
Diagnosis and Management of Febrile Neutropenia in Pediatric Oncology Patients—A Systematic Review

 , ,
, ,  ,
,
Abstract
:1. Introduction
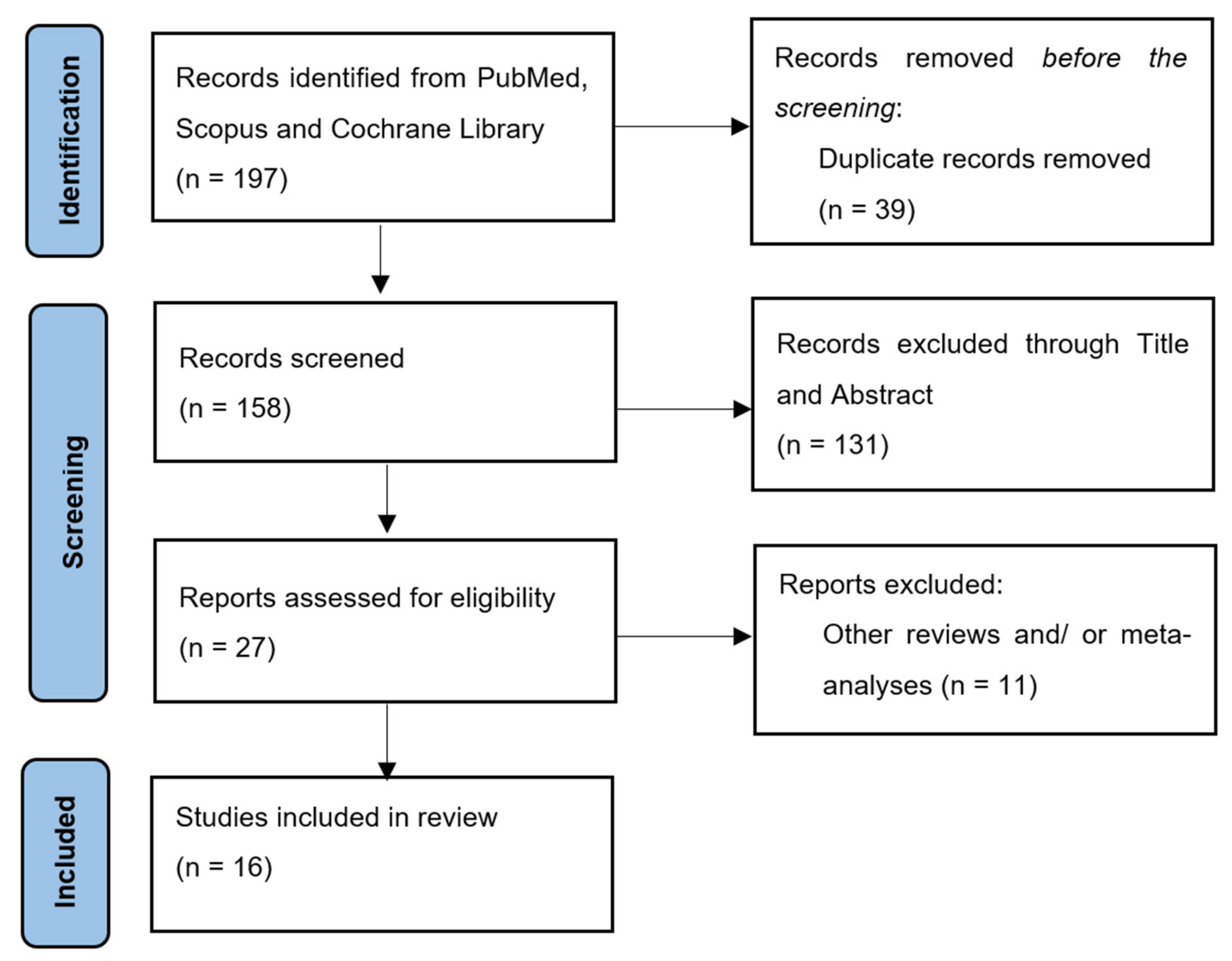
2. Materials and Methods
2.1. Study Design
- -
- Which is the optimal treatment strategy in cases of febrile neutropenia?
- -
- Which type of bacteria are most often involved in febrile neutropenia?
2.2. Selection Criteria
2.3. Data Extraction
2.4. Quality Assessment
3. Results
3.1. Overview
3.2. Definition of Febrile Neutropenia
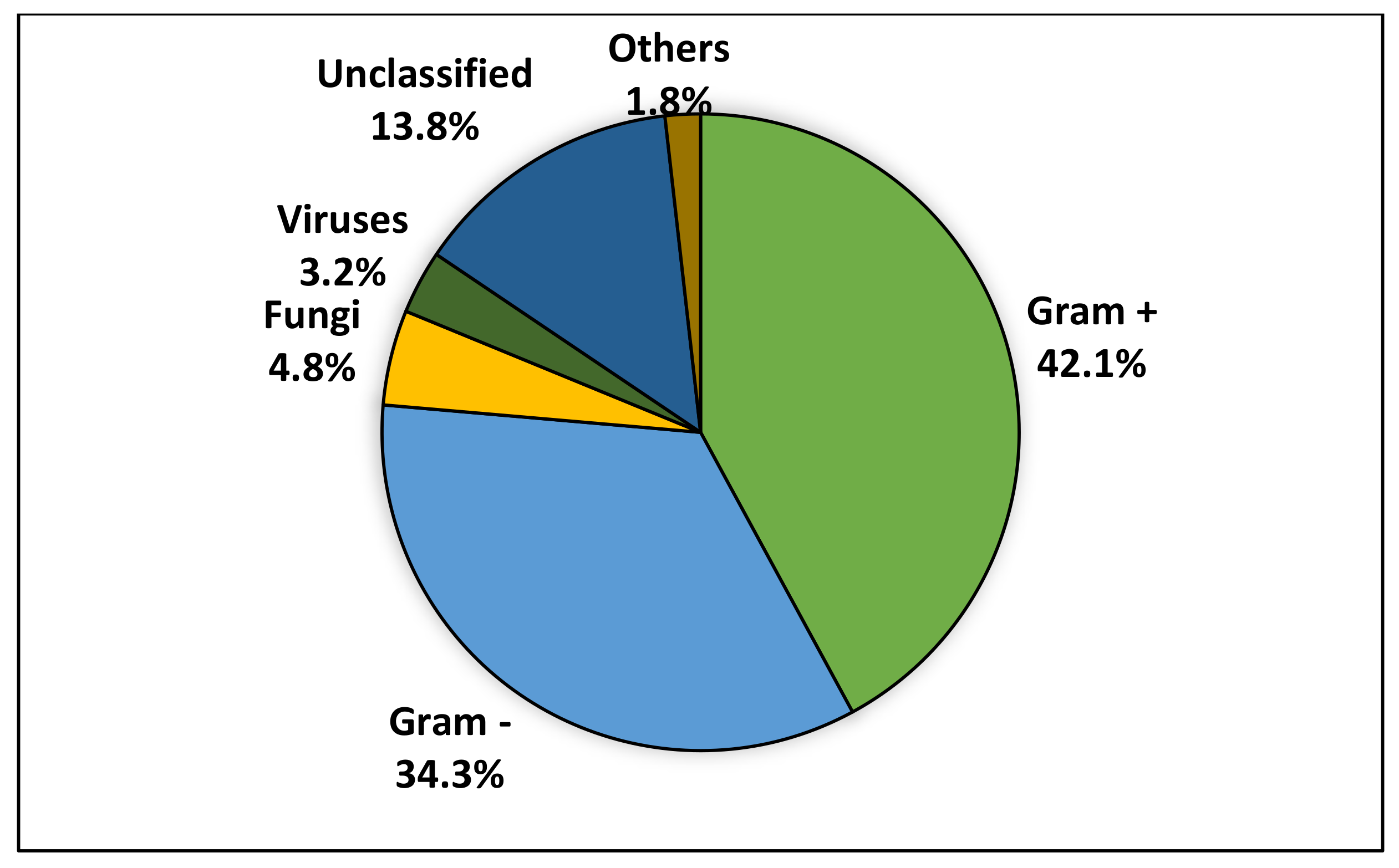
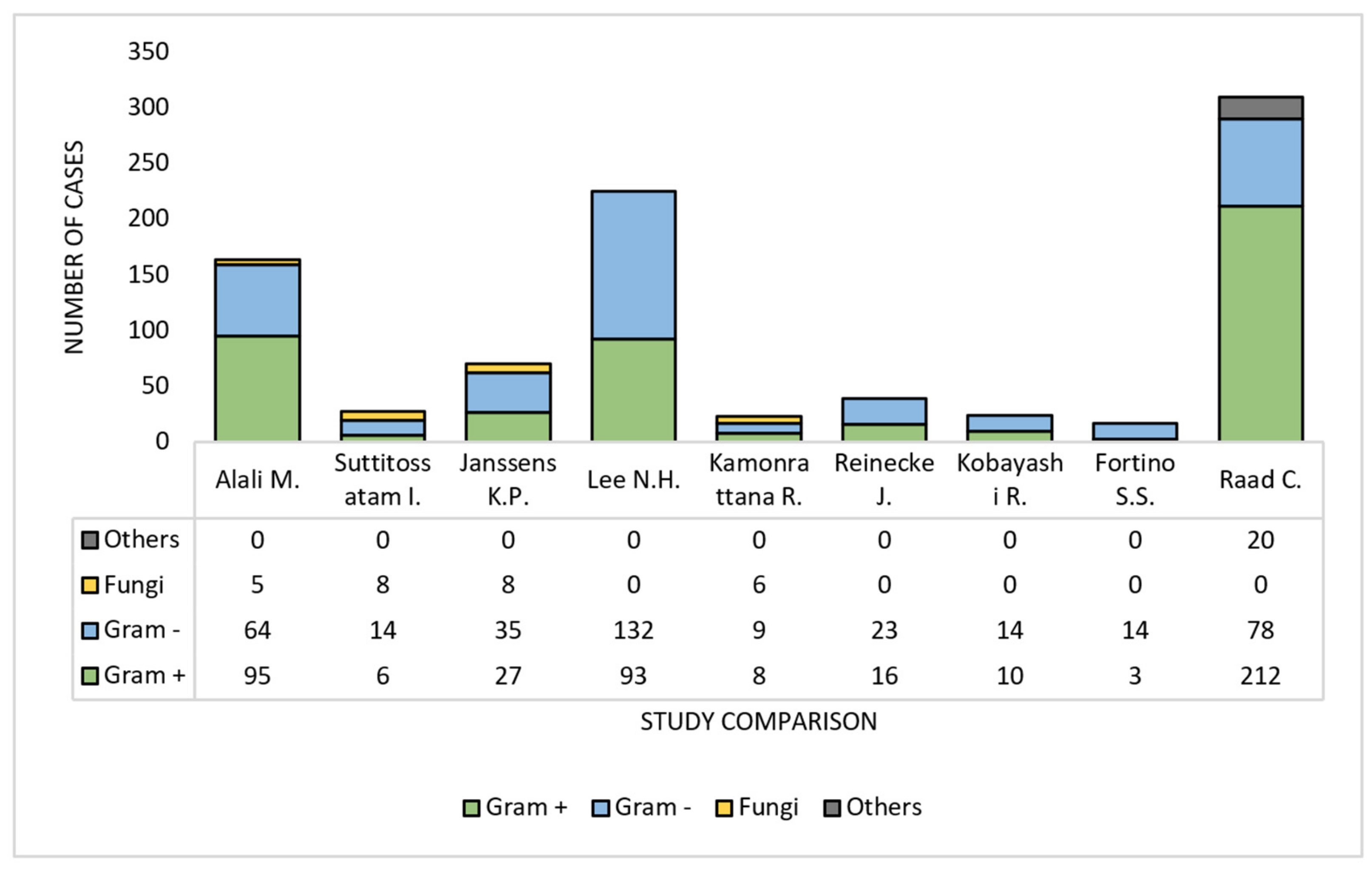
3.3. Microbiological Profile of FN
3.4. The Empirical Antibiotic of Choice
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lehrnbecher, T.; Averbuch, D.; Castagnola, E.; Cesaro, S.; Ammann, R.A.; Garcia-Vidal, C.; Kanerva, J.; Lanternier, F.; Mesini, A.; Mikulska, M.; et al. 8th European Conference on Infections in Leukaemia: 2020 guidelines for the use of antibiotics in paediatric patients with cancer or post-haematopoietic cell transplantation. Lancet Oncol. 2021, 22, e270–e280. [Google Scholar] [CrossRef]
- Mohammed, H.B.; Yismaw, M.B.; Fentie, A.M.; Tadesse, T.A. Febrile neutropenia management in pediatric cancer patients at Ethiopian Tertiary Care Teaching Hospital. BMC Res. Notes 2019, 12, 528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucas, A.J.; Olin, J.L.; Coleman, M.D. Management and Preventive Measures for Febrile Neutropenia. Pharm. Ther. 2018, 43, 228–232. [Google Scholar]
- Evaluation of risk stratification strategies in pediatric patients with febrile neutropenia. J. Pediatr. 2020, 97, 302–308.
- Long, S.S.; Prober, C.G.; Fischer, M. Principles and Practice of Pediatric Infectious Diseases; Elsevier: Amsterdam, The Netherlands, 2017; ISBN 9780323756082. [Google Scholar]
- Stephens, R.S. Neutropenic Fever in the Intensive Care Unit. In Oncologic Critical Care; Springer: Berlin/Heidelberg, Germany, 2019; pp. 1297–1311. [Google Scholar]
- Santolaya, M.E.; Alvarez, A.M.; Acuña, M.; Avilés, C.L.; Salgado, C.; Tordecilla, J.; Varas, M.; Venegas, M.; Villarroel, M.; Zubieta, M.; et al. Efficacy of pre-emptive versus empirical antifungal therapy in children with cancer and high-risk febrile neutropenia: A randomized clinical trial. J. Antimicrob. Chemother. 2018, 73, 2860–2866. [Google Scholar] [CrossRef] [PubMed]
- Lehrnbecher, T. Treatment of fever in neutropenia in pediatric oncology patients. Curr. Opin. Pediatr. 2019, 31, 35–40. [Google Scholar] [CrossRef]
- Suttitossatam, I.; Satayasai, W.; Sinlapamongkolkul, P.; Pusongchai, T.; Sritipsukho, P.; Surapolchai, P. Predictors of severe adverse outcomes in febrile neutropenia of pediatric oncology patients at a single institute in Thailand. Pediatr. Hematol. Oncol. 2020, 37, 561–572. [Google Scholar] [CrossRef]
- Tran, L.; Tam, D.N.H.; Elshafay, A.; Dang, T.; Hirayama, K.; Huy, N.T. Quality assessment tools used in systematic reviews of in vitro studies: A systematic review. BMC Med. Res. Methodol. 2021, 21, 101. [Google Scholar] [CrossRef]
- Gonzalez, M.L.; Aristizabal, P.; Loera-Reyna, A.; Torres, D.; Ornelas-Sánchez, M.; Nuño-Vázquez, L.; Aguilera, M.; Sánchez, A.; Romano, M.; Rivera-Gómez, R.; et al. The Golden Hour: Sustainability and Clinical Outcomes of Adequate Time to Antibiotic Administration in Children with Cancer and Febrile Neutropenia in Northwestern Mexico. JCO Glob. Oncol. 2021, 7, 659–670. [Google Scholar] [CrossRef]
- Schiavo, J.H. PROSPERO: An International Register of Systematic Review Protocols. Med Ref. Serv. Q. 2019, 38, 171–180. [Google Scholar] [CrossRef]
- Alali, M.; David, M.Z.; Danziger-Isakov, L.A.; Elmuti, L.; Bhagat, P.H.; Bartlett, A.H. Pediatric Febrile Neutropenia: Change in Etiology of Bacteremia, Empiric Choice of Therapy and Clinical Outcomes. J. Pediatric. Hematol. Oncol. 2020, 42, e445–e451. [Google Scholar] [CrossRef] [PubMed]
- Avilés-Robles, M.J.; Reyes-López, A.; Otero-Mendoza, F.J.; Valencia-Garin, A.U.; Peñaloza-González, J.G.; Rosales-Uribe, R.E.; Muñoz-Hernández, O.; Garduño-Espinosa, J.; Juárez-Villegas, L.; Zapata-Tarrés, M. Safety and efficacy of step-down to oral outpatient treatment versus inpatient antimicrobial treatment in pediatric cancer patients with febrile neutropenia: A noninferiority multicenter randomized clinical trial. Pediatric Blood Cancer 2020, 67, e28251. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 10, 1–11. [Google Scholar] [CrossRef]
- Lee, N.H.; Kang, J.-M.; Lee, J.W.; Huh, H.J.; Lee, N.Y.; Yoo, K.H.; Sung, K.W.; Koo, H.H.; Kim, Y.-J. Cefepime Versus Cefepime Plus Amikacin as an Initial Antibiotic Choice for Pediatric Cancer Patients with Febrile Neutropenia in an Era of Increasing Cefepime Resistance. Pediatr. Infect. Dis. J. 2020, 39, 931–936. [Google Scholar] [CrossRef] [PubMed]
- Alali, M.; David, M.Z.; Danziger-Isakov, L.A.; Bartlett, A.H.; Petty, L.A.; Schwartz, T.; Pisano, J. Association Between Depth of Neutropenia and Clinical Outcomes in Febrile Pediatric Cancer and/or Undergoing Hematopoietic Stem-cell Transplantation. Pediatr. Infect. Dis. J. 2020, 39, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Thangthong, J.; Anugulruengkitt, S.; Lauhasurayotin, S.; Chiengthong, K.; Poparn, H.; Sosothikul, D.; Techavichit, P. Predictive Factors of Severe Adverse Events in Pediatric Oncologic Patients with Febrile Neutropenia. Asian Pac. J. Cancer Prev. 2020, 21, 3487–3492. [Google Scholar] [CrossRef]
- Kamonrattana, R.; Sathitsamitphong, L.; Choeyprasert, W.; Charoenkwan, P.; Natesirinilkul, R.; Fanhchaksai, K. A Randomized, Open-Labeled, Prospective Controlled Study to Assess the Efficacy of Frontline Empirical Intravenous Piperacillin/Tazobactam Monotherapy in Comparison with Ceftazidime Plus Amikacin for Febrile Neutropenia in Pediatric Oncology Patients. Asian Pac. J. Cancer Prev. 2019, 20, 2733–2737. [Google Scholar] [CrossRef]
- Meena, J.P.; Gupta, A.K.; Seth, R. DNB Outcomes of Febrile Neutropenia in Children with Cancer Managed on an Outpatient Basis: A Report from Tertiary Care Hospital From a Resource-limited Setting. J. Pediatric Hematol. Oncol. 2020, 42, 467–473. [Google Scholar] [CrossRef]
- Haeusler, G.M.; Thursky, K.; Slavin, M.A.; Babl, F.E.; Lourenco, R.D.A.; Allaway, Z.; Mechinaud, F.; Phillips, R. Risk stratification in children with cancer and febrile neutropenia: A national, prospective, multicentre validation of nine clinical decision rules. eClinicalMedicine 2020, 18, 100220. [Google Scholar] [CrossRef] [Green Version]
- Reinecke, J.; Lowas, S.; Snowden, J.; Neemann, K. Blood Stream Infections and Antibiotic Utilization in Pediatric Leukemia Patients with Febrile Neutropenia. J. Pediatr. Hematol. 2018, 41, 251–255. [Google Scholar] [CrossRef]
- Kobayashi, R.; Sano, H.; Matsushima, S.; Hori, D.; Yanagi, M.; Kodama, K.; Suzuki, D.; Kobayashi, K. Meropenem versus piperacillin/tazobactam for febrile neutropenia in pediatric patients: Efficacy of piperacillin/tazobactam as a 1-h drip infusion four times a day. Int. J. Hematol. 2021, 113, 430–435. [Google Scholar] [CrossRef] [PubMed]
- Solórzano-Santos, F.; Quezada-Herrera, A.; Fuentes-Pacheco, Y.; Labra-Zamora, M.G.; Rodríguez-Coello, G.; Aguirre-Morales, C.E.; Izelo-Flores, D.; Muñoz-Hernández, O.; Miranda-Novales, M.G. Pperacillin/Tazobactam in continuous infusion versus intermittent infusion in children with febrile neutropenia. Rev. Investig. Clin. 2019, 71, 283–289. [Google Scholar]
- Raad, C.; Behdenna, A.; Fuhrmann, C.; Conter, C.; Cuzzubbo, D.; Rasigade, J.-P.; Bertrand, Y.; Domenech, C. Trends in bacterial bloodstream infections and resistance in immuno-compromised patients with febrile neutropenia: A retrospective analysis. Eur. J. Pediatr. 2021, 180, 2921–2930. [Google Scholar] [CrossRef] [PubMed]
- Lehrnbecher, T.; Robinson, P.; Fisher, B.; Alexander, S.; Ammann, R.A.; Beauchemin, M.; Carlesse, F.; Groll, A.H.; Haeusler, G.; Santolaya, M.; et al. Guideline for the Management of Fever and Neutropenia in Children with Cancer and Hematopoietic Stem-Cell Transplantation Recipients: 2017 Update. J. Clin. Oncol. 2017, 35, 2082–2094. [Google Scholar] [CrossRef] [Green Version]
- Melgar, M.; Reljic, T.; Barahona, G.; Camacho, K.; Chang, A.; Contreras, J.; Espinoza, D.; Estripeaut, D.; Gamero, M.; Luque, M.; et al. Guidance Statement for the Management of Febrile Neutropenia in Pediatric Patients Receiving Cancer-Directed Therapy in Central America and the Caribbean. JCO Glob. Oncol. 2020, 6, 508–517. [Google Scholar] [CrossRef]
- Haeusler, G.M.; Lourenco, R.D.A.; Clark, H.; Thursky, K.A.; Slavin, M.A.; Babl, F.E.; Mechinaud, F.; Alvaro, F.; Clark, J.; Padhye, B.; et al. Diagnostic Yield of Initial and Consecutive Blood Cultures in Children with Cancer and Febrile Neutropenia. J. Pediatr. Infect. Dis. Soc. 2021, 10, 125–130. [Google Scholar] [CrossRef]
- Meena, J.P.; Brijwal, M.; Seth, R.; Gupta, A.K.; Jethani, J.; Kapil, A.; Jat, K.R.; Choudhary, A.; Kabra, S.K.; Dwivedi, S.N.; et al. Prevalence and clinical outcome of respiratory viral infections among children with cancer and febrile neutropenia. Pediatr. Hematol. Oncol. 2019, 36, 330–343. [Google Scholar] [CrossRef]
- Masetti, R.; D’Amico, F.; Zama, D.; Leardini, D.; Muratore, E.; Ussowicz, M.; Fraczkiewicz, J.; Cesaro, S.; Caddeo, G.; Pezzella, V.; et al. Febrile Neutropenia Duration Is Associated with the Severity of Gut Microbiota Dysbiosis in Pediatric Allogeneic Hematopoietic Stem Cell Transplantation Recipients. Cancers 2022, 14, 1932. [Google Scholar] [CrossRef]
- Taplitz, R.A.; Kennedy, E.B.; Bow, E.J.; Crews, J.; Gleason, C.; Hawley, D.K.; Langston, A.A.; Nastoupil, L.J.; Rajotte, M.; Rolston, K.; et al. Outpatient Management of Fever and Neutropenia in Adults Treated for Malignancy: American Society of Clinical Oncology and Infectious Diseases Society of America Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 1443–1453. [Google Scholar] [CrossRef] [Green Version]
- Klastersky, J.; de Naurois, J.; Rolston, K.; Rapoport, B.; Maschmeyer, G.; Aapro, M.; Herrstedt, J.; on behalf of the ESMO Guidelines Committee. Management of febrile neutropaenia: ESMO Clinical Practice Guidelines. Ann. Oncol. 2016, 27, v111–v118. [Google Scholar] [CrossRef]
- Ornelas-Sánchez, M.; Nuño-Vázquez, L.; Loera-Reyna, A.; Torres-Reyes, D.; Rivera-Gómez, R.; Sánchez, A.; Romano, M.; González, M.; Caniza, M.A.; Aristizabal, P. The “Golden Hour”: A capacity-building initiative to decrease life-threating complications related to neutropenic fever in patients with hematologic malignancies in low- and middle-income countries. Blood Adv. 2018, 2 (Suppl. 1), 63–66. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| No. | Study Year | Study Type | No. of Studied FN Episodes | No. of Patients | Quality Score |
|---|---|---|---|---|---|
| 1 [11] | 2021 | Prospective observational | 204 | 105 | 11 |
| 2 [13] | 2020 | Retrospective cohort | 667 | 268 | 10 |
| 3 [7] | 2020 | Randomized multicentric clinical trial | 117 | 69 | 12 |
| 4 [2] | 2019 | Retrospective cross-sectional | 135 | 135 | 10 |
| 5 [14] | 2020 | Retrospective cohort | 95 | 95 | 11 |
| 6 [4] | 2020 | Retrospective cohort | 199 | 118 | 10 |
| 7 [16] | 2020 | Retrospective cohort | 225 | 164 | 10 |
| 8 [17] | 2020 | Retrospective cohort | 585 | 265 | 13 |
| 9 [18] | 2020 | Retrospective and prospective descriptive | 563 | 267 | 11 |
| 10 [19] | 2019 | Prospective randomized, open-labeled, controlled | 118 | 70 | 12 |
| 11 [20] | 2020 | Prospective cohort | 118 | 118 | 9 |
| 12 [21] | 2020 | Prospective, multicentric, non-interventional | 858 | 462 | 12 |
| 13 [22] | 2019 | Retrospective | 194 | 67 | 11 |
| 14 [23] | 2020 | Prospective, randomized | 394 | 99 | 10 |
| 15 [24] | 2019 | Non-blinded randomized controlled clinical trial | 100 vs. 76 | 176 | 10 |
| 16 [25] | 2021 | Retrospective monocentric descriptive | 310 | 186 | 11 |
| No. | Male % | Age * | Malignancy | ANC Before Treatment n (Mean) | Central Line n | Last Chemo-Therapy Range (Median) | Fever Days n (Median) |
|---|---|---|---|---|---|---|---|
| 1 [11] | 54.91 | 7.83 | Leukemia: 157, Lymphoma: 7, Others: 40 | <100: 95 (NR), 100–500: 86 (223) | NR | NR | NR |
| 2 [13] | 53.84 | 10 (median) | ALL 203, AML 115, lymphoma 68, neuroblastoma 110, others 171 | 667 (NR) | NR | <14 d: 43 | 1–20 (4) |
| 3 [7] | 41.02 | 7 | ALL 56%; Rhabdomyosarcoma 9%; AML 7% | 149 (264) | NR | NR | NR |
| 4 [2] | 68.88 | 5.5 | ALL: 71, AML: 10, NHL: 10, Blastomas: 17, Sarcomas: 15, Other: 12 | 135 (120) | NR | <14 d: 88 | NR |
| 5 [14] | 57.89 | 6 (median) | ALL: 57, AML 12, Non-leukemia: 26 | 95 (180) | 16 | 0–147 (8) | 0–30 (1) |
| 6 [4] | 49.2 | 8.8 | Leukemia: 23, Lymphoma: 7, Sarcoma: 29, Retinoblastoma: 7, Neuroblastoma: 6, Others: 45 | 199 (NR) | 180 | NR | NR |
| 7 [16] | 50.98 | 7.75 | ALL: 30, AML:41, Lymphoma: 25, Neuroblastoma: 33, Nephroblastomas: 5, Hepatoblastoma: 4, Other: 66 | <100: 184 (NR), <500: 194 (NR) | 154 | 1–23 (11) | 0–19 (1.2) |
| 8 [17] | NR | 11 | ALL: 173, AML: 84, Lymphoma: 66, Neuroblastoma: 103, Other: 117 | 204 (NR) | NR | 384 | NR |
| 9 [18] | 56.55 | 5.1 (median) | ALL: 114, AML: 44, Lymphoma: 20, Neuroblastoma: 17, Hepatoblastoma: 4, Retinoblastoma: 4, Sarcoma: 16, Other: 48 | 267 (170) | 226 | 0–148 (10) | 4.8 ± 4.7 (mean ± SD) |
| 10 [19] | 57.62 | 7 (median) | ALL: 55, AML:10, Lymphoma: 8, Neuroblastoma: 9, Sarcoma: 8 | 90 (122) | 0 | NR | 1–4 (2) |
| 11 [20] | 66.94 | 4.7 (median) | Hematological: 82, Solid tumors: 36 | 118 (110) | NR | <7 d: 85, >7 d: 33 | 4–6 (5) |
| 12 [21] | 51.63 | 5.8 (median) | ALL: 375, AML: 67, NHL: 55, Hodgkin: 11, Neuroblastoma: 48, Medulloblastoma: 37, Nephroblastoma: 19, Sarcoma: 177, Other: 88 | 858 (NR) | 845 | NR | NR |
| 13 [22] | 47.76 | 6.7 | ALL: 44, AML: 23 | 67 (NR) | 184 | NR | NR |
| 14 [23] | 63.63 | 9.9 (median) | ALL: 52, AML: 12, NHL:9, Solid tumors: 14, Other: 11 | 394 (103) | 380 | NR | NR |
| 15 [24] | 59.55 | 9.5 (median) | ALL: 24, AML: 10, NHL: 40, Solid tumors: 76, Other: 26) | 176 (NR) | NR | NR | NR |
| 16 [25] | NR | 5.3 | ALL: 79, AML: 21, NHL:11, Solid tumors: 114, Others: 37 | NR | 310 | NR | NR |
| No. | Infection Site | Hospital Stay/Duration of Antibiotic Therapy | Etiological Agent | MDR Strains | Most Frequent Bacterium |
|---|---|---|---|---|---|
| 1 [11] | Chest: 40, BSI: 14, GI: 29, Others: 36, Unknown: 69 | 13 ± 8.5 | Bacterial: 27 (64.5% G-), Viral: 7, Fungal: 3 | NR | Klebsiella pneumoniae |
| 2 [13] | BSI: 143 | NR | G+ 95, G- 64, Other Bacteria 17, Fungal: 5 | 21 | Alpha-hemolytic streptococcus: 35 |
| 3 [7] | NR | 4.25 ± 2.5 | NR | NR | NR |
| 4 [2] | Chest: 15, GI: 5, Urinary: 2, Unknown: 113 | NR | NR | NR | NR |
| 5 [14] | BSI: 12, Urinary: 8, GI: 2, Respiratory: 8, Other: 2 | NR | G- bacteria: 14, G+ bacteria: 5, Viral: 2, Fungal: 5 | 2 | Klebsiella pneumoniae |
| 6 [4] | NR | NR | G- bacteria: 35, G+ bacteria: 27, Fungal: 8 | NR | Klebsiella pneumoniae (14.2%) and Pseudomonas aeruginosa (14.2% |
| 7 [16] | BSI: 221, Skin/soft tissue: 14, GI: 30, Oral: 16, Other: 5 | 5 to 93 | G- bacteria: 132, G+ bacteria: 93 | 60 | Escherichia coli: 98 |
| 8 [17] | BSI: 141 | 10 (median) | G- bacteria: 64, G+ bacteria: 199, Fungal: 47 | NR | NR |
| 9 [18] | NR | NR | Bacterial: 154, Viral: 32, Fungal: 27 | NR | NR |
| 10 [19] | BSI: 6, Urinary: 11 | 7 to 12 | G- bacteria: 13, G+ bacteria: 4 | NR | Escherichia coli: 3 |
| 11 [20] | Respiratory: 81, GI: 10, Urinary: 1, Unknown: 26 | 5 to 11 | NR | NR | NR |
| 12 [18] | NR | NR | NR | NR | NR |
| 13 [22] | BSI: 67 | 2 to 24 | G- bacteria: 23, G+ bacteria: 16 | 5 | Escherichia coli: 10 |
| 14 [23] | NR | 2 to 19 | G- bacteria: 16, G+ bacteria: 8 | 4 | Staphylococcus. aureus: 4 |
| 15 [24] | NR | NR | G- bacteria: 14 | 2 | Pseudomonas aeruginosa: 5 |
| 16 [25] | BSI: 310 | 10 to 21 | G- bacteria: 25.2%, G+ bacteria: 68.4%, | 65 | Coagulase-Negative Staphylococci: 34 |
| No. | Most Used Antibiotic | Second Most Used Antibiotic | Time to Antibiotic Administration (min) | Treatment Modifications N | Other Anti-Infectious Medication |
|---|---|---|---|---|---|
| 1 [11] | Cefepime | Meropenem + Vancomycin | 47.17 | NR | NR |
| 2 [13] | Ceftazidime: 50% | Ceftazidime + Vancomycin: 33% | NR | NR | Antifungals |
| 3 [7] | Cefepime | Cefixime | NR | 3 | NA |
| 4 [2] | Ceftriaxone + Gentamycin: 97 | Ceftriaxone: 6 | NR | 22 | Antiviral: 30, Antifungal: 52 |
| 5 [14] | Ceftazidime + Amikacin | Piperacillin/Tazobactam | <120 | NR | NR |
| 6 [4] | Cefepime | Meropenem or Piperacillin/Tazobactam | NR | NR | NR |
| 7 [16] | Cefepime: 121 | Cefepime + Amikacin: 83 | 120 (median) | 57 | NR |
| 8 [17] | Ceftazidime + Vancomycin | Cefepime + Vancomycin | NR | NR | Antifungals |
| 9 [18] | NR | NR | NR | NR | Antifungal: 123 |
| 10 [19] | Piperacillin/Tazobactam: 59 | Ceftazidime + Amikacin: 59 | 30 | 44 | Antifungal: 21 |
| 11 [20] | Amoxicillin/Clavulanate + Amikacin (respiratory), Cefoperazone/Sulbactam + Metronidazole (GI) | Meropenem + Vancomycin or Teicoplanin | NR | 34 | Antifungal: 19 |
| 12 [21] | NR | NR | 552 | NR | Antiviral: 72, Antifungal: 290 |
| 13 [22] | Cefepime: 157 | Cefepime + Vancomycin: 16 | NR | 35 | NA |
| 14 [23] | Meropenem: 200 | Piperacillin/Tazobactam: 193 | NR | NA | NA |
| 15 [24] | Intermittent Piperacillin/Tazobactam: 100 | Continuous Piperacillin/Tazobactam: 76 | NR | 6 | NA |
| 16 [25] | Vancomycin: 134 | Amikacin: 90 | NR | NR | Antifungal: 44 |
| No. | Persistent Fever | Central Line Removal | Sepsis | ICU | Deaths | Treated |
|---|---|---|---|---|---|---|
| 1 [11] | NR | NR | 32 | 23 | 4 | 200 |
| 2 [13] | NR | NR | NR | 4 | 35 | 139 |
| 3 [7] | 1 | NR | NR | NR | 0 | 117 |
| 4 [2] | 2 | NR | NR | NR | 7 | 95 |
| 5 [14] | NR | NR | 3 | 11 | 0 | 95 |
| 6 [4] | NR | NR | NR | 8 | 1 | 117 |
| 7 [16] | NR | 1 | 16 | 4 | 0 | 225 |
| 8 [17] | NR | NR | NR | 87 | 8 | 577 |
| 9 [18] | NR | NR | NR | 78 | 21 | 542 |
| 10 [19] | NR | NR | NA | NR | 0 | 118 |
| 11 [20] | 11 | NR | 5 | 8 | 6 | 112 |
| 12 [21] | NR | NR | 13 | 24 | 4 | 424 |
| 13 [22] | NR | 1 | 1 | 5 | 1 | 66 |
| 14 [23] | NR | NR | NR | NR | 0 | 288 |
| 15 [24] | 1 | NR | 1 | NR | 2 | 136 |
| 16 [25] | NR | 60 | 14 | 0 | 0 | 310 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boeriu, E.; Borda, A.; Vulcanescu, D.D.; Sarbu, V.; Arghirescu, S.T.; Ciorica, O.; Bratosin, F.; Marincu, I.; Horhat, F.G. Diagnosis and Management of Febrile Neutropenia in Pediatric Oncology Patients—A Systematic Review. Diagnostics 2022, 12, 1800. https://doi.org/10.3390/diagnostics12081800
Boeriu E, Borda A, Vulcanescu DD, Sarbu V, Arghirescu ST, Ciorica O, Bratosin F, Marincu I, Horhat FG. Diagnosis and Management of Febrile Neutropenia in Pediatric Oncology Patients—A Systematic Review. Diagnostics. 2022; 12(8):1800. https://doi.org/10.3390/diagnostics12081800
Chicago/Turabian StyleBoeriu, Estera, Alexandra Borda, Dan Dumitru Vulcanescu, Vlad Sarbu, Smaranda Teodora Arghirescu, Ovidiu Ciorica, Felix Bratosin, Iosif Marincu, and Florin George Horhat. 2022. "Diagnosis and Management of Febrile Neutropenia in Pediatric Oncology Patients—A Systematic Review" Diagnostics 12, no. 8: 1800. https://doi.org/10.3390/diagnostics12081800