

Scan Aided Dental Arch Width Prediction via Internationally Recognized Formulas and Indices in a Sample of Kurdish Population/Iraq
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Registration
2.2. Sample
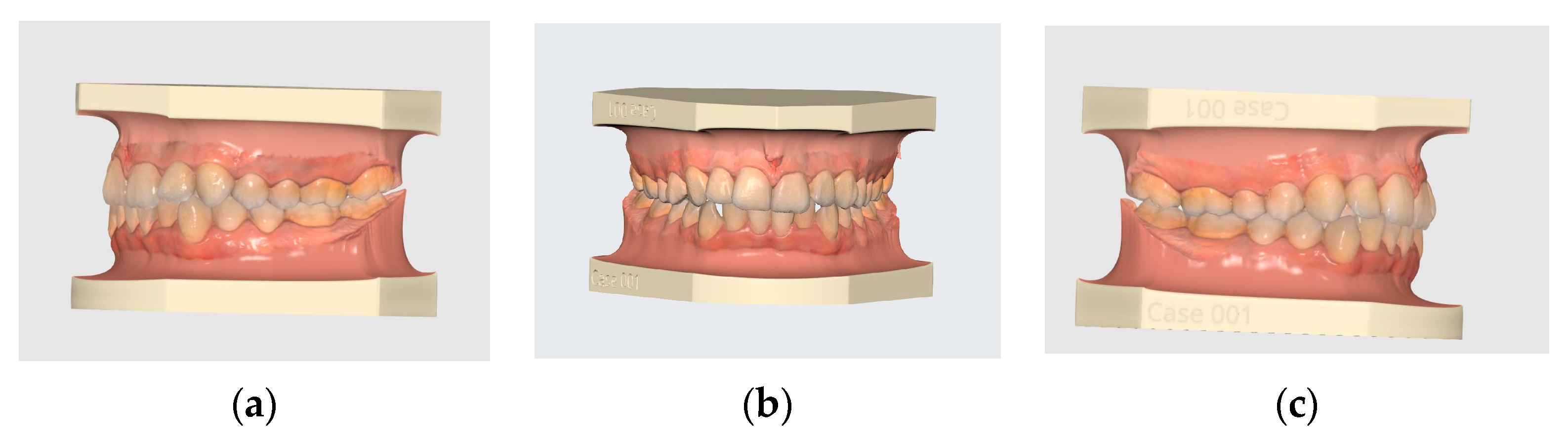
- Permanent dentition, class I skeletal and dental relationships, with normal overbite and overjet.
- Patients’ age is between (18–30) years old.
- No caries, no attrition, no crossbite, and no crowding of more than 3 mm.
- No systemic disease, no facial asymmetry, and no congenital disorders.
- No trauma and no patients under orthodontic treatment.
- Participants signed a consent form after being contacted via their registered mobile number.
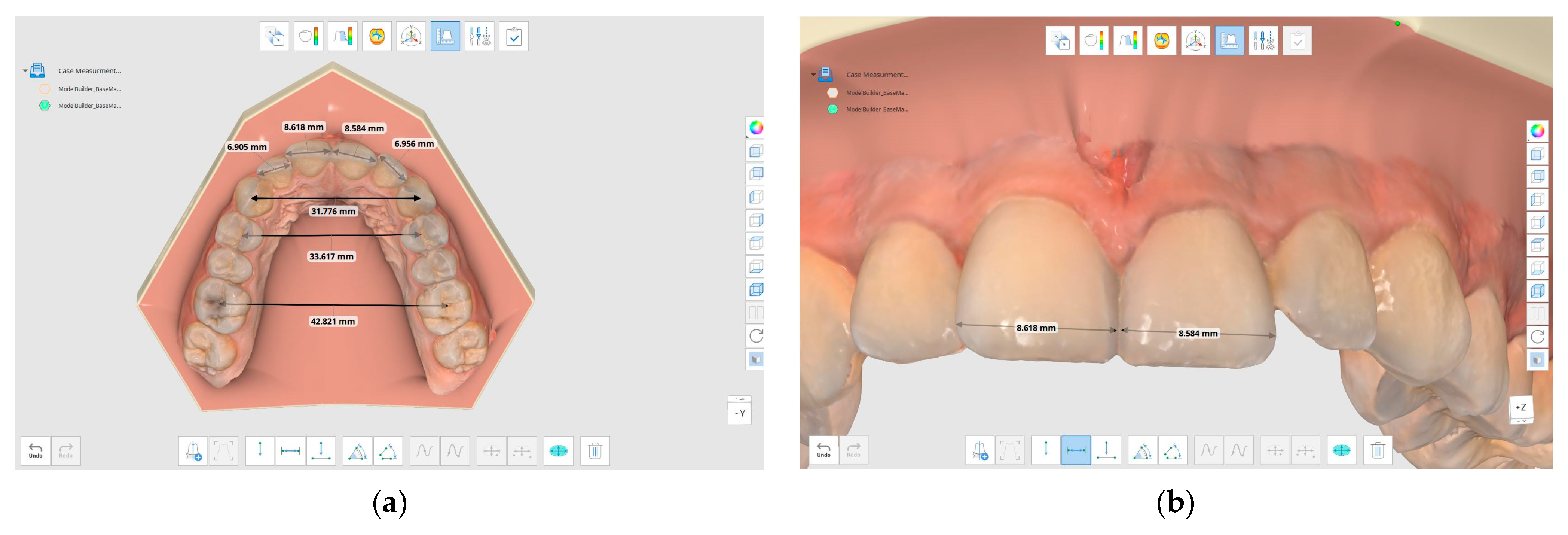
- Anterior Arch Width (AAW): the millimeter distance between the cusp tips of the canines.
- Inter-premolar width (IPW): the millimeter distance between the distal pits of the maxillary first premolars.
- Inter-molar width (IMW): the millimeter distance between the central fossae of the maxillary first molars.
- Mesiodistal dimension of permanent upper incisors (SUI).
2.3. Statistical Analysis
3. Results
3.1. Sample
3.2. Pont’s Index Reliability
4. Discussion
- New IMW
- 2.
- New IPW
- 3.
- New AAW
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aksu, M.; Kocadereli, I. Arch width changes in extraction and non-extraction treatment in class I patients. Angle Orthod. 2005, 75, 948–952. [Google Scholar] [PubMed]
- Kahl-Nieke, B.; Fischbach, H.; Schwarz, C.W. Treatment and post retention changes in dental arch width dimensions a long-term evaluation of influencing cofactors. Am. J. Orthod. 1996, 109, 368–378. [Google Scholar] [CrossRef] [PubMed]
- Stifter, J. A study of Pont’s, Howes’ Rees’ Neff’s and Bolton’s analyses on Class I adult dentitions. Angle Orthod. 1958, 28, 215–225. [Google Scholar]
- Rees, D.J. A method for assessing the proportional relation of apical bases and contact diameters of the teeth. Am. J. Orthod. 1953, 39, 695–707. [Google Scholar] [CrossRef]
- Pont, A. Der Zahn-index in der orthodontie. Zahnarztuche Orthop. 1909, 3, 306–321. [Google Scholar]
- Al-Omari, I.K.; Duaibis, R.B.; Al-Bitar, Z.B. Application of Pont’s Index to a Jordanian population. Eur. J. Orthod. 2007, 29, 627–631. [Google Scholar] [CrossRef]
- Dhakal, J.; Shrestha, R.M.; Pyakurel, U. Assessment of Validity of Pont’s Index and Establishment of Regression Equation to Predict Arch Width in Nepalese Sample. Orthod. J. 2014, 4, 12–16. [Google Scholar] [CrossRef]
- Lohakare, S. Application of Pont’s Index to Gujrati Population. J. Med. Sci. Clin. Res. 2018, 6, 171–178. [Google Scholar] [CrossRef]
- Dalidjan, M.; Sampson, W.; Townsend, G. Prediction of dental arch development: An assessment of Pont’s Index in three human populations. Am. J. Orthod. Dentofac. Orthop. 1995, 107, 465–475. [Google Scholar] [CrossRef]
- Rykman, A.; Smailiene, D. Application of Pont’s Index to Lithuanian Individuals: A Pilot Study. J. Oral Maxillofac. Res. 2015, 6, e4. [Google Scholar] [CrossRef]
- Celebi, A.A.; Tan, E.; Gelgor, I.E. Determination and application of Pont’s index in Turkish population. Sci. World J. 2012, 2012, 494623. [Google Scholar] [CrossRef]
- Ordoubazary, M.; Zafarmand, A.H.; Madani, A.; Ordoubazary, A. Comparison of Pont’s and Korkhaus indices at different populations. Ellenike Orthod. Ep. 2007, 10, 67. [Google Scholar]
- Lombardo, L.; Coppola, P.; Siciliani, G. Comparison of dental and alveolar arch forms between different ethnic groups. Int. Orthod. 2015, 13, 462–488. [Google Scholar] [CrossRef]
- Khan, S.H.; Hasan, N.; Anjum, S.; Rafique, T. Is there is any relationship between malocclusion and nutritional pattern of children. Update Dent. Coll. J. 2015, 4, 9–13. [Google Scholar] [CrossRef]
- Rahmawati, A.D.; Sudarso, I.S.R.; Pramono, D.; Arguni, E. Correlation between age and dental arch dimension of Javanese children. Dent. J. (Majalah Kedokt. Gigi) 2020, 53, 93–98. [Google Scholar] [CrossRef]
- Rakosi, T.; Jonas, I.; Graber, T.M. Study cast analysis. In Color Atlas of Dental Medicine-Orthodontic Diagnosis, 1st ed.; Thieme Medical Publishers Inc.: New York, NY, USA, 1993; pp. 207–234. [Google Scholar]
- Joondeph, D.R.; Riedel, R.A.; Moore, A.W. Pont’s index: A clinical evaluation. Angle Orthod. 1970, 40, 112–118. [Google Scholar]
- McNamara, J. Treatment of Children in the Mixed Dentition, 3rd ed.; Graber, T.M., Vanarsdall, R.L., Eds.; Orthodontics Current Principles and Techniques; Elsevier: Amsterdam, The Netherlands, 2000; pp. 525–526. [Google Scholar]
- Jehan, S.; Iftikhar, A.; Fayyaz, R. Assessment of accuracy and reliability of Pont’s index in different classes of dental malocclusion. Pak. Orthod. J. 2021, 13, 72–76. [Google Scholar]
- Kim, Y.-K.; Kim, S.-H.; Choi, T.-H.; Yen, E.H.; Zou, B.; Shin, Y.; Lee, N.-K. Accuracy of intraoral scan images in full arch with orthodontic brackets: A retrospective in vivo study. Clin. Oral Investig. 2021, 25, 4861–4869. [Google Scholar] [CrossRef]
- Christopoulou, I.; Kaklamanos, E.G.; Makrygiannakis, M.A.; Bitsanis, I.; Perlea, P.; Tsolakis, A.I. Intraoral Scanners in Orthodontics: A Critical Review. Int. J. Environ. Res. Public Health 2022, 19, 1407. [Google Scholar] [CrossRef]
- Thu, K.M.; Winn, T.; Abdullah, N.; Jayasinghe, J.A.P.; Chandima, G.L. The maxillary arch and its relationship to cephalometric landmarks of selected malay ethnic group. Malays. J. Med. Sci. 2005, 12, 29–38. [Google Scholar]
- Mangano, A.; Beretta, M.; Luongo, G.; Mangano, C.; Mangano, F. Conventional vs. Digital Impressions: Acceptability, Treatment Comfort and Stress Among Young Orthodontic Patients. Open Dent. J. 2018, 12, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Gayathri, M.; Arun, A.V.; Lalitha, P. Arch width in normal occlusion, crowding, and spacing. Drug Invent. Today 2020, 13, 107–109. [Google Scholar]
- Rathi, M.K.; Fida, M. Applicability of Pont’s Index in Orthodontics. J. Coll. Physicians Surg. Pak. 2014, 24, 256–260. [Google Scholar] [PubMed]
- Shahid, F.; Alam, M.K.; Khamis, M.F. New prediction equations for the estimation of maxillary mandibular canine and premolar widths from mandibular incisors and mandibular first permanent molar widths: A digital model study. Korean J. Orthod. 2016, 46, 171–179. [Google Scholar] [CrossRef]
- Dasgupta, M.; Roy, B.K.; Bora, G.R.H.; Bharali, T. Relationship between dental arch width and vertical facial morphology in multiethnic assamese adults. Indian J. Oral Health Res. 2021, 7, 26. [Google Scholar] [CrossRef]
- Feştilă, D.; Enache, A.M.; Nagy, E.B.; Hedeşiu, M.; Ghergie, M. Testing the Accuracy of Pont’s Index in Diagnosing Maxillary Transverse Discrepancy as Compared to the University of Pennsylvania CBCT Analysis. Dent. J. 2022, 10, 23. [Google Scholar] [CrossRef]
- Hidayati, H.; Sari, D.P. Estimation of New Equation for Triangle Anterior Dental Arch Form in Sub-Race Deutro Malay. In Proceedings of the 1st International Conference on Health Sciences and Biotechnology (ICHB 2021), virtual, 3–4 November 2021; Atlantis Press: Paris, France, 2022; pp. 192–194. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| N | Min | Max | Mean | Std. Dev | ||
|---|---|---|---|---|---|---|
| Real | IMW | 100 | 40.12 | 53.53 | 45.42 | 2.87 |
| IPW | 100 | 29.20 | 41.70 | 35.78 | 2.50 | |
| AAW | 100 | 27.45 | 40.00 | 33.65 | 2.48 | |
| Pont’s | PIM | 100 | 41.05 | 52.48 | 47.83 | 2.85 |
| PIP | 100 | 33.35 | 42.64 | 38.87 | 2.32 | |
| PAW | 100 | 31.39 | 40.13 | 36.58 | 2.18 | |
| N | Correlation | Sig. | ||
|---|---|---|---|---|
| Pair 1 | IMW and PIM | 100 | 0.326 | 0.001 * |
| Pair 2 | IPW and PIP | 100 | 0.315 | 0.001 * |
| Pair 3 | AAW and PAW | 100 | 0.518 | 0.000 * |
| Real IMW | SUI | Real IPW | SUI | Real AAW | SUI | ||
|---|---|---|---|---|---|---|---|
| Pearson Correlation | IMW | 1.000 | 0.326 | 1.000 | 0.315 | 1.000 | 0.518 |
| SUI | 0.326 | 1.000 | 0.315 | 1.000 | 0.518 | 1.000 | |
| Sig. (1-tailed) | IMW, IPW, AAW | 0.000 | 0.001 | 0.000 | |||
| SUI | 0.000 | 0.001 | 0.000 | ||||
| N | IMW | 100 | 100 | 100 | 100 | 100 | 100 |
| SUI | 100 | 100 | 100 | 100 | 100 | 100 | |
| Model | Sum of Squares | df | Mean Square | F | Sig. | |
|---|---|---|---|---|---|---|
| IMW (Dependent variable) | Regression | 86.575 | 1 | 86.575 | 11.661 | 0.001 b |
| Residual | 727.599 | 98 | 7.424 | |||
| Total | 814.174 | 99 | ||||
| IPW (Dependent variable) | Regression | 61.696 | 1 | 61.696 | 10.821 | 0.001 b |
| Residual | 558.738 | 98 | 5.701 | |||
| Total | 620.434 | 99 | ||||
| AAW (Dependent variable) | Regression | 162.975 | 1 | 162.975 | 35.939 | 0.000 b |
| Residual | 444.411 | 98 | 4.535 | |||
| Total | 607.386 | 99 | ||||
| Mean | Std. Deviation | Std. Error Mean | 95% Confidence Interval of the Difference | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||||
| Pair1 | IMW-PMW | −2.41 | 3.32 | 0.33 | −3.07 | −1.75 | −7.26 | 99 | 0.000 |
| Pair2 | IMW-New IMW | 0.15 | 2.71 | 0.27 | −0.39 | 0.68 | 0.54 | 99 | 0.589 * |
| Pair1 | IPW-PIP | −3.08 | 2.82 | 0.28 | −3.64 | −2.52 | −10.92 | 99 | 0.000 |
| Pair2 | IPW-New PIP | −0.12 | 2.38 | 0.24 | −0.59 | 0.36 | −0.49 | 99 | 0.625 * |
| Pair1 | AAW-PAW | −2.92 | 2.30 | 0.23 | −3.38 | −2.47 | −12.71 | 99 | 0.000 |
| Pair2 | AAW-New AAW | 0.081 | 2.12 | 0.21 | −0.339 | 0.50 | 0.38 | 99 | 0.704 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahmood, T.M.A.; Noori, A.J.; Aziz, Z.H.; Rauf, A.M.; Kareem, F.A. Scan Aided Dental Arch Width Prediction via Internationally Recognized Formulas and Indices in a Sample of Kurdish Population/Iraq. Diagnostics 2023, 13, 1900. https://doi.org/10.3390/diagnostics13111900
Mahmood TMA, Noori AJ, Aziz ZH, Rauf AM, Kareem FA. Scan Aided Dental Arch Width Prediction via Internationally Recognized Formulas and Indices in a Sample of Kurdish Population/Iraq. Diagnostics. 2023; 13(11):1900. https://doi.org/10.3390/diagnostics13111900
Chicago/Turabian StyleMahmood, Trefa Mohammed Ali, Arass Jalal Noori, Zana Hussein Aziz, Aras Maruf Rauf, and Fadil Abdulla Kareem. 2023. "Scan Aided Dental Arch Width Prediction via Internationally Recognized Formulas and Indices in a Sample of Kurdish Population/Iraq" Diagnostics 13, no. 11: 1900. https://doi.org/10.3390/diagnostics13111900