
Circulating microRNAs as Biomarkers of Hepatic Fibrosis in Schistosomiasis Japonica Patients in the Philippines

 ,
,  ,
,  , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
2.2. Study Area and Population
2.3. Study Design and Sampling Technique
2.4. Sample Size
2.5. Eligibility Criteria
2.6. Prospective Study
2.7. Ultrasound and Clinical Evaluation
2.8. SEA IgG ELISA
2.9. Target miRNA Identification
2.10. RNA Extraction
2.11. Reverse Transcription PCR (RT PCR)
2.12. Initial miRNA Profiling
2.13. Validation of miRNA Expression Using Quantitative PCR (qPCR)
2.14. Target Predictions
2.15. Data Analyses Plan
2.16. Statistical Analyses
3. Results
3.1. Characteristics of Patients
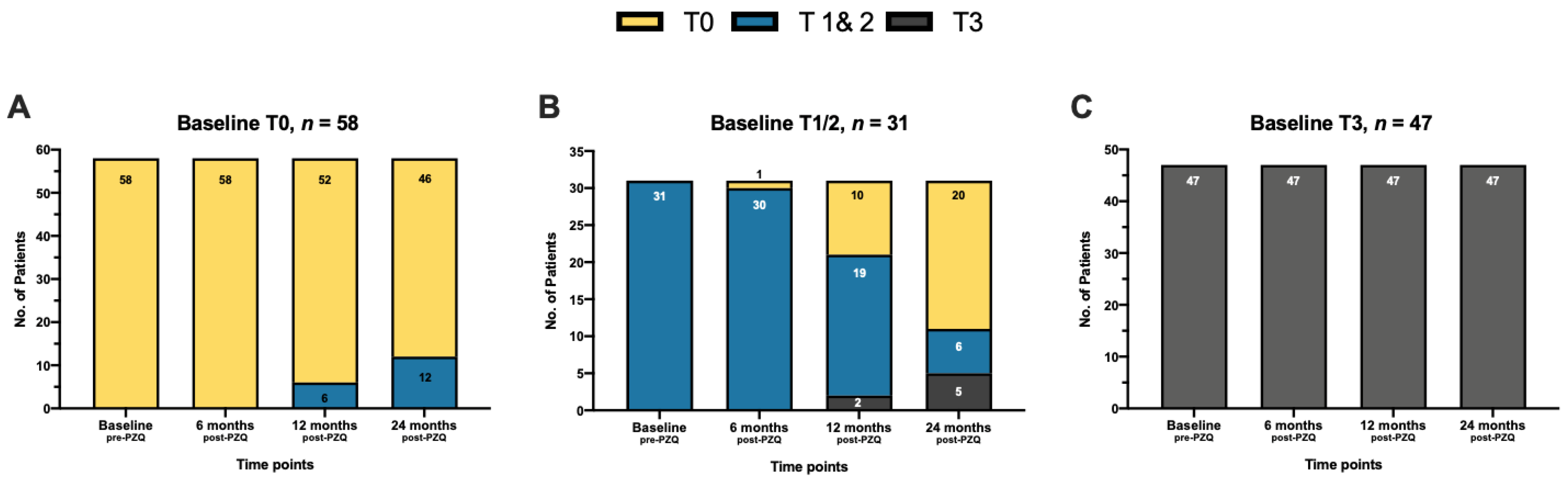
3.2. Evaluation of Hepatic Fibrosis Outcomes by Ultrasonography
3.3. Selection of miRNAs
3.4. RT-qPCR Validation of miRNAs
3.5. miRNAs as Biomarkers of Hepatic Fibrosis
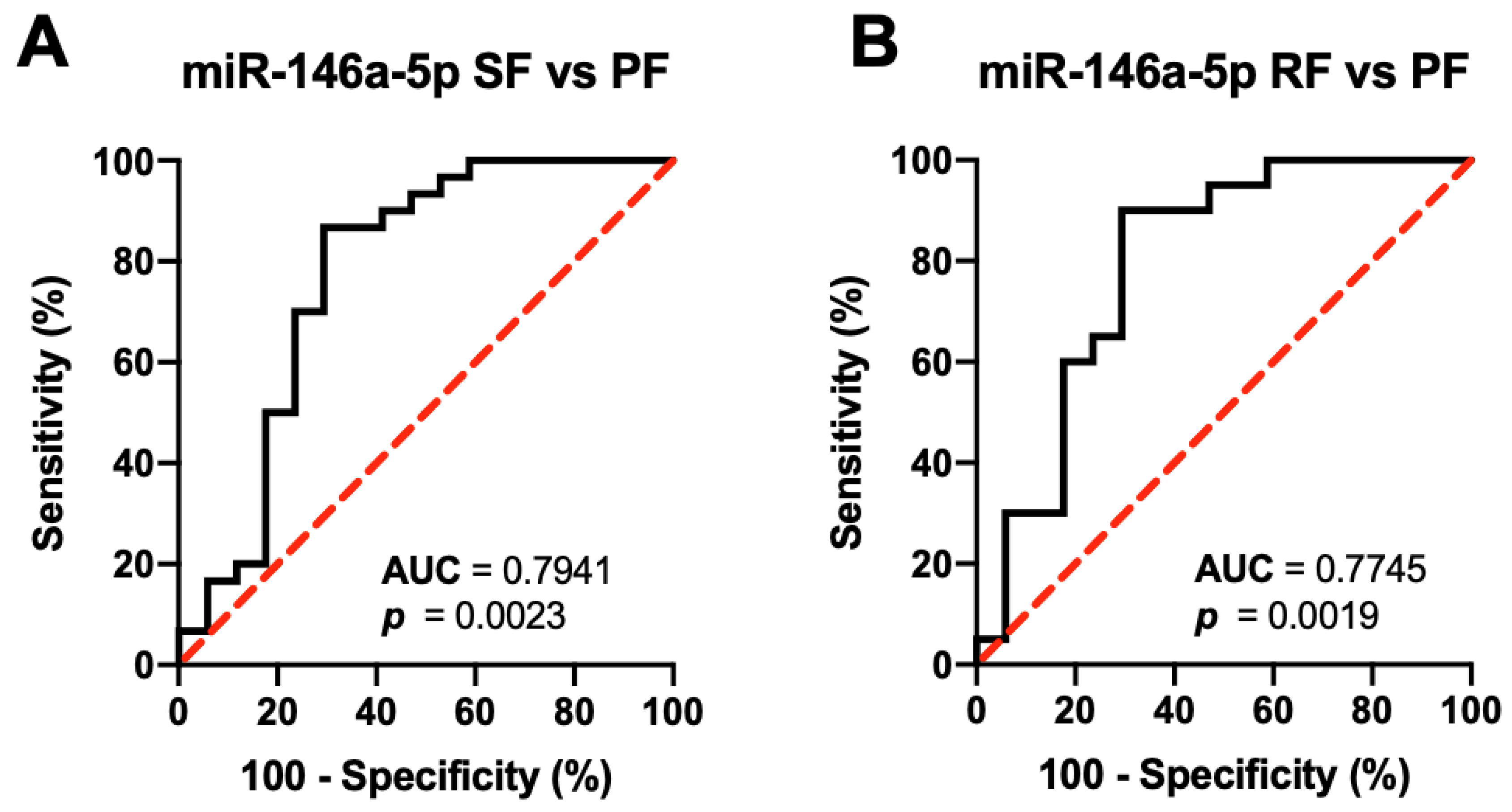
3.6. miRNAs as Biomarkers of Hepatic Fibrosis Outcomes
4. Discussion
4.1. Serological Markers of Liver Status
4.2. Hepatic Fibrosis Outcomes
4.3. Serum miRNAs as Biomarkers of Hepatic Fibrosis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chitsulo, L.; Engels, D.; Montresor, A.; Savioli, L. The Global Status of Schistosomiasis and Its Control. Acta Trop. 2000, 77, 41–51. [Google Scholar] [CrossRef] [Green Version]
- Leonardo, L.; Rivera, P.; Saniel, O.; Villacorte, E.; Lebanan, M.A.; Crisostomo, B.; Hernandez, L.; Baquilod, M.; Erce, E.; Martinez, R.; et al. A National Baseline Prevalence Survey of Schistosomiasis in the Philippines Using Stratified Two-Step Systematic Cluster Sampling Design. J. Trop. Med. 2012, 2012, 936128. [Google Scholar] [CrossRef] [PubMed]
- Leonardo, L.; Acosta, L.P.; Olveda, R.M.; Aligui, G.D.L. Difficulties and Strategies in the Control of Schistosomiasis in the Philippines. Acta Trop. 2002, 82, 295–299. [Google Scholar] [CrossRef]
- Steinmann, P.; Keiser, J.; Bos, R.; Tanner, M.; Utzinger, J. Schistosomiasis and Water Resources Development: Systematic Review, Meta-Analysis, and Estimates of People at Risk. Lancet Infect. Dis. 2006, 6, 411–425. [Google Scholar] [CrossRef]
- Region, D.L.; Li, Y.; Raso, G.; Zhao, Z.; He, Y.; Ellis, M.K.; Mcmanus, D.P. Large Water Management Projects and Schistosomiasis. Emerg. Infect. Dis. 2007, 13, 973–979. [Google Scholar]
- Utzinger, J.; Raso, G.; Brooker, S.; Savigny, D.D.E.; Tanner, M.; Singer, B.H.; Goran, E.K.N. Schistosomiasis and Neglected Tropical Diseases: Towards Integrated and Sustainable Control and a Word of Caution. Parasitology 2009, 136, 1859–1874. [Google Scholar] [CrossRef] [Green Version]
- Olveda, D.; Inobaya, M.; Olveda, R.; Vinluan, M.; Ng, S.; Weerakoon, K.; Mcmanus, D.P.; Ramm, G.A.; Harn, D.A.; Li, Y.; et al. Diagnosing Schistosomiasis-Induced Liver Morbidity: Implications for Global Control. Int. J. Infect. Dis. 2017, 54, 138–144. [Google Scholar] [CrossRef] [Green Version]
- Andrade, Z. Schistosomiasis and Liver Fibrosis. Parasite Immunol. 2009, 31, 656–663. [Google Scholar] [CrossRef]
- Andrade, J.; Silva, L.D.; Guimaraes, C.M.; Bassetti-Soares, E.; Cambraia, R.D.; Couto, O.F.M.; Teixeira, R. Chronic Hepatitis B and Liver Schistosomiasis: A Deleterious Association. Trans. R. Soc. Trop. Med. Hyg. 2014, 108, 159–164. [Google Scholar] [CrossRef]
- Olveda, D.; Olveda, R.; Lam, A.; Chau, T.; Li, Y.; Gisparil, A.; Ross, A. Utility of Diagnostic Imaging in the Diagnosis and Management of Schistosomiasis. Clin. Microbiol. 2014, 3, 142. [Google Scholar] [CrossRef] [Green Version]
- Ohmae, H.; Tanaka, M.; Hayashi, M.; Matsuzaki, Y.; Kurosaki, Y.; Blas, B.; Portillo, G.; Sy, O.; Irie, Y.; Yasuraoka, K. Ultrasonographic and Serologic Abnormalities in Schistosoma Japonicum Infection in Leyte, the Philippines. Am. J. Trop. Med. Hyg. 1992, 46, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Richter, J.; Campange, G.; Hatz, G.; Berquist, N.R.; Jenkins, J.M. Ultrasound in Schistosomiasis: A Practical Guide to the Standardized Use of Ultrasonography for the Assessment of Schistosomiasis-Related Morbidity; World Health Organization: Geneva, Switzerland, 1996. [Google Scholar]
- Lily, Y.S.; Sleigh, A.C.; Li, Y.; Tanner, M.; Dessein, A.; Willlams, G.M. Five-Year Impact of Repeated Praziquantel Due to Schistosoma Japonicum in China Treatment on Subclinical Morbidity. Trans. R. Soc. Trop. Med. Hyg. 2002, 96, 438–443. [Google Scholar]
- He, X.; Sai, X.; Chen, C.; Zhang, Y.; Xu, X.; Zhang, D.; Pan, W. Host Serum MiR-223 Is a Potential New Biomarker for Schistosoma Japonicum Infection and the Response to Chemotherapy. Parasites Vectors 2013, 6, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, P.; Gobert, G.N.; You, H.; Duke, M.; McManus, D.P. Circulating MiRNAs: Potential Novel Biomarkers for Hepatopathology Progression and Diagnosis of Schistosomiasis Japonica in Two Murine Models. PLoS Negl. Trop. Dis. 2015, 9, e0003965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, P.; Mu, Y.; Olveda, R.M.; Ross, A.G.; Olveda, D.U.; McManus, D.P. Circulating MiRNAs as Footprints for Liver Fibrosis Grading in Schistosomiasis. eBioMedicine 2018, 37, 334–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, P.; Mu, Y.; Olveda, R.M.; Ross, A.G.; Olveda, D.U.; McManus, D.P. Serum Exosomal MiRNAs for Grading Hepatic Fibrosis Due to Schistosomiasis. Int. J. Mol. Sci. 2020, 21, 3560. [Google Scholar] [CrossRef]
- Leonardo, L.; Chigusa, Y.; Kikuchi, M.; Kato-Hayashi, N.; Kawazu, S.-I.; Angeles, J.M.; Fontanilla, I.K.; Tabios, I.K.; Moendeg, K.; Goto, Y.; et al. Schistosomiasis in the Philippines: Challenges and Some Successes in Control. Southeast Asian J. Trop. Med. Publich Health 2016, 47, 651–666. [Google Scholar]
- Li, C.-I.; Su, P.-F.; Guo, Y.; Shyr, Y. Sample Size Calculation for Differential Expression Analysis of RNA-Seq Data under Poisson Distribution. Int. J. Comput. Biol. Drug Des. 2013, 6, 358–375. [Google Scholar] [CrossRef]
- Angeles, J.M.; Goto, Y.; Kirinoki, M.; Leonardo, L.; Tongol-Rivera, P.; Villacorte, E.; Inoue, N.; Chigusa, Y.; Kawazu, S. Human Antibody Response to Thioredoxin Peroxidase-1 and Tandem Repeat Proteins as Immunodiagnostic Antigen Candidates for Schistosoma Japonicum Infection. Am. J. Trop. Med. Hyg. 2011, 85, 674–679. [Google Scholar] [CrossRef] [Green Version]
- Kato-Hayashi, N.; Leonardo, L.R.; Arevalo, N.L.; Tagum, M.N.B.; Aspin, J.; Agsolid, L.M.; Chua, J.C.; Kirinoki, M.; Kikuchi, M.; Ohmae, H.; et al. Detection of Active Schistosome Infection by Cell-Free Circulating DNA of Schistosoma Japonicum in Highly Endemic Areas in Sorsogon Province, in the Philippines. Acta Trop. 2015, 141, 178–183. [Google Scholar] [CrossRef]
- Marabita, F.; De Candia, P.; Torri, A.; Tegner, J.; Abrignani, S.; Rossi, R.L. Normalization of Circulating MicroRNA Expression Data Obtained by Quantitative Real-Time RT-PCR. Brief. Bioinform. 2016, 17, 204–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livak, K.J.; Schmittgen, T.D. Analysis of Relative Gene Expression Data Using Real-Time Quantitative PCR and the 2−ΔΔCT Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Indrayan, A. Receiver Operating Characteristic (ROC) Curve for Medical Researchers. Indian Pediatr. 2011, 48, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Fabre, V.; Wu, H.; PondTor, S.; Coutinho, H.; Acosta, L.; Jiz, M.; Olveda, R.; Cheng, L.; White, E.S.; Jarilla, B.; et al. Tissue Inhibitor of Matrix-Metalloprotease-1 Predicts Risk of Hepatic Fibrosis in Human Schistosoma Japonicum Infection. J. Infect. Dis. 2011, 203, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Olveda, D.; Inobaya, M.; McManus, D.; Olveda, R.M.; Vinluan, M.L.; Ng, S.K.; Harn, D.A.; Li, Y.; Guevarra, J.R.; Lam, A.K.; et al. Biennial versus Annual Treatment for Schistosomiasis and Its Impact on Liver Morbidity. Int. J. Infect. Dis. 2017, 54, 145–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- da Silva, F.L.; Del-Rei, R.P.; Fraga, D.B.M.; Leony, L.M.; de Souza, A.M.G.C.; Santos, F.L.N. Alterations in the Lipid Profiles and Circulating Liver Enzymes in Individuals Infected by Schistosoma Mansoni. Rev. Soc. Bras. Med. Trop. 2018, 51, 795–801. [Google Scholar] [CrossRef] [PubMed]
- Hou, X.; Ellis, M.K.; McManus, D.P.; Wang, Y.; Li, S.; Williams, G.M.; Li, Y. sheng Diagnostic Value of Non-Invasive Bio-Markers for Stage-Specific Diagnosis of Hepatic Fibrosis in Patients with Advanced Schistosomiasis Japonica. Int. J. Parasitol. 2011, 41, 325–332. [Google Scholar] [CrossRef]
- Ross, A.G.P.; Olveda, R.M.; Chy, D.; Olveda, D.U.; Li, Y.; Harn, D.A.; Gray, D.J.; McManus, D.P.; Tallo, V.; Chau, T.N.P.; et al. Can Mass Drug Administration Lead to the Sustainable Control of Schistosomiasis? J. Infect. Dis. 2015, 211, 283–289. [Google Scholar] [CrossRef] [Green Version]
- Carlton, E.J.; Hsiang, M.; Zhang, Y.; Johnson, S.; Hubbard, A.; Spear, R.C. The Impact of Schistosoma Japonicum Infection and Treatment on Ultrasound-Detectable Morbidity: A Five- Year Cohort Study in Southwest China. PLoS Negl. Trop. Dis. 2010, 4, e685. [Google Scholar] [CrossRef]
- Bezman, N.A.; Chakraborty, T.; Bender, T.; Lanier, L.L. MiR-150 Regulates the Development of NK and INKT Cells. J. Exp. Med. 2011, 208, 2717–2731. [Google Scholar] [CrossRef] [Green Version]
- Guan, H.; Peng, R.; Mao, L.; Fang, F.; Xu, B.; Chen, M. Injured Tubular Epithelial Cells Activate Fibroblasts to Promote Kidney Fibrosis through MiR-150-Containing Exosomes. Exp. Cell Res. 2020, 392, 112007. [Google Scholar] [CrossRef] [PubMed]
- Deng, P.; Chen, L.; Liu, Z.; Ye, P.; Wang, S.; Wu, J.; Yao, Y.; Sun, Y.; Huang, X.; Ren, L.; et al. MicroRNA-150 Inhibits the Activation of Cardiac Fibroblasts by Regulating c-Myb. Cell. Physiol. Biochem. 2016, 38, 2103–2122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Ren, W.; Wang, X.; Yu, X.; Cui, L.; Li, X.; Zhang, X.; Shi, B. MicroRNA-150 Relieves Vascular Remodeling and Fibrosis in Hypoxia-Induced Pulmonary Hypertension. Biomed. Pharmacother. 2019, 109, 1740–1749. [Google Scholar] [CrossRef] [PubMed]
- Matsuura, K.; De Giorgi, V.; Schechterly, C.; Wang, R.Y.; Farci, P.; Tanaka, Y.; Alter, H.J. Circulating Let-7 Levels in Plasma and Extracellular Vesicles Correlate with Hepatic Fibrosis Progression in Chronic Hepatitis C. Hepatology 2016, 64, 732–745. [Google Scholar] [CrossRef] [PubMed]
- Matsuura, K.; Aizawa, N.; Enomoto, H.; Nishiguchi, S.; Toyoda, H.; Kumada, T.; Iio, E.; Ito, K.; Ogawa, S.; Isogawa, M.; et al. Circulating Let-7 Levels in Serum Correlate with the Severity of Hepatic Fibrosis in Chronic Hepatitis C. Open Forum Infect. Dis. 2018, 5, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Guo, J.; Li, Y.; Jiao, K.; Zhang, Y. Let-7a Suppresses Liver Fibrosis via TGFβ/SMAD Signaling Transduction Pathway. Exp. Ther. Med. 2019, 17, 3935–3942. [Google Scholar] [CrossRef]
- Du, J.; Niu, X.; Wang, Y.; Kong, L.; Wang, R.; Zhang, Y.; Zhao, S.; Nan, Y. MiR-146a-5p Suppresses Activation and Proliferation of Hepatic Stellate Cells in Nonalcoholic Fibrosing Steatohepatitis through Directly Targeting Wnt1 and Wnt5a. Sci. Rep. 2015, 5, 1–14. [Google Scholar] [CrossRef]
- Zou, Y.; Li, S.; Li, Z.; Song, D.; Zhang, S.; Yao, Q. MiR-146a Attenuates Liver Fibrosis by Inhibiting Transforming Growth Factor-Β1 Mediated Epithelial-Mesenchymal Transition in Hepatocytes. Cell. Signal. 2019, 58, 1–8. [Google Scholar] [CrossRef]
- Kitano, M.; Bloomston, P.M. Hepatic Stellate Cells and MicroRNAs in Pathogenesis of Liver Fibrosis. J. Clin. Med. 2016, 5, 38. [Google Scholar] [CrossRef]
- Wang, G.; Kwan, B.C.H.; Lai, F.M.M.; Chow, K.M.; Li, P.K.T.; Szeto, C.C. Urinary MiR-21, MiR-29, and MiR-93: Novel Biomarkers of Fibrosis. Am. J. Nephrol. 2012, 36, 412–418. [Google Scholar] [CrossRef]
- Ma, J.; Zhang, L.; Hao, J.; Li, N.; Tang, J.; Hao, L. Up-Regulation of MicroRNA-93 Inhibits TGF-Β1-Induced EMT and Renal Fibrogenesis by down-Regulation of Orai1. J. Pharmacol. Sci. 2018, 136, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Zhang, Y.; Zhu, H.; Hu, J.; Xie, Z. MiR-34a/MiR-93 Target c-Ski to Modulate the Proliferaton of Rat Cardiac Fibroblasts and Extracellular Matrix Deposition in Vivo and in Vitro. Cell. Signal. 2018, 46, 145–153. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Schistosomiasis Patients 1 | p-Value | ||
|---|---|---|---|---|
| Type 0 n = 58 | Types 1–2 n = 31 | Type 3 n = 47 | ||
| Female | 19 | 10 | 20 | 0.51 a, NS |
| Male | 39 | 21 | 27 | |
| Age, mean ± SD (year) | 36.9 ± 6.9 | 36.7 ± 5.6 | 37.8 ± 6.4 | 0.68 b, NS |
| BMI ± SD (kg/m2) | 28.7 ± 6.2 | 29.9 ± 5.9 | 26.1 ± 9.6 | 0.06 b, NS |
| WBC, mean ± SD (4–10 × 109/L) | 8.7 ± 4.3 | 7.5 ± 3.7 | 9.7 ± 4.1 | 0.06 b, NS |
| Hgb, mean ± SD (120–160 g/L) | 151.0 ± 32.3 | 149.3 ± 19.7 | 143.9 ± 21.1 | 0.32 b, NS |
| PLT, mean ± SD (150–450 × 109/L) | 327.3 ± 137.9 | 361.3 ± 157.2 | 384.8 ± 166.6 | 0.17 b, NS |
| ALT, mean ± SD NV M: 21–72/F: 9–52 IU/L | 35 ± 17.2 | 29 ± 11.2 | 32 ± 8.7 | 0.10 a, NS |
| ALT abnormality no. (%) > 2 × ULN | 6 (10.3) | 4 (12.9) | 6 (12.8) | 0.9 a, NS |
| AST, mean ± SD NV M: 17–59/F: 14–36 IU/L | 31 ± 10.7 | 27 ± 6.3 | 29 ± 8.9 | 0.17 b, NS |
| AST abnormality no. (%) > 2 × ULN | 4 (6.9) | 2 (6.5) | 3 (6.5) | 0.99 a, NS |
| EPG, mean ± SD | 89.2 ± 65.1 | 99.1 ± 52.3 | 157 ± 101.2 | <0.01 b, c, S |
| Infection Intensity 2 | ||||
| Low | 41 | 24 | 33 | 0.53 d, NS |
| Moderate | 16 | 5 | 10 | |
| High | 1 | 2 | 4 | |
| Parameters | Baseline No. (%) | Follow-Up | |||||
|---|---|---|---|---|---|---|---|
| 6 Months No. (%) | p-Value a | 12 Months No. (%) | p-Value a | 24 Months No. (%) | p-Value a | ||
| Schistosoma japonicum positivity | |||||||
| 3 stool K-K | 136 (100) | 0 (0.0) | - | 0 (0) | - | 34 (25.0) | - |
| EPG, mean ± SD | 106 ± 45 | - | - | - | - | 46 ± 16 | - |
| SEA ELISA | 136 (100) | 136 (100) | - | 101 (74.3) | - | 89 (65.4) | - |
| Infection intensity 1 | |||||||
| Low | 98 (72.1) | 0 (0) | - | 0 (0) | - | 32 (0) | - |
| Moderate | 31 (22.8) | 0 (0) | 0 (0) | 2 (0) | |||
| High | 7 (5.1) | 0 (0) | 0 (0) | 0 (0) | |||
| Hepatic fibrosis 2 | |||||||
| Type 0 | 58 (42.6) | 59 (43.4) | - | 63 (46.3) | - | 66 (48.5) | - |
| Types 1 and 2 | 31 (22.8) | 30 (22.1) | 24 (17.6) | 18 (13.2) | |||
| Type 3 | 47 (34.6) | 47 (34.6) | 49 (36.0) | 52 (38.2) | |||
| Portal vein wall thickness 3 | |||||||
| normal | 118 (86.8) | 117 (86.0) | 0.99 NS | 121 (89.0) | 0.71 NS | 128 (94.1) | 0.06 NS |
| thickened | 18 (13.2) | 19 (14.0) | 15 (11.0) | 8 (5.9) | |||
| Liver size 3 | |||||||
| normal | 122 (89.7) | 127 (93.4) | 0.38 NS | 132 (97.1) | 0.03 S | 133 (97.8) | 0.01 S |
| enlarged | 14 (10.3) | 9 (6.6) | 4 (2.9) | 3 (2.2) | |||
| Spleen size 3 | |||||||
| normal | 116 (85.3) | 130 (95.6) | <0.01 S | 133 (97.8) | <0.01 S | 133 (97.8) | <0.01 S |
| enlarged | 20 (14.7) | 6 (4.4) | 3 (2.2) | 3 (2.2) | |||
| Target miRNA | AUC (95% CI) | Expression Level Cut-Off | Sensitivity % (95% CI) | Specificity % (95% CI) | LR |
|---|---|---|---|---|---|
| miR-146a-5p | 0.90 (0.84–0.96) | <−8.16 | 60.34 (47.49–71.91) | 98.72 (93.09–99.93) | 47.07 |
| let-7a-5p | 0.73 (0.64–0.81) | <−8.75 | 5.172 (1.41–14.14) | 98.72 (93.09–99.93) | 4.03 |
| miR-150-5p | 0.64 (0.54–0.78) | <−7.67 | 12.07 (5.97–22.88) | 96.15 (89.29–98.95) | 3.14 |
| miR-93-5p | 0.67 (0.57–0.76) | >−3.42 | 13.79 (7.16–24.93) | 98.72 (93.09–99.93) | 10.76 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tabios, I.K.B.; Sato, M.O.; Tantengco, O.A.G.; Fornillos, R.J.C.; Kirinoki, M.; Sato, M.; Rojo, R.D.; Fontanilla, I.K.C.; Chigusa, Y.; Medina, P.M.B.; et al. Circulating microRNAs as Biomarkers of Hepatic Fibrosis in Schistosomiasis Japonica Patients in the Philippines. Diagnostics 2022, 12, 1902. https://doi.org/10.3390/diagnostics12081902
Tabios IKB, Sato MO, Tantengco OAG, Fornillos RJC, Kirinoki M, Sato M, Rojo RD, Fontanilla IKC, Chigusa Y, Medina PMB, et al. Circulating microRNAs as Biomarkers of Hepatic Fibrosis in Schistosomiasis Japonica Patients in the Philippines. Diagnostics. 2022; 12(8):1902. https://doi.org/10.3390/diagnostics12081902
Chicago/Turabian StyleTabios, Ian Kim B., Marcello Otake Sato, Ourlad Alzeus Gaddi Tantengco, Raffy Jay C. Fornillos, Masashi Kirinoki, Megumi Sato, Raniv D. Rojo, Ian Kendrich C. Fontanilla, Yuichi Chigusa, Paul Mark B. Medina, and et al. 2022. "Circulating microRNAs as Biomarkers of Hepatic Fibrosis in Schistosomiasis Japonica Patients in the Philippines" Diagnostics 12, no. 8: 1902. https://doi.org/10.3390/diagnostics12081902