
Ischiofemoral Impingement Syndrome: Clinical and Imaging/Guidance Issues with Special Focus on Ultrasonography
 , , , , , and
, , , , , and 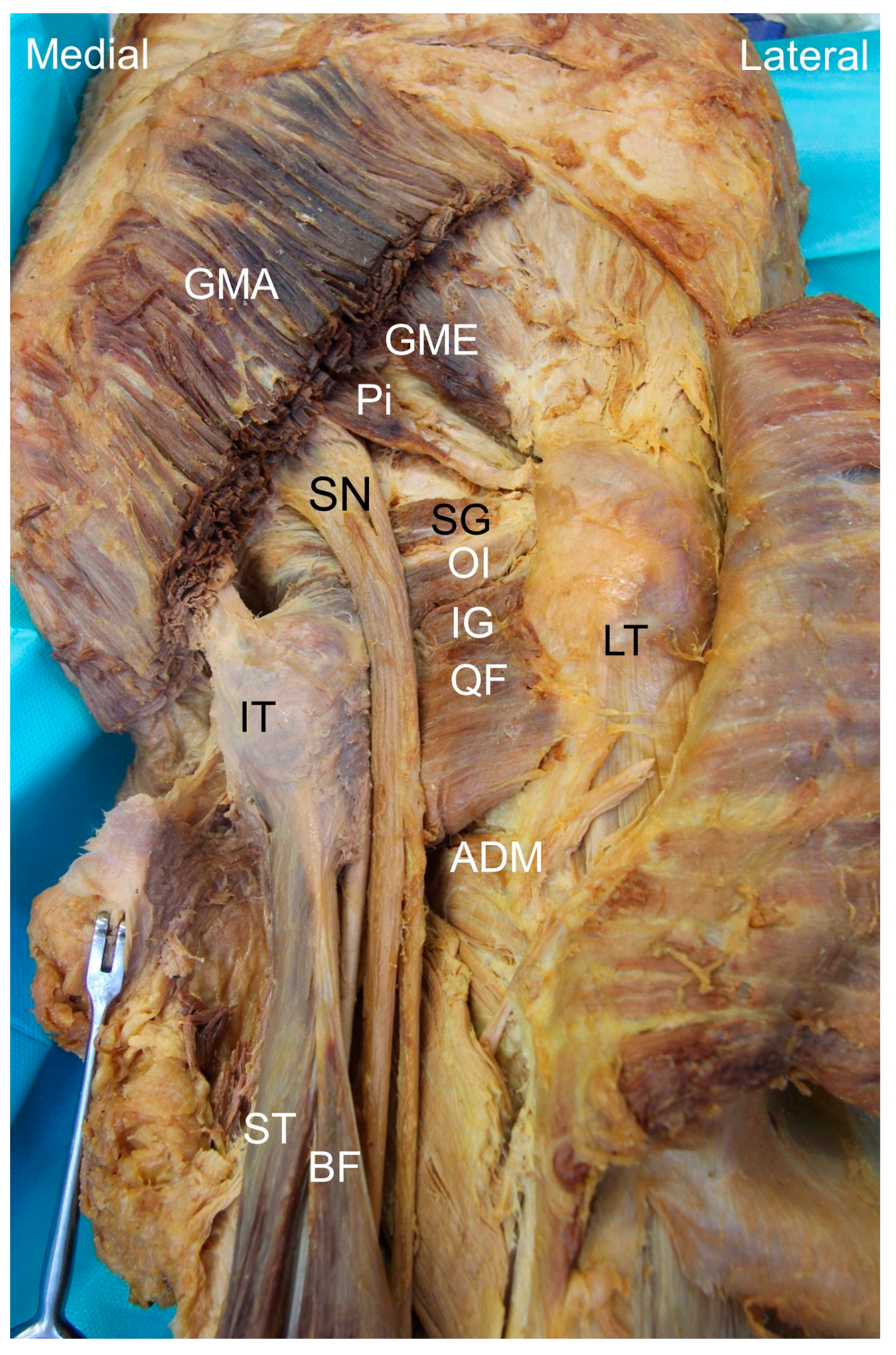{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
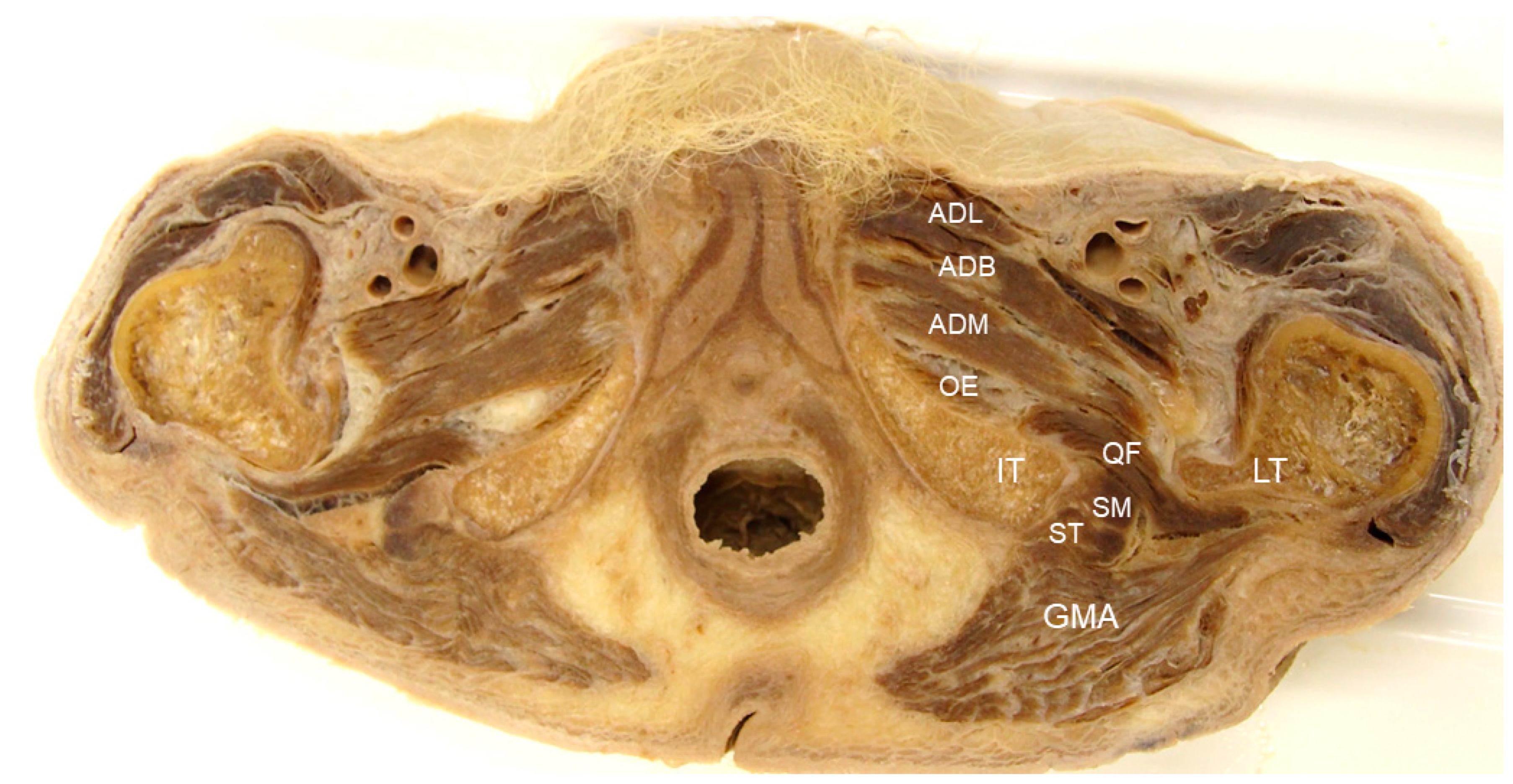
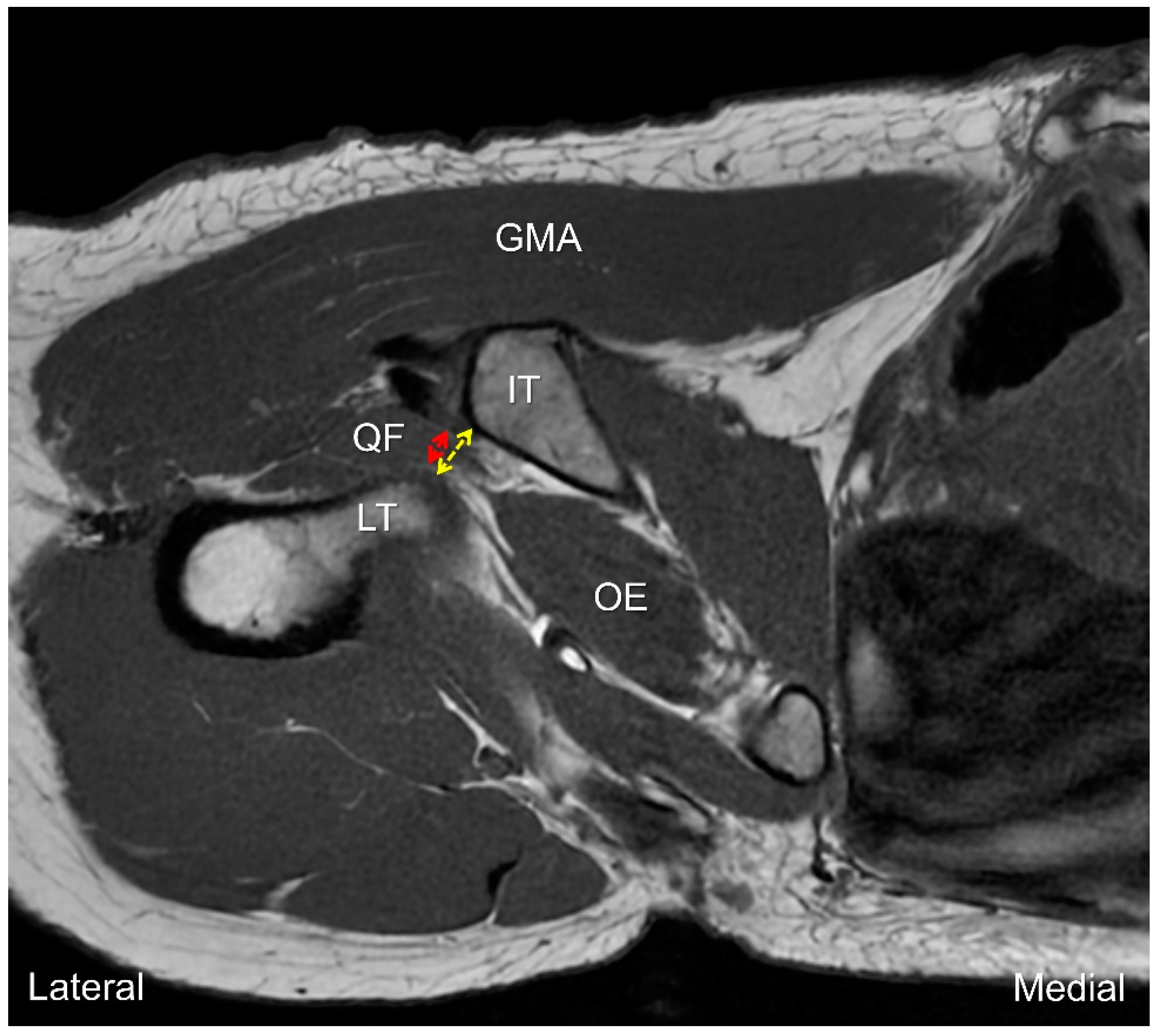
2. Anatomy
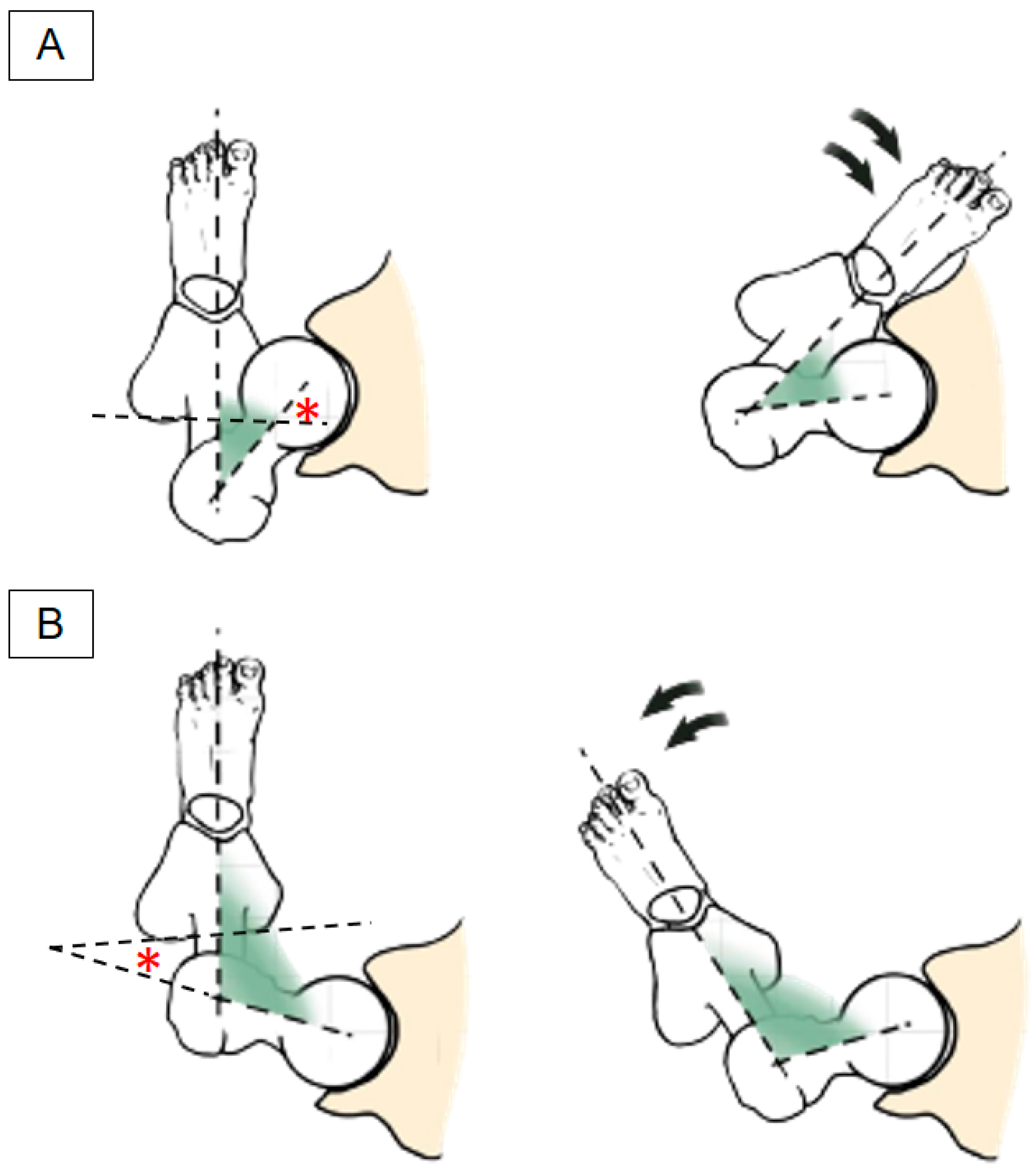
3. Biomechanics
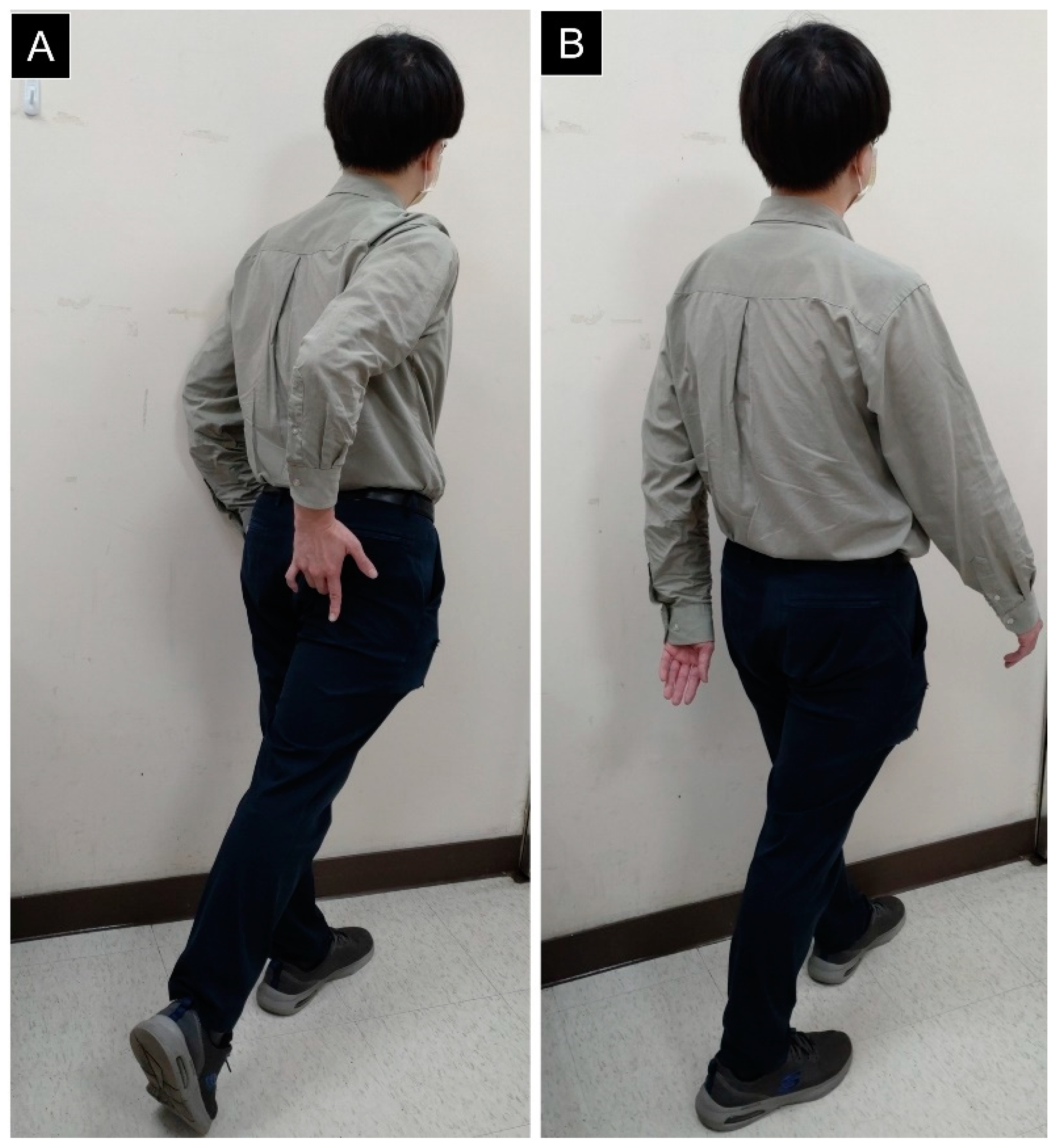
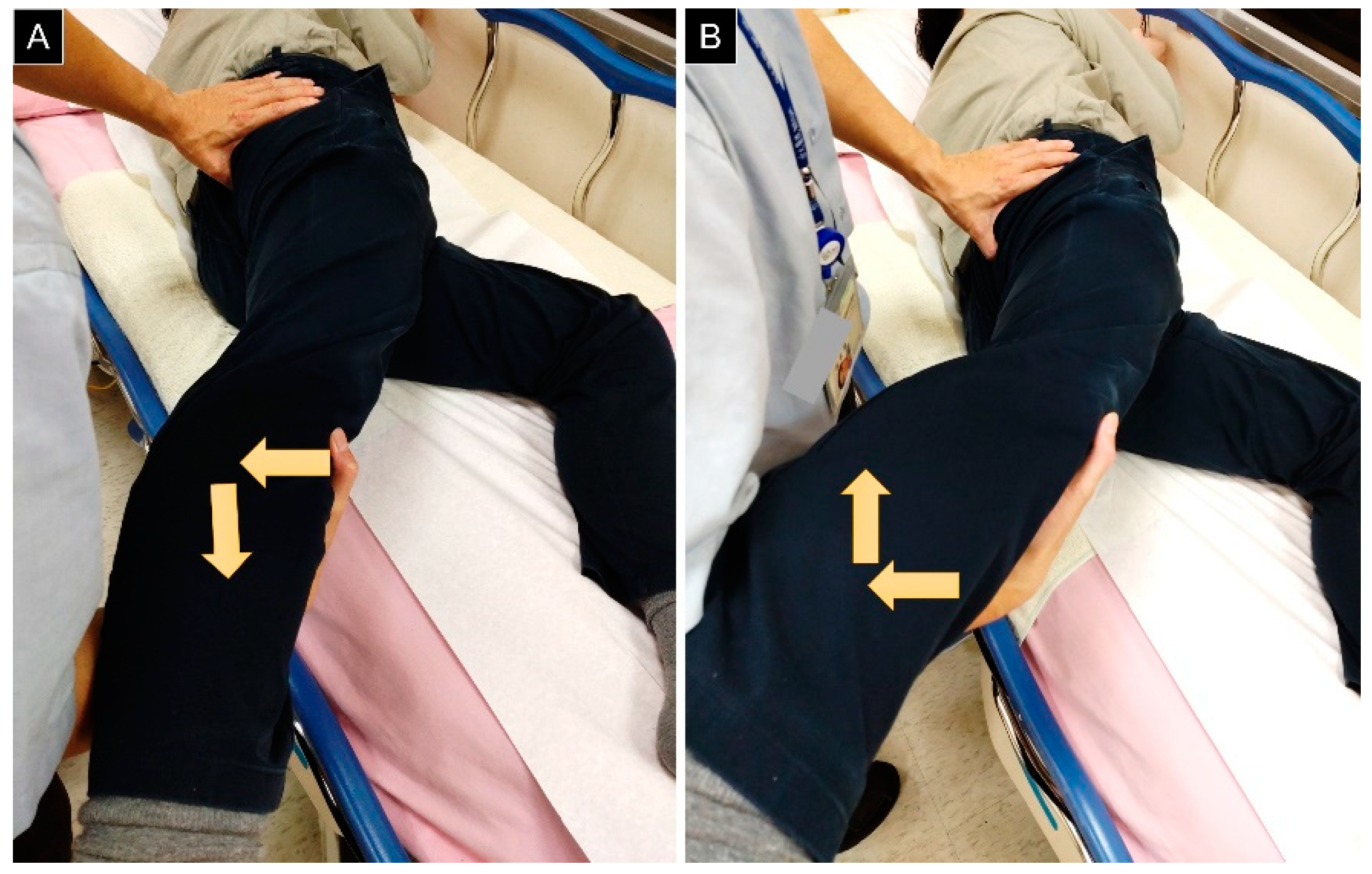
4. Physical Examination
5. Clinical Manifestations
6. Differential Diagnosis
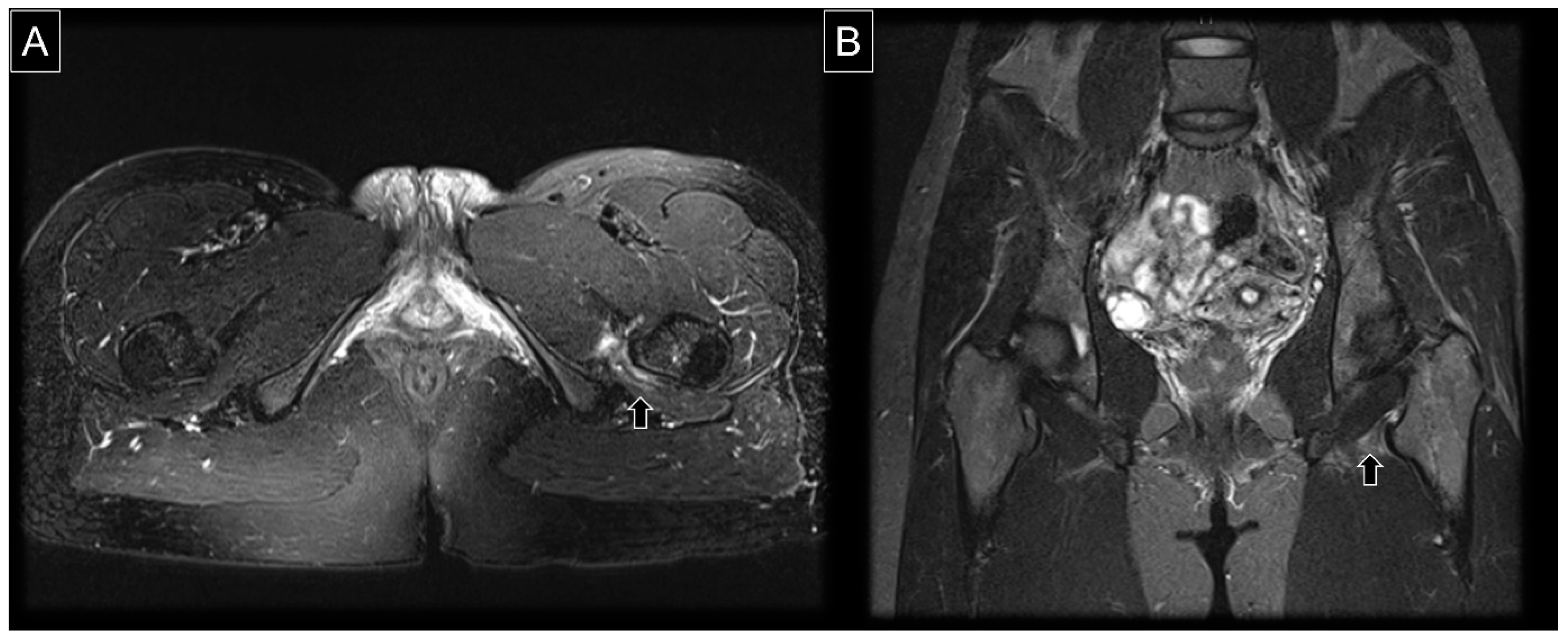
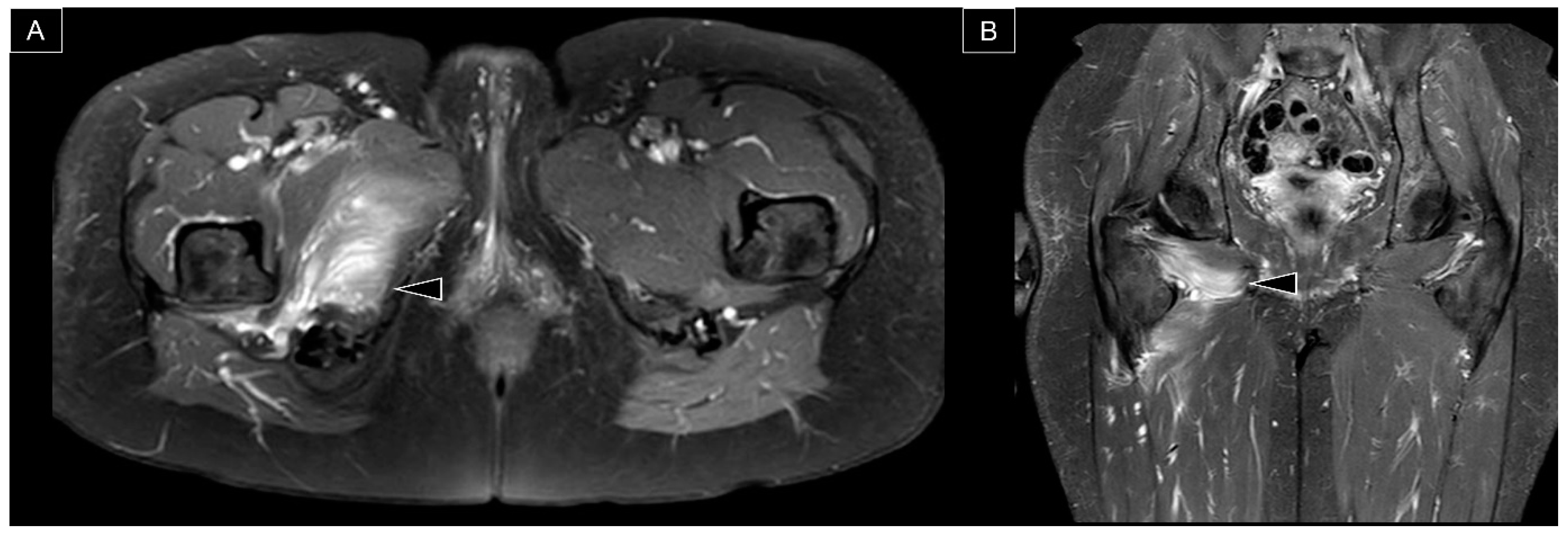
7. MRI Assessment
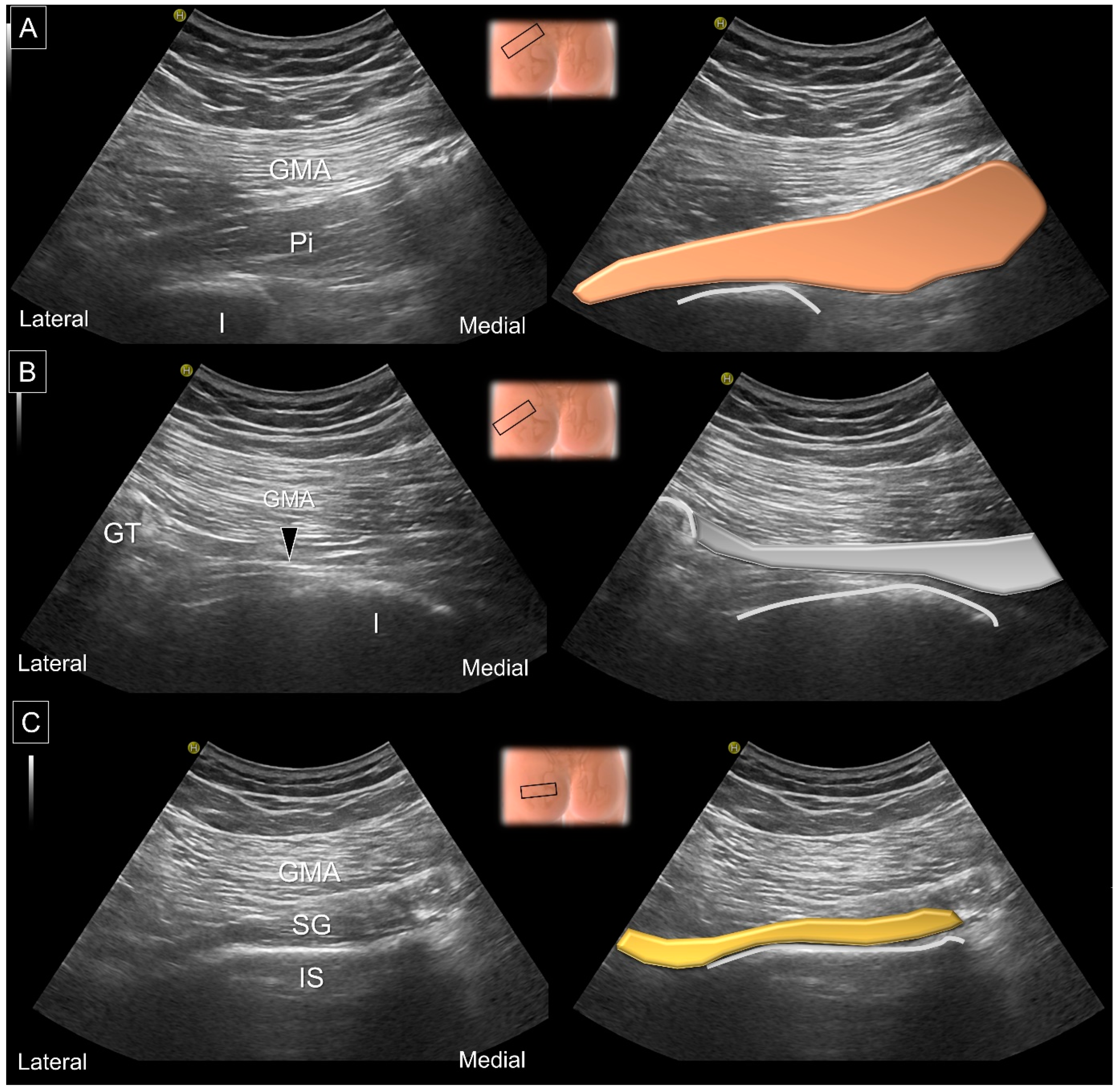
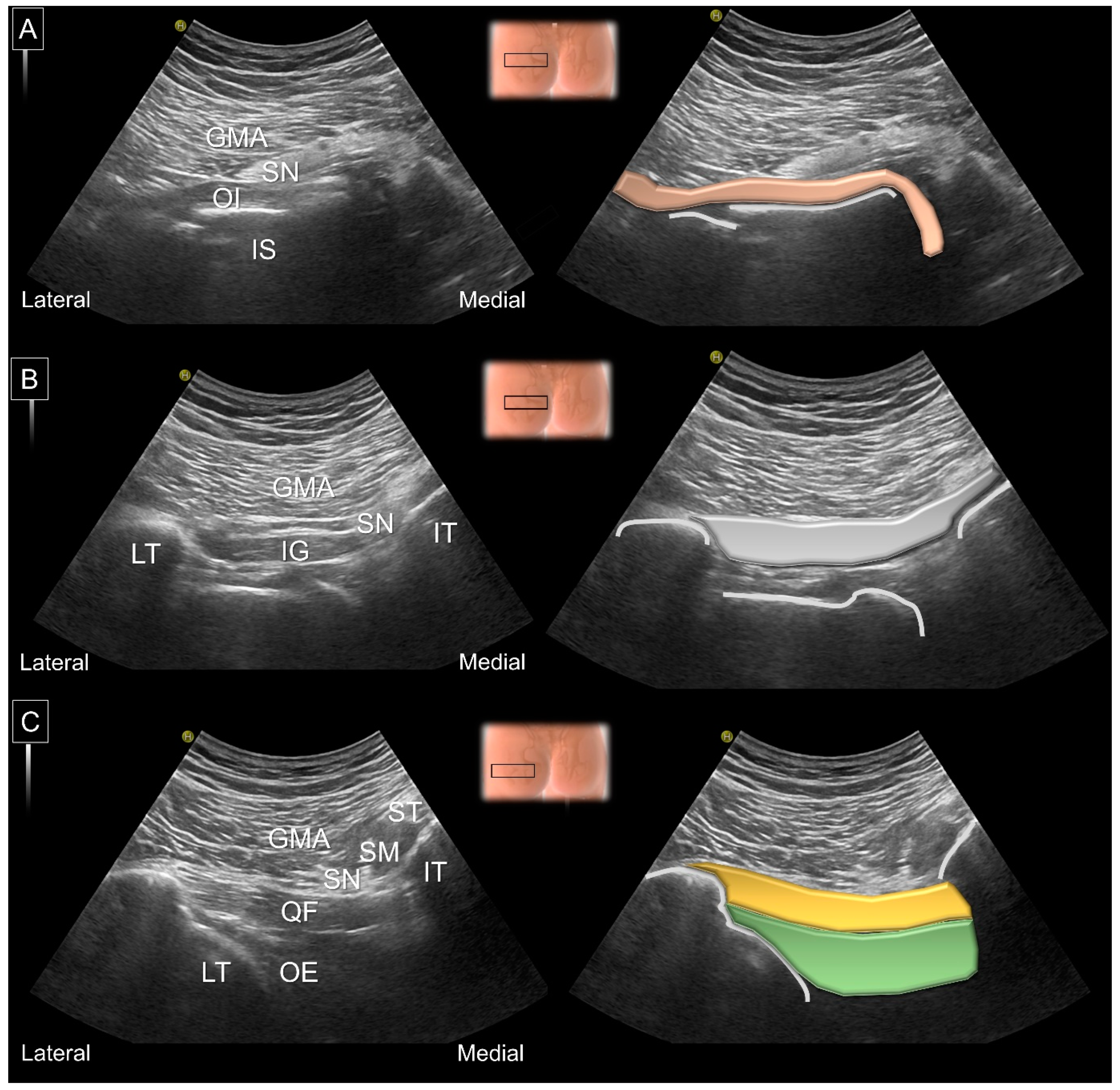
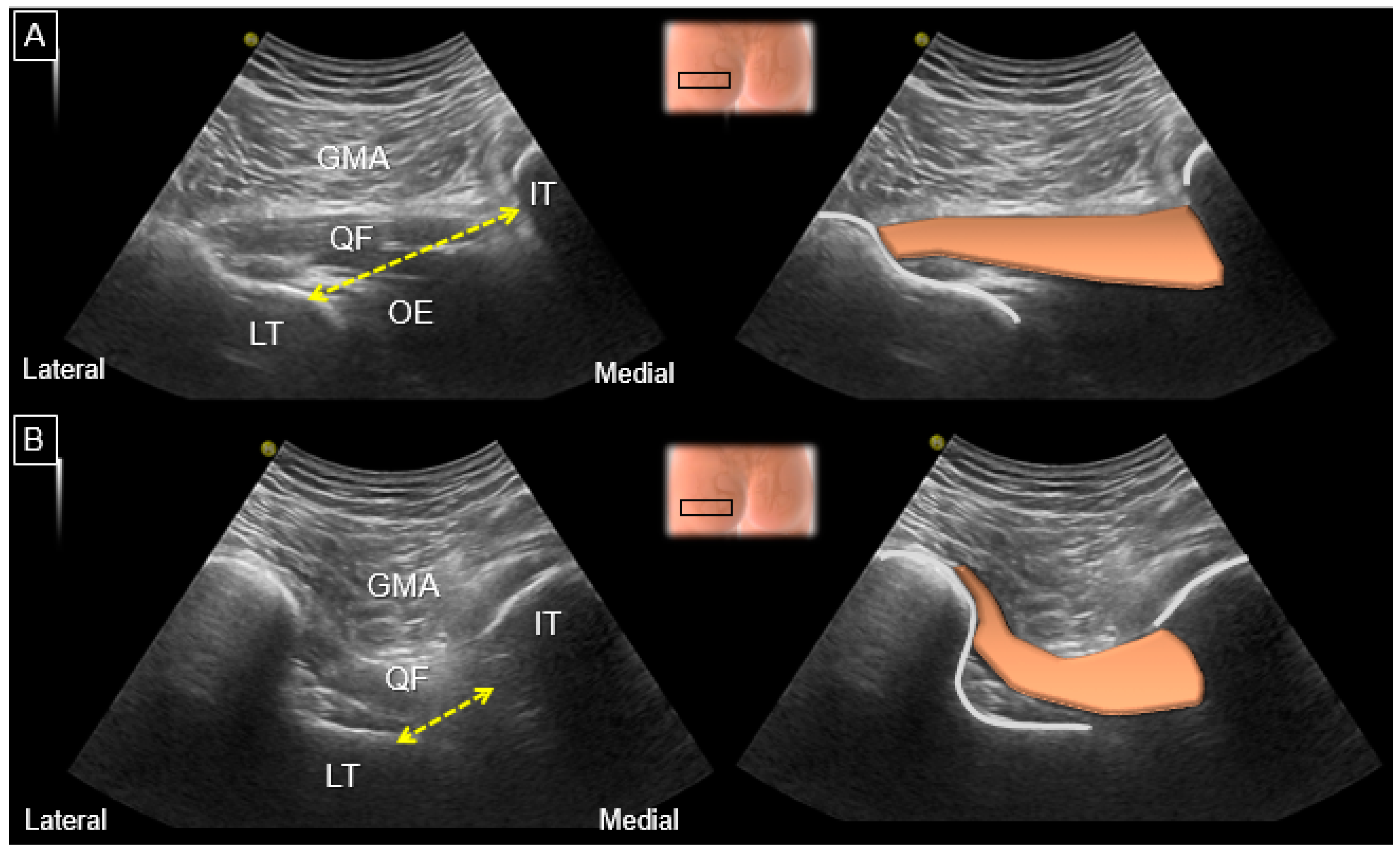
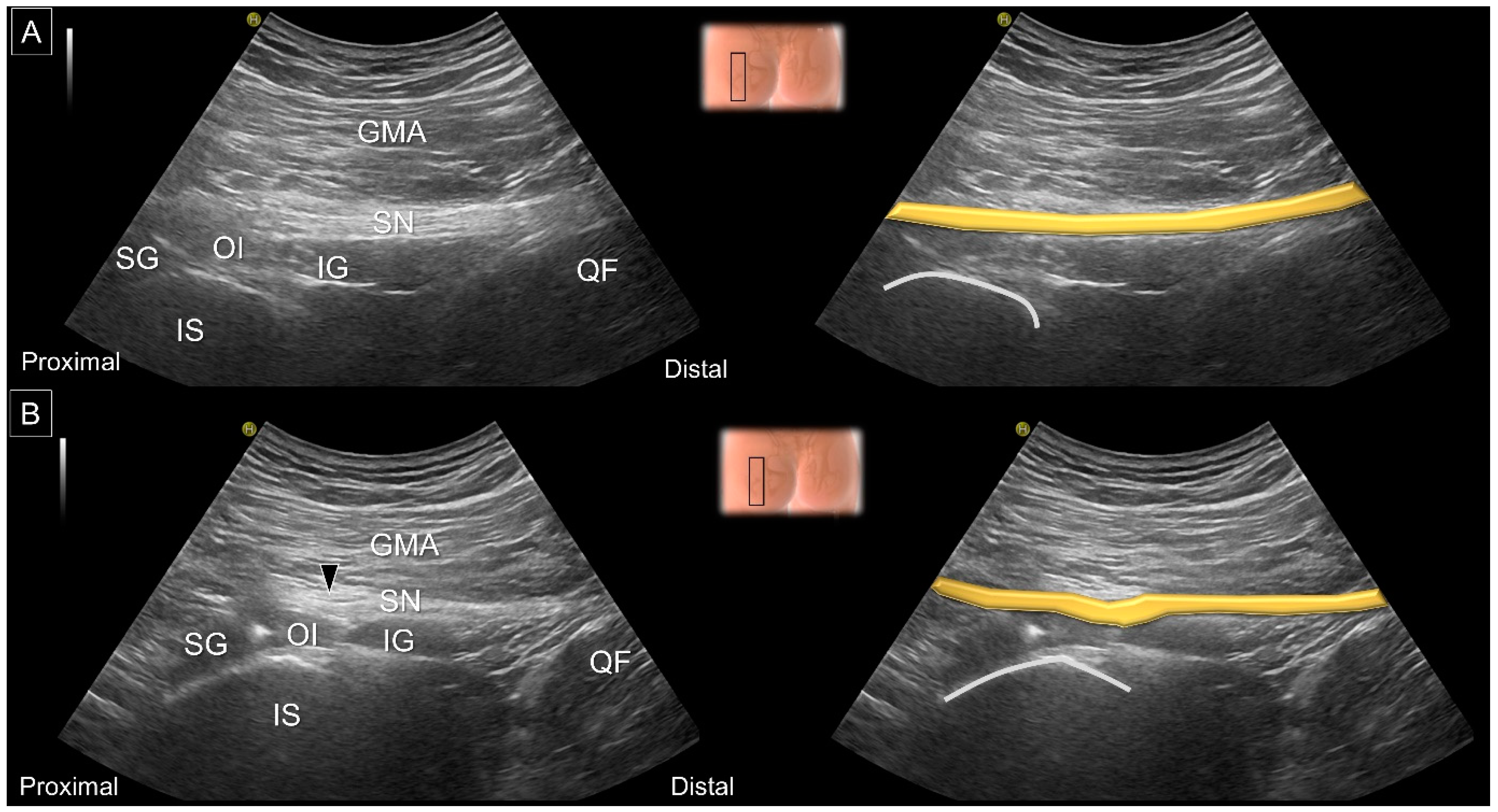
8. Dynamic Ultrasound Evaluation
9. US-Guided Intervention
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sundén-Lundius, A.; Johnsson, B.; Lohmander, S.; Ekdahl, C. Prevalence of self-reported hip disorders, relations to age, gender, pain, stiffness, weakness and other joint disorders. Adv. Physiother. 2005, 7, 108–113. [Google Scholar] [CrossRef]
- Stafford, G.H.; Villar, R.N. Ischiofemoral impingement. J. Bone Jt. Surg. Br. 2011, 93, 1300–1302. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Kim, I.; Lee, S.M.; Lee, J. Ischiofemoral impingement syndrome. Ann. Rehabil. Med. 2013, 37, 143–146. [Google Scholar] [CrossRef]
- Wu, W.T.; Lin, C.Y.; Shu, Y.C.; Chen, L.R.; Ozcakar, L.; Chang, K.V. Subacromial Motion Metrics in Painful Shoulder Impingement: A Dynamic Quantitative Ultrasonography Analysis. Arch. Phys. Med. Rehabil. 2022. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.V.; Wu, W.T.; Lew, H.L.; Ozcakar, L. Ultrasound Imaging and Guided Injection for the Lateral and Posterior Hip. Am. J. Phys. Med. Rehabil. 2018, 97, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Mezian, K.; Ricci, V.; Guvener, O.; Jacisko, J.; Novotny, T.; Kara, M.; Chang, K.V.; Nanka, O.; Pirri, C.; Stecco, C.; et al. EURO-MUSCULUS/USPRM Dynamic Ultrasound Protocols for (Adult) Hip. Am. J. Phys. Med. Rehabil. 2022, 101, e162–e168. [Google Scholar] [CrossRef] [PubMed]
- Barros, A.A.G.; Dos Santos, F.B.G.; Vassalo, C.C.; Costa, L.P.; Couto, S.G.P.; Soares, A. Evaluation of the ischiofemoral space: A case-control study. Radiol. Bras. 2019, 52, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Aung, H.H.; Sakamoto, H.; Akita, K.; Sato, T. Anatomical study of the obturator internus, gemelli and quadratus femoris muscles with special reference to their innervation. Anat. Rec. 2001, 263, 41–52. [Google Scholar] [CrossRef]
- Ransom, A.L.; Sinkler, M.A.; Nallamothu, S.V. Anatomy, Bony Pelvis and Lower Limb, Femoral Muscles. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Balius, R.; Pedret, C.; Iriarte, I.; Sáiz, R.; Cerezal, L. Sonographic landmarks in hamstring muscles. Skelet. Radiol. 2019, 48, 1675–1683. [Google Scholar] [CrossRef] [Green Version]
- Scorcelletti, M.; Reeves, N.D.; Rittweger, J.; Ireland, A. Femoral anteversion: Significance and measurement. J. Anat. 2020, 237, 811–826. [Google Scholar] [CrossRef]
- Cibulka, M.T. Determination and Significance of Femoral Neck Anteversion. Phys. Ther. 2004, 84, 550–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meier, M.K.; Reche, J.; Schmaranzer, F.; von Tengg-Kobligk, H.; Steppacher, S.D.; Tannast, M.; Novais, E.N.; Lerch, T.D. How frequent is absolute femoral retroversion in symptomatic patients with cam- and pincer-type femoroacetabular impingement? Bone Jt. Open 2022, 3, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.V.; Wu, W.T.; Ozcakar, L. Ultrasound Imaging and Rehabilitation of Muscle Disorders: Part 1. Traumatic Injuries. Am. J. Phys. Med. Rehabil. 2019, 98, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Hoyos, J.; Schröder, R.; Reddy, M.; Palmer, I.J.; Martin, H.D. Femoral Neck Anteversion and Lesser Trochanteric Retroversion in Patients With Ischiofemoral Impingement: A Case-Control Magnetic Resonance Imaging Study. Arthroscopy 2016, 32, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Hoyos, J.; Martin, R.L.; Schröder, R.; Palmer, I.J.; Martin, H.D. Accuracy of 2 Clinical Tests for Ischiofemoral Impingement in Patients With Posterior Hip Pain and Endoscopically Confirmed Diagnosis. Arthroscopy 2016, 32, 1279–1284. [Google Scholar] [CrossRef] [PubMed]
- Maraş Özdemir, Z.; Yıldırım, T.; Karaca, L.; Sağır Kahraman, A.; Aydıngöz, Ü. A Novel Physical Examination Test for Ischiofemoral Impingement: Validation With Magnetic Resonance Imaging Correlation. J. Comput. Assist. Tomogr. 2021, 45, 722–727. [Google Scholar] [CrossRef] [PubMed]
- Shanmugaraj, A.; Shell, J.R.; Horner, N.S.; Duong, A.; Simunovic, N.; Uchida, S.; Ayeni, O.R. How Useful Is the Flexion-Adduction-Internal Rotation Test for Diagnosing Femoroacetabular Impingement: A Systematic Review. Clin. J. Sport Med. 2020, 30, 76–82. [Google Scholar] [CrossRef]
- Gómez-Hoyos, J.; Khoury, A.; Schröder, R.; Johnson, E.; Palmer, I.J.; Martin, H.D. The Hip-Spine Effect: A Biomechanical Study of Ischiofemoral Impingement Effect on Lumbar Facet Joints. Arthroscopy 2017, 33, 101–107. [Google Scholar] [CrossRef]
- Martin, H.D.; Reddy, M.; Gómez-Hoyos, J. Deep gluteal syndrome. J. Hip Preserv. Surg. 2015, 2, 99–107. [Google Scholar] [CrossRef] [Green Version]
- Martin, H.D.; Khoury, A.; Schröder, R.; Palmer, I.J. Ischiofemoral Impingement and Hamstring Syndrome as Causes of Posterior Hip Pain: Where Do We Go Next? Clin. Sport. Med. 2016, 35, 469–486. [Google Scholar] [CrossRef]
- Akça, A.; Şafak, K.Y.; İliş, E.D.; Taşdemir, Z.; Baysal, T. Ischiofemoral Impingement: Assessment of Mri Findings and Their Reliability. Acta Ortop. Bras. 2016, 24, 318–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singer, A.D.; Subhawong, T.K.; Jose, J.; Tresley, J.; Clifford, P.D. Ischiofemoral impingement syndrome: A meta-analysis. Skelet. Radiol. 2015, 44, 831–837. [Google Scholar] [CrossRef]
- Tosun, O.; Algin, O.; Yalcin, N.; Cay, N.; Ocakoglu, G.; Karaoglanoglu, M. Ischiofemoral impingement: Evaluation with new MRI parameters and assessment of their reliability. Skelet. Radiol. 2012, 41, 575–587. [Google Scholar] [CrossRef]
- Papavasiliou, K.A.; Stamiris, D.; Stamiris, S.; Bintoudi, A.; Tsiridis, E. Quadratus Femoris Partial Tear Secondary to Occult Ischiofemoral Impingement. J. Orthop. Case Rep. 2021, 11, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Chua, E.; Shah, D. Hydroxyapatite crystal deposition disease around the hip: A rare cause of piriformis syndrome and ischiofemoral impingement. BJR Case Rep. 2022, 7, 20210075. [Google Scholar] [CrossRef] [PubMed]
- Hayat, Z.; Konan, S.; Pollock, R. Ischiofemoral impingement resulting from a chronic avulsion injury of the hamstrings. BMJ Case Rep. 2014, 2014, bcr2014204017. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Cheng, X.; Tian, C.; Wang, R.; Chen, J.; Zhang, X.; Zeng, X. Cinematic rendering for ischiofemoral impingement syndrome caused by osteochondroma: A case description. Quant. Imaging Med. Surg. 2022, 12, 1647–1651. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, P.J.; Mattox, R.; Haun, D.W.; Welk, A.B.; Kettner, N.W. Dynamic Ultrasonography of the Deep External Rotator Musculature of the Hip: A Descriptive Study. PM&R 2016, 8, 640–650. [Google Scholar] [CrossRef]
- Chang, K.V.; Wu, W.T.; Mezian, K.; Nanka, O.; Ozcakar, L. Letter to the Editor Regarding “Feasibility and Reliability of an Ultrasound Examination to Diagnose Piriformis Syndrome”. World Neurosurg. 2020, 137, 483–484. [Google Scholar] [CrossRef] [PubMed]
- Boettcher, B.J.; Hollman, J.H.; Payne, J.M.; Johnson, A.C.; Finnoff, J.T. Can a Brief Training Session Prepare Physician Sonographers of Differing Experience to Measure the Ischiofemoral Space? A Reliability Study. PM&R 2019, 11, 142–149. [Google Scholar] [CrossRef]
- Finnoff, J.T.; Johnson, A.C.; Hollman, J.H. Can Ultrasound Accurately Assess Ischiofemoral Space Dimensions? A Validation Study. PM&R 2017, 9, 392–397. [Google Scholar] [CrossRef]
- Lu, B.; Deng, H.; Chen, B.; Zhao, J. The accuracy assessment of ultrasound for the diagnosis of ischiofemoral space-A Validation Study. J. X-ray Sci. Technol. 2019, 27, 605–614. [Google Scholar] [CrossRef] [PubMed]
- Balius, R.; Susín, A.; Morros, C.; Pujol, M.; Pérez-Cuenca, D.; Sala-Blanch, X. Gemelli-obturator complex in the deep gluteal space: An anatomic and dynamic study. Skelet. Radiol. 2018, 47, 763–770. [Google Scholar] [CrossRef] [PubMed]
- Gollwitzer, H.; Banke, I.J.; Schauwecker, J.; Gerdesmeyer, L.; Suren, C. How to address ischiofemoral impingement? Treatment algorithm and review of the literature. J. Hip Preserv. Surg. 2017, 4, 289–298. [Google Scholar] [CrossRef] [Green Version]
- Volokhina, Y.; Dang, D. Using proximal hamstring tendons as a landmark for ultrasound- and CT-guided injections of ischiofemoral impingement. Radiol. Case Rep. 2013, 8, 789. [Google Scholar] [CrossRef] [Green Version]
- Backer, M.W.; Lee, K.S.; Blankenbaker, D.G.; Kijowski, R.; Keene, J.S. Correlation of ultrasound-guided corticosteroid injection of the quadratus femoris with MRI findings of ischiofemoral impingement. AJR Am. J. Roentgenol. 2014, 203, 589–593. [Google Scholar] [CrossRef]
- Kim, W.J.; Shin, H.Y.; Koo, G.H.; Park, H.G.; Ha, Y.C.; Park, Y.H. Ultrasound-guided Prolotherapy with Polydeoxyribonucleotide Sodium in Ischiofemoral Impingement Syndrome. Pain Pract. 2014, 14, 649–655. [Google Scholar] [CrossRef]
- Kim, D.H.; Yoon, D.M.; Yoon, K.B. Ultrasound-Guided Quadratus Femoris Muscle Injection in Patients with Lower Buttock Pain: Novel Ultrasound-Guided Approach and Clinical Effectiveness. Pain Physician 2016, 19, E863–E870. [Google Scholar]
- Chen, Y.T.; Jenkins, K.M. Ultrasound Finding of Ischiofemoral Impingement Syndrome and Novel Treatment with Botulinum Toxin Chemodenervation: A Case Report. PM&R 2018, 10, 665–670. [Google Scholar] [CrossRef]














Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, W.-T.; Chang, K.-V.; Mezian, K.; Naňka, O.; Ricci, V.; Chang, H.-C.; Wang, B.; Hung, C.-Y.; Özçakar, L. Ischiofemoral Impingement Syndrome: Clinical and Imaging/Guidance Issues with Special Focus on Ultrasonography. Diagnostics 2023, 13, 139. https://doi.org/10.3390/diagnostics13010139
Wu W-T, Chang K-V, Mezian K, Naňka O, Ricci V, Chang H-C, Wang B, Hung C-Y, Özçakar L. Ischiofemoral Impingement Syndrome: Clinical and Imaging/Guidance Issues with Special Focus on Ultrasonography. Diagnostics. 2023; 13(1):139. https://doi.org/10.3390/diagnostics13010139
Chicago/Turabian StyleWu, Wei-Ting, Ke-Vin Chang, Kamal Mezian, Ondřej Naňka, Vincenzo Ricci, Hsiang-Chi Chang, Bow Wang, Chen-Yu Hung, and Levent Özçakar. 2023. "Ischiofemoral Impingement Syndrome: Clinical and Imaging/Guidance Issues with Special Focus on Ultrasonography" Diagnostics 13, no. 1: 139. https://doi.org/10.3390/diagnostics13010139