
Assessment of Pulpal Status in Primary Teeth Following Direct Pulp Capping in an Experimental Canine Model

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
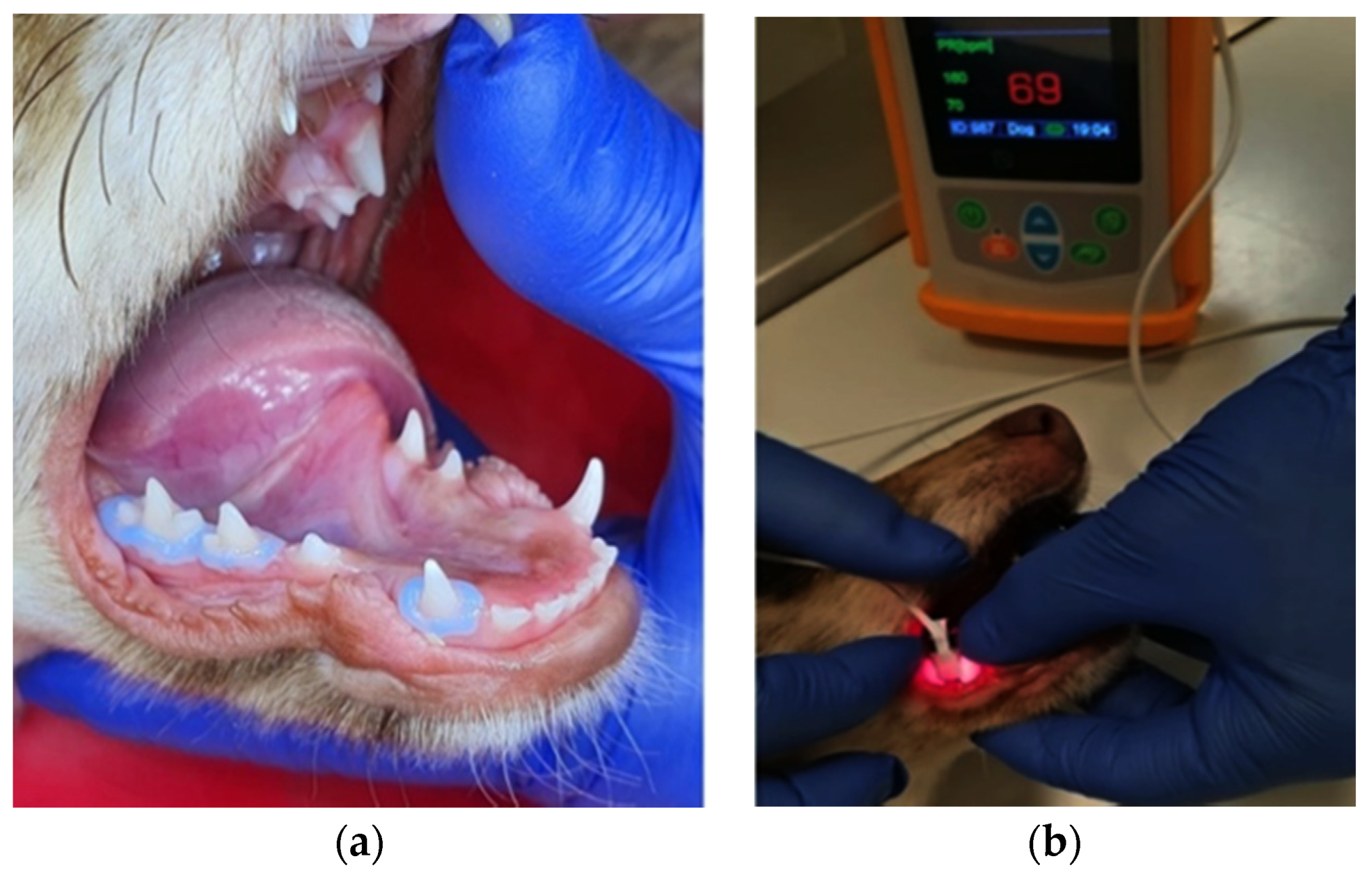
2.1. Operative Procedures
2.2. Complementary Research
2.3. Histologic Examination
2.4. Statistical Analysis
3. Results
3.1. Preoperative Research
3.2. Post-Operative Research
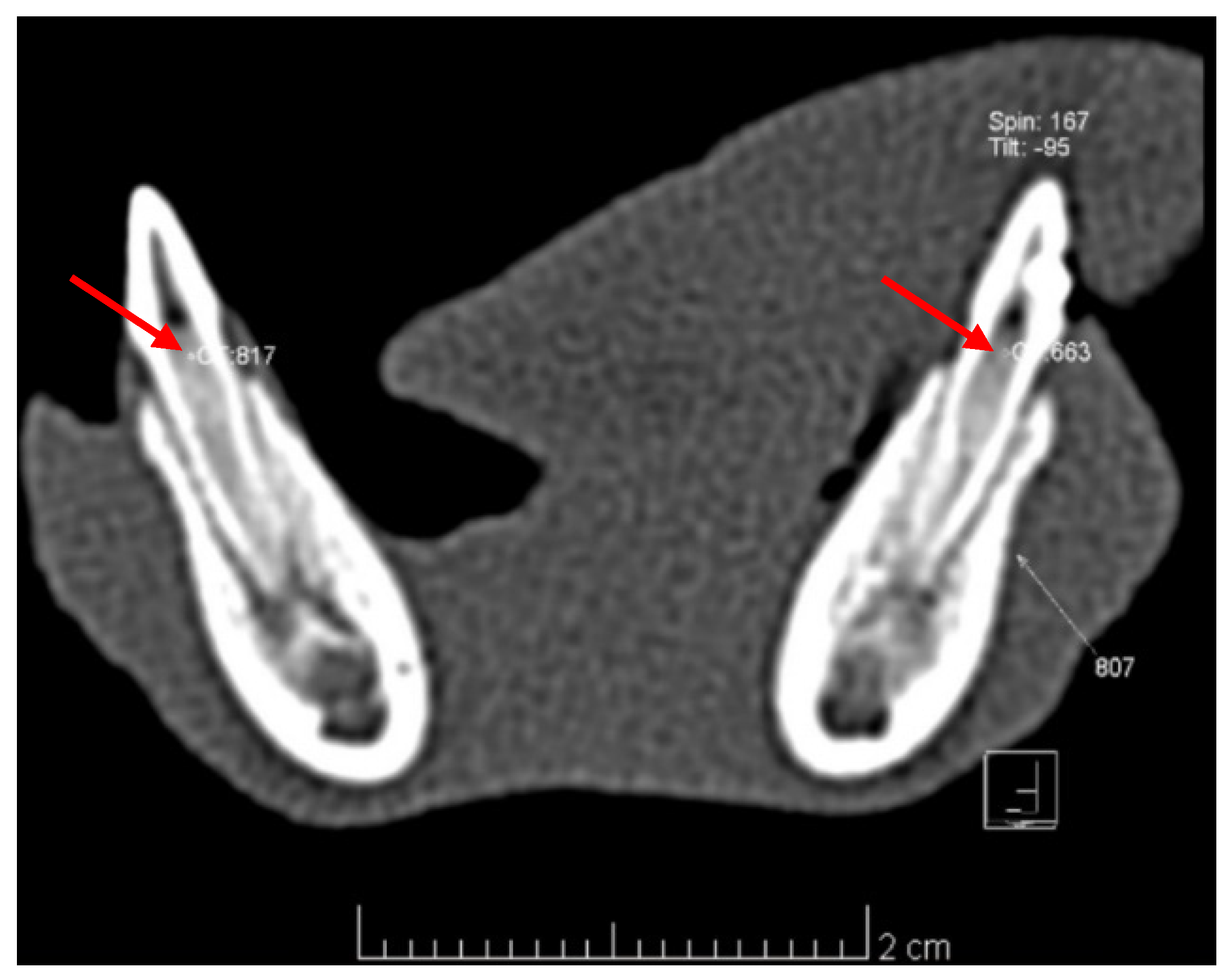
3.2.1. Imagistic Research
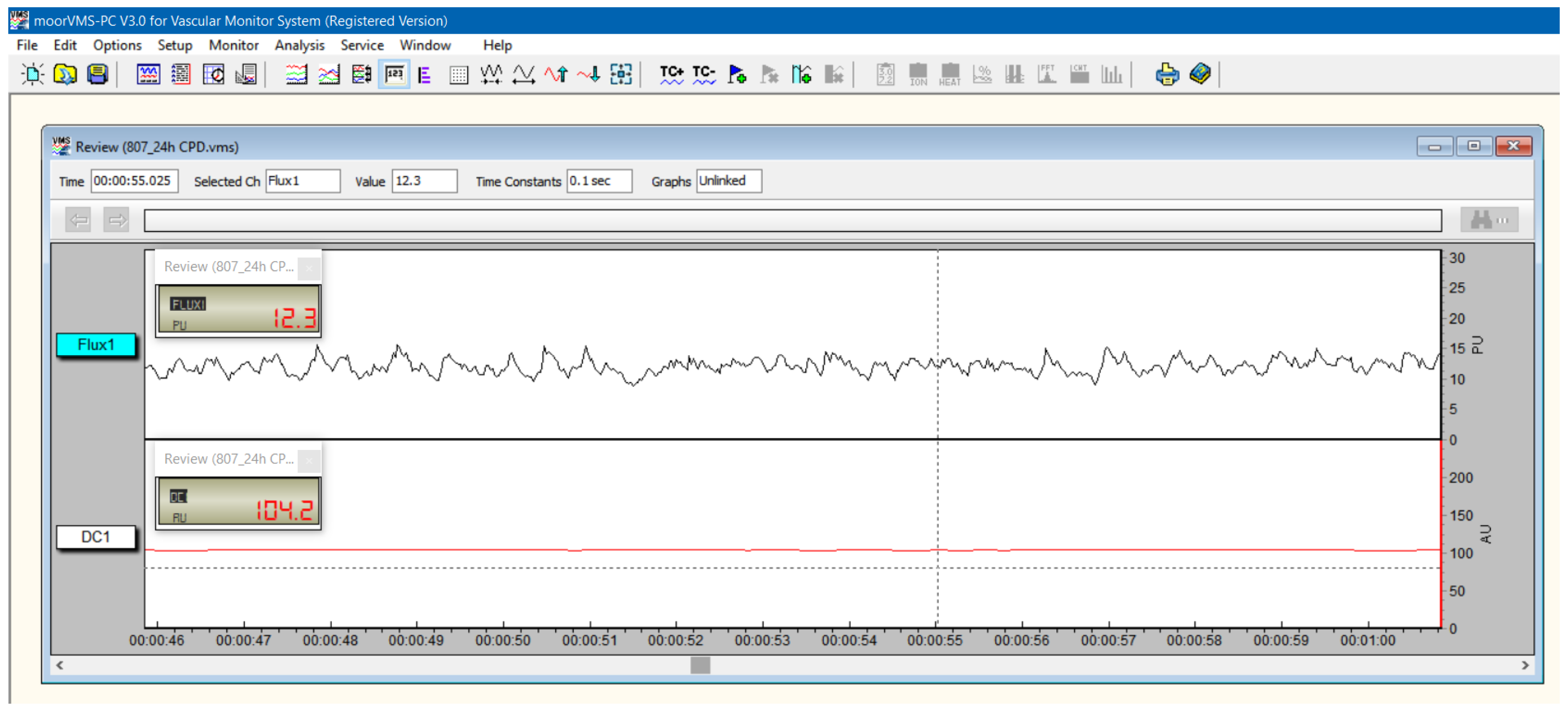
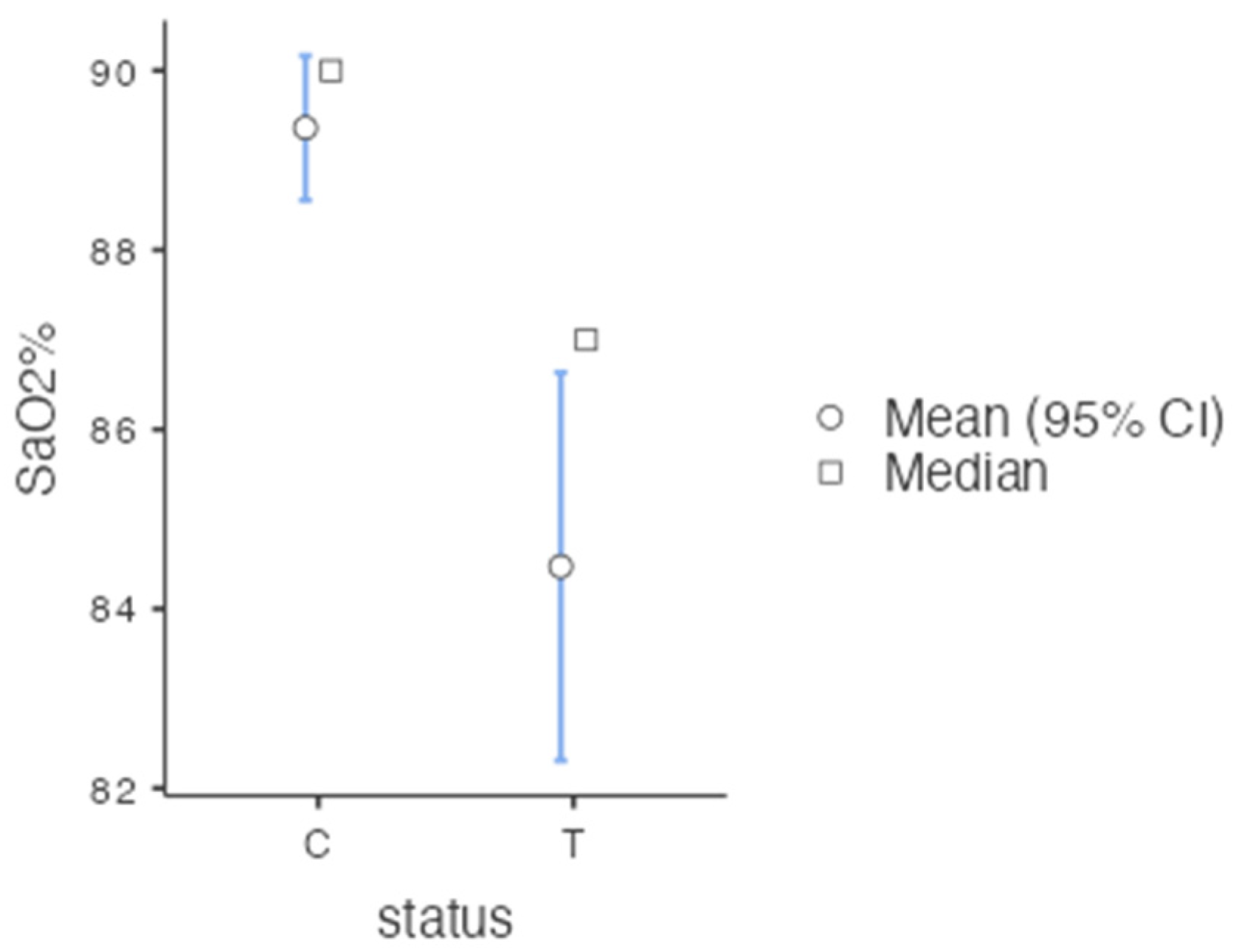
3.2.2. Vitality Tests
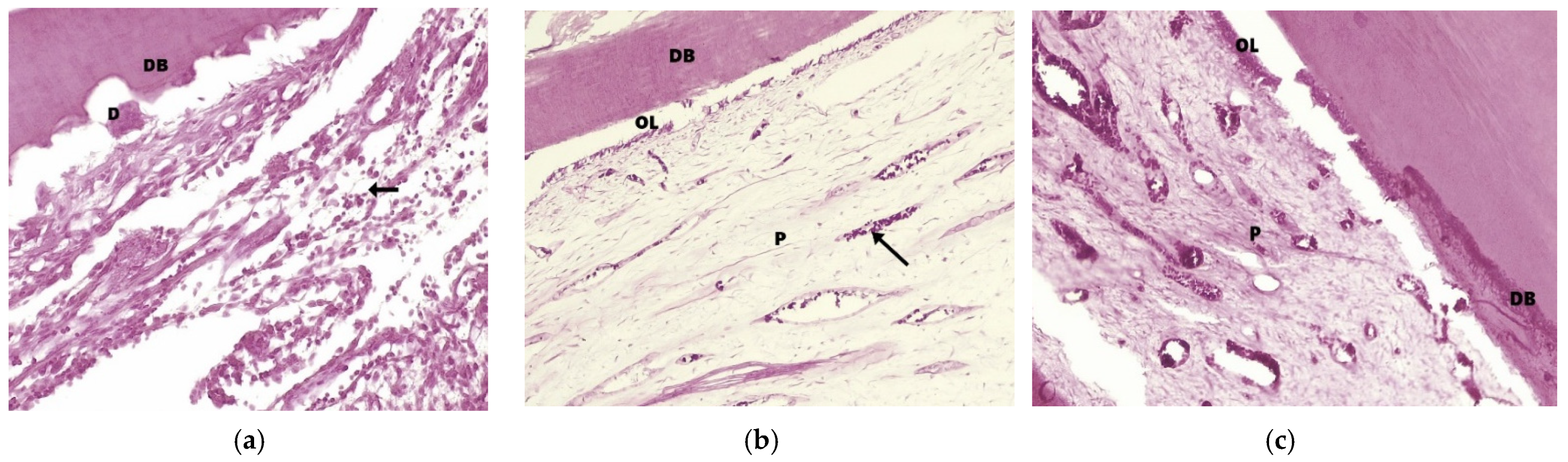
3.2.3. Histologic Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Academy of Pediatric Dentistry. The Reference Manual of Pediatric Dentistry, 3rd ed.; American Academy of Pediatric Dentistry: Chicago, IL, USA, 2020. [Google Scholar]
- Cushley, S.; Duncan, H.F.; Lundy, F.T.; Nagendrababu, V.; Clarke, M.; Karim, I.E. Outcomes reporting in systematic reviews on vital pulp treatment: A scoping review for the development of a core outcome set. Int. Endod. J. 2022, 55, 891–909. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.; Abbott, P.V. Dental Pulp Testing: A Review. Int. J. Dent. 2009, 2009, 365785. [Google Scholar] [CrossRef] [PubMed]
- Gopikrishna, V.; Pradeep, G.; Venkateshbabu, N. Assessment of pulp vitality: A review. Int. J. Paediatr. Dent. 2009, 19, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Jafarzadeh, H.; Abbott, P.V. Review of pulp sensibility tests. Part I: General information and thermal tests. Int. Endod. J. 2010, 43, 738–762. [Google Scholar] [CrossRef]
- Vaghela, D.; Sinha, A. Pulse oximetry and laser doppler flowmetry for diagnosis of pulpal vitality. J. Interdiscip. Dent. 2011, 1, 14–21. [Google Scholar] [CrossRef]
- Sharma, A.; Madan, M.; Shahi, P.; Sood, P.; Shahi, N. Comparative Study of Pulp Vitality in Primary and Young Permanent Molars in Human Children with Pulse Oximeter and Electric Pulp Tester. Int. J. Clin. Pediatr. Dent. 2015, 8, 94–98. [Google Scholar] [CrossRef]
- Mainkar, A.; Kim, S.G. Diagnostic Accuracy of 5 Dental Pulp Tests: A Systematic Review and Meta-analysis. J. Endod. 2018, 44, 694–702. [Google Scholar] [CrossRef]
- Mejàre, I.A.; Axelsson, S.; Davidson, T.; Frisk, F.; Hakeberg, M.; Kvist, T.; Norlund, A.; Petersson, A.; Portenier, I.; Sandberg, H.; et al. Diagnosis of the condition of the dental pulp: A systematic review. Int. Endod. J. 2012, 45, 597–613. [Google Scholar] [CrossRef]
- Grabliauskienė, Ž.; Zamaliauskienė, R.; Lodienė, G. Pulp vitality testing with a developed universal pulse oximeter probe holder. Medicina 2021, 57, 101. [Google Scholar] [CrossRef]
- Janani, K.; Ajitha, P.; Sandhya, R.; Subbaiyan, H.; Jose, J. Efficiency of new custom-made pulse oximeter sensor holder in assessment of actual pulp status. J. Fam. Med. Prim. Care 2020, 9, 3333–3337. [Google Scholar]
- Sharma, D.S.; Mishra, S.; Banda, N.R.; Vaswani, S. In vivo evaluation of customized pulse oximeter and sensitivity pulp tests for assessment of pulp vitality. J. Clin. Pediatr. Dent. 2019, 43, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Almudever-Garcia, A.; Forner, L.; Sanz, J.L.; Llena, C.; Rodríguez-Lozano, F.J.; Guerrero-Gironés, J.; Melo, M. Pulse oximetry as a diagnostic tool to determine pulp vitality: A systematic review. Appl. Sci. 2021, 11, 2747. [Google Scholar] [CrossRef]
- Lambert, P.; Miguens, S.A.Q.; Solda, C.; Sganzerla, J.T.; Reichert, L.A.; Estrela, C.; Barletta, F.B. Reference values for pulp oxygen saturation as a diagnostic tool in endodontics: A systematic review and meta-analysis. Restor. Dent. Endod. 2020, 45, e48. [Google Scholar] [CrossRef] [PubMed]
- Riehl, J.; Hetzel, S.J.; Snyder, C.J.; Soukup, J.W. Detection of pulpal blood flow in vivo with pulse oximetry in dogs. Front. Vet. Sci. 2016, 3, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duncan, H.F. Present status and future directions—Vital pulp treatment and pulp preservation strategies. Int. Endod. J. 2022, 55, 497–511. [Google Scholar] [CrossRef] [PubMed]
- Hanna, S.N.; Perez Alfayate, R.; Prichard, J. Vital Pulp Therapy an Insight Over the Available Literature and Future Expectations. EUR Endod. J. 2020, 5, 46–53. [Google Scholar]
- Li, Z.; Cao, L.; Fan, M.; Xu, Q. Direct Pulp Capping with Calcium Hydroxide or Mineral Trioxide Aggregate: A Meta-analysis. J. Endod. 2015, 41, 1412–1417. [Google Scholar] [CrossRef]
- Mohammadi, Z.; Dummer, P.M.H. Properties and applications of calcium hydroxide in endodontics and dental traumatology. Int. Endod. J. 2011, 44, 697–730. [Google Scholar] [CrossRef]
- Emara, R.; Elhennawy, K.; Schwendicke, F. Effects of calcium silicate cements on dental pulp cells: A systematic review. J. Dent. 2018, 77, 18–36. [Google Scholar] [CrossRef]
- Stringhini Junior, E.; dos Santos, M.G.C.; Oliveira, L.B.; Mercadé, M. MTA and Biodentine for Primary Teeth Pulpotomy: A Systematic Review and Meta-Analysis of Clinical Trials. Clin. Oral Investig. 2019, 23, 1967–1976. [Google Scholar] [CrossRef]
- Coll, J.A.; Seale, N.S.; Vargas, K.; Marghalani, A.A.; Al Shamali, S.; Graham, L. Primary Tooth Vital Pulp Therapy: A Systematic Review and Meta-analysis. Pediatr. Dent. 2017, 39, 16–27. [Google Scholar] [PubMed]
- Miron, M.-I.; Dodenciu, D.; Sarbescu, P.; Canjau, S.; Ardelean, L.; Rusu, L.C.; Todea, C. Condensation Silicones and Light-curing Resin Used within a Laser Doppler Pulp Vitality Testing Method. Mater. Plast. 2012, 49, 171–175. [Google Scholar]
- Miron, M.; Lungeanu, D.; Ciora, E.; Ogodescu, E.; Todea, C. Using laser-doppler flowmetry to evaluate the therapeutic response in dentin hypersensitivity. Int. J. Environ. Res. Public Health 2020, 17, 8787. [Google Scholar] [CrossRef] [PubMed]
- Miron, M.I.; Barcutean, M.; Luca, R.E.; Todea, C.D.; Tudor, A.; Ogodescu, E. The Effect of Changing the Toothbrush on the Marginal Gingiva Microcirculation in the Adolescent Population—A Laser Doppler Flowmetry Assessment. Diagnostics 2022, 12, 1830. [Google Scholar] [CrossRef]
- Nowicka, A.; Lipski, M.; Parafiniuk, M.; Sporniak-Tutak, K.; Lichota, D.; Kosierkiewicz, A.; Kaczmarek, W.; Buczkowska-Radlińska, J. Response of human dental pulp capped with biodentine and mineral trioxide aggregate. J. Endod. 2013, 39, 743–747. [Google Scholar] [CrossRef]
- Pramanik, F.; Firman, R.N.; Oscandar, F.; Epsilawati, L. Normal, inflammation and necrosis pulp radiograph image using 3D cone beam computed tomography. Padjadjaran J. Dent. 2016, 28. [Google Scholar] [CrossRef]
- Marzook, H.A.; Elhawary, Y.M.; El-gindy, A.A.; Radwan, L.R.S. Cone Beam Computed Tomography Voxel Values of Dental Structures. Egypt. Dent. J. 2010, 56, 111–117. [Google Scholar]
- Igna, C.; Sabău, M.; Șereș, M.; Dascălu, R. Stomatologie Veterinară; Igna, C., Ed.; Brumar: Timișoara, Romania, 2008; ISBN 978-973-602-396-5. [Google Scholar]
- Aubeux, D.; Renard, E.; Pérez, F.; Tessier, S.; Geoffroy, V.; Gaudin, A. Review of Animal Models to Study Pulp Inflammation. Front. Dent. Med. 2021, 1, 673552. Available online: www.frontiersin.org (accessed on 25 July 2022). [CrossRef]
- Schallom, M.; Prentice, D.; Sona, C.; Arroyo, C.; Mazuski, J. Comparison of nasal and forehead oximetry accuracy and pressure injury in critically ill patients. Heart Lung 2018, 47, 93–99. [Google Scholar] [CrossRef]
- Estrela, C.R.A.C.; Serpa, G.C.; Alencar, A.H.G.; Bruno, K.F.; Barletta, F.B.; Felippe, W.T.; Estrela, C.R.A.C.; Souza, J.B. Oxygen saturation in the dental pulp of maxillary premolars in different age groups—Part 1. Braz. Dent. J. 2017, 28, 573–577. [Google Scholar] [CrossRef] [Green Version]
- Estrela, C.; Oliveira, K.S.A.; Alencar, A.H.G.; Barletta, F.B.; Estrela, C.R.A.; Felippe, W.T. Oxygen saturation in the dental pulp of maxillaryandmandibularmolars-part 2. Braz. Dent. J. 2017, 28, 704–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anusha, B.; Madhusudhana, K.; Chinni, S.K.; Paramesh, Y. Assessment of pulp oxygen saturation levels by pulse oximetry for pulpal diseases -a diagnostic study. J. Clin. Diagn. Res. 2017, 11, 36–39. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, H.; Ikawa, M.; Mayanagi, H. Age-related changes of pulpal blood flow in primary teeth measured by laser Doppler blood flowmetry. Pediatr. Dent. J. 2007, 17, 27–31. [Google Scholar] [CrossRef] [Green Version]
- Karayilmaz, H.; Kirzioǧlu, Z. Evaluation of pulpal blood flow changes in primary molars with physiological root resorption by laser doppler flowmetry and pulse oximetry. J. Clin. Pediatr. Dent. 2011, 36, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Ghouth, N.; Duggal, M.S.; Kang, J.; Nazzal, H. A Diagnostic Accuracy Study of Laser Doppler Flowmetry for the Assessment of Pulpal Status in Children’s Permanent Incisor Teeth. J. Endod. 2019, 45, 543–548. [Google Scholar] [CrossRef]
- Roeykens, H.; De Moor, R. The use of laser Doppler flowmetry in paediatric dentistry. Eur. Arch. Paediatr. Dent. 2011, 12, 85–89. [Google Scholar] [CrossRef]
- Belcheva, A.; Shindova, M.; Hanna, R. Efficacy of Laser Doppler Flowmetry, as a Diagnostic Tool in Assessing Pulp Vitality of Traumatised Teeth: A Split Mouth Clinical Study. J. Pers. Med. 2021, 11, 801. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.N.; Yan, D.Y.; Huang, C.Y.; Chen, S.C.; Pan, C.Y.; Jeng, J.H.; Chen, Y.K.; Chuang, F.H. Laser Doppler for Accurate Diagnosis of Oehler’s Type III Dens Invaginatus: A Case Report. Appl. Sci. 2021, 11, 3848. [Google Scholar] [CrossRef]
- Silva, I.M.D.C.C.; De Freitas, D.Q.; Ambrosano, G.M.B.; Bóscolo, F.N.; Almeida, S.M. Bone density: Comparative evaluation of hounsfield units in multislice and cone-beam computed tomography. Braz. Oral Res. 2012, 26, 550–556. [Google Scholar] [CrossRef]
- Kühnisch, J.; Anttonen, V.; Duggal, M.S.; Loizides Spyridonos, M.; Rajasekharan, S.; Sobczak, M.; Stratigaki, E.; Van Acker, J.W.G.; Aps, J.K.M.; Horner, K.; et al. European Archives of Paediatric Dentistry Best clinical practice guidance for prescribing dental radiographs in children and adolescents: An EAPD policy document. Eur. Arch. Paediatr. Dent. 2019, 21, 375–386. [Google Scholar] [CrossRef]
- Alghaithy, R.A.; Qualtrough, A.J.E. Pulp sensibility and vitality tests for diagnosing pulpal health in permanent teeth: A critical review. Int. Endod. J. 2017, 50, 135–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrei, M.; Vacaru, R.P.; Coricovac, A.; Ilinca, R.; Didilescu, A.C.; Demetrescu, I. The effect of calcium-silicate cements on reparative dentinogenesis following direct pulp capping on animal models. Molecules 2021, 26, 2725. [Google Scholar] [CrossRef] [PubMed]
- Hamdy, M.; Fayyad, D.; Eldaharawy, M.; Hegazy, E. Physical properties of different Pulp Capping Materials and Histological Analysis of their effect on Dogs’ Dental Pulp Tissue Healing. Egypt. Dent. J. 2018, 64, 2657–2667. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SpO2 | Tooth Position | Tooth Type | Mean | Median | SD |
| Lower | C | 91.8 | 91.0 | 2.62 | |
| P2 | 89.6 | 90.5 | 3.34 | ||
| P3 | 88.6 | 89.5 | 3.33 | ||
| Upper | C | 90.1 | 90.5 | 2.93 | |
| P2 | 89.7 | 90.0 | 3.18 | ||
| P3 | 89.6 | 90.0 | 2.94 |
| Treated/Control Group | Average Values of Pulp Density |
|---|---|
| 804/704 | 328.87 HU/506.25 HU |
| 806/706 | 579.12 HU/698.37 HU |
| 807/707 | 694.37 HU/622.62 HU |
| Biomaterial | Criteria | All Criteria | ||
|---|---|---|---|---|
| Inflammation | Odontoblastic Layer | Dentinal Bridges | ||
| Ca(OH)2 | 3 | 4 | 2 | 4 |
| MTA | 2 | 1 | 3 | 2 |
| BiodentineTM | 1 | 1 | 3 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Igna, A.; Igna, C.; Miron, M.I.; Schuszler, L.; Dascălu, R.; Moldovan, M.; Voicu, A.A.; Todea, C.D.; Boariu, M.; Mârțu, M.-A.; et al. Assessment of Pulpal Status in Primary Teeth Following Direct Pulp Capping in an Experimental Canine Model. Diagnostics 2022, 12, 2022. https://doi.org/10.3390/diagnostics12082022
Igna A, Igna C, Miron MI, Schuszler L, Dascălu R, Moldovan M, Voicu AA, Todea CD, Boariu M, Mârțu M-A, et al. Assessment of Pulpal Status in Primary Teeth Following Direct Pulp Capping in an Experimental Canine Model. Diagnostics. 2022; 12(8):2022. https://doi.org/10.3390/diagnostics12082022
Chicago/Turabian StyleIgna, Andreea, Cornel Igna, Mariana Ioana Miron, Larisa Schuszler, Roxana Dascălu, Mihaela Moldovan, Adrian Aristide Voicu, Carmen Darinca Todea, Marius Boariu, Maria-Alexandra Mârțu, and et al. 2022. "Assessment of Pulpal Status in Primary Teeth Following Direct Pulp Capping in an Experimental Canine Model" Diagnostics 12, no. 8: 2022. https://doi.org/10.3390/diagnostics12082022