
Autotaxin Activity in Chronic Subdural Hematoma: A Prospective Clinical Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection and Biofluids
2.2. LysoPLD Activity Assay
2.3. Enzyme Linked Immunosorbent Assays
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics, Medical History and Clinical Findings
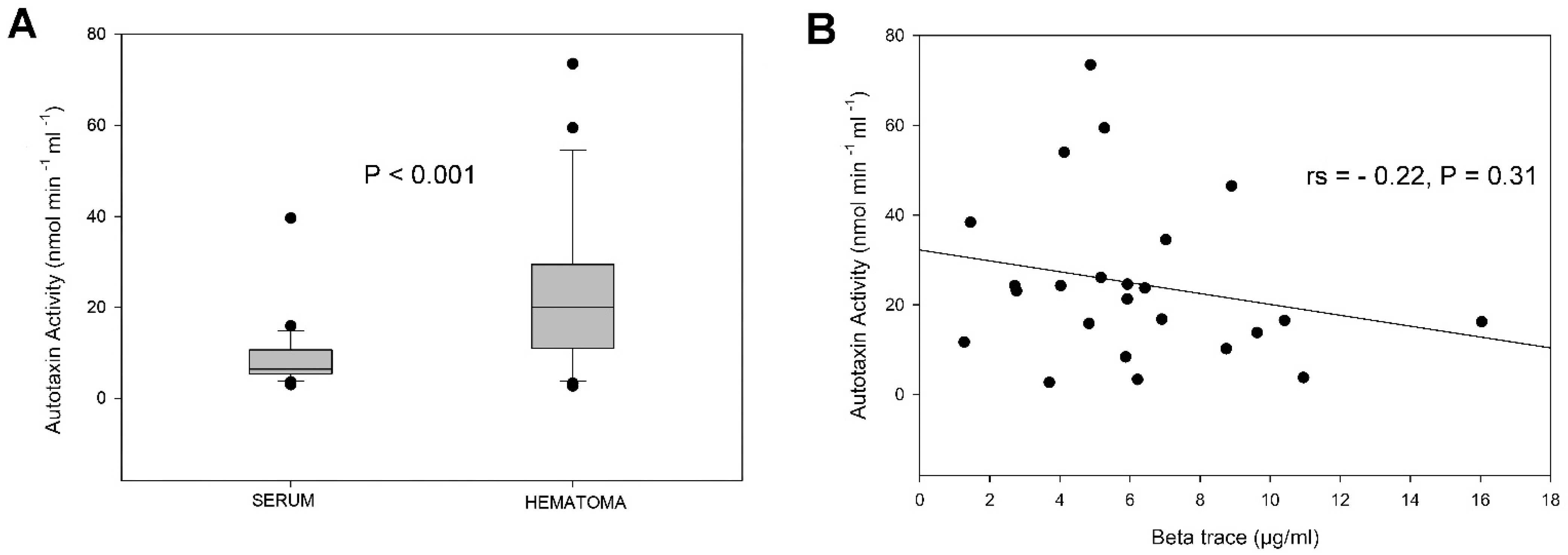
3.2. Autotaxin Activity and Beta Trace Levels
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stracke, M.; Liotta, L.A.; Schiffmann, E. The Role of Autotaxin and Other Motility Stimulating Factors in the Regulation of Tumor Cell Motility. Symp. Soc. Exp. Biol. 1993, 47, 197–214. [Google Scholar] [PubMed]
- Umezu-Goto, M.; Kishi, Y.; Taira, A.; Hama, K.; Dohmae, N.; Takio, K.; Yamori, T.; Mills, G.B.; Inoue, K.; Aoki, J.; et al. Autotaxin Has Lysophospholipase D Activity Leading to Tumor Cell Growth and Motility by Lysophosphatidic Acid Production. J. Cell Biol. 2002, 158, 227–233. [Google Scholar] [CrossRef] [PubMed]
- van Meeteren, L.A.; Ruurs, P.; Stortelers, C.; Bouwman, P.; van Rooijen, M.A.; Pradère, J.P.; Pettit, T.R.; Wakelam, M.J.O.; Saulnier-Blache, J.S.; Mummery, C.L.; et al. Autotaxin, a Secreted Lysophospholipase D, Is Essential for Blood Vessel Formation during Development. Mol. Cell. Biol. 2006, 26, 5015–5022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yukiura, H.; Kano, K.; Kise, R.; Inoue, A.; Aoki, J. Autotaxin Overexpression Causes Embryonic Lethality and Vascular Defects. PLoS ONE 2015, 10, e0126734. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, M.; Okudaira, S.; Kishi, Y.; Ohkawa, R.; Iseki, S.; Ota, M.; Noji, S.; Yatomi, Y.; Aoki, J.; Arai, H. Autotaxin Stabilizes Blood Vessels and Is Required for Embryonic Vasculature by Producing Lysophosphatidic Acid. J. Biol. Chem. 2006, 281, 25822–25830. [Google Scholar] [CrossRef] [Green Version]
- Sugden, M.; Holness, M. Lysophosphatidic Acid Effects on Atherosclerosis and Thrombosis. Clin. Lipidol. 2011, 6, 413–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benesch, M.G.K.; Ko, Y.M.; McMullen, T.P.W.; Brindley, D.N. Autotaxin in the Crosshairs: Taking Aim at Cancer and Other Inflammatory Conditions. FEBS Lett. 2014, 588, 2712–2727. [Google Scholar] [CrossRef] [Green Version]
- MacIntyre, I.; McMullen, T.; Brindley, D. Coming of Age for Autotaxin and Lysophosphatidate Signaling: Clinical Applications for Preventing, Detecting and Targeting Tumor-Promoting Inflammation. Cancers 2018, 10, 73. [Google Scholar] [CrossRef] [Green Version]
- Yasuda, D.; Kobayashi, D.; Akahoshi, N.; Ohto-Nakanishi, T.; Yoshioka, K.; Takuwa, Y.; Mizuno, S.; Takahashi, S.; Ishii, S. Lysophosphatidic Acid–Induced YAP/TAZ Activation Promotes Developmental Angiogenesis by Repressing Notch Ligand Dll4. J. Clin. Investig. 2019, 129, 4332–4349. [Google Scholar] [CrossRef]
- Feghali, J.; Yang, W.; Huang, J. Updates in Chronic Subdural Hematoma: Epidemiology, Etiology, Pathogenesis, Treatment, and Outcome. World Neurosurg. 2020, 141, 339–345. [Google Scholar] [CrossRef]
- Edlmann, E.; Giorgi-Coll, S.; Whitfield, P.C.; Carpenter, K.L.H.; Hutchinson, P.J. Pathophysiology of Chronic Subdural Haematoma: Inflammation, Angiogenesis and Implications for Pharmacotherapy. J. Neuroinflamm. 2017, 14, 108. [Google Scholar] [CrossRef] [PubMed]
- Kristof, R.A.; Grimm, J.M.; Stoffel-Wagner, B. Cerebrospinal Fluid Leakage into the Subdural Space: Possible Influence on the Pathogenesis and Recurrence Frequency of Chronic Subdural Hematoma and Subdural Hygroma. J. Neurosurg. 2008, 108, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Edlmann, E.; Whitfield, P.C.; Kolias, A.; Hutchinson, P.J. Pathogenesis of Chronic Subdural Hematoma: A Cohort Evidencing De Novo and Transformational Origins. J. Neurotrauma 2021, 38, 2580–2589. [Google Scholar] [CrossRef] [PubMed]
- Bolier, R.; Tolenaars, D.; Kremer, A.E.; Saris, J.; Parés, A.; Verheij, J.; Bosma, P.J.; Beuers, U.; Oude Elferink, R.P.J. Enteroendocrine Cells Are a Potential Source of Serum Autotaxin in Men. Biochim. Biophys. Acta BBA-Mol. Basis Dis. 2016, 1862, 696–704. [Google Scholar] [CrossRef]
- Nakamura, K.; Igarashi, K.; Ohkawa, R.; Okubo, S.; Yokota, H.; Kishimoto, T.; Ide, K.; Masuda, A.; Yamamoto, T.; Saito, N.; et al. Autotaxin Enzyme Immunoassay in Human Cerebrospinal Fluid Samples. Clin. Chim. Acta 2009, 405, 160–162. [Google Scholar] [CrossRef]
- Zahednasab, H.; Balood, M.; Harirchian, M.H.; Mesbah-Namin, S.A.; Rahimian, N.; Siroos, B. Increased Autotaxin Activity in Multiple Sclerosis. J. Neuroimmunol. 2014, 273, 120–123. [Google Scholar] [CrossRef]
- Link, T.W.; Rapoport, B.I.; Paine, S.M.; Kamel, H.; Knopman, J. Middle Meningeal Artery Embolization for Chronic Subdural Hematoma: Endovascular Technique and Radiographic Findings. Interv. Neuroradiol. 2018, 24, 455–462. [Google Scholar] [CrossRef]
- Omori, W.; Kano, K.; Hattori, K.; Kajitani, N.; Okada-Tsuchioka, M.; Boku, S.; Kunugi, H.; Aoki, J.; Takebayashi, M. Reduced Cerebrospinal Fluid Levels of Lysophosphatidic Acid Docosahexaenoic Acid in Patients With Major Depressive Disorder and Schizophrenia. Int. J. Neuropsychopharmacol. 2021, 24, 948–955. [Google Scholar] [CrossRef]
- Itagaki, K.; Takebayashi, M.; Abe, H.; Shibasaki, C.; Kajitani, N.; Okada-Tsuchioka, M.; Hattori, K.; Yoshida, S.; Kunugi, H.; Yamawaki, S. Reduced Serum and Cerebrospinal Fluid Levels of Autotaxin in Major Depressive Disorder. Int. J. Neuropsychopharmacol. 2019, 22, 261–269. [Google Scholar] [CrossRef] [Green Version]
- Ikeda, H.; Yatomi, Y. Autotaxin in Liver Fibrosis. Clin. Chim. Acta 2012, 413, 1817–1821. [Google Scholar] [CrossRef]
- Nakai, Y.; Ikeda, H.; Nakamura, K.; Kume, Y.; Fujishiro, M.; Sasahira, N.; Hirano, K.; Isayama, H.; Tada, M.; Kawabe, T.; et al. Specific increase in serum autotaxin activity in patients with pancreatic cancer. Clin. Biochem. 2011, 44, 576–581. [Google Scholar] [CrossRef] [PubMed]
- Kalamatianos, T.; Stavrinou, L.C.; Koutsarnakis, C.; Psachoulia, C.; Sakas, D.E.; Stranjalis, G. PlGF and SVEGFR-1 in Chronic Subdural Hematoma: Implications for Hematoma Development: Clinical Article. J. Neurosurg. 2013, 118, 353–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakaguchi, H.; Tanishima, T.; Yoshimasu, N. Factors in the Natural History of Chronic Subdural Hematomas That Influence Their Postoperative Recurrence. J. Neurosurg. 2001, 95, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Wunsch, E.; Krawczyk, M.; Milkiewicz, M.; Trottier, J.; Barbier, O.; Neurath, M.F.; Lammert, F.; Kremer, A.E.; Milkiewicz, P. Serum Autotaxin Is a Marker of the Severity of Liver Injury and Overall Survival in Patients with Cholestatic Liver Diseases. Sci. Rep. 2016, 6, 30847. [Google Scholar] [CrossRef] [PubMed]
- Yagi, T.; Shoaib, M.; Kuschner, C.; Nishikimi, M.; Becker, L.; Lee, A.; Kim, J. Challenges and Inconsistencies in Using Lysophosphatidic Acid as a Biomarker for Ovarian Cancer. Cancers 2019, 11, 520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, K.; Ohkawa, R.; Okubo, S.; Tozuka, M.; Okada, M.; Aoki, S.; Aoki, J.; Arai, H.; Ikeda, H.; Yatomi, Y. Measurement of Lysophospholipase D/Autotaxin Activity in Human Serum Samples. Clin. Biochem. 2007, 40, 274–277. [Google Scholar] [CrossRef]
- Nakamura, K.; Igarashi, K.; Ide, K.; Ohkawa, R.; Okubo, S.; Yokota, H.; Masuda, A.; Oshima, N.; Takeuchi, T.; Nangaku, M.; et al. Validation of an Autotaxin Enzyme Immunoassay in Human Serum Samples and Its Application to Hypoalbuminemia Differentiation. Clin. Chim. Acta 2008, 388, 51–58. [Google Scholar] [CrossRef]
- Reeves, V.L.; Trybula, J.S.; Wills, R.C.; Goodpaster, B.H.; Dubé, J.J.; Kienesberger, P.C.; Kershaw, E.E. Serum Autotaxin/ENPP2 Correlates with Insulin Resistance in Older Humans with Obesity: Serum Autotaxin and Insulin Resistance. Obesity 2015, 23, 2371–2376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miah, I.P.; Tank, Y.; Rosendaal, F.R.; Peul, W.C.; Dammers, R.; Lingsma, H.F.; den Hertog, H.M.; Jellema, K.; van der Gaag, N.A.; on behalf of the Dutch Chronic Subdural Hematoma Research Group. Radiological Prognostic Factors of Chronic Subdural Hematoma Recurrence: A Systematic Review and Meta-Analysis. Neuroradiology 2021, 63, 27–40. [Google Scholar] [CrossRef]
- Holl, D.C.; Volovici, V.; Dirven, C.M.F.; Peul, W.C.; van Kooten, F.; Jellema, K.; van der Gaag, N.A.; Miah, I.P.; Kho, K.H.; den Hertog, H.M.; et al. Pathophysiology and Nonsurgical Treatment of Chronic Subdural Hematoma: From Past to Present to Future. World Neurosurg. 2018, 116, 402–411.e2. [Google Scholar] [CrossRef]
- Castelino, F.V.; Bain, G.; Pace, V.A.; Black, K.E.; George, L.; Probst, C.K.; Goulet, L.; Lafyatis, R.; Tager, A.M. An Autotaxin/Lysophosphatidic Acid/Interleukin-6 Amplification Loop Drives Scleroderma Fibrosis: ATX/LPA/IL-6 amplification loop in SSc. Arthritis Rheumatol. 2016, 68, 2964–2974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakasaki, T.; Tanaka, T.; Okudaira, S.; Hirosawa, M.; Umemoto, E.; Otani, K.; Jin, S.; Bai, Z.; Hayasaka, H.; Fukui, Y.; et al. Involvement of the Lysophosphatidic Acid-Generating Enzyme Autotaxin in Lymphocyte-Endothelial Cell Interactions. Am. J. Pathol. 2008, 173, 1566–1576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, G.Y.; Lee, Y.G.; Berdyshev, E.; Nyenhuis, S.; Du, J.; Fu, P.; Gorshkova, I.A.; Li, Y.; Chung, S.; Karpurapu, M.; et al. Autotaxin Production of Lysophosphatidic Acid Mediates Allergic Asthmatic Inflammation. Am. J. Respir. Crit. Care Med. 2013, 188, 928–940. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.-L.; Lin, C.-I.; Huang, Y.-L.; Chen, P.-S.; Kuo, C.-H.; Chen, M.-S.; Wu, G.C.-C.; Shi, G.-Y.; Yang, H.-Y.; Lee, H. Lysophosphatidic Acid Stimulates Thrombomodulin Lectin-like Domain Shedding in Human Endothelial Cells. Biochem. Biophys. Res. Commun. 2008, 367, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Murakami, H.; Hirose, Y.; Sagoh, M.; Shimizu, K.; Kojima, M.; Gotoh, K.; Mine, Y.; Hayashi, T.; Kawase, T. Why Do Chronic Subdural Hematomas Continue to Grow Slowly and Not Coagulate? Role of Thrombomodulin in the Mechanism. J. Neurosurg. 2002, 96, 877–884. [Google Scholar] [CrossRef]
- On, N.H.; Savant, S.; Toews, M.; Miller, D.W. Rapid and Reversible Enhancement of Blood-Brain Barrier Permeability Using Lysophosphatidic Acid. J. Cereb. Blood Flow Metab. Off. J. Int. Soc. Cereb. Blood Flow Metab. 2013, 33, 1944–1954. [Google Scholar] [CrossRef]
- Hemmings, D.G.; Brindley, D.N. Signalling by Lysophosphatidate and Its Health Implications. Essays Biochem. 2020, 64, 547–563. [Google Scholar] [CrossRef]
- Frati, A.; Salvati, M.; Mainiero, F.; Ippoliti, F.; Rocchi, G.; Raco, A.; Caroli, E.; Cantore, G.; Delfini, R. Inflammation Markers and Risk Factors for Recurrence in 35 Patients with a Posttraumatic Chronic Subdural Hematoma: A Prospective Study. J. Neurosurg. 2004, 100, 24–32. [Google Scholar] [CrossRef] [Green Version]
- Onorato, J.M.; Shipkova, P.; Minnich, A.; Aubry, A.-F.; Easter, J.; Tymiak, A. Challenges in Accurate Quantitation of Lysophosphatidic Acids in Human Biofluids. J. Lipid Res. 2014, 55, 1784–1796. [Google Scholar] [CrossRef] [Green Version]
- Tan, Z.; Lei, H.; Guo, M.; Chen, Y.; Zhai, X. An Updated Patent Review of Autotaxin Inhibitors (2017–Present). Expert Opin. Ther. Pat. 2021, 31, 421–434. [Google Scholar] [CrossRef]
- Magkrioti, C.; Kaffe, E.; Stylianaki, E.-A.; Sidahmet, C.; Melagraki, G.; Afantitis, A.; Matralis, A.N.; Aidinis, V. Structure-Based Discovery of Novel Chemical Classes of Autotaxin Inhibitors. Int. J. Mol. Sci. 2020, 21, 7002. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Demographics and Medical History | Value |
|---|---|
| Age [median (IQR)] years | 80.5 (72–86) |
| Sex, N (%) | |
| Male | 16 (57.1) |
| Female | 12 (42.9) |
| Trauma, N (%) | |
| Remembered/Established | 17 (60.7) |
| Not Established | 11 (39.3) |
| CT findings, N (%) | |
| Unilateral | 20 (71.4) |
| Bilateral * | 8 (28.6) |
| Homogenous | 8 (8.6) |
| Non-homogenous ** | 20 (71.4) |
| Neurological Deficits, N (%) | |
| Hemiparesis | 16 (57.1) |
| Headache | 7 (25) |
| Disorientation | 4 (14.3) |
| Seizure | 1 (3.6) |
| Aphasia | 6 (21.4) |
| Dysarthria | 2 (7.1) |
| Antiplatelet or | |
| Anticoagulant | |
| YES | 13 (46.4) |
| NO | 15 (53.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalamatianos, T.; Drosos, E.; Magkrioti, C.; Nikitopoulou, I.; Koutsarnakis, C.; Kotanidou, A.; Paraskevas, G.P.; Aidinis, V.; Stranjalis, G. Autotaxin Activity in Chronic Subdural Hematoma: A Prospective Clinical Study. Diagnostics 2022, 12, 1865. https://doi.org/10.3390/diagnostics12081865
Kalamatianos T, Drosos E, Magkrioti C, Nikitopoulou I, Koutsarnakis C, Kotanidou A, Paraskevas GP, Aidinis V, Stranjalis G. Autotaxin Activity in Chronic Subdural Hematoma: A Prospective Clinical Study. Diagnostics. 2022; 12(8):1865. https://doi.org/10.3390/diagnostics12081865
Chicago/Turabian StyleKalamatianos, Theodosis, Evangelos Drosos, Christiana Magkrioti, Ioanna Nikitopoulou, Christos Koutsarnakis, Anastasia Kotanidou, George P. Paraskevas, Vassilis Aidinis, and George Stranjalis. 2022. "Autotaxin Activity in Chronic Subdural Hematoma: A Prospective Clinical Study" Diagnostics 12, no. 8: 1865. https://doi.org/10.3390/diagnostics12081865