
Post-Operative and Mid-Term Renal Function Impairment Following Elective Fenestrated Endovascular Aortic Repair for Complex Aortic Aneurysms: Incidence and Risk Factors Analysis
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Definitions
2.2. Renal Function Monitoring
2.3. Endpoints
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Antoniou, G.A.; Juszczak, M.T.; Antoniou, S.A.; Katsargyris, A.; Haulon, S. Editor’s Choice-Fenestrated or Branched Endovascular versus Open Repair for Complex Aortic Aneurysms: Meta-Analysis of Time to Event Propensity Score Matched Data. Eur. J. Soc. Vasc. Surg. 2021, 61, 228–237. [Google Scholar] [CrossRef] [PubMed]
- Latz, C.A.; Boitano, L.; Schwartz, S.; Swerdlow, N.; Dansey, K.; Varkevisser, R.R.; Patel, V.; Schermerhorn, M.L. Editor’s Choice-Mortality is High Following Elective Open Repair of Complex Abdominal Aortic Aneurysms. Eur. J. Soc. Vasc. Surg. 2021, 61, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Wanhainen, A.; Verzini, F.; Van Herzeele, I.; Allaire, E.; Bown, M.; Cohnert, T.; Dick, F.; van Herwaarden, J.; Karkos, C.; Koelemay, M.; et al. Editor’s Choice-European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-iliac Artery Aneurysms. Eur. J. Soc. Vasc. Surg. 2019, 57, 8–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mastracci, T.M.; Eagleton, M.J.; Kuramochi, Y.; Bathurst, S.; Wolski, K. Twelve-year results of fenestrated endografts for juxtarenal and group IV thoracoabdominal aneurysms. J. Vasc. Surg. 2015, 61, 355–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verhoeven, E.L.G.; Katsargyris, A.; Oikonomou, K.; Kouvelos, G.; Renner, H.; Ritter, W. Fenestrated Endovascular Aortic Aneurysm Repair as a First Line Treatment Option to Treat Short Necked, Juxtarenal, and Suprarenal Aneurysms. Eur. J. Soc. Vasc. Surg. 2016, 51, 775–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oderich, G.S.; Tenorio, E.R.M.; Mendes, B.C.; Lima, G.B.B.; Marcondes, G.B.; Saqib, N.M.; Hofer, J.R.; Wong, J.M.; Macedo, T.A. Midterm Outcomes of a Prospective, Nonrandomized Study to Evaluate Endovascular Repair of Complex Aortic Aneurysms Using Fenestrated-Branched Endografts. Ann. Surg. 2021, 274, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Bellomo, R.; Ronco, C.; Kellum, J.A.; Mehta, R.L.; Palevsky, P. Acute renal failure-definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2004, 8, R204–R212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motta, F.; Crowner, J.R.; Kalbaugh, C.A.; Marston, W.A.; Pascarella, L.; McGinigle, K.L.; Kibbe, M.R.; Farber, M.A. Outcomes and complications after fenestrated-branched endovascular aortic repair. J. Vasc. Surg. 2019, 70, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, T.M.; Mastracci, T.M.; Carrell, T.; Constantinou, J.; Dias, N.; Katsargyris, A.; Modarai, B.; Resch, T.; Verhoeven, E.; Haulon, S. Mid-term Outcomes of Renal Branches Versus Renal Fenestrations for Thoraco-abdominal Aneurysm Repair. Eur. J. Soc. Vasc. Surg. 2016, 52, 141–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin-Gonzalez, T.; Pinçon, C.; Maurel, B.; Hertault, A.; Sobocinski, J.; Spear, R.; Le Roux, M.; Azzaoui, R.; Mastracci, T.M.; Haulon, S. Renal Outcomes Following Fenestrated and Branched Endografting. Eur. J. Soc. Vasc. Surg. 2015, 50, 420–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rastogi, V.; de Bruin, J.L.; Bouwens, E.; Hoeks, S.E.; Raa, S.T.; van Rijn, M.J.; Fioole, B.; Schermerhorn, M.L.; Verhagen, H.J. Incidence, Prognostic Significance, and Risk Factors of Acute Kidney Injury Following Elective Infrarenal and Complex Endovascular Aneurysm Repair. Eur. J. Soc. Vasc. Surg. 2022, 64, 621–629. [Google Scholar] [CrossRef] [PubMed]
- de Lachomette, M.F.; Della, N.; Maucort-Boulch, D.; Duprey, A.; Rosset, E.; Feugier, P.; Lermusiaux, P.; Albertini, J.-N.; Millon, A. Renal Function after Fenestrated or Branched Endovascular Aortic Repair: The Early Impairment Predictive Factors. Ann. Vasc. Surg. 2017, 40, 1–9. [Google Scholar] [CrossRef] [PubMed]
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am. J. Kidney Dis. 2002, 39 (Suppl. 1), S1–S266. [Google Scholar]
- Oderich, G.S.; Forbes, T.L.; Chaer, R.; Davies, M.G.; Lindsay, T.F.; Mastracci, T.; Singh, M.J.; Timaran, C.; Woo, E.Y. Reporting standards for endovascular aortic repair of aneurysms involving the renal-mesenteric arteries. J. Vasc. Surg. 2021, 73, 4S–52S. [Google Scholar] [CrossRef] [PubMed]
- Safi, H.J.; Winnerkvist, A.; Miller, C.C.; Iliopoulos, D.C.; Reardon, M.J.; Espada, R.; Baldwin, J.C. Effect of extended cross-clamp time during thoracoabdominal aortic aneurysm repair. Ann. Thorac. Surg. 1998, 66, 1204–1209. [Google Scholar] [CrossRef] [PubMed]
- Chaikof, E.L.; Fillinger, M.F.; Matsumura, J.S.; Rutherford, R.B.; White, G.H.; Blankensteijn, J.D.; Bernhard, V.M.; Harris, P.L.; Kent, K.; May, J.; et al. Identifying and grading factors that modify the outcome of endovascular aortic aneurysm repair. J. Vasc. Surg. 2002, 35, 1061–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Firth, D. Bias reduction of maximum likelihood estimates. Biometrika 1993, 80, 27–38. [Google Scholar] [CrossRef]
- Saratzis, A.N.; Bath, M.F.; Harrison, S.C.; Sayers, R.D.; Bown, M.J. Impact of Fenestrated Endovascular Abdominal Aortic Aneurysm Repair on Renal Function. J. Endovasc. Ther. 2015, 22, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Ftouh, S.; Thomas, M. Acute kidney injury: Summary of NICE guidance. BMJ 2013, 347, f4930. [Google Scholar] [CrossRef] [PubMed]
- D’Oria, M.; Wanhainen, A.; Lindström, D.; Tegler, G.; Mani, K. Editor’s Choice-Pre-Operative Moderate to Severe Chronic Kidney Disease is Associated with Worse Short-Term and Mid-Term Outcomes in Patients Undergoing Fenestrated-Branched Endovascular Aortic Repair. Eur. J. Vasc. Endovasc. Surg. 2021, 62, 859–868. [Google Scholar] [CrossRef] [PubMed]



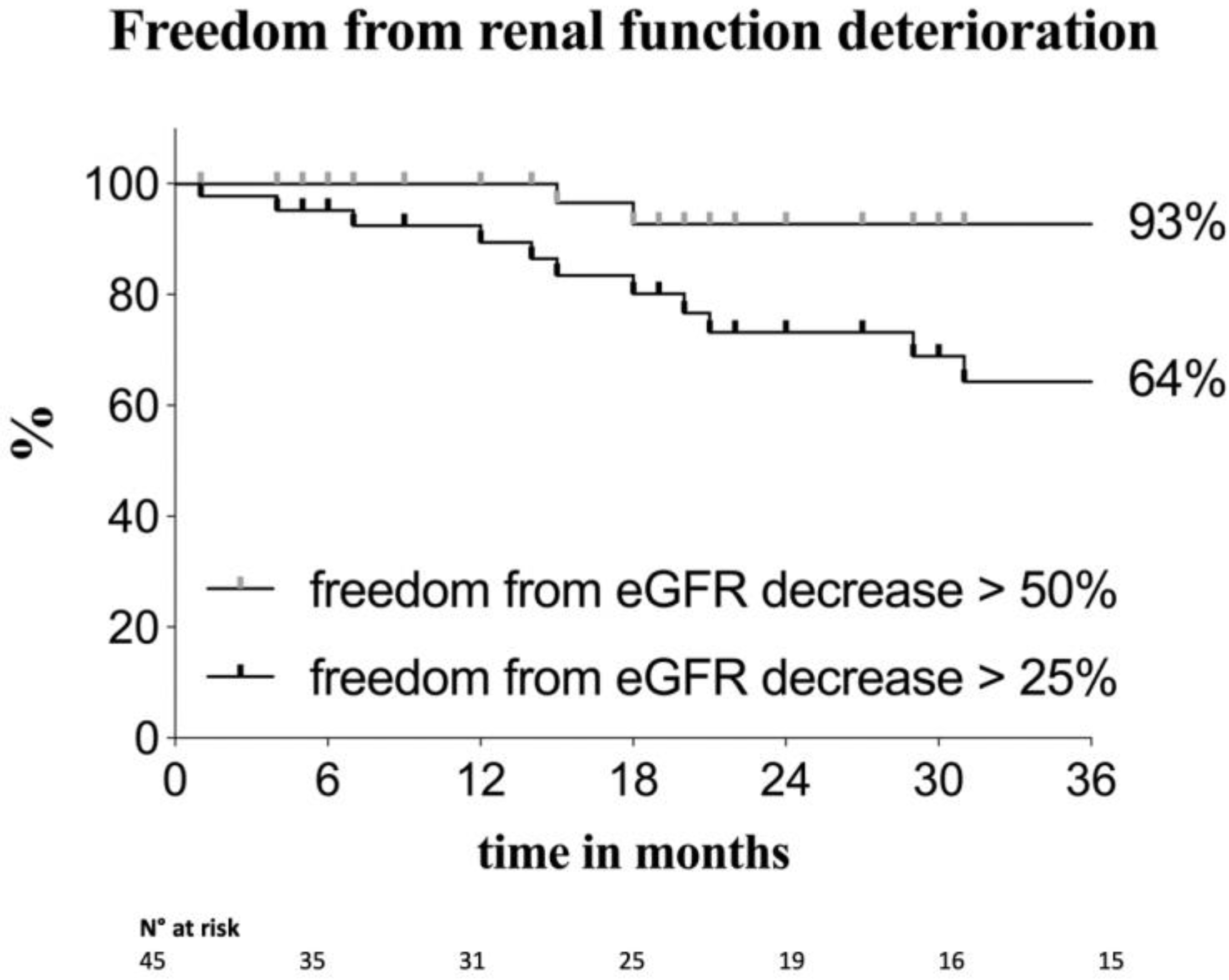{kind=link}
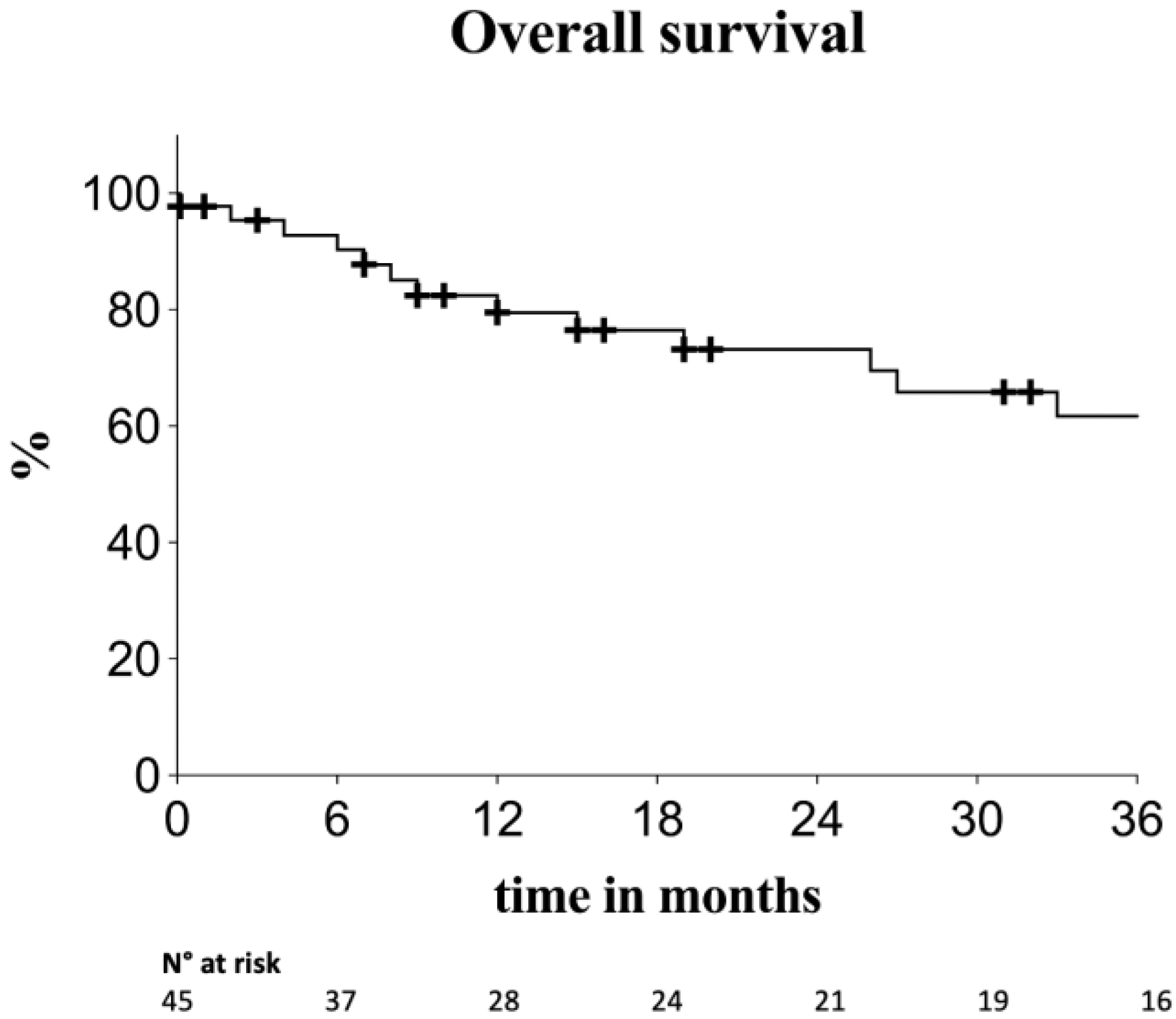{kind=link}
| Variable | 45 Patients N° (%), Mean ± SD, Median (IQR) |
|---|---|
| Age | 73.9 ± 6.1 |
| Male sex | 41 (91) |
| Cigarette smoking | |
| current | 13 (29) |
| past | 17 (38) |
| Arterial hypertension | 36 (80) |
| Dyslipidaemia | 26 (58) |
| Diabetes mellitus | 8 (18) |
| Chronic kidney disease (stage ≥ 3) | 13 (29) |
| Coronary artery disease | 23 (51) |
| Percutaneous revascularisation | 14 (31) |
| CABG | 8 (18) |
| COPD | 9 (20) |
| SVS total score | 0.9 ± 0.4 |
| ASA ≥ 3 | 38 (84) |
| Aneurysm diameter | 55.6 ± 11.3 |
| Aneurysm classification | |
| Juxtarenal | 26 (58) |
| Pararenal | 9 (20) |
| TAAA | 10 (22) a |
| Aetiology: atherosclerotic | 45 (100) |
| Multiple steps procedures | 7 (15) |
| Elective setting | 45 (100) |
| Main endograft type | |
| All fenestrations | 41 (91) |
| Mixed design b | 4 (9) |
| N° of fenestrations | |
| 1 | 1 (2) |
| 2 | 8 (18) |
| 3 | 16 (36) |
| 4 | 20 (44) |
| Brachial access | 13 (29) |
| Days of hospitalisation | 7.5 (4–17) |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Age (per year) | 0.98 (0.85–1.14) | 0.801 | ||
| Male sex | 0.09 (0.01–0.75) | 0.027 | 0.09 (0.001–1.16) | 0.064 |
| Arterial hypertension | 0.45 (0.05–5.22) | 0.475 | ||
| Diabetes mellitus | 1.85 (0.16–13.50) | 0.570 | ||
| COPD | 7.43 (1.20–53.36) | 0.031 | 2.32 (0.20–21.92) | 0.470 |
| CKD ≥ stage 3 | 0.76 (0.07–4.70) | 0.780 | ||
| PAAA or TAAA | 2.08 (0.36–13.70) | 0.405 | ||
| TAAA | 6.25 (1.03–43.97) | 0.046 | 2.009 (0.16–19.51) | 0.555 |
| Aneurysm diameter (per mm) | 1.05 (1.005–1.20) | 0.030 | 1.05 (0.97–1.43) | 0.188 |
| ≥3 fenestrations | 0.78 (0.12–8.58) | 0.814 | ||
| Endograft with only fenestrations | 1.35 (0.11–189.03) | 0.839 | ||
| Primary technical success | 0.19 (0.02–2.46) | 0.181 | ||
| Adjunctive procedures | 2.70 (0.23–19.96) | 0.377 | ||
| Days of hospitalisation | 1.01 (0.97–1.03) | 0.440 | ||
| Multiple step intervention | 1.76 (0.15–11.93) | 0.594 | ||
| Univariate | Multivariate | |||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age (per year) | 1.08 (0.98–1.20) | 0.100 | 1.16 (1.02–1.34) | 0.023 |
| Male sex | 0.47 (0.13–2.55) | 0.343 | ||
| PAAA or TAAA | 0.35 (0.10–1.0006) | 0.050 | 0.32 (0.08–1.09) | 0.071 |
| TAAA | 0.67 (0.13–2.24) | 0.548 | ||
| ≥3 fenestrations | 1.84 (0.58–6.87) | 0.306 | ||
| Endograft with only fenestrations | 1.33 (0.39–6.91) | 0.675 | ||
| Adjunctive procedures | 1.56 (0.30–5.33) | 0.545 | ||
| R-AKI | 1.36 (0.45–3.84) | 0.569 | ||
| I-AKI | 10.25 (2.21–43.73) | 0.004 | 26.82 (4.18–218.10) | <0.001 |
| Multiple step intervention | 2.62 (0.64–8.56) | 0.162 | 3.32 (0.72–12.81) | 0.113 |
| Renal artery occlusion a | 9.95 (0.99–54.02) | 0.050 | 29.87 (2.33–309.05) | 0.013 |
| Reinterventions a | 0.66 (0.07–2.77) | 0.615 | ||
| Multivariate | ||
|---|---|---|
| HR (95% CI) | p Value | |
| Preoperative CKD ≥ stage 3 | 5.68 (1.63–21.80) | 0.006 |
| Post-operative AKI (eGFR decline ≥ 50%) | 11.60 (1.70–97.51) | 0.012 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colacchio, E.C.; Berton, M.; Grego, F.; Piazza, M.; Menegolo, M.; Squizzato, F.; Antonello, M. Post-Operative and Mid-Term Renal Function Impairment Following Elective Fenestrated Endovascular Aortic Repair for Complex Aortic Aneurysms: Incidence and Risk Factors Analysis. Diagnostics 2023, 13, 1955. https://doi.org/10.3390/diagnostics13111955
Colacchio EC, Berton M, Grego F, Piazza M, Menegolo M, Squizzato F, Antonello M. Post-Operative and Mid-Term Renal Function Impairment Following Elective Fenestrated Endovascular Aortic Repair for Complex Aortic Aneurysms: Incidence and Risk Factors Analysis. Diagnostics. 2023; 13(11):1955. https://doi.org/10.3390/diagnostics13111955
Chicago/Turabian StyleColacchio, Elda Chiara, Mariagiovanna Berton, Franco Grego, Michele Piazza, Mirko Menegolo, Francesco Squizzato, and Michele Antonello. 2023. "Post-Operative and Mid-Term Renal Function Impairment Following Elective Fenestrated Endovascular Aortic Repair for Complex Aortic Aneurysms: Incidence and Risk Factors Analysis" Diagnostics 13, no. 11: 1955. https://doi.org/10.3390/diagnostics13111955