
Association between High-Sensitivity Cardiac Troponin I and Clinical Prognosis of Neurosurgical and Neurocritically Ill Patients

Abstract
:1. Background
2. Methods
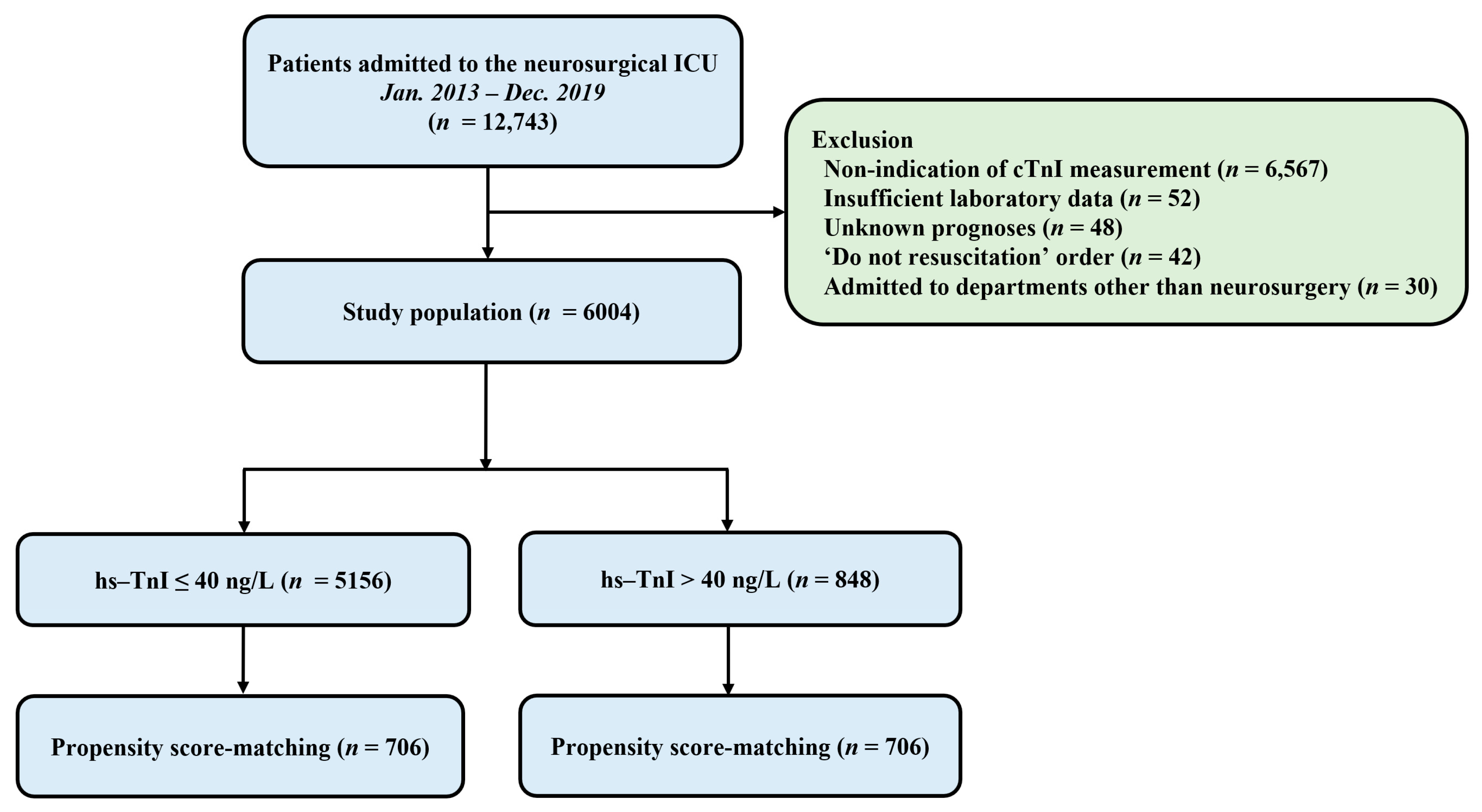
2.1. Study Population
2.2. Definitions and Endpoints
2.3. Statistical Analyses
3. Results
3.1. Baseline Characteristics
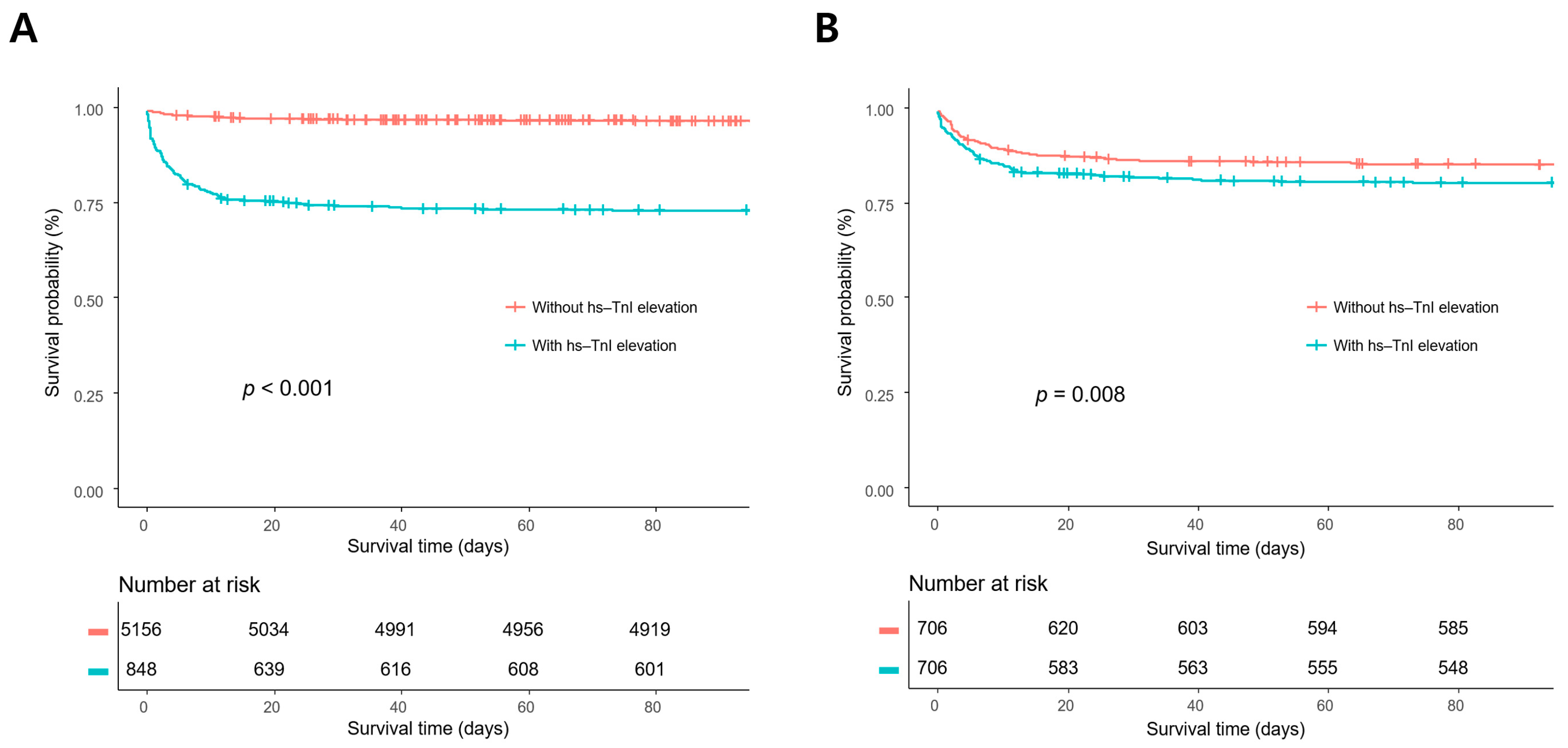
3.2. Clinical Outcomes
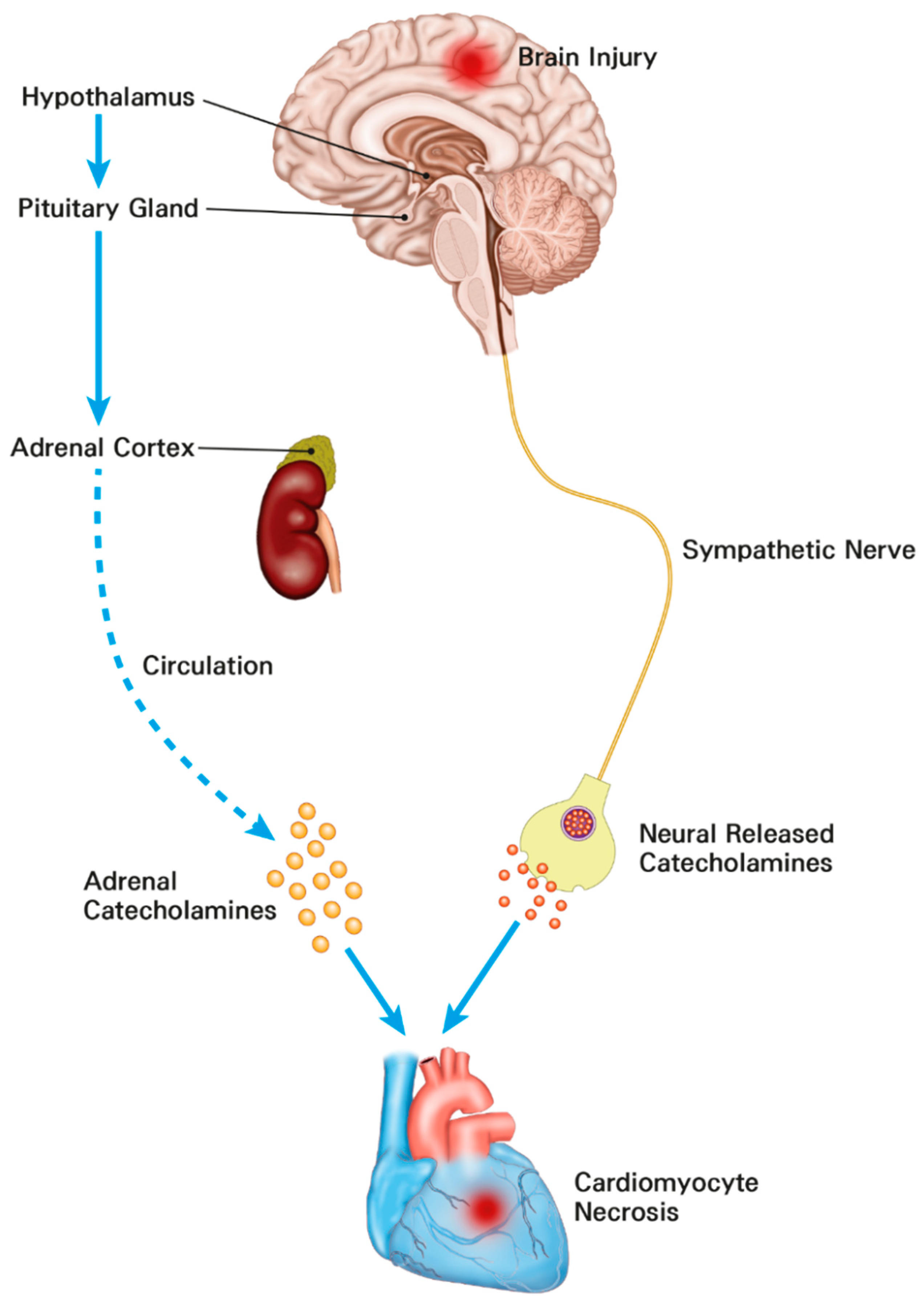
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Ekeloef, S.; Alamili, M.; Devereaux, P.J.; Gogenur, I. Troponin elevations after non-cardiac, non-vascular surgery are predictive of major adverse cardiac events and mortality: A systematic review and meta-analysis. Br. J. Anaesth. 2016, 117, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Oscarsson, A.; Fredrikson, M.; Sorliden, M.; Anskar, S.; Gupta, A.; Swahn, E.; Eintrei, C. Predictors of cardiac events in high-risk patients undergoing emergency surgery. Acta Anaesthesiol. Scand. 2009, 53, 986–994. [Google Scholar] [CrossRef]
- Devereaux, P.J.; Xavier, D.; Pogue, J.; Guyatt, G.; Sigamani, A.; Garutti, I.; Leslie, K.; Rao-Melacini, P.; Chrolavicius, S.; Yang, H.; et al. Characteristics and short-term prognosis of perioperative myocardial infarction in patients undergoing noncardiac surgery: A cohort study. Ann. Intern. Med. 2011, 154, 523–528. [Google Scholar] [CrossRef]
- Devereaux, P.J.; Mrkobrada, M.; Sessler, D.I.; Leslie, K.; Alonso-Coello, P.; Kurz, A.; Villar, J.C.; Sigamani, A.; Biccard, B.M.; Meyhoff, C.S.; et al. Aspirin in patients undergoing noncardiac surgery. N. Engl. J. Med. 2014, 370, 1494–1503. [Google Scholar] [CrossRef] [PubMed]
- Devereaux, P.J.; Chan, M.T.; Alonso-Coello, P.; Walsh, M.; Berwanger, O.; Villar, J.C.; Wang, C.Y.; Garutti, R.I.; Jacka, M.J.; Sigamani, A.; et al. Association between postoperative troponin levels and 30-day mortality among patients undergoing noncardiac surgery. JAMA 2012, 307, 2295–2304. [Google Scholar] [PubMed]
- Lim, W.; Qushmaq, I.; Devereaux, P.J.; Heels-Ansdell, D.; Lauzier, F.; Ismaila, A.S.; Crowther, M.A.; Cook, D.J. Elevated cardiac troponin measurements in critically ill patients. Arch. Intern. Med. 2006, 166, 2446–2454. [Google Scholar] [CrossRef]
- Omland, T.; de Lemos, J.A.; Sabatine, M.S.; Christophi, C.A.; Rice, M.M.; Jablonski, K.A.; Tjora, S.; Domanski, M.J.; Gersh, B.J.; Rouleau, J.L.; et al. A sensitive cardiac troponin T assay in stable coronary artery disease. N. Engl. J. Med. 2009, 361, 2538–2547. [Google Scholar] [CrossRef]
- Ford, I.; Shah, A.S.; Zhang, R.; McAllister, D.A.; Strachan, F.E.; Caslake, M.; Newby, D.E.; Packard, C.J.; Mills, N.L. High-Sensitivity Cardiac Troponin, Statin Therapy, and Risk of Coronary Heart Disease. J. Am. Coll. Cardiol. 2016, 68, 2719–2728. [Google Scholar] [CrossRef]
- Park, J.; Hyeon, C.W.; Lee, S.H.; Kim, J.; Kwon, J.H.; Yang, K.; Min, J.J.; Lee, J.H.; Lee, S.M.; Yang, J.H.; et al. Mildly Elevated Cardiac Troponin below the 99th-Percentile Upper Reference Limit after Noncardiac Surgery. Korean Circ. J. 2020, 50, 925–937. [Google Scholar] [CrossRef]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Group, E.S.D. Fourth universal definition of myocardial infarction. Eur. Heart J. 2018, 40, 237–269. [Google Scholar] [CrossRef] [PubMed]
- Chaulin, A. Cardiac Troponins: Contemporary Biological Data and New Methods of Determination. Vasc. Health Risk Manag. 2021, 17, 299–316. [Google Scholar] [CrossRef] [PubMed]
- Clerico, A.; Zaninotto, M.; Padoan, A.; Masotti, S.; Musetti, V.; Prontera, C.; Ndreu, R.; Zucchelli, G.; Passino, C.; Migliardi, M.; et al. Evaluation of analytical performance of immunoassay methods for cTnI and cTnT: From theory to practice. Adv. Clin. Chem. 2019, 93, 239–262. [Google Scholar] [PubMed]
- Chaulin, A.M. Cardiac Troponins Metabolism: From Biochemical Mechanisms to Clinical Practice (Literature Review). Int. J. Mol. Sci. 2021, 22, 10928. [Google Scholar] [CrossRef]
- Garrett, M.C.; Komotar, R.J.; Starke, R.M.; Doshi, D.; Otten, M.L.; Connolly, E.S. Elevated troponin levels are predictive of mortality in surgical intracerebral hemorrhage patients. Neurocrit. Care 2010, 12, 199–203. [Google Scholar] [CrossRef]
- Connor, R.C. Myocardial damage secondary to brain lesions. Am. Heart J. 1969, 78, 145–148. [Google Scholar] [CrossRef]
- Doshi, R.; Neil-Dwyer, G. Hypothalamic and myocardial lesions after subarachnoid haemorrhage. J. Neurol. Neurosurg. Psychiatry 1977, 40, 821–826. [Google Scholar] [CrossRef]
- Zaroff, J.G.; Rordorf, G.A.; Ogilvy, C.S.; Picard, M.H. egional patterns of left ventricular systolic dysfunction after subarachnoid hemorrhage: Evidence for neurally mediated cardiac injury. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2000, 13, 774–779. [Google Scholar] [CrossRef]
- Naidech, A.M.; Kreiter, K.T.; Janjua, N.; Ostapkovich, N.D.; Parra, A.; Commichau, C.; Fitzsimmons, B.F.; Connolly, E.S.; Mayer, S.A. Cardiac troponin elevation, cardiovascular morbidity, and outcome after subarachnoid hemorrhage. Circulation 2005, 112, 2851–2856. [Google Scholar] [CrossRef]
- Kristensen, S.D.; Knuuti, J. New ESC/ESA Guidelines on non-cardiac surgery: Cardiovascular assessment and management. Eur. Heart J. 2014, 35, 2344–2345. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Capuzzo, M.; Valpondi, V.; Sgarbi, A.; Bortolazzi, S.; Pavoni, V.; Gilli, G.; Candini, G.; Gritti, G.; Alvisi, R. Validation of severity scoring systems SAPS II and APACHE II in a single-center population. Intensive Care Med. 2000, 26, 1779–1785. [Google Scholar] [CrossRef] [PubMed]
- Meredith, W.; Rutledge, R.; Fakhry, S.M.; Emery, S.; Kromhout-Schiro, S. The conundrum of the Glasgow Coma Scale in intubated patients: A linear regression prediction of the Glasgow verbal score from the Glasgow eye and motor scores. J. Trauma 1998, 44, 839–845. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm. Stat. 2011, 10, 150–161. [Google Scholar] [CrossRef]
- Adams, J.E., 3rd; Abendschein, D.R.; Jaffe, A.S. Biochemical markers of myocardial injury. Is MB creatine kinase the choice for the 1990s? Circulation 1993, 88, 750–763. [Google Scholar] [CrossRef]
- Noordzij, P.G.; van Geffen, O.; Dijkstra, I.M.; Boerma, D.; Meinders, A.J.; Rettig, T.C.; Eefting, F.D.; van Loon, D.; van de Garde, E.M.; van Dongen, E.P. High-sensitive cardiac troponin T measurements in prediction of non-cardiac complications after major abdominal surgery. Br. J. Anaesth. 2015, 114, 909–918. [Google Scholar] [CrossRef]
- Gillies, M.A.; Shah, A.S.; Mullenheim, J.; Tricklebank, S.; Owen, T.; Antonelli, J.; Strachan, F.; Mills, N.L.; Pearse, R.M. Perioperative myocardial injury in patients receiving cardiac output-guided haemodynamic therapy: A substudy of the OPTIMISE Trial. Br. J. Anaesth. 2015, 115, 227–233. [Google Scholar] [CrossRef]
- Rimaz, S.; Ashraf, A.; Marzban, S.; Haghighi, M.; Zia Ziabari, S.M.; Biazar, G.; Rimaz, S.; Omidi, S. Significance of Cardiac Troponin I Elevation in Traumatic Brain Injury Patients. Anesth. Pain Med. 2019, 9, e90858. [Google Scholar] [CrossRef]
- Chen, Z.; Venkat, P.; Seyfried, D.; Chopp, M.; Yan, T.; Chen, J. Brain-Heart Interaction: Cardiac Complications After Stroke. Circ. Res. 2017, 121, 451–468. [Google Scholar] [CrossRef]
- Todd, G.L.; Baroldi, G.; Pieper, G.M.; Clayton, F.C.; Eliot, R.S. Experimental catecholamine-induced myocardial necrosis. I. Morphology, quantification and regional distribution of acute contraction band lesions. J. Mol. Cell. Cardiol. 1985, 17, 317–338. [Google Scholar] [CrossRef]
- Ibrahim, M.S.; Samuel, B.; Mohamed, W.; Suchdev, K. Cardiac Dysfunction in Neurocritical Care: An Autonomic Perspective. Neurocrit. Care 2019, 30, 508–521. [Google Scholar] [CrossRef] [PubMed]
- Samuels, M.A. Neurogenic heart disease: A unifying hypothesis. Am. J. Cardiol. 1987, 60, 15j–19j. [Google Scholar] [CrossRef]
- Samuels, M.A. The brain-heart connection. Circulation 2007, 116, 77–84. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Overall Study Population | Propensity Score-Matched Population | |||||||
|---|---|---|---|---|---|---|---|---|
| No Elevation (n = 5156) | Elevation (n = 848) | p Value | SMD | No Elevation (n = 706) | Elevation (n = 706) | p Value | SMD | |
| Patient demographics | ||||||||
| Age (year) | 54.7 ± 15.3 | 62.1 ± 15.9 | <0.001 | 0.471 | 62.0 ± 14.6 | 61.8 ± 16.0 | 0.770 | 0.016 |
| Sex, male | 2266 (43.9) | 432 (50.9) | <0.001 | 0.14 | 349 (49.4) | 366 (51.8) | 0.394 | 0.048 |
| Comorbidities | ||||||||
| Malignancy | 2657 (51.5) | 373 (44.0) | <0.001 | 0.152 | 350 (49.6) | 344 (48.7) | 0.790 | 0.017 |
| Hypertension | 1678 (32.5) | 412 (48.6) | <0.001 | 0.331 | 341 (48.3) | 347 (49.2) | 0.790 | 0.017 |
| Diabetes mellitus | 567 (11.0) | 162 (19.1) | <0.001 | 0.228 | 111 (15.7) | 141 (20.0) | 0.044 | 0.111 |
| Chronic kidney disease | 154 (3.0) | 95 (11.2) | <0.001 | 0.324 | 61 (8.6) | 69 (9.8) | 0.519 | 0.039 |
| Cardiovascular disease | 92 (1.8) | 88 (10.4) | <0.001 | 0.366 | 57 (8.1) | 65 (9.2) | 0.507 | 0.040 |
| Chronic liver disease | 99 (1.9) | 31 (3.7) | 0.002 | 0.106 | 24 (3.4) | 25 (3.5) | 0.999 | 0.008 |
| Behavioral risk factors | ||||||||
| Current alcohol consumption | 1257 (24.4) | 172 (20.3) | 0.011 | 0.098 | 151 (21.4) | 147 (20.8) | 0.845 | 0.014 |
| Current smoking | 577 (11.2) | 90 (10.6) | 0.662 | 0.019 | 83 (11.8) | 77 (10.9) | 0.675 | 0.027 |
| Cause of ICU admission | <0.001 | 1.132 | 0.907 | 0.098 | ||||
| Brain tumor | 1961 (38.0) | 200 (23.6) | 200 (28.3) | 196 (27.8) | ||||
| Elective vascular surgery | 2137 (41.4) | 93 (11.0) | 74 (10.5) | 93 (13.2) | ||||
| Intracerebral hemorrhage | 234 (4.5) | 160 (18.9) | 138 (19.5) | 129 (18.3) | ||||
| Traumatic brain injury | 221 (4.3) | 155 (18.3) | 122 (17.3) | 116 (16.4) | ||||
| Subarachnoid hemorrhage | 202 (3.9) | 144 (17.0) | 100 (14.2) | 100 (14.2) | ||||
| Spinal surgery | 213 (4.1) | 29 (3.4) | 25 (3.5) | 28 (4.0) | ||||
| Central nervous system infection | 41 (0.8) | 10 (1.2) | 7 (1.0) | 8 (1.1) | ||||
| Cerebral infarction | 29 (0.6) | 18 (2.1) | 18 (2.5) | 14 (2.0) | ||||
| Others | 118 (2.3) | 39 (4.6) | 22 (3.1) | 22 (3.1) | ||||
| APACHE II score on ICU admission | 3.2 ± 4.3 | 7.54 ± 7.83 | <0.001 | 0.691 | 6.0 ± 6.3 | 6.41 ±7.04 | 0.254 | 0.061 |
| Glasgow coma scale on ICU admission | 14.6 ± 1.5 | 12.2 ± 4.2 | <0.001 | 0.776 | 13.2 ± 3.3 | 13.1 ± 3.4 | 0.706 | 0.020 |
| ICU management | ||||||||
| Use of vasopressors | 112 (2.2) | 103 (12.1) | <0.001 | 0.394 | 68 (9.6) | 73 (10.3) | 0.723 | 0.024 |
| Mechanical ventilation | 775 (15.0) | 504 (59.4) | <0.001 | 1.034 | 374 (53.0) | 367 (52.0) | 0.749 | 0.020 |
| Continuous renal replacement therapy | 11 (0.2) | 46 (5.4) | <0.001 | 0.319 | 10 (1.4) | 13 (1.8) | 0.674 | 0.034 |
| ICP monitoring | 376 (7.3) | 170 (20.0) | <0.001 | 0.378 | 137 (19.4) | 139 (19.7) | 0.946 | 0.007 |
| Use of mannitol a | 2250 (43.6) | 349 (41.2) | 0.189 | 0.05 | 295 (41.8) | 286 (40.5) | 0.665 | 0.026 |
| Use of glycerin a | 508 (9.9) | 267 (31.5) | <0.001 | 0.554 | 207 (29.3) | 209 (29.6) | 0.953 | 0.006 |
| Clinical outcomes b | ||||||||
| In-hospital mortality | 158 (3.1) | 226 (26.7) | <0.001 | 102 (14.4) | 136 (19.3) | 0.019 | ||
| 28-day mortality | 144 (2.8) | 223 (26.3) | <0.001 | 93 (13.2) | 134 (19.0) | 0.004 | ||
| ICU mortality | 87 (1.7) | 163 (19.2) | <0.001 | 68 (9.6) | 83 (11.8) | 0.228 | ||
| ICU length of stay (hour) | 57.0 ± 334.2 | 131.8 ± 200.2 | <0.001 | 145.3 ± 827.1 | 132.8 ± 203.3 | 0.695 | ||
| Hospital length of stay (day) | 22.9 ± 93.9 | 45.7 ± 205.1 | <0.001 | 55.7 ± 237.7 | 38.6 ± 59.8 | 0.065 | ||
| Major adverse cardiac events b | 57 (1.1) | 56 (6.6) | <0.001 | 17 (2.4) | 56 (7.9) | <0.001 | ||
| New onset arrhythmia | 53 (1.0) | 24 (2.8) | 16 (2.3) | 24 (3.4) | ||||
| Heart failure | 2 (0.0) | 15 (1.8) | 0 (0.0) | 15 (2.1) | ||||
| Acute coronary syndrome | 1 (0.0) | 12 (1.4) | 0 (0.0) | 12 (1.7) | ||||
| Cardiac arrest | 1 (0.0) | 5 (0.6) | 1 (0.1) | 5 (0.7) | ||||
| Cardiovascular death | 0 (0.0) | 15 (1.8) | 0 (0.0) | 15 (2.1) | ||||
| hs-TnI Elevation within 7 Days | a Adjusted Odds Ratio (95% CI) | p Value |
|---|---|---|
| In-hospital mortality | ||
| Overall population | 2.37 (1.68–3.33) | < 0.001 |
| Propensity score-matched population | 1.89 (1.28–2.81) | 0.002 |
| Major adverse cardiac events | ||
| Overall population | 2.73 (1.74–4.29) | < 0.001 |
| Propensity score-matched population | 2.64 (1.60–4.51) | < 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.H.; Lee, Y.I.; Ahn, J.; Ryu, J.-A. Association between High-Sensitivity Cardiac Troponin I and Clinical Prognosis of Neurosurgical and Neurocritically Ill Patients. Diagnostics 2022, 12, 2259. https://doi.org/10.3390/diagnostics12092259
Lee JH, Lee YI, Ahn J, Ryu J-A. Association between High-Sensitivity Cardiac Troponin I and Clinical Prognosis of Neurosurgical and Neurocritically Ill Patients. Diagnostics. 2022; 12(9):2259. https://doi.org/10.3390/diagnostics12092259
Chicago/Turabian StyleLee, Jung Hwa, Yun Im Lee, Joonghyun Ahn, and Jeong-Am Ryu. 2022. "Association between High-Sensitivity Cardiac Troponin I and Clinical Prognosis of Neurosurgical and Neurocritically Ill Patients" Diagnostics 12, no. 9: 2259. https://doi.org/10.3390/diagnostics12092259