


Contemporary Review of Multimodality Imaging of the Prostate Gland
 , , and
, , and 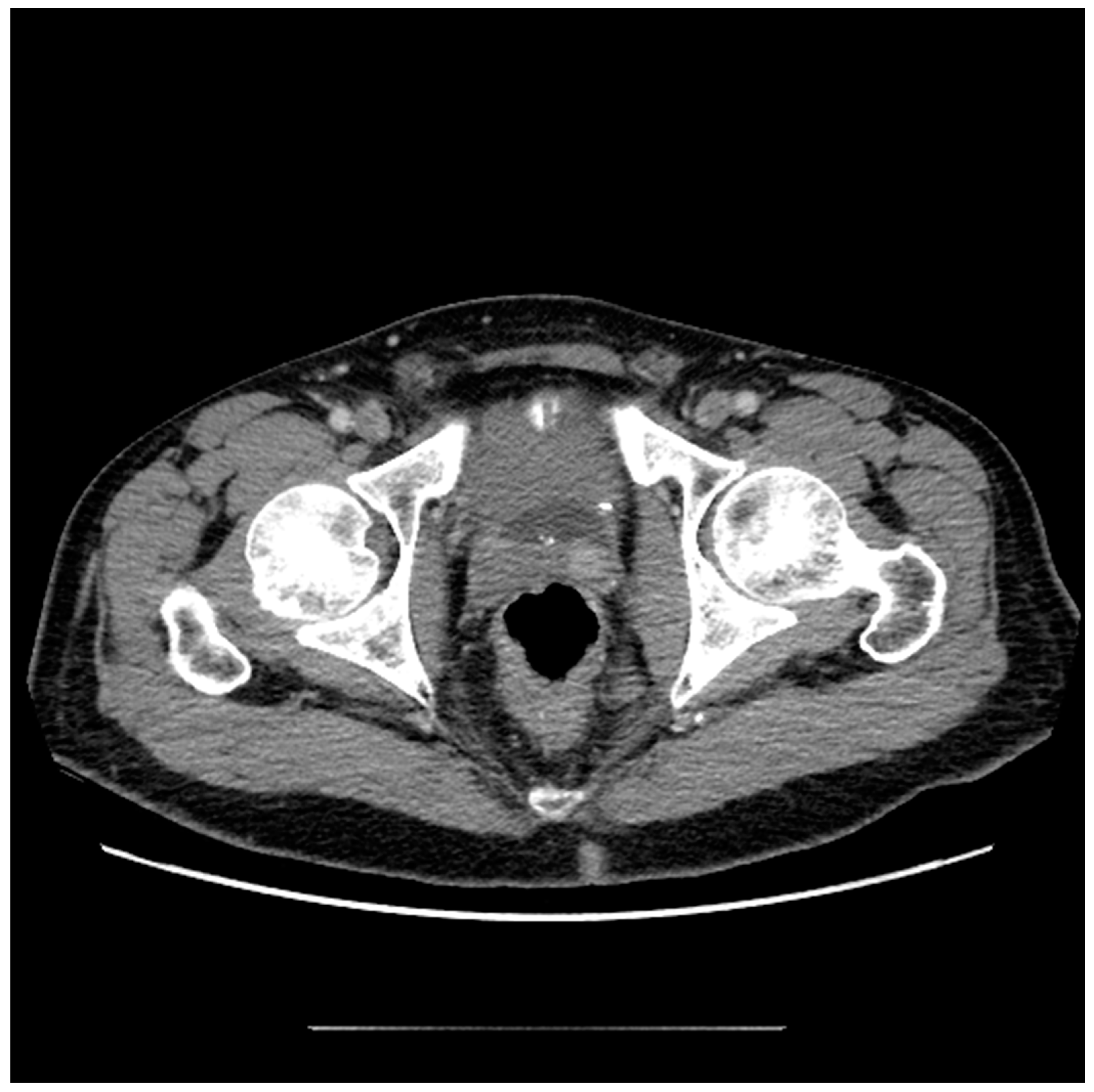{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Imaging Modalities Used to Evaluate Prostate Pathology
2.1. Computed Tomography (CT)
2.2. Ultrasound
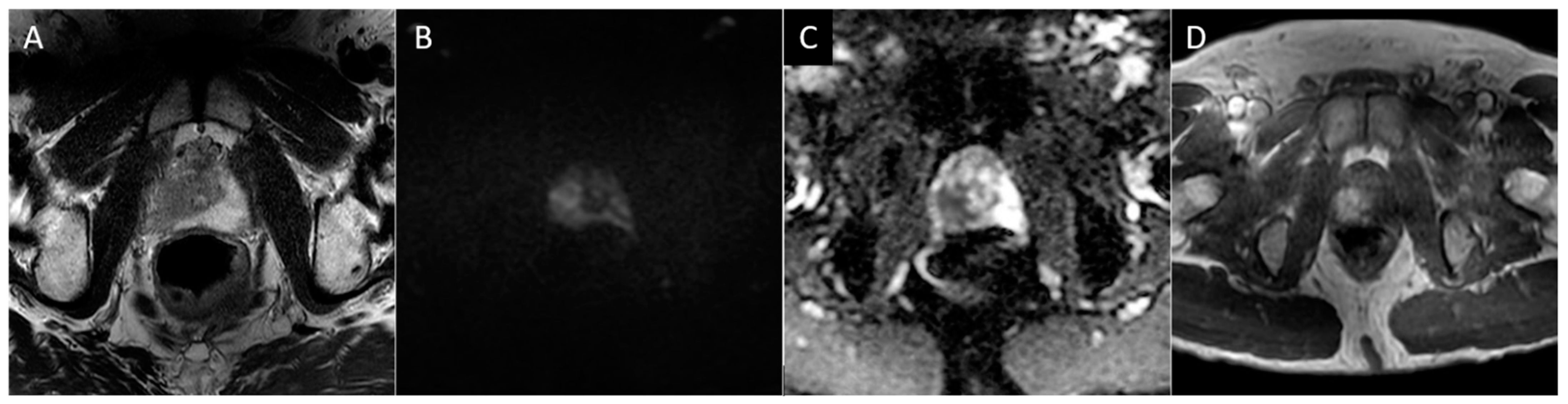
2.3. Magnetic Resonance Imaging (MRI)
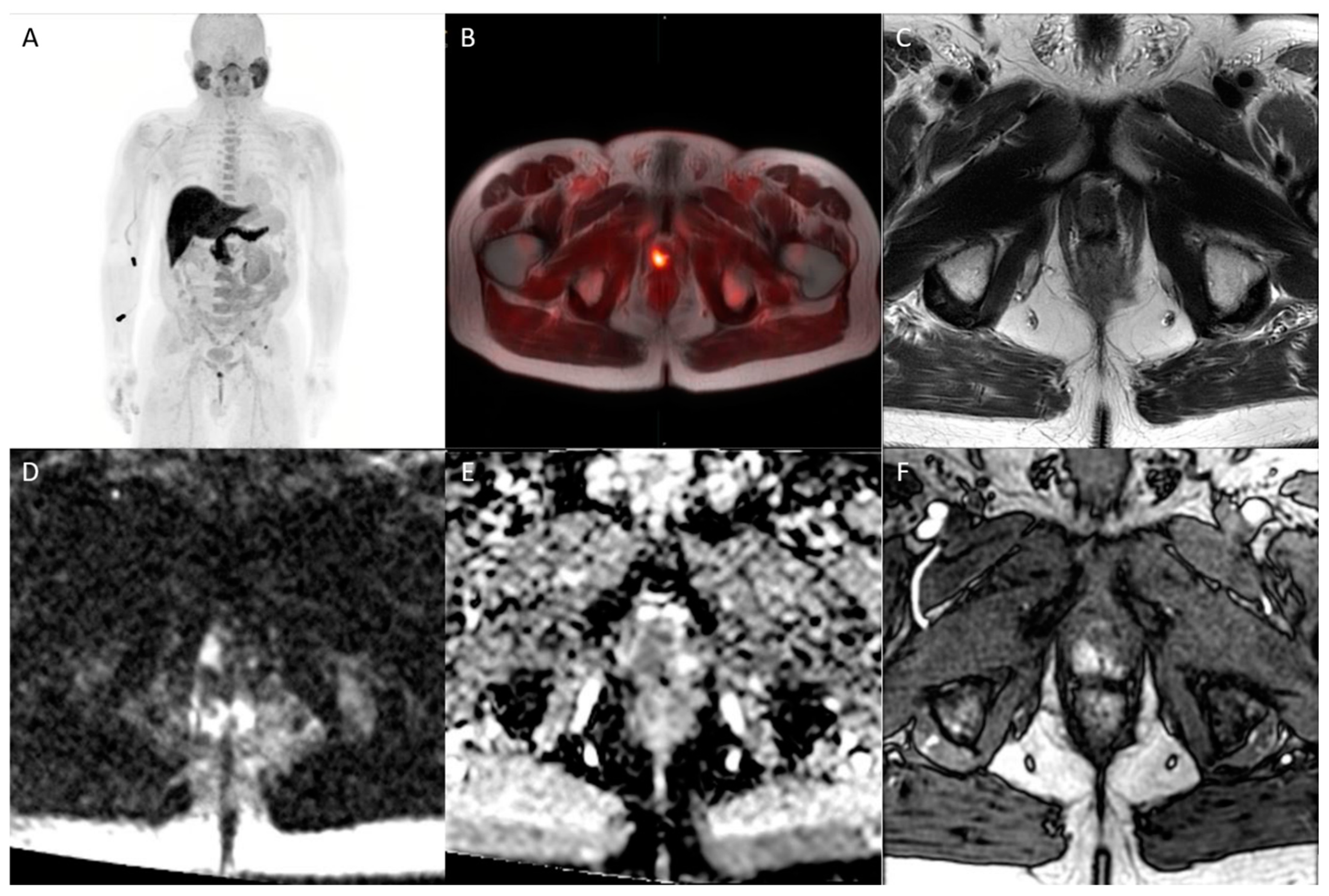
2.4. Positron Emission Tomography (PET)
3. Treatment Options and Expected Imaging Appearance
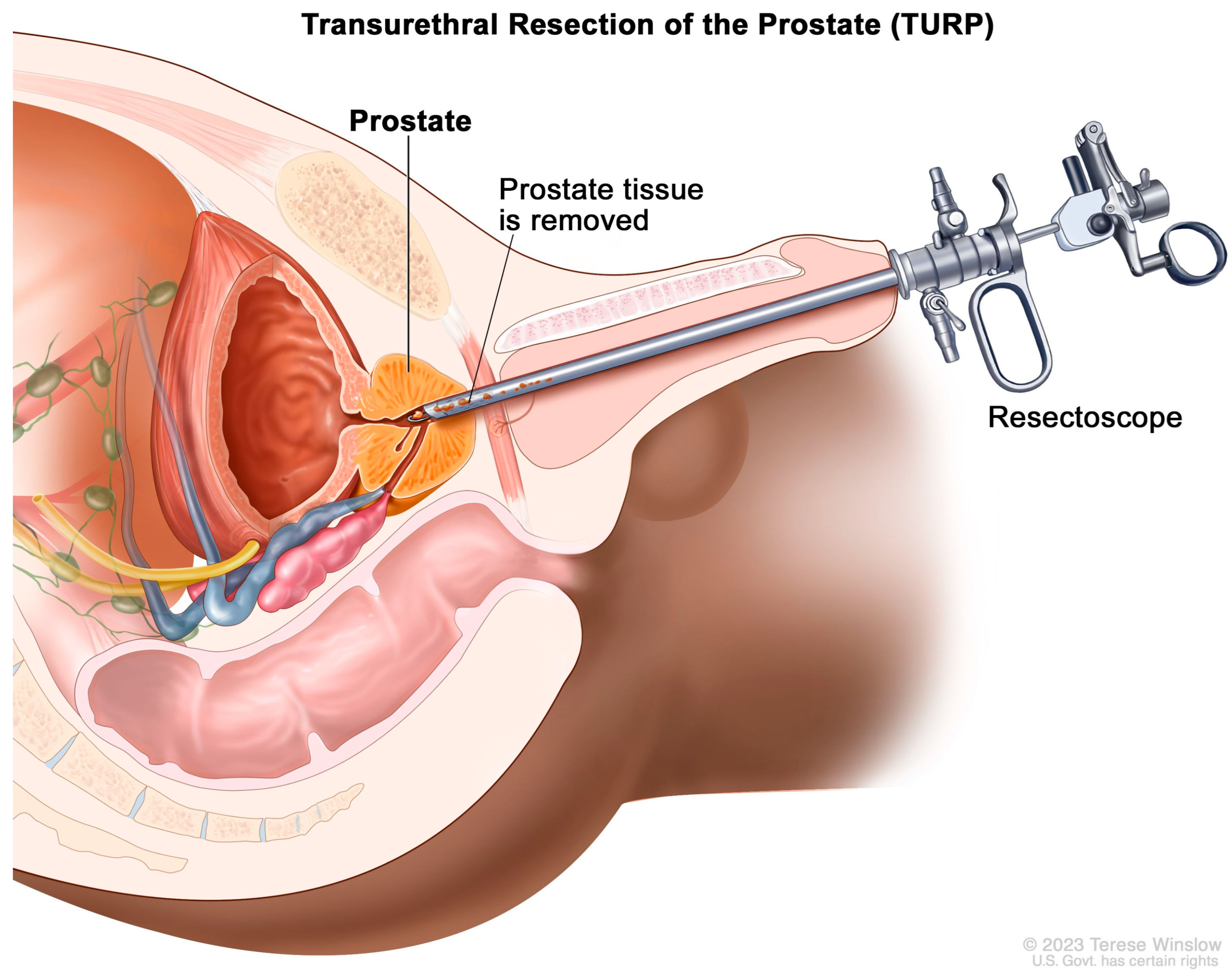
3.1. Treatment of Benign Disease
3.2. Treatment of Malignant Disease
4. Conclusions and Future Perspectives
Author Contributions
Funding
Conflicts of Interest
References
- Berry, S.J.; Coffey, D.S.; Walsh, P.C.; Ewing, L.L. The development of human benign prostatic hyperplasia with age. J. Urol. 1984, 132, 474–479. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, M.M.; Rais-Bahrami, S.; Turkbey, B.; George, A.K.; Rothwax, J.; Shakir, N.; Okoro, C.; Raskolnikov, D.; Parnes, H.L.; Linehan, W.M.; et al. Comparison of MR/ultrasound fusion-guided biopsy with ultrasound-guided biopsy for the diagnosis of prostate cancer. JAMA 2015, 313, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Banker, H.; Selvarajan, S.K. Prostate Imaging, in StatPearls; StatPearls Publishing LLC: Treasure Island, FL, USA, 2023. [Google Scholar]
- Jia, J.B.; Houshyar, R.; Verma, S.; Uchio, E.; Lall, C. Prostate cancer on computed tomography: A direct comparison with multi-parametric magnetic resonance imaging and tissue pathology. Eur. J. Radiol. 2016, 85, 261–267. [Google Scholar] [CrossRef]
- Engeler, C.E.; Wasserman, N.F.; Zhang, G. Preoperative assessment of prostatic carcinoma by computerized tomography. Weaknesses and new perspectives. Urology 1992, 40, 346–350. [Google Scholar] [CrossRef]
- Ferro, M.; de Cobelli, O.; Musi, G.; del Giudice, F.; Carrieri, G.; Busetto, G.M.; Falagario, U.G.; Sciarra, A.; Maggi, M.; Crocetto, F.; et al. Radiomics in prostate cancer: An up-to-date review. Ther. Adv. Urol. 2022, 14, 17562872221109020. [Google Scholar] [CrossRef]
- Ferro, M.; de Cobelli, O.; Vartolomei, M.D.; Lucarelli, G.; Crocetto, F.; Barone, B.; Sciarra, A.; Del Giudice, F.; Muto, M.; Maggi, M.; et al. Prostate Cancer Radiogenomics-From Imaging to Molecular Characterization. Int. J. Mol. Sci. 2021, 22, 9971. [Google Scholar] [CrossRef]
- Korevaar, S.; Tennakoon, R.; Page, M.; Brotchie, P.; Thangarajah, J.; Florescu, C.; Sutherland, T.; Kam, N.M.; Bab-Hadiashar, A. Incidental detection of prostate cancer with computed tomography scans. Sci. Rep. 2021, 11, 7956. [Google Scholar] [CrossRef]
- Prando, A.; Wallace, S. Helical CT of prostate cancer: Early clinical experience. AJR Am. J. Roentgenol. 2000, 175, 343–346. [Google Scholar] [CrossRef]
- Mena, E.; Black, P.C.; Rais-Bahrami, S.; Gorin, M.; Allaf, M.; Choyke, P. Novel PET imaging methods for prostate cancer. World. J. Urol. 2021, 39, 687–699. [Google Scholar] [CrossRef]
- Galgano, S.J.; McDonald, A.M.; West, J.T.; Rais-Bahrami, S. Defining Oligometastatic Disease in the New Era of PSMA-PET Imaging for Primary Staging of Prostate Cancer. Cancers 2022, 14, 3302. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Raghavan, M. Diagnostic imaging and image-guided therapy of skeletal metastases. Cancer Control 2012, 19, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Tyloch, J.F.; Wieczorek, A.P. The standards of an ultrasound examination of the prostate gland. Part 1. J. Ultrason. 2016, 16, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Mitterberger, M.; Horninger, W.; Aigner, F.; Pinggera, G.M.; Steppan, I.; Rehder, P.; Frauscher, F. Ultrasound of the prostate. Cancer Imaging 2010, 10, 40–48. [Google Scholar] [CrossRef]
- Tyloch, J.F.; Wieczorek, A.P. The standards of an ultrasound examination of the prostate gland. Part 2. J. Ultrason. 2017, 17, 43–58. [Google Scholar] [CrossRef]
- Taymoorian, K.; Thomas, A.; Slowinski, T.; Khiabanchian, M.; Stephan, C.; Lein, M.; Deger, S.; Lenk, S.; A Loening, S.; Fischer, T. Transrectal broadband-Doppler sonography with intravenous contrast medium administration for prostate imaging and biopsy in men with an elevated PSA value and previous negative biopsies. Anticancer Res. 2007, 27, 4315–4320. [Google Scholar]
- Basso Dias, A.; Ghai, S. Micro-Ultrasound: Current Role in Prostate Cancer Diagnosis and Future Possibilities. Cancers 2023, 15, 1280. [Google Scholar] [CrossRef]
- Calace, F.P.; Napolitano, L.; Arcaniolo, D.; Stizzo, M.; Barone, B.; Crocetto, F.; Olivetta, M.; Amicuzi, U.; Cirillo, L.; Rubinacci, A.; et al. Micro-Ultrasound in the Diagnosis and Staging of Prostate and Bladder Cancer: A Comprehensive Review. Medicina 2022, 58, 1264. [Google Scholar] [CrossRef]
- Ghai, S.; Eure, G.; Fradet, V.; Hyndman, M.E.; McGrath, T.; Wodlinger, B.; Pavlovich, C.P. Assessing Cancer Risk on Novel 29 MHz Micro-Ultrasound Images of the Prostate: Creation of the Micro-Ultrasound Protocol for Prostate Risk Identification. J. Urol. 2016, 196, 562–569. [Google Scholar] [CrossRef]
- Laurence Klotz, C.M. Can high resolution micro-ultrasound replace MRI in the diagnosis of prostate cancer? Eur. Urol. Focus 2020, 6, 419–423. [Google Scholar] [CrossRef]
- Sountoulides, P.; Pyrgidis, N.; Polyzos, S.A.; Mykoniatis, I.; Asouhidou, E.; Papatsoris, A.; Dellis, A.; Anastasiadis, A.; Lusuardi, L.; Hatzichristou, D. Micro-Ultrasound-Guided vs Multiparametric Magnetic Resonance Imaging-Targeted Biopsy in the Detection of Prostate Cancer: A Systematic Review and Meta-Analysis. J. Urol. 2021, 205, 1254–1262. [Google Scholar] [CrossRef]
- Zhang, M.; Tang, J.; Luo, Y.; Wang, Y.; Wu, M.; Memmott, B.; Gao, J. Diagnostic Performance of Multiparametric Transrectal Ultrasound in Localized Prostate Cancer: A Comparative Study With Magnetic Resonance Imaging. J. Ultrasound. Med. 2019, 38, 1823–1830. [Google Scholar] [CrossRef]
- Chen, T.; Wang, F.; Chen, H.; Wang, M.; Liu, P.; Liu, S.; Zhou, Y.; Ma, Q. Multiparametric transrectal ultrasound for the diagnosis of peripheral zone prostate cancer and clinically significant prostate cancer: Novel scoring systems. BMC Urol. 2022, 22, 64. [Google Scholar] [CrossRef]
- Kaneko, M.; Lenon, M.S.L.; Ramacciotti, L.S.; Medina, L.G.; Sayegh, A.S.; Rincon, A.L.R.; Perez, L.C.; Ghoreifi, A.; Lizana, M.; Jadvar, D.S.; et al. Multiparametric ultrasound of prostate: Role in prostate cancer diagnosis. Ther. Adv. Urol. 2022, 14, 17562872221145625. [Google Scholar] [CrossRef]
- Bjurlin, M.A.; Carroll, P.R.; Eggener, S.; Fulgham, P.F.; Margolis, D.J.; Pinto, P.A.; Rosenkrantz, A.B.; Rubenstein, J.N.; Rukstalis, D.B.; Taneja, S.S.; et al. Update of the Standard Operating Procedure on the Use of Multiparametric Magnetic Resonance Imaging for the Diagnosis, Staging and Management of Prostate Cancer. J. Urol. 2020, 203, 706–712. [Google Scholar] [CrossRef]
- Purysko, A.S.; Rosenkrantz, A.B.; Turkbey, I.B.; Macura, K.J. RadioGraphics Update: PI-RADS Version 2.1-A Pictorial Update. Radiographics 2020, 40, E33–E37. [Google Scholar] [CrossRef]
- Hassanzadeh, E.; Glazer, D.I.; Dunne, R.M.; Fennessy, F.M.; Harisinghani, M.G.; Tempany, C.M. Prostate imaging reporting and data system version 2 (PI-RADS v2): A pictorial review. Abdom. Radiol. 2017, 42, 278–289. [Google Scholar] [CrossRef]
- de Rooij, M.; Israël, B.; Tummers, M.; Ahmed, H.U.; Barrett, T.; Giganti, F.; Hamm, B.; Løgager, V.; Padhani, A.; Panebianco, V.; et al. ESUR/ESUI consensus statements on multi-parametric MRI for the detection of clinically significant prostate cancer: Quality requirements for image acquisition, interpretation and radiologists’ training. Eur. Radiol. 2020, 30, 5404–5416. [Google Scholar] [CrossRef]
- Giganti, F.; Allen, C.; Emberton, M.; Moore, C.M.; Kasivisvanathan, V. Prostate Imaging Quality (PI-QUAL): A New Quality Control Scoring System for Multiparametric Magnetic Resonance Imaging of the Prostate from the PRECISION trial. Eur. Urol. Oncol. 2020, 3, 615–619. [Google Scholar] [CrossRef]
- Giganti, F.; Kirkham, A.; Kasivisvanathan, V.; Papoutsaki, M.-V.; Punwani, S.; Emberton, M.; Moore, C.M.; Allen, C. Understanding PI-QUAL for prostate MRI quality: A practical primer for radiologists. Insights Imaging 2021, 12, 59. [Google Scholar] [CrossRef]
- Karanasios, E.; Caglic, I.; Zawaideh, J.P.; Barrett, T. Prostate MRI quality: Clinical impact of the PI-QUAL score in prostate cancer diagnostic work-up. Br. J. Radiol. 2022, 95, 20211372. [Google Scholar] [CrossRef]
- Pötsch, N.; Rainer, E.; Clauser, P.; Vatteroni, G.; Hübner, N.; Korn, S.; Shariat, S.; Helbich, T.; Baltzer, P. Impact of PI-QUAL on PI-RADS and cancer yield in an MRI-TRUS fusion biopsy population. Eur. J. Radiol. 2022, 154, 110431. [Google Scholar] [CrossRef]
- Ling, D.; Lee, J.K.; Heiken, J.P.; Balfe, D.M.; Glazer, H.S.; McCLENNAN, B.L. Prostatic carcinoma and benign prostatic hyperplasia: Inability of MR imaging to distinguish between the two diseases. Radiology 1986, 158, 103–107. [Google Scholar] [CrossRef]
- Schiebler, M.; E Tomaszewski, J.; Bezzi, M.; Pollack, H.M.; Kressel, H.Y.; Cohen, E.K.; Altman, H.G.; Gefter, W.B.; Wein, A.J.; Axel, L. Prostatic carcinoma and benign prostatic hyperplasia: Correlation of high-resolution MR and histopathologic findings. Radiology 1989, 172, 131–137. [Google Scholar] [CrossRef]
- Grossfeld, G.D.; Coakley, F.V. Benign prostatic hyperplasia: Clinical overview and value of diagnostic imaging. Radiol. Clin. N. Am. 2000, 38, 31–47. [Google Scholar] [CrossRef]
- Massanova, M.; Robertson, S.; Barone, B.; Dutto, L.; Caputo, V.F.; Bhatt, J.R.; Ahmad, I.; Bada, M.; Obeidallah, A.; Crocetto, F. The Comparison of Imaging and Clinical Methods to Estimate Prostate Volume: A Single-Centre Retrospective Study. Urol. Int. 2021, 105, 804–810. [Google Scholar] [CrossRef]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef]
- Drost, F.-J.H.; Osses, D.; Nieboer, D.; Bangma, C.H.; Steyerberg, E.W.; Roobol, M.J.; Schoots, I.G. Prostate Magnetic Resonance Imaging, with or Without Magnetic Resonance Imaging-targeted Biopsy, and Systematic Biopsy for Detecting Prostate Cancer: A Cochrane Systematic Review and Meta-analysis. Eur. Urol. 2020, 77, 78–94. [Google Scholar] [CrossRef]
- Moldovan, P.C.; Broeck, T.V.D.; Sylvester, R.; Marconi, L.; Bellmunt, J.; Bergh, R.C.v.D.; Bolla, M.; Briers, E.; Cumberbatch, M.G.; Fossati, N.; et al. What Is the Negative Predictive Value of Multiparametric Magnetic Resonance Imaging in Excluding Prostate Cancer at Biopsy? A Systematic Review and Meta-analysis from the European Association of Urology Prostate Cancer Guidelines Panel. Eur. Urol. 2017, 72, 250–266. [Google Scholar] [CrossRef]
- Kasivisvanathan, V.; Rannikko, A.S.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budäus, L.; Hellawell, G.; Hindley, R.G.; et al. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef]
- Kornienko, K.; Siegel, F.; Borkowetz, A.; Hoffmann, M.A.; Drerup, M.; Lieb, V.; Bruendl, J.; Höfner, T.; Cash, H.; von Hardenberg, J.; et al. Active surveillance inclusion criteria under scrutiny in magnetic resonance imaging-guided prostate biopsy: A multicenter cohort study. Prostate Cancer Prostatic. Dis. 2022, 25, 109–116. [Google Scholar] [CrossRef]
- Muller, B.G.; Shih, J.H.; Sankineni, S.; Marko, J.; Rais-Bahrami, S.; George, A.K.; de la Rosette, J.J.M.C.H.; Merino, M.J.; Wood, B.J.; Pinto, P.A.; et al. Prostate Cancer: Interobserver Agreement and Accuracy with the Revised Prostate Imaging Reporting and Data System at Multiparametric MR Imaging. Radiology 2015, 277, 741–750. [Google Scholar] [CrossRef]
- Rosenkrantz, A.B.; Oto, A.; Turkbey, B.; Westphalen, A.C. Prostate Imaging Reporting and Data System (PI-RADS), Version 2: A Critical Look. AJR Am. J. Roentgenol. 2016, 206, 1179–1183. [Google Scholar] [CrossRef]
- Caglic, I.; Sushentsev, N.; Gnanapragasam, V.J.; Sala, E.; Shaida, N.; Koo, B.C.; Kozlov, V.; Warren, A.Y.; Kastner, C.; Barrett, T. MRI-derived PRECISE scores for predicting pathologically-confirmed radiological progression in prostate cancer patients on active surveillance. Eur. Radiol. 2021, 31, 2696–2705. [Google Scholar] [CrossRef]
- Calderone, C.E.; Lerner, S.P.; Taylor, J.M. The case for salvage cystectomy after pelvic radiation. Minerva. Urol. Nefrol. 2016, 68, 161–171. [Google Scholar]
- Panebianco, V.; Villeirs, G.; Weinreb, J.C.; Turkbey, B.I.; Margolis, D.J.; Richenberg, J.; Schoots, I.G.; Moore, C.M.; Futterer, J.; Macura, K.J.; et al. Prostate Magnetic Resonance Imaging for Local Recurrence Reporting (PI-RR): International Consensus -based Guidelines on Multiparametric Magnetic Resonance Imaging for Prostate Cancer Recurrence after Radiation Therapy and Radical Prostatectomy. Eur. Urol. Oncol. 2021, 4, 868–876. [Google Scholar] [CrossRef]
- Chan, T.W.; Kressel, H.Y. Prostate and seminal vesicles after irradiation: MR appearance. J. Magn. Reson. Imaging 1991, 1, 503–511. [Google Scholar] [CrossRef]
- Patel, P.; Mathew, M.S.; Trilisky, I.; Oto, A. Multiparametric MR Imaging of the Prostate after Treatment of Prostate Cancer. Radiographics 2018, 38, 437–449. [Google Scholar] [CrossRef]
- Haider, M.A.; Chung, P.; Sweet, J.; Toi, A.; Jhaveri, K.; Ménard, C.; Warde, P.; Trachtenberg, J.; Lockwood, G.; Milosevic, M. Dynamic contrast-enhanced magnetic resonance imaging for localization of recurrent prostate cancer after external beam radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 425–430. [Google Scholar] [CrossRef]
- Foltz, W.D.; Wu, A.; Chung, P.; Catton, C.; Bayley, A.; Milosevic, M.; Bristow, R.; Warde, P.; Simeonov, A.; Jaffray, D.A.; et al. Changes in apparent diffusion coefficient and T2 relaxation during radiotherapy for prostate cancer. J. Magn. Reson. Imaging 2013, 37, 909–916. [Google Scholar] [CrossRef]
- Cirillo, S.; Petracchini, M.; Scotti, L.; Gallo, T.; Macera, A.; Bona, M.C.; Ortega, C.; Gabriele, P.; Regge, D. Endorectal magnetic resonance imaging at 1.5 Tesla to assess local recurrence following radical prostatectomy using T2-weighted and contrast-enhanced imaging. Eur. Radiol. 2009, 19, 761–769. [Google Scholar] [CrossRef]
- De Visschere, P.J.; Standaert, C.; Fütterer, J.J.; Villeirs, G.M.; Panebianco, V.; Walz, J.; Maurer, T.; Hadaschik, B.A.; Lecouvet, F.E.; Giannarini, G.; et al. A Systematic Review on the Role of Imaging in Early Recurrent Prostate Cancer. Eur. Urol. Oncol. 2019, 2, 47–76. [Google Scholar] [CrossRef]
- Kwon, T.; Kim, J.K.; Lee, C.; Jung, J.; Ahn, H.; Kim, C.-S.; Hong, J.H. Discrimination of local recurrence after radical prostatectomy: Value of diffusion-weighted magnetic resonance imaging. Prostate Int. 2018, 6, 12–17. [Google Scholar] [CrossRef]
- Kelly, B.D.; Perera, M.; Bolton, D.M.; Papa, N. Social determinants of health: Does socioeconomic status affect access to staging imaging for men with prostate cancer. Prostate Cancer Prostatic. Dis. 2022, 2022, 1–3. [Google Scholar] [CrossRef]
- Liu, Y.; Zuckier, L.S.; Ghesani, N.V. Dominant uptake of fatty acid over glucose by prostate cells: A potential new diagnostic and therapeutic approach. Anticancer. Res. 2010, 30, 369–374. [Google Scholar]
- Jadvar, H. Imaging evaluation of prostate cancer with 18F-fluorodeoxyglucose PET/CT: Utility and limitations. Eur. J. Nucl. Med. Mol. Imaging 2013, 40 (Suppl. S1), S5–S10. [Google Scholar] [CrossRef]
- Reinicke, K.; Sotomayor, P.; Cisterna, P.; Delgado, C.; Nualart, F.; Godoy, A. Cellular distribution of Glut-1 and Glut-5 in benign and malignant human prostate tissue. J. Cell Biochem. 2012, 113, 553–562. [Google Scholar] [CrossRef]
- McParland, B.J.; Wall, A.; Johansson, S.; Sørensen, J. The clinical safety, biodistribution and internal radiation dosimetry of [(1)(8)F]fluciclovine in healthy adult volunteers. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 1256–1264. [Google Scholar] [CrossRef]
- Rais-Bahrami, S.; Efstathiou, J.A.; Turnbull, C.M.; Camper, S.B.; Kenwright, A.; Schuster, D.M.; Scarsbrook, A.F. (18)F-Fluciclovine PET/CT performance in biochemical recurrence of prostate cancer: A systematic review. Prostate Cancer Prostatic. Dis. 2021, 24, 997–1006. [Google Scholar] [CrossRef]
- Turkbey, B.; Mena, E.; Shih, J.; Pinto, P.A.; Merino, M.J.; Lindenberg, M.L.; Bernardo, M.; McKinney, Y.L.; Adler, S.; Owenius, R.; et al. Localized prostate cancer detection with 18F FACBC PET/CT: Comparison with MR imaging and histopathologic analysis. Radiology 2014, 270, 849–856. [Google Scholar] [CrossRef]
- Mason, B.R.; Eastham, J.A.; Davis, B.J.; Mynderse, L.A.; Pugh, T.J.; Lee, R.J.; Ippolito, J.E. Current Status of MRI and PET in the NCCN Guidelines for Prostate Cancer. J. Natl. Compr. Canc. Netw. 2019, 17, 506–513. [Google Scholar] [CrossRef]
- Odewole, O.A.; Tade, F.I.; Nieh, P.T.; Savir-Baruch, B.; Jani, A.B.; Master, V.A.; Rossi, P.J.; Halkar, R.K.; Osunkoya, A.O.; Akin-Akintayo, O.; et al. Recurrent prostate cancer detection with anti-3-[(18)F]FACBC PET/CT: Comparison with CT. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1773–1783. [Google Scholar] [CrossRef]
- Schuster, D.M.; Nieh, P.T.; Jani, A.B.; Amzat, R.; Bowman, F.D.; Halkar, R.K.; Master, V.A.; Nye, J.A.; Odewole, O.A.; Osunkoya, A.O.; et al. Anti-3-[(18)F]FACBC positron emission tomography-computerized tomography and (111) In-capromab pendetide single photon emission computerized tomography-computerized tomography for recurrent prostate carcinoma: Results of a prospective clinical trial. J. Urol. 2014, 191, 1446–1453. [Google Scholar] [CrossRef]
- Maurer, T.; Gschwend, J.E.; Rauscher, I.; Souvatzoglou, M.; Haller, B.; Weirich, G.; Wester, H.-J.; Heck, M.; Kübler, H.; Beer, A.J.; et al. Diagnostic Efficacy of (68) Gallium-PSMA Positron Emission Tomography Compared to Conventional Imaging for Lymph Node Staging of 130 Consecutive Patients with Intermediate to High Risk Prostate Cancer. J. Urol. 2016, 195, 1436–1443. [Google Scholar] [CrossRef]
- Eiber, M.; Maurer, T.; Souvatzoglou, M.; Beer, A.J.; Ruffani, A.; Haller, B.; Graner, F.-P.; Kübler, H.; Haberhorn, U.; Eisenhut, M.; et al. Evaluation of Hybrid (6) (8) Ga-PSMA Ligand PET/CT in 248 Patients with Biochemical Recurrence after Radical Prostatectomy. J. Nucl. Med. 2015, 56, 668–674. [Google Scholar] [CrossRef]
- Galgano, S.J.; West, J.T.; Rais-Bahrami, S. Role of molecular imaging in the detection of localized prostate cancer. Ther. Adv. Urol. 2022, 14, 17562872221105018. [Google Scholar] [CrossRef]
- Albisinni, S.; Sarkis, J.; Diamand, R.; De Nunzio, C. Prebiopsy (68) Ga-PSMA PET imaging: Can we improve the current diagnostic pathway for prostate cancer? Prostate Cancer Prostatic. Dis. 2023, 26, 47–49. [Google Scholar] [CrossRef]
- Tian, A.; Lin, R.; Yu, J.; Zhang, F.; Zheng, Q.; Yuan, X.; Sun, Z.; Zhong, Z. The differential diagnostic value of dual-phase (18) F-DCFPyL PET/CT in prostate carcinoma. Prostate Cancer Prostatic. Dis. 2022, 25, 351–358. [Google Scholar] [CrossRef]
- Lerner, L.B.; McVary, K.T.; Barry, M.J.; Bixler, B.R.; Dahm, P.; Das, A.K.; Gandhi, M.C.; Kaplan, S.A.; Kohler, T.S.; Martin, L.; et al. Management of Lower Urinary Tract Symptoms Attributed to Benign Prostatic Hyperplasia: AUA GUIDELINE PART II-Surgical Evaluation and Treatment. J. Urol. 2021, 206, 818–826. [Google Scholar] [CrossRef]
- Kuo, R.L.; Paterson, R.F.; Kim, S.C.; Siqueira, T.M., Jr.; Elhilali, M.M.; Lingeman, J.E. Holmium Laser Enucleation of the Prostate (HoLEP): A Technical Update. World J. Surg. Oncol. 2003, 1, 6. [Google Scholar] [CrossRef]
- McVary, K.T.; Gange, S.N.; Shore, N.D.; Bolton, D.M.; Cowan, B.E.; Brown, B.T.; Te, A.E.; Chin, P.T.; Rukstalis, D.B.; Roehrborn, C.G. Treatment of LUTS secondary to BPH while preserving sexual function: Randomized controlled study of prostatic urethral lift. J. Sex. Med. 2014, 11, 279–287. [Google Scholar] [CrossRef]
- Westwood, J.; Geraghty, R.; Jones, P.; Rai, B.P.; Somani, B.K. Rezum: A new transurethral water vapour therapy for benign prostatic hyperplasia. Ther. Adv. Urol. 2018, 10, 327–333. [Google Scholar] [CrossRef]
- Bruinsma, S.M.; Bangma, C.H.; Carroll, P.R.; Leapman, M.S.; Rannikko, A.; Petrides, N.; Weerakoon, M.; Bokhorst, L.P.; Roobol, M.J.; Movember GAP3 consortium. Active surveillance for prostate cancer: A narrative review of clinical guidelines. Nat. Rev. Urol. 2016, 13, 151–167. [Google Scholar] [CrossRef]
- Nassiri, N.; Margolis, D.J.; Natarajan, S.; Sharma, D.S.; Huang, J.; Dorey, F.J.; Marks, L.S. Targeted Biopsy to Detect Gleason Score Upgrading during Active Surveillance for Men with Low versus Intermediate Risk Prostate Cancer. J. Urol. 2017, 197, 632–639. [Google Scholar] [CrossRef]
- Lai, W.S.; Gordetsky, J.B.; Thomas, J.V.; Nix, J.W.; Rais-Bahrami, S. Factors predicting prostate cancer upgrading on magnetic resonance imaging-targeted biopsy in an active surveillance population. Cancer 2017, 123, 1941–1948. [Google Scholar] [CrossRef]
- Glaser, Z.A.; Porter, K.K.; Thomas, J.V.; Gordetsky, J.B.; Rais-Bahrami, S. MRI findings guiding selection of active surveillance for prostate cancer: A review of emerging evidence. Transl. Androl. Urol. 2018, 7 (Suppl. S4), S411–S419. [Google Scholar] [CrossRef]
- Fang, A.M.; Glaser, Z.A.; Rais-Bahrami, S. Increasing the use of active surveillance for prostate cancer in younger men. Cancer 2019, 125, 3292–3295. [Google Scholar] [CrossRef]
- Kang, S.K.; Mali, R.D.; Prabhu, V.; Ferket, B.S.; Loeb, S. Active Surveillance Strategies for Low-Grade Prostate Cancer: Comparative Benefits and Cost-effectiveness. Radiology 2021, 300, 594–604. [Google Scholar] [CrossRef]
- Sathianathen, N.J.; Konety, B.R.; Alarid-Escudero, F.; Lawrentschuk, N.; Bolton, D.M.; Kuntz, K.M. Cost-effectiveness Analysis of Active Surveillance Strategies for Men with Low-risk Prostate Cancer. Eur. Urol. 2019, 75, 910–917. [Google Scholar] [CrossRef]
- Eastham, J.A.; Auffenberg, G.B.; Barocas, D.A.; Chou, R.; Crispino, T.; Davis, J.W.; Eggener, S.; Horwitz, E.M.; Kane, C.J.; Kirkby, E.; et al. Clinically Localized Prostate Cancer: AUA/ASTRO Guideline, Part II: Principles of Active Surveillance, Principles of Surgery, and Follow-Up. J. Urol. 2022, 208, 19–25. [Google Scholar] [CrossRef]
- Tewari, A.; Peabody, J.; Sarle, R.; Balakrishnan, G.; Hemal, A.; Shrivastava, A.; Menon, M. Technique of da Vinci robot-assisted anatomic radical prostatectomy. Urology 2002, 60, 569–572. [Google Scholar] [CrossRef]
- Napoli, A.; Anzidei, M.; Ciolina, F.; Marotta, E.; Marincola, B.C.; Brachetti, G.; Di Mare, L.; Cartocci, G.; Boni, F.; Noce, V.; et al. MR-guided high-intensity focused ultrasound: Current status of an emerging technology. Cardiovasc. Intervent. Radiol. 2013, 36, 1190–1203. [Google Scholar] [CrossRef]
- Galgano, S.J.; Planz, V.B.; Arora, S.; Rais-Bahrami, S. MR-Guided High-Intensity Directional Ultrasound Ablation of Prostate Cancer. Curr. Urol. Rep. 2021, 22, 3. [Google Scholar] [CrossRef]
- Donin, N.M.; Reiter, R.E. Why Targeting PSMA Is a Game Changer in the Management of Prostate Cancer. J. Nucl. Med. 2018, 59, 177–182. [Google Scholar] [CrossRef]










Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calderone, C.E.; Turner, E.M.; Hayek, O.E.; Summerlin, D.; West, J.T.; Rais-Bahrami, S.; Galgano, S.J. Contemporary Review of Multimodality Imaging of the Prostate Gland. Diagnostics 2023, 13, 1860. https://doi.org/10.3390/diagnostics13111860
Calderone CE, Turner EM, Hayek OE, Summerlin D, West JT, Rais-Bahrami S, Galgano SJ. Contemporary Review of Multimodality Imaging of the Prostate Gland. Diagnostics. 2023; 13(11):1860. https://doi.org/10.3390/diagnostics13111860
Chicago/Turabian StyleCalderone, Carli E., Eric M. Turner, Omar E. Hayek, David Summerlin, Janelle T. West, Soroush Rais-Bahrami, and Samuel J. Galgano. 2023. "Contemporary Review of Multimodality Imaging of the Prostate Gland" Diagnostics 13, no. 11: 1860. https://doi.org/10.3390/diagnostics13111860