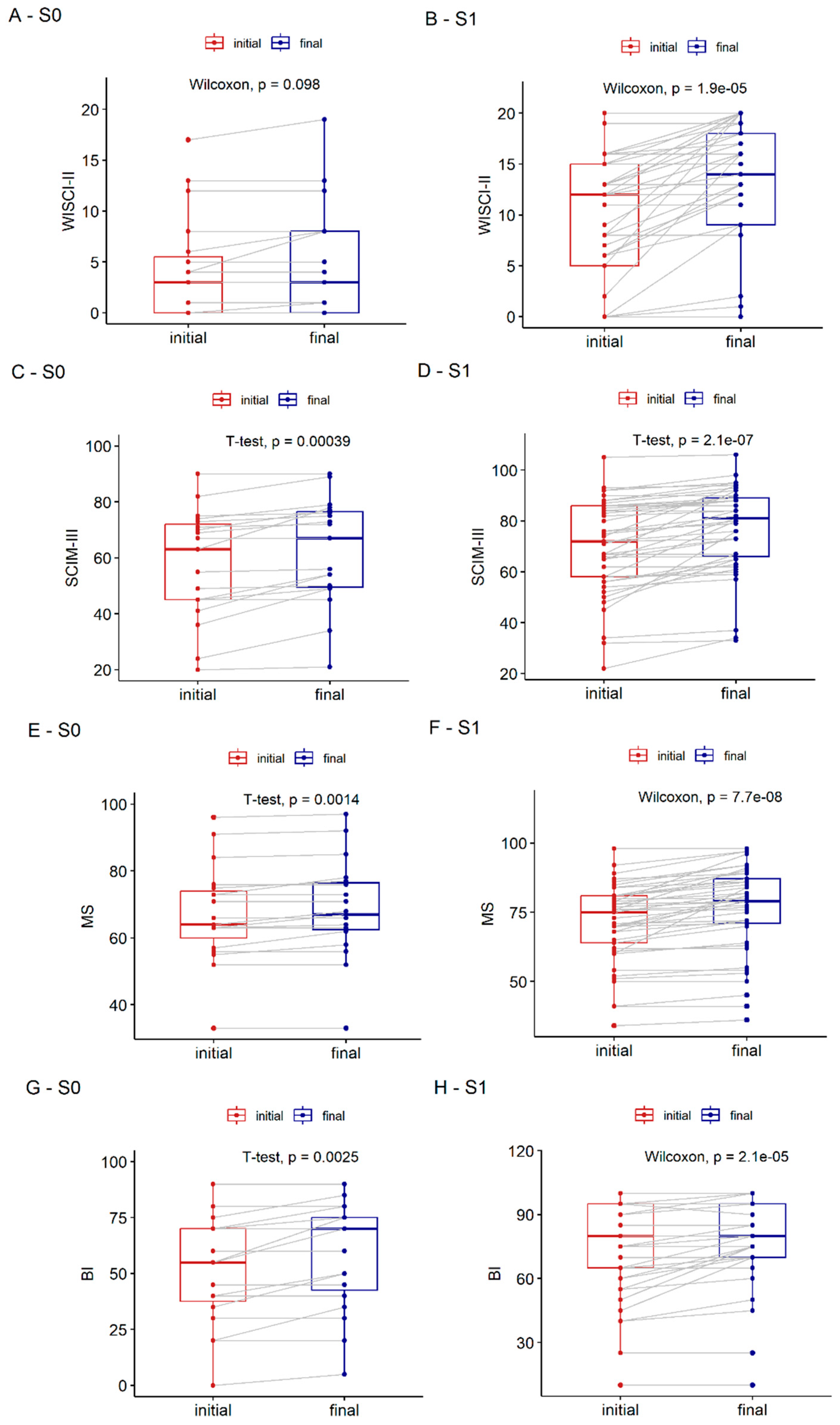
3.2. Functional and Neurological Improvement Depending on the Type of Rehabilitation
3.3. Effect of Rehabilitation on the Functional and Neurological Scales in Patients with Incomplete Spinal Cord Injury (AIS-B, C, and D)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haas, B.; Playford, E.D.; Ahmad, A.Q.; Yildiran, T.; Gibbon, A.J.; Freeman, J.A. Rehabilitation goals of people with spinal cord injuries can be classified against the International Classification of Functioning, Disability and Health Core Set for spinal cord injuries. Spinal Cord 2016, 54, 324–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ditunno, P.L.; Patrick, M.; Stineman, M.; Ditunno, J.F. Who wants to walk? Preferences for recovery after SCI: A longitudinal and cross-sectional study. Spinal Cord 2008, 46, 500–506. [Google Scholar] [CrossRef] [PubMed]
- Simpson, L.A.; Eng, J.J.; Hsieh, J.T.; Wolfe, D.L. Spinal Cord Injury Rehabilitation Evidence Scire Research Team. The health and life priorities of individuals with spinal cord injury: A systematic review. J. Neurotrauma 2012, 29, 1548–1555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mekki, M.; Delgado, A.D.; Fry, A.; Putrino, D.; Huang, V. Robotic Rehabilitation and Spinal Cord Injury: A Narrative Review. Neurotherapeutics 2018, 15, 604–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gómara-Toldrà, N.; Sliwinski, M.; Dijkers, M.P. Physical therapy after spinal cord injury: A systematic review of treatments focused on participation. J. Spinal Cord Med. 2014, 37, 371–379. [Google Scholar] [CrossRef] [Green Version]
- Chang, F.; Zhang, Q.; Xie, H.; Yang, Y.; Sun, M.; Wu, A.; Wu, J.; Chen, G.; Shen, F.; Li, C.; et al. Effects of a rehabilitation program for individuals with chronic spinal cord injury in Shanghai, China. BMC Health Serv. Res. 2020, 20, 298. [Google Scholar] [CrossRef] [Green Version]
- Sconza, C.; Negrini, F.; Di Matteo, B.; Borboni, A.; Boccia, G.; Petrikonis, I.; Stankevičius, E.; Casale, R. Robot-Assisted Gait Training in Patients with Multiple Sclerosis: A Randomized Controlled Crossover Trial. Medicina 2021, 57, 713. [Google Scholar] [CrossRef]
- Jin, L.H.; Yang, S.S.; Choi, J.Y.; Sohn, M.K. The Effect of Robot-Assisted Gait Training on Locomotor Function and Functional Capability for Daily Activities in Children with Cerebral Palsy: A Single-Blinded, Randomized Cross-Over Trial. Brain Sci. 2020, 10, 801. [Google Scholar] [CrossRef]
- Yun, S.J.; Lee, H.H.; Lee, W.H.; Lee, S.H.; Oh, B.M.; Seo, H.G. Effect of robot-assisted gait training on gait automaticity in Parkinson disease: A prospective, open-label, single-arm, pilot study. Medicine 2021, 100, e24348. [Google Scholar] [CrossRef]
- Duan, R.; Qu, M.; Yuan, Y.; Lin, M.; Liu, T.; Huang, W.; Gao, J.; Zhang, M.; Yu, X. Clinical Benefit of Rehabilitation Training in Spinal Cord Injury: A Systematic Review and Meta-Analysis. Spine 2021, 46, 398–410. [Google Scholar] [CrossRef]
- Holanda, L.J.; Silva, P.M.M.; Amorim, T.C.; Lacerda, M.O.; Simão, C.R.; Morya, E. Robotic assisted gait as a tool for rehabilitation of individuals with spinal cord injury: A systematic review. J. Neuroeng. Rehabil. 2017, 14, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nam, K.Y.; Kim, H.J.; Kwon, B.S.; Park, J.W.; Lee, H.J.; Yoo, A. Robot-assisted gait training (Lokomat) improves walking function and activity in people with spinal cord injury: A systematic review. J. NeuroEng. Rehabil. 2017, 14, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguirre-Güemez, A.V.; Pérez-Sanpablo, A.I.; Quinzaños-Fresnedo, J.; Pérez-Zavala, R.; Barrera-Ortiz, A. Walking speed is not the best outcome to evaluate the effect of robotic assisted gait training in people with motor incomplete Spinal Cord Injury: A Systematic Review with meta-analysis. J. Spinal Cord Med. 2019, 42, 142–154. [Google Scholar] [CrossRef]
- Fang, C.Y.; Tsai, J.L.; Li, G.S.; Lien, A.S.; Chang, Y.J. Effects of Robot-Assisted Gait Training in Individuals with Spinal Cord Injury: A Meta-analysis. BioMed Res. Int. 2020, 2020, 2102785. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Ding, M.; Wang, J.; Pan, H.; Sun, X.; Huang, L.; Fu, C.; He, C.; Wei, Q. Effectiveness of robotic-assisted gait training on cardiopulmonary fitness and exercise capacity for incomplete spinal cord injury: A systematic review and meta-analysis of randomized controlled trials. Clin. Rehabil. 2023, 37, 312–329. [Google Scholar] [CrossRef]
- Alashram, A.R.; Annino, G.; Padua, E. Robot-assisted gait training in individuals with spinal cord injury: A systematic review for the clinical effectiveness of Lokomat. J. Clin. Neurosci. 2021, 91, 260–269. [Google Scholar] [CrossRef]
- Ilha, J.; Meireles, A.; de Freitas, G.R.; do Espírito Santo, C.C.; Machado-Pereira, N.A.M.M.; Swarowsky, A.; Santos, A.R.S. Overground gait training promotes functional recovery and cortical neuroplasticity in an incomplete spinal cord injury model. Life Sci. 2019, 232, 116627. [Google Scholar] [CrossRef]
- Zhang, M.; Davies, T.; Xie, S. Effectiveness of robot-assisted therapy on ankle rehabilitation—A systematic review. J. Neuroeng. Rehabil. 2013, 10, 30. [Google Scholar] [CrossRef] [Green Version]
- Bae, Y.; Chang, W.H.; Fong, S. Different Effects of Robot-Assisted Gait and independent Over-Ground Gait on Foot Plantar Pressure in Incomplete Spinal Cord Injury: A Preliminary Study. Int. J. Environ. Res. Public Health 2021, 18, 12072. [Google Scholar] [CrossRef]
- Hong, E.; Gorman, P.H.; Forrest, G.F.; Asselin, P.K.; Knezevic, S.; Scott, W.; Wojciehowski, S.B.; Kornfeld, S.; Spungen, A.M. Mobility Skills with Exoskeletal-Assisted Walking in Persons With SCI: Results From a Three Center Randomized Clinical Trial. Front. Robot AI 2020, 7, 93. [Google Scholar] [CrossRef]
- American Spinal Injury Association. International Standards for Neurological Classification of Spinal Cord Injury, 2002 Revision; American Spinal Injury Association: Chicago, IL, USA, 2002. [Google Scholar]
- Itzkovich, M.; Gelernter, I.; Biering-Sorensen, F.; Weeks, C.; Laramee, M.T.; Craven, B.C.; Tonack, M.; Hitzig, S.L.; Glaser, E.; Zeilig, G.; et al. The Spinal Cord Independence Measure (SCIM) version III: Reliability and validity in a multi-center international study. Disabil Rehabil. 2007, 29, 1926–1933. [Google Scholar] [CrossRef] [PubMed]
- Ditunno, J.F.; Scivoletto, G.; Patrick, M.; Biering-Sorensen, F.; Abel, R.; Marino, R. Validation of the walking index for spinal cord injury in a US and European clinical population. Spinal Cord 2008, 46, 181–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collin, C.; Wade, D.T.; Davies, S.; Horne, V. The Barthel ADL Index: A reliability study. Int. Disabil Stud. 1988, 10, 61–63. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment Software for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 14 November 2021).
- Wickham, H.; Bryan, J. Readxl: Read Excel Files. R Package Version 1.3.1. 2019. Available online: https://CRAN.R-project.org/package=readxl (accessed on 11 November 2021).
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016; ISBN 978-3-319-24277-4. Available online: http://ggplot2.org (accessed on 11 November 2021).
- DeWitt, P. Qwraps2: Quick Wraps 2. R Package Version 0.5.2. 2021. Available online: https://CRAN.R-project.org/package=qwraps2 (accessed on 11 November 2021).
- Allaire, J.; Xie, Y.; McPherson, J.; Luraschi, J.; Ushey, K.; Atkins, A.; Wickham, H.; Cheng, J.; Chang, W.; Iannone, R. Rmarkdown: Dynamic Documents for R. R Package Version 2.14. 2022. Available online: https://github.com/rstudio/rmarkdown (accessed on 11 November 2021).
- Kassambara, A. ggpubr: “ggplot2” Based Publication Ready Plots. 2018. Available online: https://cran.r-project.org/package=ggpubr (accessed on 11 November 2021).
- Hugh-Jones, D. Huxtable: Easily Create and Style Tables for ## LaTeX, HTML and Other Formats. R Package Version 5.4.0. 2021. Available online: https://CRAN.R-project.org/package=huxtable (accessed on 11 November 2021).
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; D’Agostino McGowan, L.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef] [Green Version]
- Zieriacks, A.; Aach, M.; Brinkemper, A.; Koller, D.; Schildhauer, T.A.; Grasmücke, D. Rehabilitation of Acute vs. Chronic Patients with Spinal Cord Injury with a Neurologically Controlled Hybrid Assistive Limb Exoskeleton: Is There a Difference in Outcome? Front. Neurorobot. 2021, 15, 728327. [Google Scholar] [CrossRef]
- Shin, J.C.; Kim, J.Y.; Park, H.K.; Kim, N.Y. Effect of robotic-assisted gait training in patients with incomplete spinal cord injury. Ann. Rehabil. Med. 2014, 38, 719–725. [Google Scholar] [CrossRef]
- Alcobendas-Maestro, M.; Esclarín-Ruz, A.; Casado-López, R.M.; Muñoz-González, A.; Pérez-Mateos, G.; González-Valdizán, E.; Martín, J.L. Lokomat robotic-assisted versus overground training within 3 to 6 months of incomplete spinal cord lesion: Randomized controlled trial. Neurorehabil. Neural Repair 2012, 26, 1058–1063. [Google Scholar] [CrossRef]
- Esclarín-Ruz, A.; Alcobendas-Maestro, M.; Casado-Lopez, R.; Perez-Mateos, G.; Florido-Sanchez, M.A.; Gonzalez-Valdizan, E.; Martin, J.L. A comparison of robotic walking therapy and conventional walking therapy in individuals with upper versus lower motor neuron lesions: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2014, 95, 1023–1031. [Google Scholar] [CrossRef]
- Labruyère, R.; van Hedel, H.J. Strength training versus robot-assisted gait training after incomplete spinal cord injury: A randomized pilot study in patients depending on walking assistance. J. Neuroeng. Rehabil. 2014, 11, 4. [Google Scholar] [CrossRef] [Green Version]
- Wirth, B.; van Hedel, H.J.; Kometer, B.; Dietz, V.; Curt, A. Changes in activity after a complete spinal cord injury as measured by the Spinal Cord Independence Measure II (SCIM II). Neurorehabil. Neural Repair 2008, 22, 145–153. [Google Scholar] [CrossRef] [Green Version]
- Anderson, K.; Aito, S.; Atkins, M.; Biering-Sørensen, F.; Charlifue, S.; Curt, A.; Ditunno, J.; Glass, C.; Marino, R.; Marshall, R.; et al. Functional Recovery Outcome Measures Work Group. Functional recovery measures for spinal cord injury: An evidence-based review for clinical practice and research. J. Spinal Cord Med. 2008, 31, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Benito-Penalva, J.; Edwards, D.J.; Opisso, E.; Cortes, M.; Lopez-Blazquez, R.; Murillo, N.; Costa, U.; Tormos, J.M.; Vidal-Samsó, J.; Eurpean Multicenter Study about Human Spinal Cord Injury Study Group; et al. Gait training in human spinal cord injury using electromechanical systems: Effect of device type and patient characteristics. Arch. Phys. Med. Rehabil. 2012, 93, 404–412. [Google Scholar] [CrossRef] [PubMed]
- Jackson, A.B.; Carnel, C.T.; Ditunno, J.F.; Read, M.S.; Boninger, M.L.; Schmeler, M.R.; Williams, S.R.; Donovan, W.H. Gait and Ambulation Subcommittee. Outcome measures for gait and ambulation in the spinal cord injury population. J. Spinal Cord Med. 2008, 31, 487–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirshblum, S.; Snider, B.; Eren, F.; Guest, J. Characterizing Natural Recovery after Traumatic Spinal Cord Injury. J. Neurotrauma 2021, 38, 1267–1284. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Lin, F.; Sun, L.; Chen, C. Comparison of Efficacy of Lokomat and Wearable Exoskeleton-Assisted Gait Training in People with Spinal Cord Injury: A Systematic Review and Network Meta-Analysis. Front. Neurol. 2022, 13, 772660. [Google Scholar] [CrossRef]
- Lee, S.H.; Park, G.; Cho, D.Y.; Kim, H.Y.; Lee, J.Y.; Kim, S.; Park, S.B.; Shin, J.H. Comparisons between end-effector and exoskeleton rehabilitation robots regarding upper extremity function among chronic stroke patients with moderate-to-severe upper limb impairment. Sci. Rep. 2020, 10, 1806. [Google Scholar] [CrossRef] [Green Version]
- Molteni, F.; Gasperini, G.; Cannaviello, G.; Guanziroli, E. Exoskeleton and End-Effector Robots for Upper and Lower Limbs Rehabilitation: Narrative Review. PM&R 2018, 10, 174–188. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | S0 (N = 33) | S1 (N = 72) | p-Value |
|---|---|---|---|
| Sex | |||
| Women | 5 (15.15%) | 14 (19.44%) | 0.797 1 |
| Men | 28 (84.85%) | 58 (80.56%) | |
| Cause of injury | |||
| Vehicle accident | 13 (39.39%) | 24 (33.33%) | 0.067 2 |
| Fall < 1 m | 2 (6.06%) | 4 (5.56%) | |
| Fall > 1 m | 9 (27.27%) | 24 (33.33%) | |
| Dive | 1 (3.03%) | 4 (5.56%) | |
| Body crushing | 4 (12.12%) | 0 (0.00%) | |
| Others | 4 (12.12%) | 16 (22.22%) | |
| AIS | |||
| A | 14 (42.42%) | 27 (37.50%) | 0.068 2 |
| B | 4 (12.12%) | 7 (9.72%) | |
| C | 11 (33.33%) | 13 (18.06%) | |
| D | 4 (12.12%) | 25 (34.72%) | |
| Level of neurological impairment | |||
| Cervical | 7 (21.21%) | 17 (23.61%) | 0.794 1 |
| Thoracic | 17 (51.52%) | 32 (44.44%) | |
| Lumbar | 9 (27.27%) | 23 (31.94%) | |
| Age | |||
| Median (IQR) | 36.5 (20.5) | 35.5 (16.75) | 0.767 3 |
| Time from accident (months) | |||
| Median (IQR) | 13 (13) | 13 (10) | 0.594 3 |
| S0 (N = 33) | S1 (N = 72) | Unadjusted Model | Adjusted Model | |||||
|---|---|---|---|---|---|---|---|---|
| Baseline, Mean ± SD | Final Mean ± SD | Change from Baseline, Mean ± SD | Baseline, Mean ± SD | Final, Mean ± SD | Change from Baseline, Mean ± SD | S0–S1 Difference (SE) | S0–S1 Difference $ (SE) | |
| WISCI-II | 2.73 ± 4.69 | 3.09 ± 4.97 | 0.36 ± 0.96 | 6.54 ± 6.52 | 8.83 ± 7.61 | 2.29 ± 3.43 | 1.93 (0.61) ** | 1.940 (0.63) ** |
| SCIM-III | 57.97 ± 17.10 | 63.61 ± 15.90 | 5.64 ± 5.43 | 66.97 ± 15.88 | 72.65 ± 15.39 | 5.68 ± 6.67 | 0.044 (1.33) | 1.113 (1.23) |
| MS | 60.09 ± 14.74 | 61.30 ± 14.97 | 1.21 ± 1.71 | 63.96 ± 14.91 | 67.16 ± 17.30 | 3.20 ± 4.54 | 1.99 (0.82) * | 1.73 (1.12) * |
| BI | 56.21 ± 21.25 | 61.21 ± 19.53 | 5.00 ± 6.96 | 70.35 ± 19.94 | 75.28 ± 17.97 | 5.00 ± 7.12 | 0 (1.49) | −0.26 (1.5) |
| Parameter | MS_Change | pval | WISCI_Change | pval | SCIM_Change | pval | BI_Change | pval |
|---|---|---|---|---|---|---|---|---|
| Age | −0.04 | 0.56 | −0.11 | 0.15 | 0.14 | 0.05 | 0.03 | 0.66 |
| Time since the accident | 0.08 | 0.29 | 0.06 | 0.41 | −0.007 | 0.92 | 0.01 | 0.89 |
| AIS-A (n = 14) | AIS-B, C, and D (n = 19) | |||
| S0 N = 33 | Median (IQR) | Median (IQR) | p-Value | |
| WISCI-II | 0 (0–0) | 0 (0–0) | 0.32 | |
| SCIM-III | 4 (11–1.25) | 4 (8–1) | 0.45 | |
| MS | 0 (0.75–0) | 1 (3.5–0) | 0.08 | |
| BI | 0 (5–0) | 0 (10–0) | 0.60 | |
| AIS-A (n = 27) | AIS-B, C, and D (n = 45) | |||
| S1 N = 72 | Median (IQR) | Median (IQR) | p-Value | |
| WISCI-II | 0 (1–0) | 1 (5–0) | 0.63 | |
| SCIM-III | 2 (6–0) | 4 (9–2) | 0.06 | |
| MS | 0 (0–0) | 4 (7–2) | <0.001 | |
| BI | 0 (5–0) | 5 (5–0) | 0.64 |
| S0 (N = 19) | S1 (N = 45) | Unadjusted Model | Adjusted Model | |||||
|---|---|---|---|---|---|---|---|---|
| Baseline, Mean ±SD | Final Mean ± SD | Change from Baseline, Mean ± SD | Baseline, Mean ± SD | Final, Mean ± SD | Change from Baseline, Mean ± SD | S0–S1 Difference (SE) | S0–S1 Difference $ (SE) | |
| WISCI-II | 4.05 ± 5.09 | 4.53 ± 5.47 | 0.47± 1.07 | 9.42 ± 6.42 | 12.47 ± 6.92 | 3.04± 3.95 | 2.57 (0.92) ** | 3.07 (1.02) ** |
| SCIM-III | 57.58 ± 19.55 | 62.53 ± 18.69 | 4.95 ± 4.96 | 70.56 ± 18.05 | 77.24 ± 16.75 | 6.69± 7.30 | 1.74 (1.8) | 2.29 (1.799) |
| MS | 67.05 ± 14.45 | 68.68 ± 14.50 | 1.63± 1.89 | 71.47 ± 14.08 | 76.46 ± 15.46 | 4.99± 4.93 | 3.36 (1.17) ** | 2.583 (1.21) * |
| BI | 52.37 ± 23.94 | 57.89 ± 23.65 | 5.53 ± 6.85 | 75.33 ± 21.41 | 80.33 ± 19.61 | 5 ± 6.83 | −0.53 (1.87) | 1.15 (1.86) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tarnacka, B.; Korczyński, B.; Frasuńska, J. Impact of Robotic-Assisted Gait Training in Subacute Spinal Cord Injury Patients on Outcome Measure. Diagnostics 2023, 13, 1966. https://doi.org/10.3390/diagnostics13111966
Tarnacka B, Korczyński B, Frasuńska J. Impact of Robotic-Assisted Gait Training in Subacute Spinal Cord Injury Patients on Outcome Measure. Diagnostics. 2023; 13(11):1966. https://doi.org/10.3390/diagnostics13111966
Chicago/Turabian StyleTarnacka, Beata, Bogumił Korczyński, and Justyna Frasuńska. 2023. "Impact of Robotic-Assisted Gait Training in Subacute Spinal Cord Injury Patients on Outcome Measure" Diagnostics 13, no. 11: 1966. https://doi.org/10.3390/diagnostics13111966