
Applying Deep Transfer Learning to Assess the Impact of Imaging Modalities on Colon Cancer Detection

Abstract
:1. Introduction
- (1)
- (2)
- We comprehensively reported the performance behavior for the detection of colon cancer, including generated images via different modalities coupled with DL models in the transfer learning setting. Moreover, we constructed 26 ensemble DL models and compared their performance against the 5 studied DL models.
- (3)
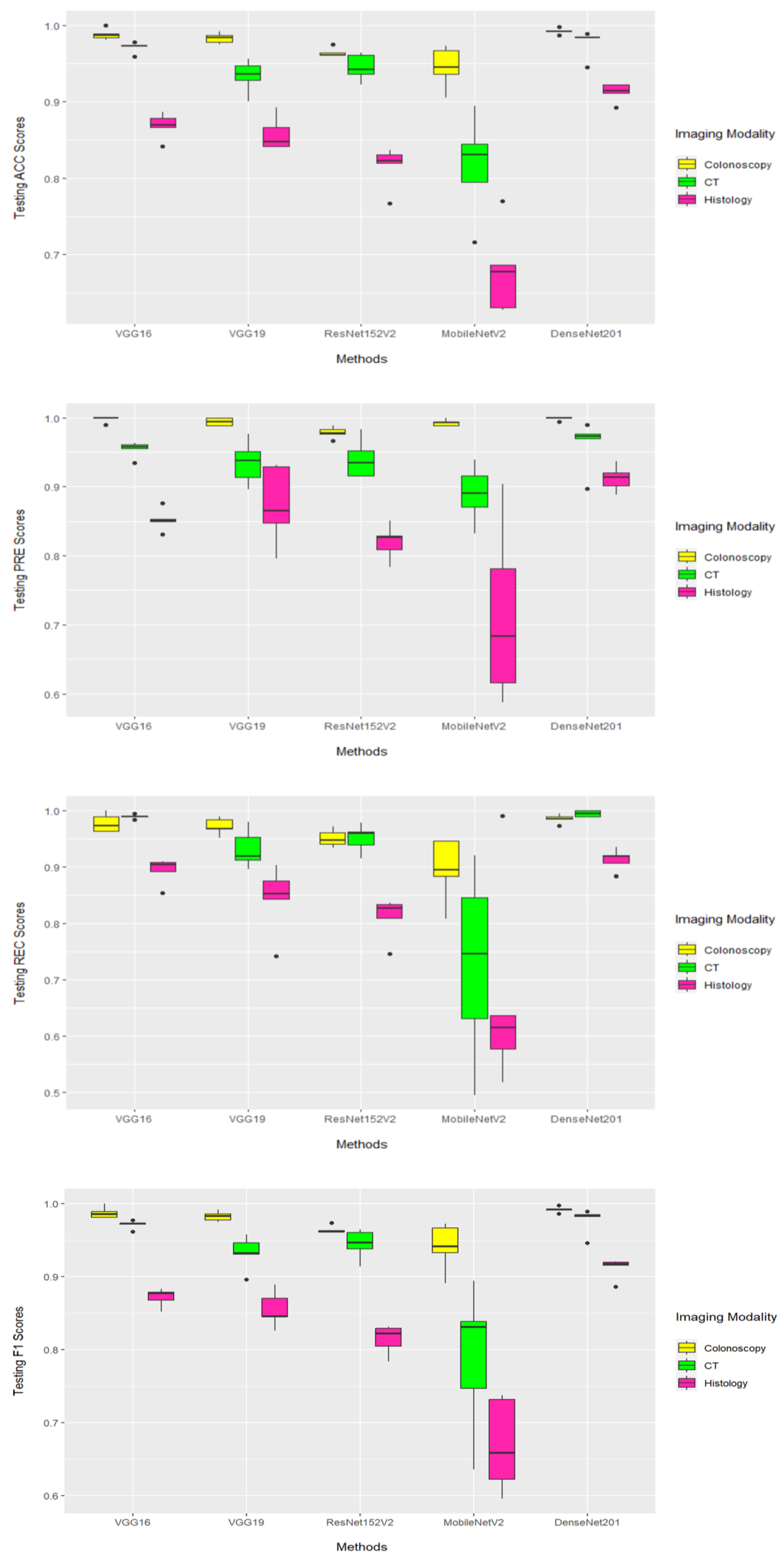
- We identified the best overall imaging modality and DL model for the detection of colon cancer. Specifically, our results reported that colonoscopy-based images outperformed CT-based (and histology-based) images when coupled with DL models.
- (4)
- Our reported results demonstrate the superiority of DenseNet201 compared to 30 other DL models, including 4 DL methods and 26 ensemble DL models. According to the average performance results, measured using a 5-fold cross-validation of the whole dataset of colonoscopy-based colon cancer images, DenseNet201 generated the highest average accuracy of 99.1%, the highest average area under the ROC curve of 99.1%, the highest average F1 of 99.1%, and the highest average precision of 99.8%. Since the 26 ensemble DL models generated inferior performance results, we moved their results into the Supplementary Materials File.
2. Materials and Methods
2.1. Datasets
2.2. Pre-Processing
2.3. Deep Learning Approach
3. Results
3.1. Classification Methodology
3.2. Implementation Details
3.3. Classification Results
3.3.1. Training Results
3.3.2. Testing Results
4. Discussion
5. Conclusions and Future Work
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| DL | Deep Learning |
| CT | Computed Tomography |
| VGG | Visual Geometry Group |
| ResNet | Residual Neural Network |
| CNN | Convolutional Neural Network |
| SVM | Support Vector Machine |
| CLAHE | Contrast Limited Adaptive Histogram Equalization |
| Conv | Convolutional |
| FC | Fully Connected |
| CC | Colon Cancer |
| SGD | Stochastic Gradient Descent |
| MRI | Magnetic Resonance Imaging |
| PET | Positron Emission Tomography |
| ACC | Accuracy |
| PRE | Precision |
| REC | Recall |
| ROC | Receiver Operating Characteristic |
| AUC | Area Under the ROC Curve |
References
- Hassin, O.; Nataraj, N.B.; Shreberk-Shaked, M.; Aylon, Y.; Yaeger, R.; Fontemaggi, G.; Mukherjee, S.; Maddalena, M.; Avioz, A.; Iancu, O. Different hotspot p53 mutants exert distinct phenotypes and predict outcome of colorectal cancer patients. Nat. Commun. 2022, 13, 2800. [Google Scholar] [CrossRef] [PubMed]
- Mori, G.; Rampelli, S.; Orena, B.S.; Rengucci, C.; De Maio, G.; Barbieri, G.; Passardi, A.; Casadei Gardini, A.; Frassineti, G.L.; Gaiarsa, S. Shifts of faecal microbiota during sporadic colorectal carcinogenesis. Sci. Rep. 2018, 8, 10329. [Google Scholar] [CrossRef] [PubMed]
- Chhikara, B.S.; Parang, K. Global Cancer Statistics 2022: The trends projection analysis. Chem. Biol. Lett. 2023, 10, 451. [Google Scholar]
- Li, J.N.; Yuan, S.Y. Fecal occult blood test in colorectal cancer screening. J. Dig. Dis. 2019, 20, 62–64. [Google Scholar] [CrossRef] [PubMed]
- Carethers, J.M. Fecal DNA testing for colorectal cancer screening. Annu. Rev. Med. 2020, 71, 59–69. [Google Scholar] [CrossRef]
- Gluecker, T.M.; Johnson, C.D.; Harmsen, W.S.; Offord, K.P.; Harris, A.M.; Wilson, L.A.; Ahlquist, D.A. Colorectal cancer screening with CT colonography, colonoscopy, and double-contrast barium enema examination: Prospective assessment of patient perceptions and preferences. Radiology 2003, 227, 378–384. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Verheul, H.M.; Flamen, P.; Rougier, P.; Beets-Tan, R.; Glynne-Jones, R.; Seufferlein, T. Imaging in colorectal cancer: Progress and challenges for the clinicians. Cancers 2016, 8, 81. [Google Scholar] [CrossRef]
- Patino-Barrientos, S.; Sierra-Sosa, D.; Garcia-Zapirain, B.; Castillo-Olea, C.; Elmaghraby, A. Kudo’s classification for colon polyps assessment using a deep learning approach. Appl. Sci. 2020, 10, 501. [Google Scholar] [CrossRef]
- Sarwinda, D.; Paradisa, R.H.; Bustamam, A.; Anggia, P. Deep learning in image classification using residual network (ResNet) variants for detection of colorectal cancer. Procedia Comput. Sci. 2021, 179, 423–431. [Google Scholar] [CrossRef]
- Ponzio, F.; Macii, E.; Ficarra, E.; Di Cataldo, S. Colorectal cancer classification using deep convolutional networks. In Proceedings of the 11th International Joint Conference on Biomedical Engineering Systems and Technologies, Madeira, Portugal, 19–21 January 2018; pp. 58–66. [Google Scholar] [CrossRef]
- Basha, S.S.; Ghosh, S.; Babu, K.K.; Dubey, S.R.; Pulabaigari, V.; Mukherjee, S. Rccnet: An efficient convolutional neural network for histological routine colon cancer nuclei classification. In Proceedings of the 15th International Conference on Control, Automation, Robotics and Vision (ICARCV), Singapore, 18–21 November 2018; pp. 1222–1227. [Google Scholar] [CrossRef]
- Ribeiro, E.; Uhl, A.; Häfner, M. Colonic polyp classification with convolutional neural networks. In Proceedings of the 2016 IEEE 29th International Symposium on Computer-Based Medical Systems (CBMS), Belfast and Dublin, Ireland, 20–24 June 2016; pp. 253–258. [Google Scholar] [CrossRef]
- Boellaard, T.N. Refining CT colonography methods. Eur. J. Radiol. 2013, 82, 1144–1158. [Google Scholar] [CrossRef]
- Schwab, M. Encyclopedia of Cancer; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Sena, P.; Fioresi, R.; Faglioni, F.; Losi, L.; Faglioni, G.; Roncucci, L. Deep learning techniques for detecting preneoplastic and neoplastic lesions in human colorectal histological images. Oncol. Lett. 2019, 18, 6101–6107. [Google Scholar] [CrossRef] [PubMed]
- Noorbakhsh, J.; Farahmand, S.; Foroughi Pour, A.; Namburi, S.; Caruana, D.; Rimm, D.; Soltanieh-Ha, M.; Zarringhalam, K.; Chuang, J.H. Deep learning-based cross-classifications reveal conserved spatial behaviors within tumor histological images. Nat. Commun. 2020, 11, 6367. [Google Scholar] [CrossRef] [PubMed]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar] [CrossRef]
- Leibe, B.; Matas, J.; Sebe, N.; Welling, M. Computer Vision–ECCV 2016: 14th European Conference, Amsterdam, The Netherlands, 11–14 October 2016, Proceedings, Part IV; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar] [CrossRef]
- Sandler, M.; Howard, A.; Zhu, M.; Zhmoginov, A.; Chen, L. Mobilenetv2: Inverted residuals and linear bottlenecks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 4510–4520. [Google Scholar] [CrossRef]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Proceedings of the IEEE conference on computer vision and pattern recognition. Densely Connect. Convolutional Netw. 2017, 4700–4708. [Google Scholar] [CrossRef]
- The Cancer Genome Atlas Program (TCGA). Available online: http://cancergenome.nih.gov/ (accessed on 6 January 2023).
- Kirk, S.; Lee, Y.; Sadow, C.A.; Levine, S.; Roche, C.; Bonaccio, E.; Filiippini, J. Radiology data from the cancer genome atlas colon adenocarcinoma [TCGA-COAD] collection. Cancer Imaging Arch. 2016. [Google Scholar] [CrossRef]
- Clark, K.; Vendt, B.; Smith, K.; Freymann, J.; Kirby, J.; Koppel, P.; Moore, S.; Phillips, S.; Maffitt, D.; Pringle, M. The Cancer Imaging Archive (TCIA): Maintaining and operating a public information repository. J. Digit. Imaging 2013, 26, 1045–1057. [Google Scholar] [CrossRef]
- Smith, K.; Clark, K.; Bennett, W.; Nolan, T.; Kirby, J.; Wolfsberger, M.; Moulton, J.; Vendt, B.; Freymann, J. Data from CT_COLONOGRAPHY. Cancer Imaging Arch. 2015. [Google Scholar] [CrossRef]
- Johnson, C.D.; Chen, M.; Toledano, A.Y.; Heiken, J.P.; Dachman, A.; Kuo, M.D.; Menias, C.O.; Siewert, B.; Cheema, J.I.; Obregon, R.G. Accuracy of CT colonography for detection of large adenomas and cancers. N. Engl. J. Med. 2008, 359, 1207–1217. [Google Scholar] [CrossRef]
- Borgli, H.; Thambawita, V.; Smedsrud, P.H.; Hicks, S.; Jha, D.; Eskeland, S.L.; Randel, K.R.; Pogorelov, K.; Lux, M.; Nguyen, D.T.D. HyperKvasir, a comprehensive multi-class image and video dataset for gastrointestinal endoscopy. Sci. Data 2020, 7, 283. [Google Scholar] [CrossRef]
- The HyperKvasir Dataset. Available online: https://osf.io/mh9sj/ (accessed on 6 January 2023).
- Kather, J.N.; Halama, N.; Marx, A. 100,000 Histological Images of Human Colorectal Cancer and Healthy Tissue. Zenodo 2018. [Google Scholar] [CrossRef]
- Srivaramangai, R.; Hiremath, P.; Patil, A.S. Preprocessing MRI images of colorectal cancer. Int. J. Comput. Sci. Issues (IJCSI) 2017, 14, 48. [Google Scholar]
- Sarraf, S.; Noori, M. Multimodal deep learning approach for event detection in sports using Amazon SageMaker. AWS Mach. Learn. Blog 2021. [Google Scholar]
- Minichino, J.; Howse, J. Learning OpenCV 3 Computer Vision with Python; Packt Publishing Ltd.: Birmingham, UK, 2015. [Google Scholar]
- Lokhande, D.; Zope, R.G.; Bendre, V.; Kopargaon, S.C. Image Inpainting Image Inpainting. Available online: http://ijcsn.org/IJCSN-2014/3-1/Image-Inpainting.pdf (accessed on 6 January 2023).
- Mohammed, R.; Rawashdeh, J.; Abdullah, M. Machine learning with oversampling and undersampling techniques: Overview study and experimental results. In Proceedings of the 2020 11th International Conference on Information and Communication Systems (ICICS), Irbid, Jordan, 7–9 April 2020; pp. 243–248. [Google Scholar] [CrossRef]
- Zuiderveld, K. Contrast limited adaptive histogram equalization. Graph. Gems 1994, 4, 474–485. [Google Scholar]
- Cadena, L.; Zotin, A.; Cadena, F.; Korneeva, A.; Legalov, A.; Morales, B. Noise reduction techniques for processing of medical images. In Proceedings of the World Congress on Engineering, London, UK, 5–7 July 2017; pp. 5–9. [Google Scholar]
- Lestari, T.; Luthfi, A. Retinal blood vessel segmentation using Gaussian filter. J. Phys. Conf. Ser. 2019, 1376, 012023. [Google Scholar] [CrossRef]
- Cogan, T.; Cogan, M.; Tamil, L. MAPGI: Accurate identification of anatomical landmarks and diseased tissue in gastrointestinal tract using deep learning. Comput. Biol. Med. 2019, 111, 103351. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.W.; Krishna, A.V. A study on the effect of Canny edge detection on downscaled images. Pattern Recognit. Image Anal. 2020, 30, 372–381. [Google Scholar] [CrossRef]
- Welikala, R.A.; Remagnino, P.; Lim, J.H.; Chan, C.S.; Rajendran, S.; Kallarakkal, T.G.; Zain, R.B.; Jayasinghe, R.D.; Rimal, J.; Kerr, A.R. Fine-tuning deep learning architectures for early detection of oral cancer. In Proceedings of the Mathematical and Computational Oncology: Second International Symposium, ISMCO 2020, San Diego, CA, USA, 8–10 October 2020; Proceedings 2. Springer: Berlin/Heidelberg, Germany, 2020; pp. 25–31. [Google Scholar] [CrossRef]
- Sakr, A.S.; Soliman, N.F.; Al-Gaashani, M.S.; Pławiak, P.; Ateya, A.A.; Hammad, M. An efficient deep learning approach for colon cancer detection. Appl. Sci. 2022, 12, 8450. [Google Scholar] [CrossRef]
- Fuhrman, J.; Yip, R.; Zhu, Y.; Jirapatnakul, A.C.; Li, F.; Henschke, C.I.; Yankelevitz, D.F.; Giger, M.L. Evaluation of emphysema on thoracic low-dose CTs through attention-based multiple instance deep learning. Sci. Rep. 2023, 13, 1187. [Google Scholar] [CrossRef]
- Rolon-Mérette, D.; Ross, M.; Rolon-Mérette, T.; Church, K. Introduction to Anaconda and Python: Installation and setup. Quant. Methods Psychol. 2016, 16, S3–S11. [Google Scholar] [CrossRef]
- Haslwanter, T. An Introduction to Statistics with Python. In With Applications in the Life Sciences; Springer International Publishing: Cham, Switzerland, 2016. [Google Scholar]
- Gulli, A.; Pal, S. Deep Learning with Keras; Packt Publishing Ltd.: Birmingham, UK, 2017. [Google Scholar]
- Gollapudi, S. Learn Computer Vision Using OpenCV; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar]
- Trappenberg, T.P. Fundamentals of Machine Learning; Oxford University Press: Oxford, UK, 2019. [Google Scholar]
- Wickham, H.; Chang, W.; Wickham, M.H. Package ‘ggplot2’. Creat. Elegant Data Vis. Using Gramm. Graph. Version 2016, 2, 1–189. [Google Scholar]
- Chollet, F. Deep Learning with Python; Simon and Schuster: New York, NY, USA, 2021. [Google Scholar]
- Goel, A.; Agarwal, A.; Vatsa, M.; Singh, R.; Ratha, N.K. DNDNet: Reconfiguring CNN for Adversarial Robustness. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition Workshops, Seattle, WA, USA, 14–19 June 2020; pp. 22–23. [Google Scholar]
- Zhang, J.; Lin, X.; Jiang, M.; Yu, Y.; Gong, C.; Zhang, W.; Tan, X.; Li, Y.; Ding, E.; Li, G. A Multi-Granularity Retrieval System for Natural Language-Based Vehicle Retrieval. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, New Orleans, LA, USA, 19–20 June 2022; pp. 3216–3225. [Google Scholar]
- Alaskar, H.; Hussain, A.; Al-Aseem, N.; Liatsis, P.; Al-Jumeily, D. Application of convolutional neural networks for automated ulcer detection in wireless capsule endoscopy images. Sensors 2019, 19, 1265. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dataset | Modality | Distribution | |
|---|---|---|---|
| POS 1 | NEG 2 | ||
| TCGA-COAD | CT | 900 | - |
| CT COLONOGRAPHY | CT | - | 900 |
| NCT-CRC-HE-100KNONORM | Histology | 900 | 900 |
| HyperKvasir | Colonoscopy | 900 | 900 |
| Imaging Modality | Method | MACC | MPRE | MREC | MF1 | MAUC |
|---|---|---|---|---|---|---|
| CT | VGG16 | 0.970 | 0.954 | 0.988 | 0.971 | 0.970 |
| VGG19 | 0.933 | 0.935 | 0.931 | 0.933 | 0.933 | |
| ResNet152V2 | 0.945 | 0.939 | 0.950 | 0.945 | 0.945 | |
| MobileNetV2 | 0.816 | 0.889 | 0.727 | 0.798 | 0.816 | |
| DenseNet201 | 0.976 | 0.961 | 0.994 | 0.977 | 0.976 | |
| Histology | VGG16 | 0.868 | 0.851 | 0.892 | 0.871 | 0.868 |
| VGG19 | 0.857 | 0.873 | 0.842 | 0.855 | 0.857 | |
| ResNet152V2 | 0.815 | 0.819 | 0.810 | 0.813 | 0.815 | |
| MobileNetV2 | 0.678 | 0.714 | 0.666 | 0.675 | 0.678 | |
| DenseNet201 | 0.912 | 0.911 | 0.912 | 0.912 | 0.912 | |
| Colonoscopy | VGG16 | 0.987 | 0.997 | 0.977 | 0.987 | 0.987 |
| VGG19 | 0.982 | 0.994 | 0.971 | 0.982 | 0.982 | |
| ResNet152V2 | 0.964 | 0.978 | 0.950 | 0.963 | 0.964 | |
| MobileNetV2 | 0.945 | 0.992 | 0.895 | 0.942 | 0.945 | |
| DenseNet201 | 0.991 | 0.998 | 0.984 | 0.991 | 0.991 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhazmi, W.; Turki, T. Applying Deep Transfer Learning to Assess the Impact of Imaging Modalities on Colon Cancer Detection. Diagnostics 2023, 13, 1721. https://doi.org/10.3390/diagnostics13101721
Alhazmi W, Turki T. Applying Deep Transfer Learning to Assess the Impact of Imaging Modalities on Colon Cancer Detection. Diagnostics. 2023; 13(10):1721. https://doi.org/10.3390/diagnostics13101721
Chicago/Turabian StyleAlhazmi, Wael, and Turki Turki. 2023. "Applying Deep Transfer Learning to Assess the Impact of Imaging Modalities on Colon Cancer Detection" Diagnostics 13, no. 10: 1721. https://doi.org/10.3390/diagnostics13101721