
Evaluation of the BioFire® FilmArray® Pneumonia Panel with Conventional Bacterial Culture in Conjunction with Leukocyte Esterase Test
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Conventional Culture
2.3. BioFire FilmArray Pneumonia Panel (PN-Panel)
2.4. Leukocyte Esterase (LE) Strip Test
2.5. Discrepancy Analysis for Bacterial Pathogens
2.6. Statistical Analysis
3. Results
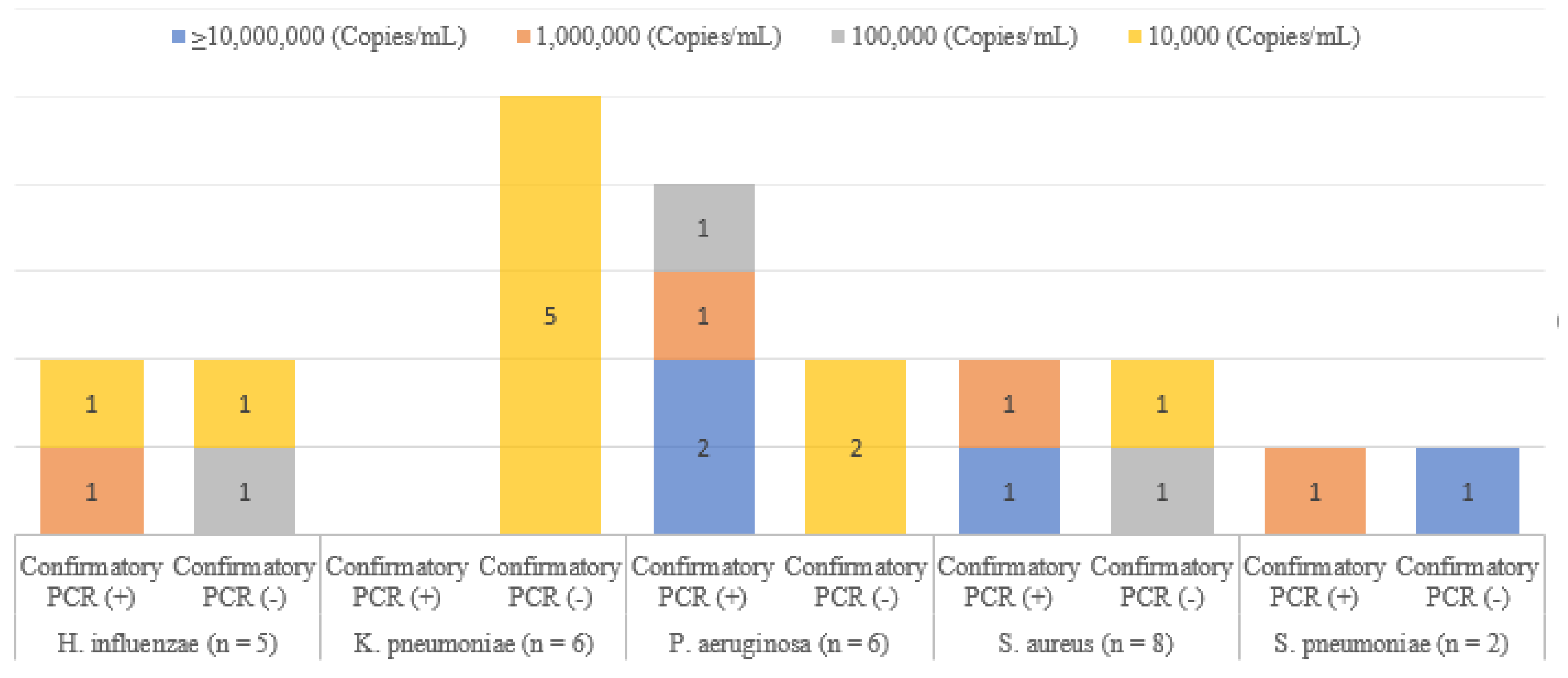
3.1. Pathogens Detected by PN-Panel vs. Conventional Culture
3.2. Correlation between LE Test and Sputum Quality Grading, Culture-Positive Rate, and PN-Panel-Positive Rate
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McLaughlin, J.M.; Khan, F.L.; Thoburn, E.A.; Isturiz, R.E.; Swerdlow, D.L. Rates of hospitalization for community-acquired pneumonia among US adults: A systematic review. Vaccine 2020, 38, 741–751. [Google Scholar] [CrossRef] [PubMed]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and treatment of adults with community-acquired pneumonia. An official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America. Am. J. Respir. Crit. Care Med. 2019, 200, e45–e67. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, J.G.; Mundy, L.M. Community-acquired pneumonia. N. Engl. J. Med. 1995, 333, 1618–1624. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Self, W.H.; Wunderink, R.G.; Fakhran, S.; Balk, R.; Bramley, A.M.; Reed, C.; Grijalva, C.G.; Anderson, E.J.; Courtney, D.M.; et al. Community-acquired pneumonia requiring hospitalization among U.S. adults. N. Engl. J. Med. 2015, 373, 415–427. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, H.; Kitsios, G.D.; Iwata, M.; Terasawa, T. Sputum Gram stain for bacterial pathogen diagnosis in community-acquired pneumonia: A systematic review and bayesian meta-analysis of diagnostic accuracy and yield. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, 71, 499–513. [Google Scholar] [CrossRef]
- Losier, A.; Dela Cruz, C.S. New testing guidelines for community-acquired pneumonia. Curr. Opin. Infect. Dis. 2022, 35, 128–132. [Google Scholar] [CrossRef]
- Webber, D.M.; Wallace, M.A.; Burnham, C.-A.D.; Anderson, N.W. Evaluation of the BioFire FilmArray pneumonia panel for detection of viral and bacterial pathogens in lower respiratory tract specimens in the setting of a tertiary care academic medical center. J. Clin. Microbiol. 2020, 58, e00343-20. [Google Scholar] [CrossRef]
- Kamel, N.A.; Alshahrani, M.Y.; Aboshanab, K.M.; El Borhamy, M.I. Evaluation of the BioFire FilmArray pneumonia panel plus to the conventional diagnostic methods in determining the microbiological etiology of hospital-acquired pneumonia. Biology 2022, 11, 377. [Google Scholar] [CrossRef]
- CLSI. Collection, Transport, Preparation, and Storage of Specimens for Molecular Methods, 2nd ed.; CLSI Guideline MM13; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2020. [Google Scholar]
- Jacobs, J.A.; De Brauwer, E.I.; Cornelissen, E.I.; Drent, M. Correlation of leukocyte esterase detection by reagent strips and the presence of neutrophils: A study in BAL fluid. Chest 2000, 118, 1450–1454. [Google Scholar] [CrossRef]
- Azoulay, E.; Fartoukh, M.; Galliot, R.; Baud, F.; Simonneau, G.; Le Gall, J.R.; Schlemmer, B.; Chevret, S. Rapid diagnosis of infectious pleural effusions by use of reagent strips. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2000, 31, 914–919. [Google Scholar] [CrossRef]
- Leber, A.L. Clinical Microbiology Procedures Handbook; John Wiley & Sons: Hoboken, NJ, USA, 2020. [Google Scholar]
- Murray, P.R.; Washington, J.A. Microscopic and bacteriologic analysis of expectorated sputum. Mayo Clin. Proc. 1975, 50, 339–344. [Google Scholar] [PubMed]
- Heineman, H.S.; Radano, R.R. Acceptability and cost savings of selective sputum microbiology in a community teaching hospital. J. Clin. Microbiol. 1979, 10, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Price, L.B.; Hungate, B.A.; Koch, B.J.; Davis, G.S.; Liu, C.M. Colonizing opportunistic pathogens (COPs): The beasts in all of us. PLoS Pathog. 2017, 13, e1006369. [Google Scholar] [CrossRef] [PubMed]
- Chapin, K.C.; Doern, G.V. Selective media for recovery of Haemophilus influenzae from specimens contaminated with upper respiratory tract microbial flora. J. Clin. Microbiol. 1983, 17, 1163–1165. [Google Scholar] [CrossRef] [PubMed]
- Kurt, I.S.; Unluer, E.E.; Evrin, T.; Katipoglu, B.; Eser, U. Urine dipstick of sputum for the rapid diagnosis of community acquired pneumonia. J. Natl. Med. Assoc. 2018, 110, 579–582. [Google Scholar] [CrossRef]
- Gal-Oz, A.; Kassis, I.; Shprecher, H.; Beck, R.; Bentur, L. Correlation between rapid strip test and the quality of sputum. Chest 2004, 126, 1667–1671. [Google Scholar] [CrossRef]
- Nik Zuraina, N.M.N.; Goni, M.D.; Amalina, K.N.; Hasan, H.; Mohamad, S.; Suraiya, S. Thermostable heptaplex PCR assay for the detection of six respiratory bacterial pathogens. Diagnostics 2021, 11, 753. [Google Scholar] [CrossRef]
- Benitez, A.J.; Winchell, J.M. Clinical application of a multiplex real-time PCR assay for simultaneous detection of Legionella species, Legionella pneumophila, and Legionella pneumophila serogroup 1. J. Clin. Microbiol. 2013, 51, 348–351. [Google Scholar] [CrossRef]
- Lindsay, D.S.; Abraham, W.H.; Fallon, R.J. Detection of mip gene by PCR for diagnosis of Legionnaires’ disease. J. Clin. Microbiol. 1994, 32, 3068–3069. [Google Scholar] [CrossRef]
- Rouby, J.J.; Martin De Lassale, E.; Poete, P.; Nicolas, M.H.; Bodin, L.; Jarlier, V.; Le Charpentier, Y.; Grosset, J.; Viars, P. Nosocomial bronchopneumonia in the critically ill: Histologic and bacteriologic aspects. Am. Rev. Respir. Dis. 1992, 146, 1059–1066. [Google Scholar] [CrossRef]
- Dicker, A.J.; Lonergan, M.; Keir, H.R.; Smith, A.H.; Pollock, J.; Finch, S.; Cassidy, A.J.; Huang, J.T.J.; Chalmers, J.D. The sputum microbiome and clinical outcomes in patients with bronchiectasis: A prospective observational study. Lancet Respir. Med. 2021, 9, 885–896. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.J.; Procop, G.W.; Vogel, S.; Yen-Lieberman, B.; Richter, S.S. Utility of PCR, culture, and antigen detection methods for diagnosis of Legionellosis. J. Clin. Microbiol. 2015, 53, 3474–3477. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| FilmArray Pneumonia Panel (Number of Detected Pathogens) | Conventional Culture | |
|---|---|---|
| Detected | Not Detected | |
| Not detected (n = 27) | 3 1 | 24 |
| 1 (n = 28) | 14 2 | 14 |
| 2 (n = 5) | 2 | 3 |
| 3 (n = 4) | 3 | 1 |
| 4 (n = 3) | 3 | 0 |
| Total (n = 67) | 25 | 42 |
| FilmArray Pneumonia Panel | Number of Results for FilmArray Pneumonia Panel/Conventional Culture | OPA (95% CI) | |||
|---|---|---|---|---|---|
| (+/+) | (+/−) | (−/+) | (−/−) | ||
| A. baumannii | 2 | 3 | 0 | 62 | 95.5 (87.5–99.0) |
| E. cloacae complex | 0 | 1 | 0 | 66 | 98.5 (92.0–99.9) |
| E. coli | 2 | 2 | 0 | 63 | 97.0 (89.6–99.6) |
| H. influenzae | 1 | 5 | 0 | 61 | 92.5 (83.4–97.5) |
| K. aerogenes | 0 | 1 | 0 | 66 | 98.5 (92.0–99.9) |
| K. oxytoca | 0 | 1 | 0 | 66 | 98.5 (92.0–99.9) |
| K. pneumoniae | 4 | 6 | 0 | 57 | 91.0 (81.5–96.6) |
| M. catarrhalis | 0 | 1 | 0 | 66 | 98.5 (92.0–99.9) |
| P. aeruginosa | 6 | 6 | 0 | 55 | 91.0 (81.5–96.6) |
| S. marcescens | 0 | 1 | 0 | 66 | 98.5 (92.0–99.9) |
| S. aureus | 6 | 8 | 0 | 53 | 88.1 (77.8–94.7) |
| S. agalactiae | 1 | 1 | 0 | 65 | 98.5 (92.0–99.9) |
| S. pneumoniae | 1 | 2 | 0 | 64 | 97.0 (89.6–99.6) |
| L. pneumophila | 0 | 1 | 0 | 66 | 98.5 (92.0–99.9) |
| Total | 23 | 39 | 0 | 876 | 95.8 (94.4–97.0) |
| PN-Panel Result (Copies/mL) | Sputum Quality | Concordance Rate | |||
|---|---|---|---|---|---|
| Adequate | Inadequate | ||||
| PN-Panel (+)/ Conventional Culture (+) | PN-Panel (+)/ Conventional Culture (−) | PN-Panel (+)/ Conventional Culture (+) | PN-Panel (+)/ Conventional Culture (−) | ||
| 104 (n = 17) | 1 | 10 | 0 | 6 | 1/17 |
| 105 (n = 8) | 0 | 4 | 0 | 4 | 0/8 |
| 106 (n = 10) | 1 | 4 | 1 | 4 | 2/10 |
| ≥107 (n = 26) | 11 | 4 | 9 | 2 | 20/26 |
| Total | 13 | 22 | 10 1 | 16 | 23/61 |
| Urine Strip Grade for Leukocyte Esterase | Sputum Quality (Adequate) (n = 39) | Sputum Quality (Inadequate) (n = 28) | ||
|---|---|---|---|---|
| PN-Panel (+) | PN-Panel (−) | PN-Panel (+) | PN-Panel (−) | |
| Negative (n = 21) | 4 | 4 | 4 | 9 |
| Positive (1+, 2+, 3+) (n = 45) | 20 | 11 | 11 | 3 |
| Mucoid (n = 1) | 0 | 0 | 1 | 0 |
| Total | 24 | 15 | 16 | 12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, I.Y.; Seok, H.S.; Kwon, J.A.; Lee, J.; Jo, S.; Kim, S.Y.; Park, Y.-J. Evaluation of the BioFire® FilmArray® Pneumonia Panel with Conventional Bacterial Culture in Conjunction with Leukocyte Esterase Test. Diagnostics 2023, 13, 1847. https://doi.org/10.3390/diagnostics13111847
Yoo IY, Seok HS, Kwon JA, Lee J, Jo S, Kim SY, Park Y-J. Evaluation of the BioFire® FilmArray® Pneumonia Panel with Conventional Bacterial Culture in Conjunction with Leukocyte Esterase Test. Diagnostics. 2023; 13(11):1847. https://doi.org/10.3390/diagnostics13111847
Chicago/Turabian StyleYoo, In Young, Hyun Soo Seok, Joo An Kwon, Jongmin Lee, Sungjin Jo, Soo Young Kim, and Yeon-Joon Park. 2023. "Evaluation of the BioFire® FilmArray® Pneumonia Panel with Conventional Bacterial Culture in Conjunction with Leukocyte Esterase Test" Diagnostics 13, no. 11: 1847. https://doi.org/10.3390/diagnostics13111847