
Serum Insulin-Like Growth Factor 1 Levels, Facture Risk Assessment Tool Scores and Bone Disorders in Patients with Primary Biliary Cholangitis

 ,
, 
Abstract
:1. Introduction
2. Patients and Methods
2.1. Participants and Study Design
2.2. Evaluation of Osteoporosis and Vertebral Fracture
2.3. Fracture Risk Assessment with the FRAX
2.4. Grouping of Patients Based on Serum IGF-1 Levels
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Patients
3.2. Clinical Characteristics of the High- and Non-High-Risk Groups
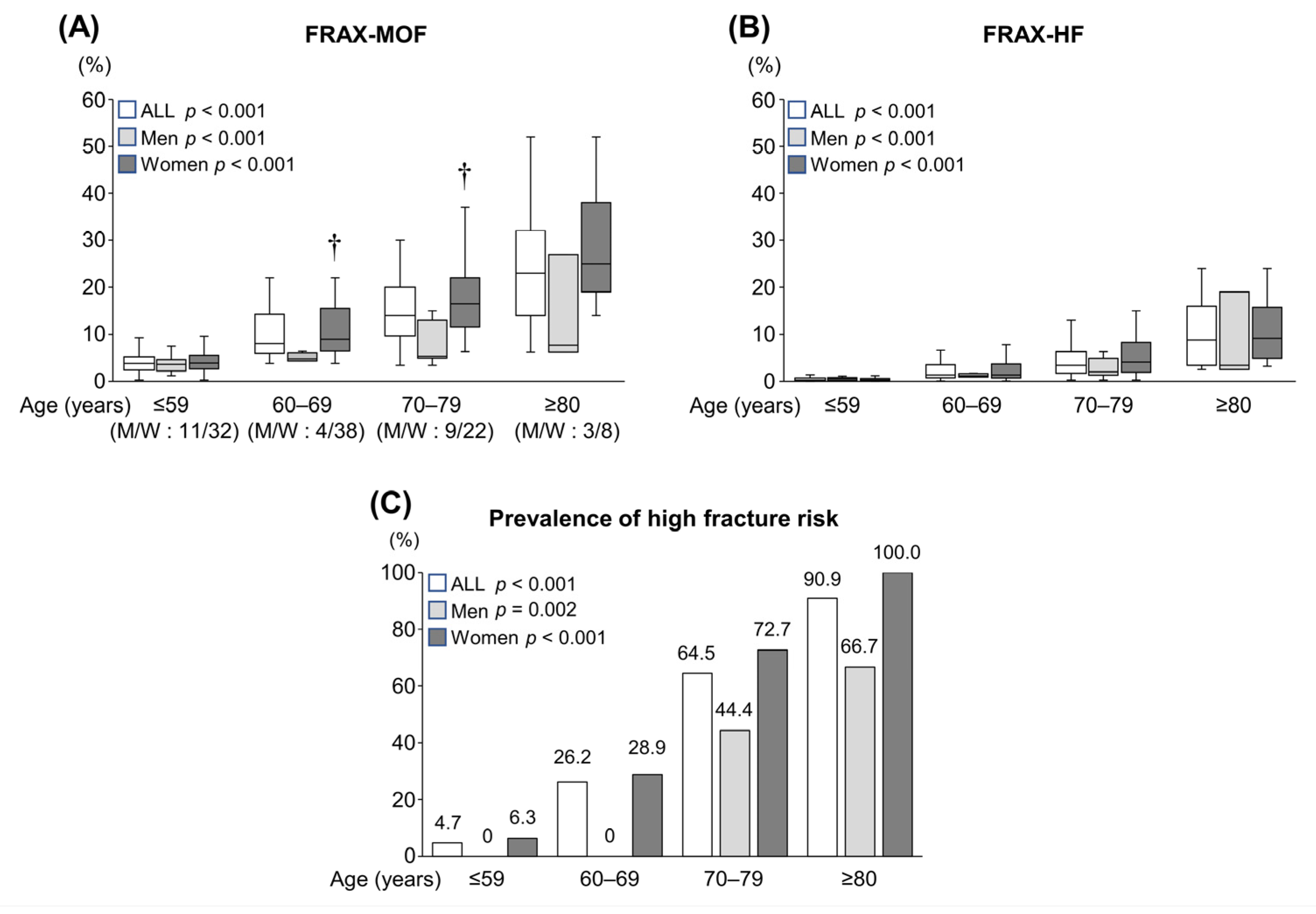
3.3. Prevalence of High Fracture Risk According to the Age Groups
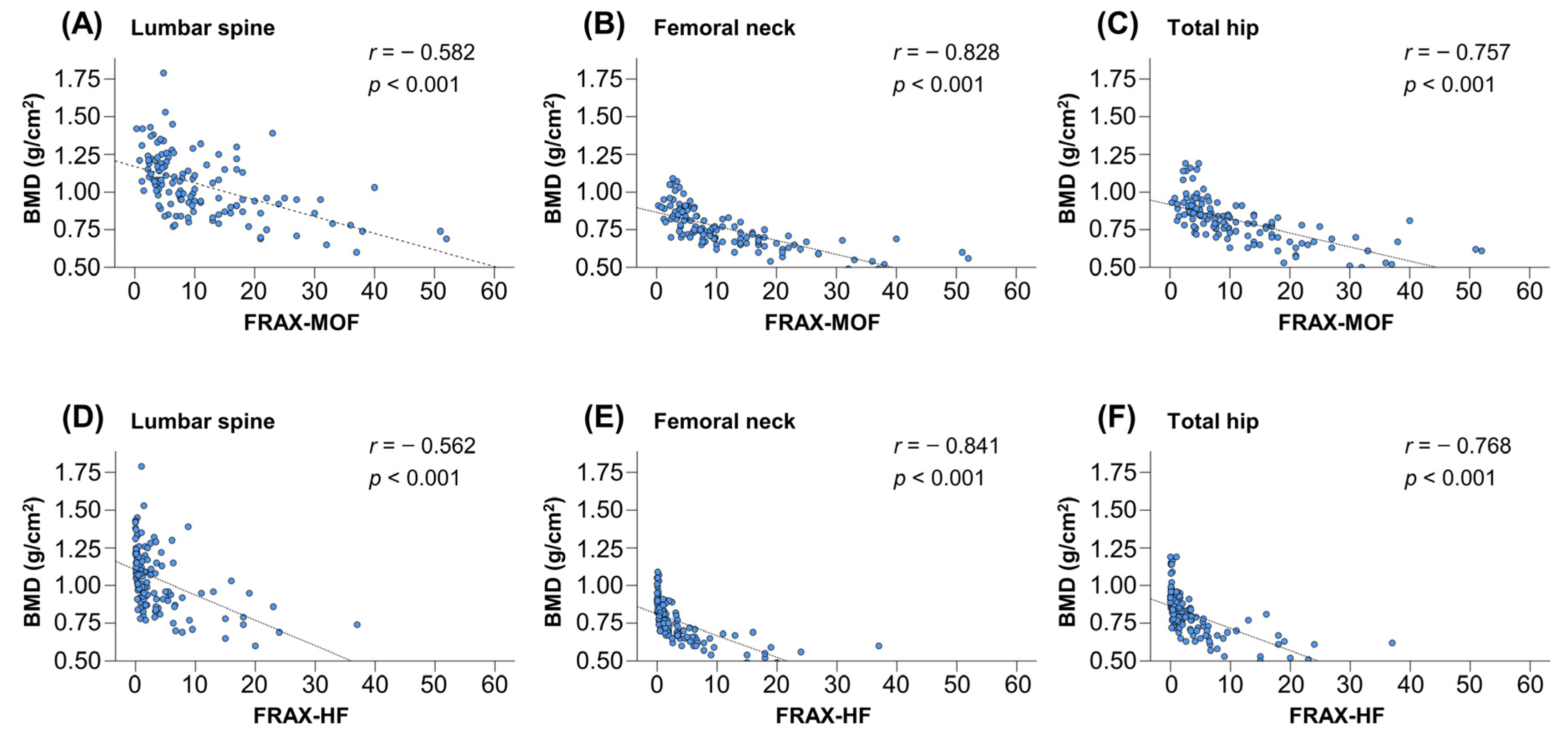
3.4. Correlations between BMD and FRAX Scores
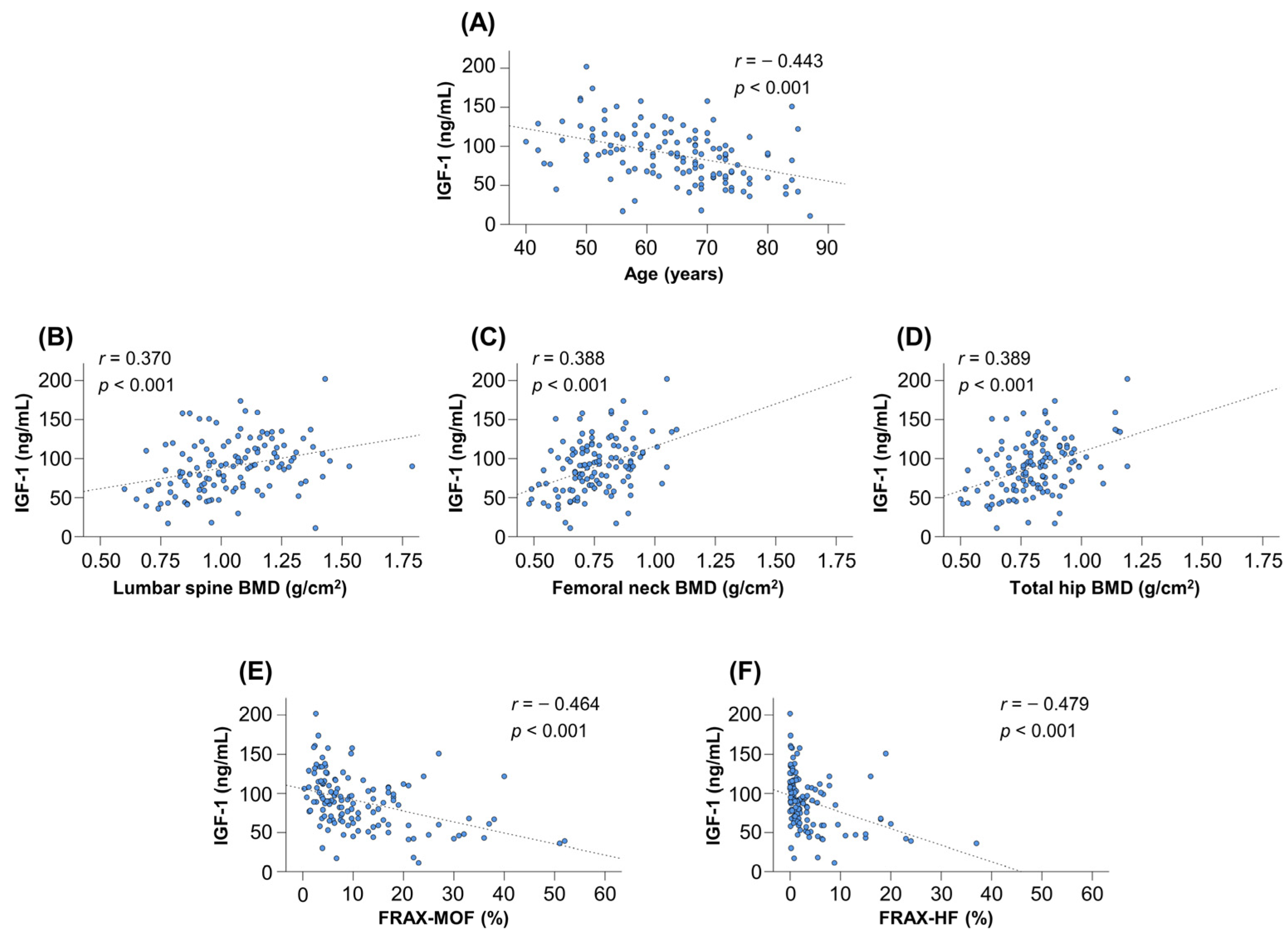
3.5. Serum IGF-1 Levels According to Age Groups
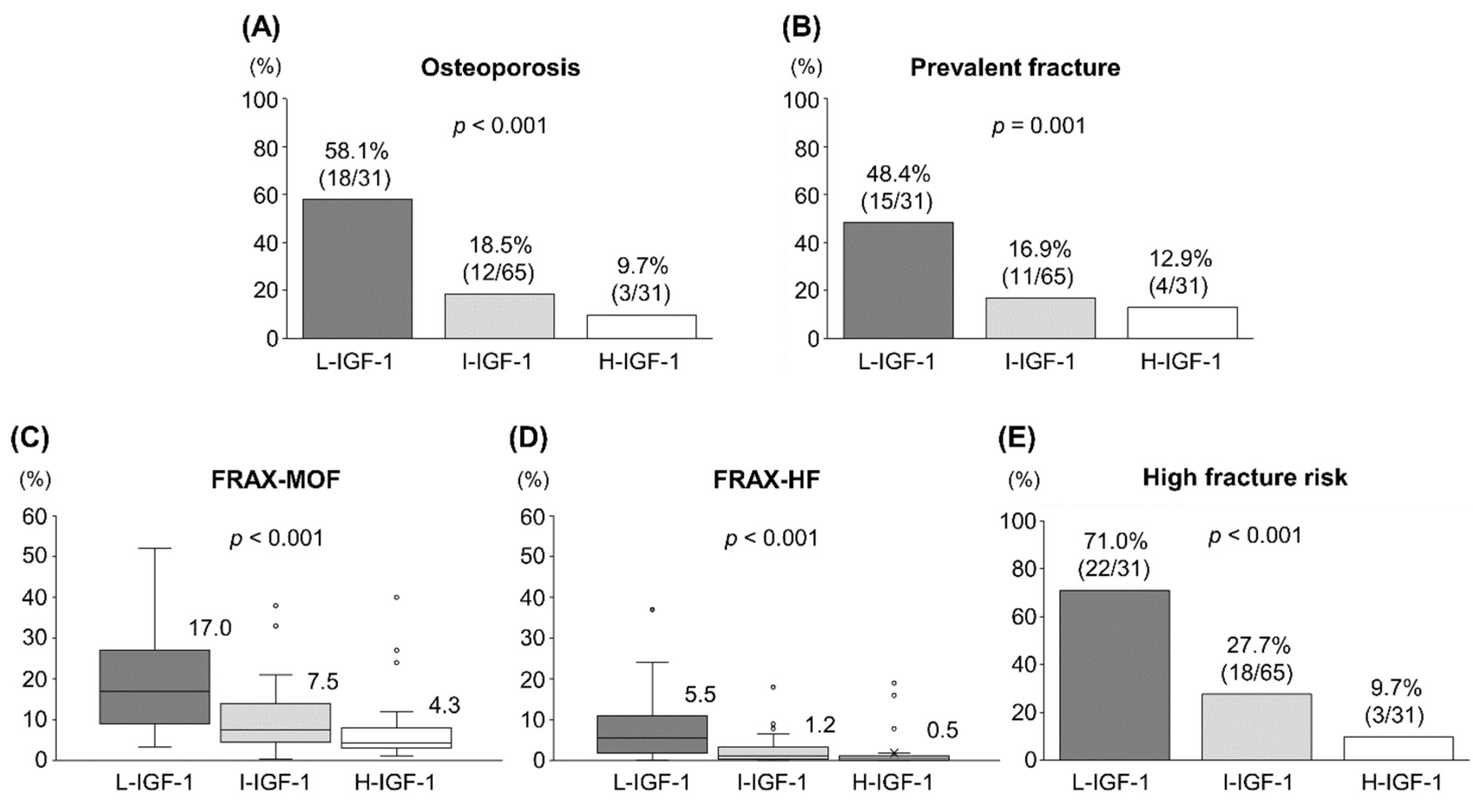
3.6. Clinical Characteristics of the Three Groups Based on Serum IGF-1 Levels
3.7. Correlations between Serum IGF-1 Levels and FRAX Scores
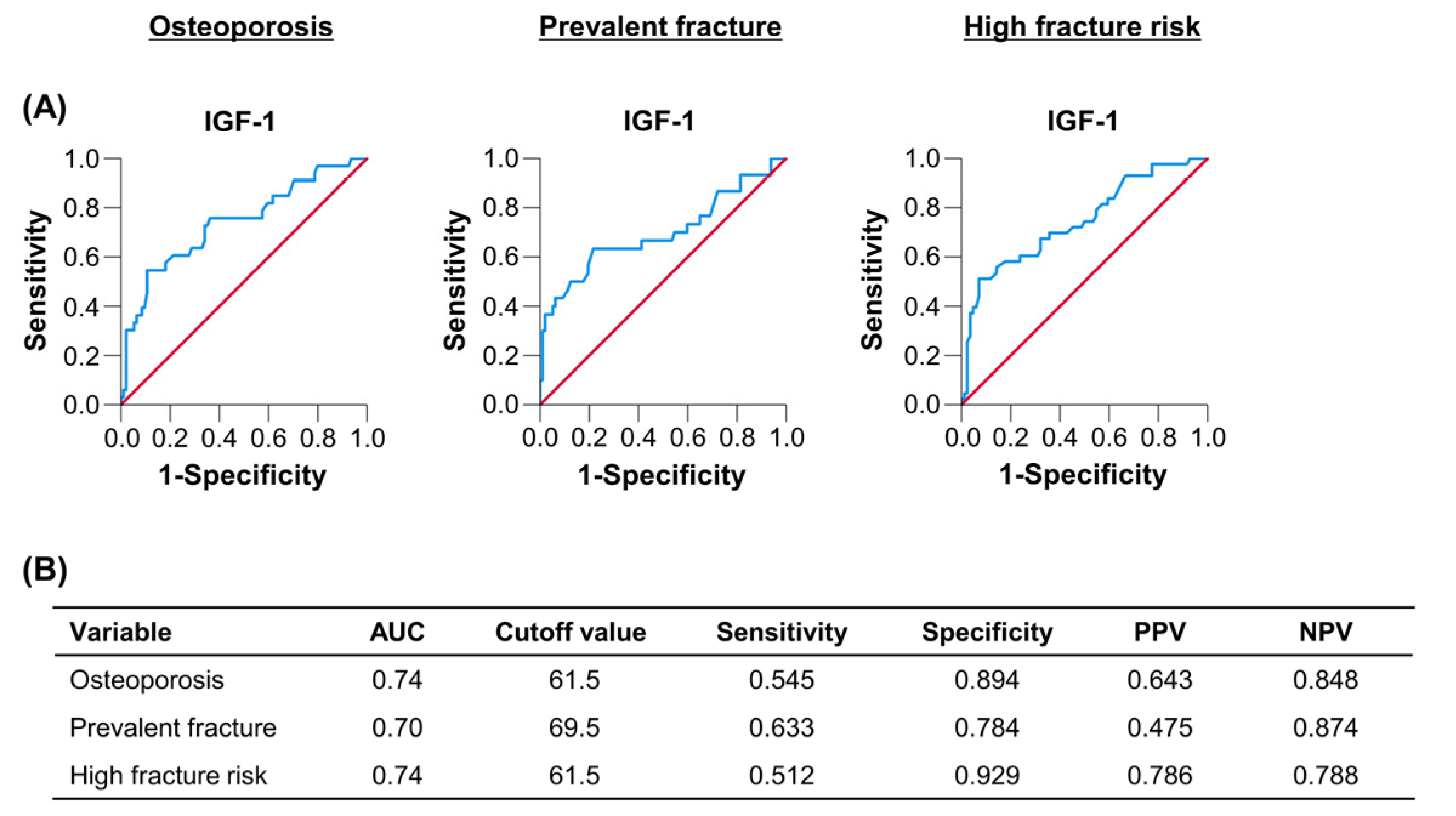
3.8. Optimal Cutoff Values of IGF-1 for Predicting Osteoporosis, Prevalent Fracture and High Fracture Risk
3.9. Fracture Risk between the Cirrhosis and Non-Cirrhosis Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Selmi, C.; Bowlus, C.L.; Gershwin, M.E.; Coppel, R.L. Primary biliary cirrhosis. Lancet 2011, 377, 1600–1609. [Google Scholar] [CrossRef]
- Kaplan, M.M.; Gershwin, M.E. Primary biliary cirrhosis. N. Engl. J. Med. 2005, 353, 1261–1273. [Google Scholar] [CrossRef] [PubMed]
- Guañabens, N.; Parés, A.; Ros, I.; Caballería, L.; Pons, F.; Vidal, S.; Monegal, A.; Peris, P.; Rodés, J. Severity of cholestasis and advanced histological stage but not menopausal status are the major risk factors for osteoporosis in primary biliary cirrhosis. J. Hepatol. 2005, 42, 573–577. [Google Scholar] [CrossRef]
- Guañabens, N.; Cerdá, D.; Monegal, A.; Pons, F.; Caballería, L.; Peris, P.; Parés, A. Low bone mass and severity of cholestasis affect fracture risk in patients with primary biliary cirrhosis. Gastroenterology 2010, 138, 2348–2356. [Google Scholar] [CrossRef]
- Seki, A.; Ikeda, F.; Miyatake, H.; Takaguchi, K.; Hayashi, S.; Osawa, T.; Fujioka, S.I.; Tanaka, R.; Ando, M.; Seki, H.; et al. Risk of secondary osteoporosis due to lobular cholestasis in non-cirrhotic primary biliary cholangitis. J. Gastroenterol. Hepatol. 2017, 32, 1611–1616. [Google Scholar] [CrossRef] [PubMed]
- Saeki, C.; Oikawa, T.; Kanai, T.; Nakano, M.; Torisu, Y.; Sasaki, N.; Abo, M.; Saruta, M.; Tsubota, A. Relationship between osteoporosis, sarcopenia, vertebral fracture, and osteosarcopenia in patients with primary biliary cholangitis. Eur. J. Gastroenterol. Hepatol. 2021, 33, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Wang, Q.; Sun, L. Association between primary biliary cholangitis and osteoporosis: Meta-analysis. Clin. Rheumatol. 2017, 36, 2565–2571. [Google Scholar] [CrossRef] [PubMed]
- Menon, K.V.; Angulo, P.; Weston, S.; Dickson, E.R.; Lindor, K.D. Bone disease in primary biliary cirrhosis: Independent indicators and rate of progression. J. Hepatol. 2001, 35, 316–323. [Google Scholar] [CrossRef]
- Solaymani-Dodaran, M.; Card, T.R.; Aithal, G.P.; West, J. Fracture risk in people with primary biliary cirrhosis: A population-based cohort study. Gastroenterology 2006, 131, 1752–1757. [Google Scholar] [CrossRef]
- Santos, L.A.; Romeiro, F.G. Diagnosis and Management of Cirrhosis-Related Osteoporosis. Biomed. Res. Int. 2016, 2016, 1423462. [Google Scholar] [CrossRef]
- Kanis, J.A.; Johnell, O.; Oden, A.; Johansson, H.; McCloskey, E. FRAX and the assessment of fracture probability in men and women from the UK. Osteoporos. Int. 2008, 19, 385–397. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: The diagnosis and management of patients with primary biliary cholangitis. J. Hepatol. 2017, 67, 145–172. [Google Scholar] [CrossRef] [PubMed]
- LeBoff, M.S.; Greenspan, S.L.; Insogna, K.L.; Lewiecki, E.M.; Saag, K.G.; Singer, A.J.; Siris, E.S. The clinician’s guide to prevention and treatment of osteoporosis. Osteoporos. Int. 2022. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Mazziotti, G.; Lania, A.G.; Canalis, E. Skeletal disorders associated with the growth hormone-insulin-like growth factor 1 axis. Nat. Rev. Endocrinol. 2022, 18, 353–365. [Google Scholar] [CrossRef] [PubMed]
- Locatelli, V.; Bianchi, V.E. Effect of GH/IGF-1 on Bone Metabolism and Osteoporosis. Int. J. Endocrinol. 2014, 2014, 235060. [Google Scholar] [CrossRef] [PubMed]
- Saeki, C.; Takano, K.; Oikawa, T.; Aoki, Y.; Kanai, T.; Takakura, K.; Nakano, M.; Torisu, Y.; Sasaki, N.; Abo, M.; et al. Comparative assessment of sarcopenia using the JSH, AWGS, and EWGSOP2 criteria and the relationship between sarcopenia, osteoporosis, and osteosarcopenia in patients with liver cirrhosis. BMC Musculoskelet. Disord. 2019, 20, 615. [Google Scholar] [CrossRef] [PubMed]
- Lv, F.; Cai, X.; Zhang, R.; Zhou, L.; Zhou, X.; Han, X.; Ji, L. Sex-specific associations of serum insulin-like growth factor-1 with bone density and risk of fractures in Chinese patients with type 2 diabetes. Osteoporos. Int. 2021, 32, 1165–1173. [Google Scholar] [CrossRef]
- Ohlsson, C.; Mellström, D.; Carlzon, D.; Orwoll, E.; Ljunggren, O.; Karlsson, M.K.; Vandenput, L. Older men with low serum IGF-1 have an increased risk of incident fractures: The MrOS Sweden study. J. Bone Miner. Res. 2011, 26, 865–872. [Google Scholar] [CrossRef]
- Working Subgroup (English Version) for Clinical Practice Guidelines for Primary Biliary Cirrhosis. Guidelines for the management of primary biliary cirrhosis. The Intractable Hepatobiliary Disease Study Group supported by the Ministry of Health, Labour and Welfare of Japan. Hepatol. Res. 2014, 44 (Suppl. S1), 71–90. [Google Scholar] [CrossRef]
- WHO. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. WHO Study Group. World Health Organ. Tech. Rep. Ser. 1994, 843, 1–129. [Google Scholar]
- Genant, H.K.; Wu, C.Y.; van Kuijk, C.; Nevitt, M.C. Vertebral fracture assessment using a semiquantitative technique. J. Bone Miner. Res. 1993, 8, 1137–1148. [Google Scholar] [CrossRef] [PubMed]
- Ehnert, S.; Aspera-Werz, R.H.; Ruoß, M.; Dooley, S.; Hengstler, J.G.; Nadalin, S.; Relja, B.; Badke, A.; Nussler, A.K. Hepatic Osteodystrophy-Molecular Mechanisms Proposed to Favor Its Development. Int. J. Mol. Sci. 2019, 20, 2555. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.L.; Lin, C.S.; Shih, C.C.; Huang, Y.F.; Yeh, C.C.; Wu, C.H.; Cherng, Y.G.; Liao, C.C. Risk and adverse outcomes of fractures in patients with liver cirrhosis: Two nationwide retrospective cohort studies. BMJ Open 2017, 7, e017342. [Google Scholar] [CrossRef] [PubMed]
- Kanazawa, I.; Notsu, M.; Miyake, H.; Tanaka, K.; Sugimoto, T. Assessment using serum insulin-like growth factor-I and bone mineral density is useful for detecting prevalent vertebral fractures in patients with type 2 diabetes mellitus. Osteoporos. Int. 2018, 29, 2527–2535. [Google Scholar] [CrossRef]
- Caregaro, L.; Alberino, F.; Amodio, P.; Merkel, C.; Angeli, P.; Plebani, M.; Bolognesi, M.; Gatta, A. Nutritional and prognostic significance of insulin-like growth factor 1 in patients with liver cirrhosis. Nutrition 1997, 13, 185–190. [Google Scholar] [CrossRef]
- Lee, H.J.; Lee, D.C.; Kim, C.O. Association Between 10-Year Fracture Probability and Nonalcoholic Fatty Liver Disease With or Without Sarcopenia in Korean Men: A Nationwide Population-Based Cross-Sectional Study. Front. Endocrinol 2021, 12, 599339. [Google Scholar] [CrossRef]
- Nishizawa, H.; Iguchi, G.; Fukuoka, H.; Takahashi, M.; Suda, K.; Bando, H.; Matsumoto, R.; Yoshida, K.; Odake, Y.; Ogawa, W.; et al. IGF-I induces senescence of hepatic stellate cells and limits fibrosis in a p53-dependent manner. Sci. Rep. 2016, 6, 34605. [Google Scholar] [CrossRef]
- Okajima, H.; Shigeno, C.; Inomata, Y.; Egawa, H.; Uemoto, S.; Asonuma, K.; Kiuchi, T.; Konishi, J.; Tanaka, K. Long-term effects of liver transplantation on bone mineral density in children with end-stage liver disease: A 2-year prospective study. Liver Transplant. 2003, 9, 360–364. [Google Scholar] [CrossRef]
- Sinclair, M.; Gow, P.J.; Grossmann, M.; Angus, P.W. Review article: Sarcopenia in cirrhosis-aetiology, implications and potential therapeutic interventions. Aliment. Pharmacol. Ther. 2016, 43, 765–777. [Google Scholar] [CrossRef]
- Saeki, C.; Kanai, T.; Nakano, M.; Oikawa, T.; Torisu, Y.; Saruta, M.; Tsubota, A. Low Serum Branched-Chain Amino Acid and Insulin-Like Growth Factor-1 Levels Are Associated with Sarcopenia and Slow Gait Speed in Patients with Liver Cirrhosis. J. Clin. Med. 2020, 9, 3239. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients | FRAX | FRAX | p Value |
|---|---|---|---|---|
| High Risk | Non-High Risk | |||
| Patients, n (%) | 127 | 43 (33.9) | 84 (66.1) | 0.150 |
| Women, n (%) | 100 (78.7) | 37 (86.0) | 63 (75.0) | <0.001 |
| Age (years) | 66.0 (56.0–72.0) | 73.0 (69.0–77.0) | 60.0 (53.3–68.0) | <0.001 |
| Body height (cm) | 157.0 (150.0–162.0) | 151.3 (145.0–156.0) | 158.5 (153.3–164.9) | <0.001 |
| Body weight (kg) | 54.0 (48.6–63.2) | 49.5 (44.1–55.4) | 56.6 (51.3–65.2) | 0.418 |
| BMI (kg/m2) | 22.2 (20.3–24.7) | 22.2 (20.1–24.7) | 22.3 (20.4–24.7) | 0.048 |
| Disease duration (years) | 2.0 (1.0–8.0) | 4.0 (1.0–9.0) | 2.0 (1.0–6.0) | 0.002 |
| Cirrhosis, n (%) | 12 (9.4) | 9 (20.9) | 3 (3.6) | 0.514 |
| Smoking, n (%) | 31 (24.4) | 9 (20.9) | 22 (26.2) | 0.486 |
| Alcohol intake, n (%) | 9 (7.1) | 4 (9.3) | 5 (6.0) | <0.001 |
| M2BPGi (C.O.I) | 0.85 (0.62–1.28) | 1.24 (0.68–1.79) | 0.73 (0.57–0.99) | <0.001 |
| IGF-1 (ng/mL) | 90 (65–112) | 61 (46–97) | 96 (77–118) | <0.001 |
| Lumbar spine BMD (g/cm2) | 1.03 (0.90–1.19) | 0.90 (0.78–0.96) | 1.09 (0.98–1.22) | <0.001 |
| Lumbar spine T score | −1.00 (−1.96–−0.10) | −1.92 (−2.90–−1.20) | −0.58 (−1.40–0.29) | <0.001 |
| Femoral neck BMD (g/cm2) | 0.74 (0.67–0.86) | 0.65 (0.59–0.69) | 0.82 (0.74–0.90) | <0.001 |
| Femoral neck T score | −1.76 (−2.34–−1.00) | −2.60 (−3.11–−2.20) | −1.23 (−1.80–−0.52) | <0.001 |
| Total hip BMD (g/cm2) | 0.80 (0.72–0.89) | 0.69 (0.62–0.77) | 0.85 (0.79–0.93) | <0.001 |
| Total hip T score | −1.31 (−1.90–−0.80) | −2.20 (−2.69–−1.50) | −0.98 (−1.48–−0.32) | <0.001 |
| Osteoporosis, n (%) | 33 (26.0) | 30 (69.8) | 3 (3.6) | <0.001 |
| Prevalent fracture, n (%) | 30 (23.6) | 27 (62.8) | 3 (3.6) |
| 10-Year Probability of Fracture | All Patients | FRAX | FRAX |
|---|---|---|---|
| High Risk | Non-High Risk | ||
| Major osteoporotic fracture (%) | 7.7 (4.3–16.0) | 19.0 (15.0–27.0) | 5.1 (3.7–7.8) |
| Hip fracture (%) | 1.3 (0.4–4.1) | 6.3 (3.8–13.0) | 0.7 (0.2–1.3) |
| Variable | L-IGF-1 | I-IGF-1 | H-IGF-1 | p Value |
|---|---|---|---|---|
| Patients, n (%) | 31 (24.4) | 65 (51.2) | 31 (24.4) | |
| Women, n (%) | 26 (83.9) | 53 (81.5) | 21 (67.7) | 0.220 |
| Age (years) | 73.0 (68.0–77.0) | 65.0 (56.0–71.5) | 58.0 (51.0–64.0) | <0.001 |
| Body height (cm) | 152.5 (144.2–160.7) | 152.0 (157.0–160.1) | 159.8 (151.0–169.0) | 0.033 |
| Body weight (kg) | 52.6 (45.0–57.0) | 54.9 (48.3–62.7) | 56.0 (49.8–68.0) | 0.147 |
| BMI (kg/m2) | 22.2 (20.4–24.0) | 22.3 (19.5–24.6) | 21.5 (20.3–25.7) | 0.993 |
| Disease duration (years) | 7.0 (1.0–13.0) | 2.0 (1.0–7.0) | 2.0 (1.0–4.0) | 0.020 |
| Cirrhosis, n (%) | 9 (29.0) | 3 (4.6) | 0 (0.0) | <0.001 |
| Smoking, n (%) | 6 (19.4) | 17 (26.2) | 8 (25.8) | 0.752 |
| Alcohol intake, n (%) | 1 (3.2) | 4 (6.2) | 4 (12.9) | 0.304 |
| M2BPGi (C.O.I) | 1.33 (0.89–2.39) | 0.74 (0.59–1.11) | 0.74 (0.55–0.99) | <0.001 |
| IGF-1 (ng/mL) | 48 (42–59) | 90 (77–100) | 129 (118–151) | <0.001 |
| Lumbar spine BMD (g/cm2) | 0.91 (0.78–1.05) | 1.07 (0.94–1.22) | 1.12 (0.95–1.21) | <0.001 |
| Lumbar spine T score | −1.80 (−2.90–−1.00) | −0.80 (−1.78–0.26) | −0.38 (−1.20–0.26) | <0.001 |
| Femoral neck BMD (g/cm2) | 0.66 (0.60–0.75) | 0.75 (0.69–0.88) | 0.82 (0.72–0.91) | <0.001 |
| Femoral neck T score | −2.50 (−2.99–−1.66) | −1.70 (−2.20–−0.90) | −1.26 (−2.06–−0.40) | <0.001 |
| Total hip BMD (g/cm2) | 0.72 (0.63–0.83) | 0.80 (0.75–0.89) | 0.85 (0.80–0.94) | <0.001 |
| Total hip T score | −1.90 (−2.60–−1.20) | −1.31 (−1.75–−0.76) | −0.90 (−1.50–−0.30) | <0.001 |
| Osteoporosis, n (%) | 18 (58.1) | 12 (18.5) | 3 (9.7) | <0.001 |
| Prevalent fracture, n (%) | 15 (48.4) | 11 (16.9) | 4 (12.9) | <0.001 |
| 10-year probability of MOF, (%) | 17.0 (9.0–27.0) | 7.5 (4.5–14.0) | 4.3 (3.1–8.0) | <0.001 |
| 10-year probability of HF, (%) | 5.5 (1.9–11.0) | 1.2 (0.4–3.3) | 0.5 (0.1–1.2) | <0.001 |
| High fracture risk, n (%) | 22 (71.0) | 18 (27.7) | 3 (9.7) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saeki, C.; Oikawa, T.; Ueda, K.; Nakano, M.; Torisu, Y.; Saruta, M.; Tsubota, A. Serum Insulin-Like Growth Factor 1 Levels, Facture Risk Assessment Tool Scores and Bone Disorders in Patients with Primary Biliary Cholangitis. Diagnostics 2022, 12, 1957. https://doi.org/10.3390/diagnostics12081957
Saeki C, Oikawa T, Ueda K, Nakano M, Torisu Y, Saruta M, Tsubota A. Serum Insulin-Like Growth Factor 1 Levels, Facture Risk Assessment Tool Scores and Bone Disorders in Patients with Primary Biliary Cholangitis. Diagnostics. 2022; 12(8):1957. https://doi.org/10.3390/diagnostics12081957
Chicago/Turabian StyleSaeki, Chisato, Tsunekazu Oikawa, Kaoru Ueda, Masanori Nakano, Yuichi Torisu, Masayuki Saruta, and Akihito Tsubota. 2022. "Serum Insulin-Like Growth Factor 1 Levels, Facture Risk Assessment Tool Scores and Bone Disorders in Patients with Primary Biliary Cholangitis" Diagnostics 12, no. 8: 1957. https://doi.org/10.3390/diagnostics12081957