
Automatic Classification of Magnetic Resonance Histology of Peripheral Arterial Chronic Total Occlusions Using a Variational Autoencoder: A Feasibility Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Ultra-High Field Magnetic Resonance Imaging of Amputated Limbs
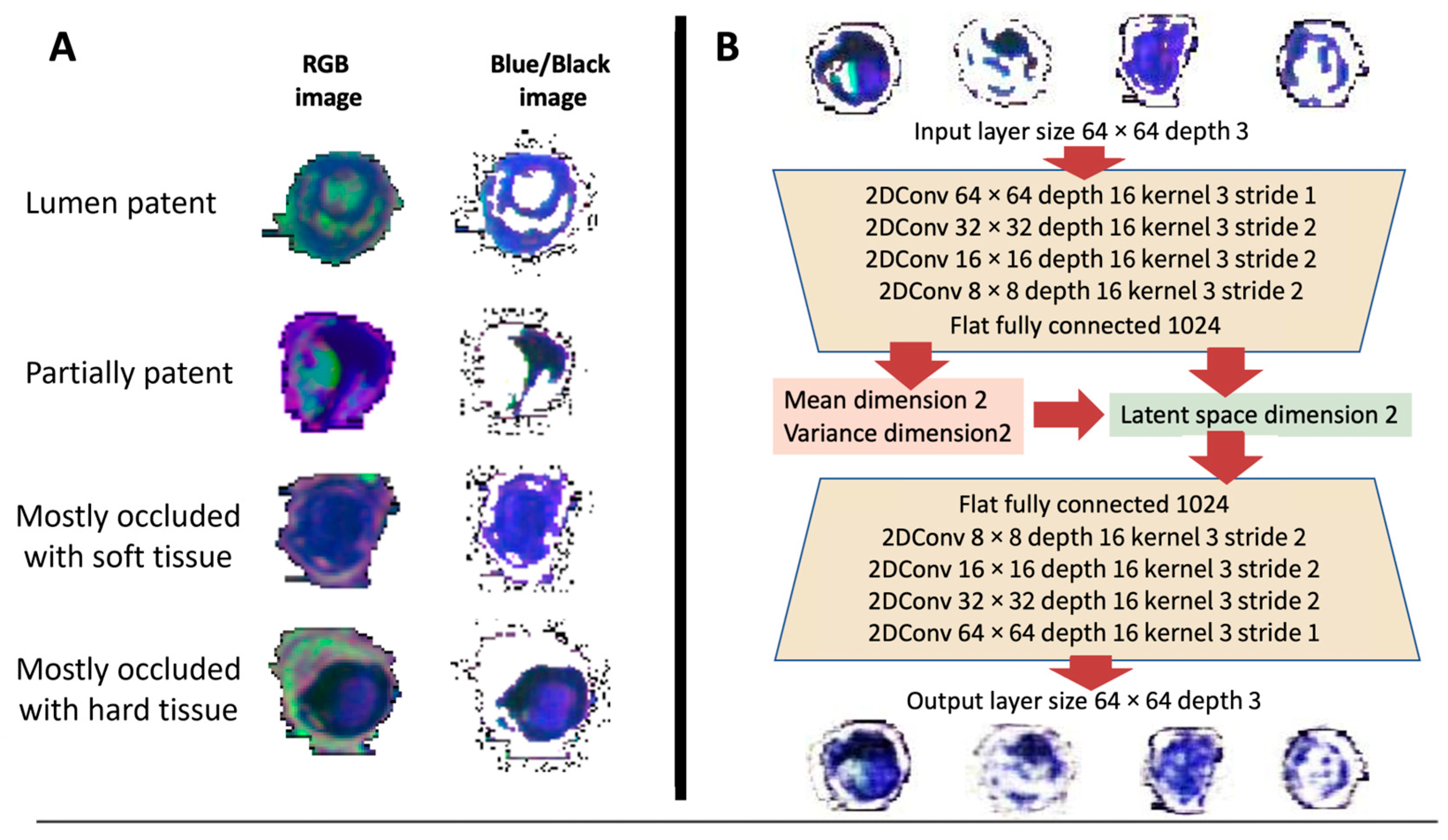
2.2. Image Preprocessing
2.3. Variational Autoencoder
2.4. Latent Space Classification and Tissue Scores
3. Results
3.1. Image Preprocessing
3.2. Variational Autoencoder
3.3. Tissue Scores
4. Discussion
4.1. Limitations
4.2. Novelties
- (1)
- We were able to extract a sufficient number of images for training a 2D CNN VAE algorithm from multi-contrast high-resolution MRI images of PAD lesions.
- (2)
- In our custom-made AI algorithm, we adapted the structure of the CNN layers to enable image reconstruction of multi-contrast MRI lesion tissue components.
- (3)
- The multi-contrast MRI lesion images were sorted into separate classes based on the presence or absence of hard tissue types, with corresponding tissue scores assigned.
- (4)
- The tissue scores were evaluated by visually assessing the pseudo-color multi-contrast MRI coronal images in a concurrent display.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bradbury, A.W.; Adam, D.J.; Bell, J.; Forbes, J.F.; Fowkes, F.G.R.; Gillespie, I.; Ruckley, C.V.; Raab, G.M. Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) trial: Analysis of amputation free and overall survival by treatment received. J. Vasc. Surg. 2010, 51, 18S–31S. [Google Scholar]
- Farber, A.; Menard, M.T.; Conte, M.S.; Kaufman, J.A.; Powell, R.J.; Choudhry, N.K.; Hamza, T.H.; Assmann, S.F.; Creager, M.A.; Cziraky, M.J.; et al. Surgery or Endovascular Therapy for Chronic Limb-Threatening Ischemia. N. Engl. J. Med. 2022, 387, 2305–2316. [Google Scholar] [CrossRef]
- Roy, T.L.; Chen, H.-J.; Dueck, A.D.; Wright, G.A. Magnetic resonance imaging characteristics of lesions relate to the difficulty of peripheral arterial endovascular procedures. J. Vasc. Surg. 2018, 67, 1844–1854.e2. [Google Scholar] [CrossRef] [PubMed]
- Conte, M.S.; Bradbury, A.W.; Kolh, P.; White, J.V.; Dick, F.; Fitridge, R.; Mills, J.I.; Ricco, J.-B.; Suresh, K.R.; Murad, M.H.; et al. Global vascular guidelines on the management of chronic limb-threatening ischemia. J. Vasc. Surg. 2019, 69, 3S–125S.e40. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Boujraf, S.; Bornstedt, A.; Hombach, V.; Ignatius, A.; Oberhuber, A.; Rasche, V. Quantification of Calcifications in Endarterectomy Samples by Means of High-Resolution Ultra-Short Echo Time Imaging. Investig. Radiol. 2010, 45, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, M.; Takehara, Y.; Fujisaki, K.; Okuaki, T.; Fukuma, Y.; Tooyama, N.; Ichijo, K.; Amano, T.; Goshima, S.; Naganawa, S. Three Dimensional Ultra-short Echo Time MRI Can Depict Cholesterol Components of Gallstones Bright. Magn. Reson. Med. Sci. 2021, 20, 359–370. [Google Scholar] [CrossRef]
- Yassin, A.; Pedrosa, I.; Kearney, M.; Genega, E.; Rofsky, N.M.; Lenkinski, R.E. In Vitro MR Imaging of Renal Stones with an Ultra-short Echo Time Magnetic Resonance Imaging Sequence. Acad. Radiol. 2012, 19, 1566–1572. [Google Scholar] [CrossRef]
- Finkenstaedt, T.; Biswas, R.; Abeydeera, N.A.; Siriwanarangsun, P.; Healey, R.; Statum, S.; Bae, W.C.; Chung, C.B. Ultrashort Time to Echo Magnetic Resonance Evaluation of Calcium Pyrophosphate Crystal Deposition in Human Menisci. Investig. Radiol. 2019, 54, 349–355. [Google Scholar] [CrossRef]
- Dou, W.; Mastrogiacomo, S.; Veltien, A.; Alghamdi, H.S.; Walboomers, X.F.; Heerschap, A. Visualization of calcium phosphate cement in teeth by zero echo time 1H MRI at high field. NMR Biomed. 2018, 31, e3859. [Google Scholar] [CrossRef]
- Siu, A.G.; Ramadeen, A.; Hu, X.; Morikawa, L.; Zhang, L.; Lau, J.Y.C.; Liu, G.; Pop, M.; Connelly, K.A.; Dorian, P.; et al. Characterization of the ultrashort-TE (UTE) MR collagen signal. NMR Biomed. 2015, 28, 1236–1244. [Google Scholar] [CrossRef]
- Roy, T.; Liu, G.; Shaikh, N.; Dueck, A.D.; Wright, G.A. Puncturing Plaques. J. Endovasc. Ther. Off. J. Int. Soc. Endovasc. Spec. 2017, 24, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Gore, J.C. Artificial intelligence in medical imaging. Magn. Reson. Imaging 2020, 68, A1–A4. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.Q.; Wang, J.Y.; Yu, S.Y.; Wu, G.G.; Wei, Q.; Deng, Y.B.; Wu, X.L.; Cui, X.W.; Dietrich, C.F. Artificial intelligence in medical imaging of the liver. World J. Gastroenterol. 2019, 25, 672–682. [Google Scholar] [CrossRef] [PubMed]
- Chassagnon, G.; Vakalopoulou, M.; Paragios, N.; Revel, M.-P. Artificial intelligence applications for thoracic imaging. Eur. J. Radiol. 2020, 123, 108774. [Google Scholar] [CrossRef]
- Le, E.; Wang, Y.; Huang, Y.; Hickman, S.; Gilbert, F. Artificial intelligence in breast imaging. Clin. Radiol. 2019, 74, 357–366. [Google Scholar] [CrossRef]
- Currie, G.; Hawk, K.E.; Rohren, E.; Vial, A.; Klein, R. Machine Learning and Deep Learning in Medical Imaging: Intelligent Imaging. J. Med. Imaging Radiat. Sci. 2019, 50, 477–487. [Google Scholar] [CrossRef]
- Nensa, F.; Demircioglu, A.; Rischpler, C. Artificial Intelligence in Nuclear Medicine. J. Nucl. Med. 2019, 60 (Suppl. S2), 29S–37S. [Google Scholar] [CrossRef]
- Wagner, J.B. Artificial Intelligence in Medical Imaging. Radiol. Technol. 2019, 90, 489–501. [Google Scholar]
- Seah, J.; Brady, Z.; Ewert, K.; Law, M. Artificial intelligence in medical imaging: Implications for patient radiation safety. Br. J. Radiol. 2021, 94, 20210406. [Google Scholar] [CrossRef]
- Shen, Y.-T.; Chen, L.; Yue, W.-W.; Xu, H.-X. Artificial intelligence in ultrasound. Eur. J. Radiol. 2021, 139, 109717. [Google Scholar] [CrossRef]
- Chen, X.; Huo, X.; Wu, Z.; Lu, J. Advances of Artificial Intelligence Application in Medical Imaging of Ovarian Cancers. Chin. Med. Sci. J. 2021, 36, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Streiner, D.L.; Saboury, B.; Zukotynski, K.A. Evidence-Based Artificial Intelligence in Medical Imaging. PET Clin. 2022, 17, 51–55. [Google Scholar] [CrossRef]
- Singh, A.; Ogunfunmi, T. An Overview of Variational Autoencoders for Source Separation, Finance, and Bio-Signal Applications. Entropy 2021, 24, 55. [Google Scholar] [CrossRef] [PubMed]
- Marino, J. Predictive Coding, Variational Autoencoders, and Biological Connections. Neural Comput. 2021, 34, 1–44. [Google Scholar] [CrossRef]
- Ye, F.; Bors, A.G. Lifelong Mixture of Variational Autoencoders. IEEE Trans. Neural Netw. Learn. Syst. 2021, 34, 461–474. [Google Scholar] [CrossRef]
- Gomari, D.P.; Schweickart, A.; Cerchietti, L.; Paietta, E.; Fernandez, H.; Al-Amin, H.; Suhre, K.; Krumsiek, J. Variational autoencoders learn transferrable representations of metabolomics data. Commun. Biol. 2022, 5, 645. [Google Scholar] [CrossRef] [PubMed]
- Barrejon, D.; Olmos, P.M.; Artes-Rodriguez, A. Medical Data Wrangling with Sequential Variational Autoencoders. IEEE J. Biomed. Health Informatics 2022, 26, 2737–2745. [Google Scholar] [CrossRef]
- Perl, Y.S.; Bocaccio, H.; Pérez-Ipiña, I.; Zamberlán, F.; Piccinini, J.; Laufs, H.; Kringelbach, M.; Deco, G.; Tagliazucchi, E. Generative Embeddings of Brain Collective Dynamics Using Variational Autoencoders. Phys. Rev. Lett. 2020, 125, 238101. [Google Scholar] [CrossRef]
- Baucum, M.; Khojandi, A.; Vasudevan, R. Improving Deep Reinforcement Learning with Transitional Variational Autoencoders: A Healthcare Application. IEEE J. Biomed. Health Inform. 2021, 25, 2273–2280. [Google Scholar] [CrossRef]
- Uzunova, H.; Schultz, S.; Handels, H.; Ehrhardt, J. Unsupervised pathology detection in medical images using conditional variational autoencoders. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 451–461. [Google Scholar] [CrossRef]
- Edupuganti, V.; Mardani, M.; Vasanawala, S.; Pauly, J. Uncertainty Quantification in Deep MRI Reconstruction. IEEE Trans. Med. Imaging 2021, 40, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Everett, R.; Flores, K.B.; Henscheid, N.; Lagergren, J.; Larripa, K.; Li, D.; Nardini, J.T.; Nguyen, P.T.T.; Pitman, E.B.; Rutter, E.M. A tutorial review of mathematical techniques for quantifying tumor heterogeneity. Math. Biosci. Eng. 2020, 17, 3660–3709. [Google Scholar] [CrossRef]
- Ahmad, B.; Sun, J.; You, Q.; Palade, V.; Mao, Z. Brain Tumor Classification Using a Combination of Variational Autoencoders and Generative Adversarial Networks. Biomedicines 2022, 10, 223. [Google Scholar] [CrossRef] [PubMed]
- Tschuchnig, M.E.; Zillner, D.; Romanelli, P.; Hercher, D.; Heimel, P.; Oostingh, G.J.; Couillard-Després, S.; Gadermayr, M. Quantification of anomalies in rats’ spinal cords using autoencoders. Comput. Biol. Med. 2021, 138, 104939. [Google Scholar] [CrossRef]
- Baur, C.; Denner, S.; Wiestler, B.; Navab, N.; Albarqouni, S. Autoencoders for unsupervised anomaly segmentation in brain MR images: A comparative study. Med. Image Anal. 2021, 69, 101952. [Google Scholar] [CrossRef] [PubMed]
- Nakao, T.; Hanaoka, S.; Nomura, Y.; Murata, M.; Takenaga, T.; Miki, S.; Watadani, T.; Yoshikawa, T.; Hayashi, N.; Abe, O. Unsupervised Deep Anomaly Detection in Chest Radiographs. J. Digit. Imaging 2021, 34, 418–427. [Google Scholar] [CrossRef]
- Pinaya, W.H.; Tudosiu, P.-D.; Gray, R.; Rees, G.; Nachev, P.; Ourselin, S.; Cardoso, M.J. Unsupervised brain imaging 3D anomaly detection and segmentation with transformers. Med. Image Anal. 2022, 79, 102475. [Google Scholar] [CrossRef]
- Geenjaar, E.; Lewis, N.; Fu, Z.; Venkatdas, R.; Plis, S.; Calhoun, V. Fusing multimodal neuroimaging data with a variational autoencoder. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2021, 2021, 3630–3633. [Google Scholar] [CrossRef] [PubMed]
- Guleria, H.V.; Luqmani, A.M.; Kothari, H.D.; Phukan, P.; Patil, S.; Pareek, P.; Kotecha, K.; Abraham, A.; Gabralla, L.A. Enhancing the Breast Histopathology Image Analysis for Cancer Detection Using Variational Autoencoder. Int. J. Environ. Res. Public Health 2023, 20, 4244. [Google Scholar] [CrossRef]
- Balaji, K. Image Augmentation based on Variational Autoencoder for Breast Tumor Segmentation. Acad. Radiol. 2023, 15. [Google Scholar] [CrossRef]
- Chatterjee, S.; Maity, S.; Bhattacharjee, M.; Banerjee, S.; Das, A.K.; Ding, W. Variational Autoencoder Based Imbalanced COVID-19 Detection Using Chest X-Ray Images. New Gener. Comput. 2023, 41, 25–60. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Wang, S.; Zhang, X.; Zhang, Y.-D. WVALE: Weak variational autoencoder for localisation and enhancement of COVID-19 lung infections. Comput. Methods Programs Biomed. 2022, 221, 106883. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Sciarra, A.; Dünnwald, M.; Tummala, P.; Agrawal, S.K.; Jauhari, A.; Kalra, A.; Oeltze-Jafra, S.; Speck, O.; Nürnberger, A. StRegA: Unsupervised anomaly detection in brain MRIs using a compact context-encoding variational autoencoder. Comput. Biol. Med. 2022, 149, 106093. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Tan, Y. Semisupervised Text Classification by Variational Autoencoder. IEEE Trans. Neural. Netw. Learn. Syst. 2020, 31, 295–308. [Google Scholar] [CrossRef]
- Chen, J.; Du, L.; Liao, L. Discriminative Mixture Variational Autoencoder for Semisupervised Classification. IEEE Trans. Cybern. 2022, 52, 3032–3046. [Google Scholar] [CrossRef]
- Harefa, E.; Zhou, W. Performing sequential forward selection and variational autoencoder techniques in soil classification based on laser-induced breakdown spectroscopy. Anal. Methods 2021, 13, 4926–4933. [Google Scholar] [CrossRef]
- Mansour, R.F.; Escorcia-Gutierrez, J.; Gamarra, M.; Gupta, D.; Castillo, O.; Kumar, S. Unsupervised Deep Learning based Variational Autoencoder Model for COVID-19 Diagnosis and Classification. Pattern Recognit. Lett. 2021, 151, 267–274. [Google Scholar] [CrossRef]
- Yang, Y.; Zheng, K.; Wu, C.; Yang, Y. Improving the Classification Effectiveness of Intrusion Detection by Using Improved Conditional Variational AutoEncoder and Deep Neural Network. Sensors 2019, 19, 2528. [Google Scholar] [CrossRef]
- Way, G.P.; Greene, C.S. Extracting a biologically relevant latent space from cancer transcriptomes with variational autoencoders. Pac. Symp. Biocomput. 2018, 23, 80–91. [Google Scholar]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef]
- Schneider, C.A.; Rasband, W.S.; Eliceiri, K.W. NIH Image to ImageJ: 25 Years of image analysis. Nat. Methods 2012, 9, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Rocha-Singh, K.J.; Zeller, T.; Jaff, M.R. Peripheral arterial calcification: Prevalence, mechanism, detection, and clinical implications. Catheter. Cardiovasc. Interv. 2014, 83, E212–E220. [Google Scholar] [CrossRef] [PubMed]
- Fanelli, F.; Cannavale, A.; Gazzetti, M.; Lucatelli, P.; Wlderk, A.; Cirelli, C.; D’adamo, A.; Salvatori, F.M. Calcium Burden Assessment and Impact on Drug-Eluting Balloons in Peripheral Arterial Disease. Cardiovasc. Interv. Radiol. 2014, 37, 898–907. [Google Scholar] [CrossRef] [PubMed]
- Mohebali, J.; Patel, V.I.; Romero, J.M.; Hannon, K.M.; Jaff, M.R.; Cambria, R.P.; LaMuraglia, G.M. Acoustic shadowing impairs accurate characterization of stenosis in carotid ultrasound examinations. J. Vasc. Surg. 2015, 62, 1236–1244. [Google Scholar] [CrossRef]
- Roy, T.; Forbes, T.; Wright, G.; Dueck, A. Burning Bridges: Mechanisms and Implications of Endovascular Failure in the Treatment of Peripheral Artery Disease. J. Endovasc. Ther. 2015, 22, 874–880. [Google Scholar] [CrossRef]
- Roy, T.L.; Forbes, T.L.; Dueck, A.D.; Wright, G.A. MRI for peripheral artery disease: Introductory physics for vascular physicians. Vasc. Med. 2018, 23, 153–162. [Google Scholar] [CrossRef]
- Edelman, R.R.; Flanagan, O.; Grodzki, D.; Giri, S.; Gupta, N.; Koktzoglou, I. Projection MR imaging of peripheral arterial calcifications: Projection MR Imaging of Peripheral Arterial Calcifications. Magn. Reson. Med. 2015, 73, 1939–1945. [Google Scholar] [CrossRef]
- Karolyi, M.; Seifarth, H.; Liew, G.; Schlett, C.L.; Maurovich-Horvat, P.; Dai, G.; Huang, S.; Goergen, C.J.; Hoffmann, U.; Sosnovik, D.E. Classification of human coronary atherosclerotic plaques with T1, T2 and Ultrashort TE MRI. J. Cardiovasc. Magn. Reson. 2012, 14, P135, 1532–429X-14-S1-P135. [Google Scholar] [CrossRef]
- Saba, L.; Sanagala, S.S.; Gupta, S.K.; Koppula, V.K.; Johri, A.M.; Khanna, N.N.; Mavrogeni, S.; Laird, J.R.; Pareek, G.; Miner, M.; et al. Multimodality carotid plaque tissue characterization and classification in the artificial intelligence paradigm: A narrative review for stroke application. Ann. Transl. Med. 2021, 9, 1206. [Google Scholar] [CrossRef]
- Lanzafame, L.R.M.; Bucolo, G.M.; Muscogiuri, G.; Sironi, S.; Gaeta, M.; Ascenti, G.; Booz, C.; Vogl, T.J.; Blandino, A.; Mazziotti, S.; et al. Artificial Intelligence in Cardiovascular CT and MR Imaging. Life 2023, 13, 507. [Google Scholar] [CrossRef]
- Azeez, M.; Laivuori, M.; Tolva, J.; Linder, N.; Lundin, J.; Albäck, A.; Venermo, M.; Mäyränpää, M.I.; Lokki, M.L.; Lokki, A.I.; et al. High relative amount of nodular calcification in femoral plaques is associated with milder lower extremity arterial disease. BMC Cardiovasc. Disord. 2022, 22, 563. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Sample Number | Tissue Class I (%) | Tissue Class II (%) | Tissue Class III (%) | Tissue Class IV (%) |
|---|---|---|---|---|
| #1 | 100 | 0 | 0 | 0 |
| #2 | 4.2 | 75.9 | 19.9 | 0 |
| #3 | 9.8 | 72.2 | 18 | 0 |
| #4 | 0.2 | 46.3 | 33.5 | 20 |
| #5 | 5.8 | 69.6 | 24.7 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Csore, J.; Karmonik, C.; Wilhoit, K.; Buckner, L.; Roy, T.L. Automatic Classification of Magnetic Resonance Histology of Peripheral Arterial Chronic Total Occlusions Using a Variational Autoencoder: A Feasibility Study. Diagnostics 2023, 13, 1925. https://doi.org/10.3390/diagnostics13111925
Csore J, Karmonik C, Wilhoit K, Buckner L, Roy TL. Automatic Classification of Magnetic Resonance Histology of Peripheral Arterial Chronic Total Occlusions Using a Variational Autoencoder: A Feasibility Study. Diagnostics. 2023; 13(11):1925. https://doi.org/10.3390/diagnostics13111925
Chicago/Turabian StyleCsore, Judit, Christof Karmonik, Kayla Wilhoit, Lily Buckner, and Trisha L. Roy. 2023. "Automatic Classification of Magnetic Resonance Histology of Peripheral Arterial Chronic Total Occlusions Using a Variational Autoencoder: A Feasibility Study" Diagnostics 13, no. 11: 1925. https://doi.org/10.3390/diagnostics13111925