
Molecular Epidemiology of Genital Infections in Campania Region: A Retrospective Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Specimen Collection
2.2. Molecular Testing for GIs Detection
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Study Subjects
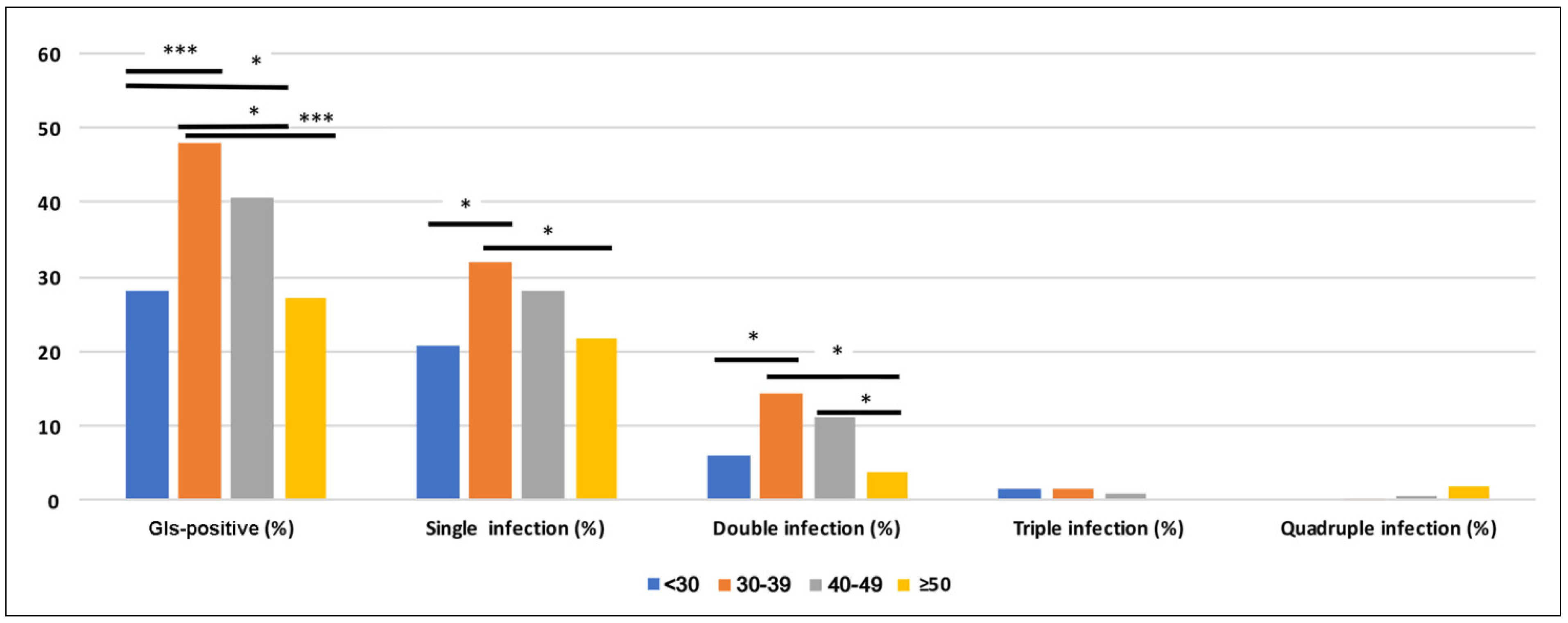
3.2. Prevalence of Single and Multiple Infections
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Farsimadan, M.; Motamedifar, M. Bacterial infection of the male reproductive system causing infertility. J. Reprod. Immunol. 2020, 142, 103183. [Google Scholar] [CrossRef] [PubMed]
- Henkel, R. Long-term consequences of sexually transmitted infections on men’s sexual function: A systematic review. Arab. J. Urol. 2021, 19, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Moragianni, D.; Dryllis, G.; Andromidas, P.; Kapeta-Korkouli, R.; Kouskouni, E.; Pessach, I.; Papalexis, P.; Kodonaki, A.; Athanasiou, N.; PouliakAis, A.; et al. Genital tract infection and associated factors affect the reproductive outcome in fertile females and females undergoing in vitro fertilization. Biomed. Rep. 2019, 10, 231–237. [Google Scholar] [CrossRef]
- Huang, C.; Zhu, H.L.; Xu, K.R.; Wang, S.Y.; Fan, L.Q.; Zhu, W.B. Mycoplasma and ureaplasma infection and male infertility: A systematic review and meta-analysis. Andrology 2015, 3, 809–816. [Google Scholar] [CrossRef]
- Stary, A. The changing spectrum of sexually transmitted infections in Europe. Acta Derm. Venereol. 2020, 100, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Casillas-Vega, N.; Morfín-Otero, R.; García, S.; Llaca-Díaz, J.; Rodríguez-Noriega, E.; Camacho-Ortiz, A.; Ayala-Castellanos, M.L.; Mendoza-Olazarán, S.; Flores-Treviño, S.; Petersen-Morfín, S.; et al. Sexually transmitted pathogens, coinfections and risk factors in patients attending obstetrics and gynecology clinics in Jalisco, Mexico. Salud Publica Mex. 2016, 58, 437–445. [Google Scholar] [CrossRef] [Green Version]
- Rowley, J.; Vander Hoorn, S.; Korenromp, E.; Low, N.; Unemo, M.; Abu-Raddad, L.J.; Chico, R.M.; Smolak, A.; Newman, L.; Gottlieb, S.; et al. Chlamydia, gonorrhoea, trichomoniasis and syphilis: Global prevalence and incidence estimates, 2016. Bull. World Health Organ. 2019, 97, 548–562. [Google Scholar] [CrossRef]
- World Health Organization. Global Health Sector Strategy on Sexually Transmitted Infections 2016–2021; Towards ending STIs. Report No.: WHO/RHR/16.09; WHO: Geneva, Switezrland, 2016. [Google Scholar]
- Raj, J.S.; Rawre, J.; Dhawan, N.; Khanna, N.; Dhawan, B. Mycoplasma genitalium: A new superbug. Indian J. Sex Transm. Dis. AIDS 2022, 43, 1–12. [Google Scholar]
- Deguchi, T.; Yoshida, T.; Miyazawa, T.; Yasuda, M.; Tamaki, M.; Ishiko, H.; Maeda, S. Association of Ureaplasma urealyticum (biovar 2) with nongonococcal urethritis. Sex Transm. Dis. 2004, 31, 192–195. [Google Scholar] [CrossRef]
- Moodley, P.; Wilkinson, D.; Connolly, C.; Moodley, J.; Sturm, A.W. Trichomonas vaginalis is associated with pelvic inflammatory disease in women infected with human immunodeficiency virus. Clin. Infect. Dis. 2002, 34, 519–522. [Google Scholar] [CrossRef] [Green Version]
- Steinhandler, L.; Peipert, J.F.; Heber, W.; Montagno, A.; Cruickshank, C. Combination of bacterial vaginosis and leukorrhea as a predictor of cervical chlamydial or gonococcal infection. Obstet. Gynecol. 2002, 99, 603–607. [Google Scholar] [PubMed]
- Waites, K.B.; Xiao, L.; Paralanov, V.; Viscardi, R.M.; Glass, J.I. Molecular methods for the detection of Mycoplasma and ureaplasma infections in humans: A paper from the 2011 William Beaumont Hospital Symposium on molecular pathology. J. Mol. Diagn. 2012, 14, 437–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsen, B.; DeSeta, F.; Hwang, J.; Merialdi, M.; Tirán-Saucedo, J. Infectious diseases and prematurity. Infect. Dis. Obstet. Gynecol. 2010, 2010, 163046. [Google Scholar] [CrossRef] [Green Version]
- Sieving, R.E.; Gewirtz O’Brien, J.R.; Saftner, M.A.; Argo, T.A. Sexually Transmitted Diseases Among US Adolescents and Young Adults: Patterns, Clinical Considerations, and Prevention. Nurs. Clin. N. Am. 2019, 54, 207–225. [Google Scholar] [CrossRef] [PubMed]
- Pagliuca, C.; Cariati, F.; Bagnulo, F.; Scaglione, E.; Carotenuto, C.; Farina, F.; D’Argenio, V.; Carraturo, F.; D’Aprile, P.; Vitiello, M.; et al. Microbiological Evaluation and Sperm DNA Fragmentation in Semen Samples of Patients Undergoing Fertility Investigation. Genes 2021, 12, 654. [Google Scholar] [CrossRef]
- Amabebe, E.; Anumba, D.O.C. The Vaginal Microenvironment: The Physiologic Role of Lactobacilli. Front. Med. 2018, 5, 181. [Google Scholar] [CrossRef] [Green Version]
- Marchesi, J.R.; Ravel, J. The vocabulary of microbiome research: A proposal. Microbiome 2015, 3, 31. [Google Scholar] [CrossRef] [Green Version]
- Edwards, T.; Burke, P.; Smalley, H.; Hobbs, G. Trichomonas vaginalis: Clinical relevance, pathogenicity and diagnosis. Crit. Rev. Microbiol. 2016, 42, 406–417. [Google Scholar] [CrossRef]
- Nateghi Rostami, M.; Hossein Rashidi, B.; Habibi, A.; Nazari, R.; Dolati, M. Genital infections and reproductive complications associated with Trichomonas vaginalis, Neisseria gonorrhoeae, and Streptococcus agalactiae in women of Qom, central Iran. Int. J. Reprod. Biomed. 2017, 15, 357–366. [Google Scholar] [CrossRef] [Green Version]
- Ginocchio, C.C.; Chapin, K.; Smith, J.S.; Aslanzadeh, J.; Snook, J.; Hill, C.S.; Gaydos, C.A. Prevalence of Trichomonas vaginalis and coinfection with Chlamydia trachomatis and Neisseria gonorrhoeae in the United States as determined by the Aptima Trichomonas vaginalis nucleic acid amplification assay. J. Clin. Microbiol. 2012, 50, 2601–2608. [Google Scholar] [CrossRef] [Green Version]
- Leli, C.; Mencacci, A.; Latino, M.A.; Clerici, P.; Rassu, M.; Perito, S.; Castronari, R.; Pistoni, E.; Luciano, E.; De Maria, D.; et al. Prevalence of cervical colonization by Ureaplasma parvum, Ureaplasma urealyticum, Mycoplasma hominis and Mycoplasma genitalium in childbearing age women by a commercially available multiplex real-time PCR: An Italian observational multicentre study. J. Microbiol. Immunol. Infect. 2018, 51, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Martín-Saco, G.; Tristancho, A.; Arias, A.; Ferrer, I.; Milagro, A.; García-Lechuz, J.M. Mycoplasma genitalium and sexually transmitted infections: Evidences and figures in a tertiary hospital. Rev. Esp. Quimioter. 2022, 35, 76–79. [Google Scholar] [CrossRef] [PubMed]
- Kriesel, J.D.; Bhatia, A.S.; Barrus, C.; Vaughn, M.; Gardner, J.; Crisp, R.J. Multiplex PCR testing for nine different sexually transmitted infections. Int. J. STD AIDS 2016, 27, 1275–1282. [Google Scholar] [CrossRef] [PubMed]
- Xiu, L.; Zhang, C.; Li, Y.; Wang, F.; Peng, J. Simultaneous detection of eleven sexually transmitted agents using multiplexed PCR coupled with MALDI-TOF analysis. Infect. Drug. Resist. 2019, 12, 2671–2682. [Google Scholar] [CrossRef] [Green Version]
- Hu, X.M.; Xu, J.X.; Jiang, L.X.; Deng, L.R.; Gu, Z.M.; Xie, X.Y.; Ji, H.C.; Wang, W.H.; Li, L.M.; Tian, C.N.; et al. Design and Evaluation of a Novel Multiplex Real-Time PCR Melting Curve Assay for the Simultaneous Detection of Nine Sexually Transmitted Disease Pathogens in Genitourinary Secretions. Front. Cell Infect. Microbiol. 2019, 9, 382. [Google Scholar] [CrossRef] [PubMed]
- Fischer, N.; Peeters, I.; Klamer, S.; Montourcy, M.; Cuylaerts, V.; Van Beckhoven, D.; De Baetselier, I.; Van der Heyden, J.; Vanden Berghe, W. Prevalence estimates of genital Chlamydia trachomatis infection in Belgium: Results from two cross-sectional studies. BMC Infect. Dis. 2021, 21, 947. [Google Scholar] [CrossRef]
- U.S. Preventive Services Task Force. Screening for chlamydial infection-recommendations statement. Ann. Intern. Med. 2007, 76, 1695–1698. [Google Scholar]
- Fasciana, T.; Capra, G.; Di Carlo, P.; Calà, C.; Vella, M.; Pistone, G.; Colomba, C.; Giammanco, A. Socio-Demographic Characteristics and Sexual Behavioral Factors of Patients with Sexually Transmitted Infections Attending a Hospital in Southern Italy. Int. J. Environ. Res. Public Health 2021, 18, 4722. [Google Scholar] [CrossRef]
- Wellings, K.; Collumbien, M.; Slaymaker, E.; Singh, S.; Hodges, Z.; Patel, D.; Bajos, N. Sexual behaviour in context: A global perspective. Lancet 2006, 368, 1706–1728. [Google Scholar] [CrossRef]
- Vitale, S.G.; Ferrari, F.; Ciebiera, M.; Zgliczyńska, M.; Rapisarda, A.M.C.; Vecchio, G.M.; Pino, A.; Angelico, G.; Knafel, A.; Riemma, G.; et al. The Role of Genital Tract Microbiome in Fertility: A Systematic Review. Int. J. Mol. Sci. 2021, 23, 180. [Google Scholar] [CrossRef]
- Sarshar, M.; Behzadi, P.; Ambrosi, C.; Zagaglia, C.; Palamara, A.T.; Scribano, D. FimH and Anti-Adhesive Therapeutics: A Disarming Strategy Against Uropathogens. Antibiotics 2020, 9, 397. [Google Scholar] [CrossRef] [PubMed]
- López de Munain, J. Epidemiology and current control of sexually transmitted infections. The role of STI clinics. Enferm. Infect. Microbiol. Clin. 2019, 37, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Cox, C.; Watt, A.P.; McKenna, J.P.; Coyle, P.V. Mycoplasma hominis and Gardnerella vaginalis display a significant synergistic relationship in bacterial vaginosis. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 481–487. [Google Scholar] [CrossRef]
- Muzny, C.A.; Łaniewski, P.; Schwebke, J.R.; Herbst-Kralovetz, M.M. Host-vaginal microbiota interactions in the pathogenesis of bacterial vaginosis. Curr. Opin. Infect. Dis. 2020, 33, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Abou Chacra, L.; Fenollar, F.; Diop, K. Bacterial Vaginosis: What Do We Currently Know? Front. Cell Infect. Microbiol. 2022, 11, 672429. [Google Scholar] [CrossRef] [PubMed]
- McKechnie, M.L.; Hillman, R.J.; Jones, R.; Lowe, P.C.; Couldwell, D.L.; Davies, S.C.; King, F.; Kong, F.; Gilbert, G.L. The prevalence of urogenital micro-organisms detected by a multiplex PCR-reverse line blot assay in women attending three sexual health clinics in Sydney, Australia. J. Med. Microbiol. 2011, 60, 1010–1016. [Google Scholar] [CrossRef]
- Cassell, G.H.; Waites, K.B.; Watson, H.L.; Crouse, D.T.; Harasawa, R. Ureaplasma urealyticum intrauterine infection: Role in prematurity and disease in newborns. Clin. Microbiol. Rev. 1993, 6, 69–87. [Google Scholar] [CrossRef]
- Taylor-Robinson, D. Mollicutes in vaginal microbiology: Mycoplasma hominis, Ureaplasma urealyticum, Ureaplasma parvum and Mycoplasma genitalium. Res. Microbiol. 2017, 168, 875–881. [Google Scholar] [CrossRef]
- Combaz-Söhnchen, N.; Kuhn, A. A Systematic Review of Mycoplasma and Ureaplasma in Urogynaecology. Geburtshilfe Frauenheilkd. 2017, 77, 1299–1303. [Google Scholar] [CrossRef] [Green Version]
- García-Castillo, M.; Morosini, M.I.; Gálvez, M.; Baquero, F.; del Campo, R.; Meseguer, M.A. Differences in biofilm development and antibiotic susceptibility among clinical Ureaplasma urealyticum and Ureaplasma parvum isolates. J. Antimicrob. Chemother. 2008, 62, 1027–1030. [Google Scholar] [CrossRef] [Green Version]
- Beeton, M.L.; Payne, M.S.; Jones, L. The Role of Ureaplasma spp. in the Development of Nongonococcal Urethritis and Infertility among Men. Clin. Microbiol. Rev. 2019, 32, e00137-18. [Google Scholar] [CrossRef] [PubMed]
- Capoccia, R.; Greub, G.; Baud, D. Ureaplasma urealyticum, Mycoplasma hominis and adverse pregnancy outcomes. Curr. Opin. Infect. Dis. 2013, 26, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, E.L.; Dando, S.J.; Kallapur, S.G.; Knox, C.L. The human Ureaplasma species as causative agents of chorioamnionitis. Clin. Microbiol. Rev. 2017, 30, 349–379. [Google Scholar] [CrossRef] [Green Version]
- Patel, M.A.; Nyirjesy, P. Role of Mycoplasma and ureaplasma species in female lower genital tract infections. Curr. Infect. Dis. Rep. 2010, 12, 417–422. [Google Scholar] [CrossRef]
- Iovene, M.R.; Martora, F.; Mallardo, E.; De Sio, M.; Arcaniolo, D.; Del Vecchio, C.; Pagliuca, C.; Signoriello, G.; Vitiello, M. Enrichment of semen culture in the diagnosis of bacterial prostatitis. J. Microbiol. Methods 2018, 154, 124–126. [Google Scholar] [CrossRef] [PubMed]
- Guven, M.A.; Gunyeli, I.; Dogan, M.; Ciragil, P.; Bakaris, S.; Gul, M. The demographic and behavioural profile of women with cervicitis infected with Chlamydia trachomatis, Mycoplasma hominis and Ureaplasma urealyticum and the comparison of two medical regimens. Arch. Gynecol. Obstet. 2005, 272, 197–200. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics of the Whole Population (717) | Patients Positive for Genital Pathogens Detection (302) | Patients Negative for Genital Pathogens Detection (415) | Chi Square Fisher’s Exact Test p-Value |
|---|---|---|---|
| Women: 363 (50.63%) | 190/302 (62.91%) | 173/415 (41.68%) | <0.001 |
| Men: 354 (49.37%) | 112/302 (37.08%) | 242/415 (58.31%) | <0.001 |
| Women (years ± SD) | 36.91 ± 5.23 | 37.67 ± 10.41 | 0.375 |
| Men (years ± SD) | 38.69 ± 8.26 | 39.85 ± 8.98 | 0.243 |
| Mean age (years ± SD) | 37.59 ± 6.60 | 38.92 ± 9.66 | 0.145 |
| Multiple GIs | SF + SM N (%) | |
|---|---|---|
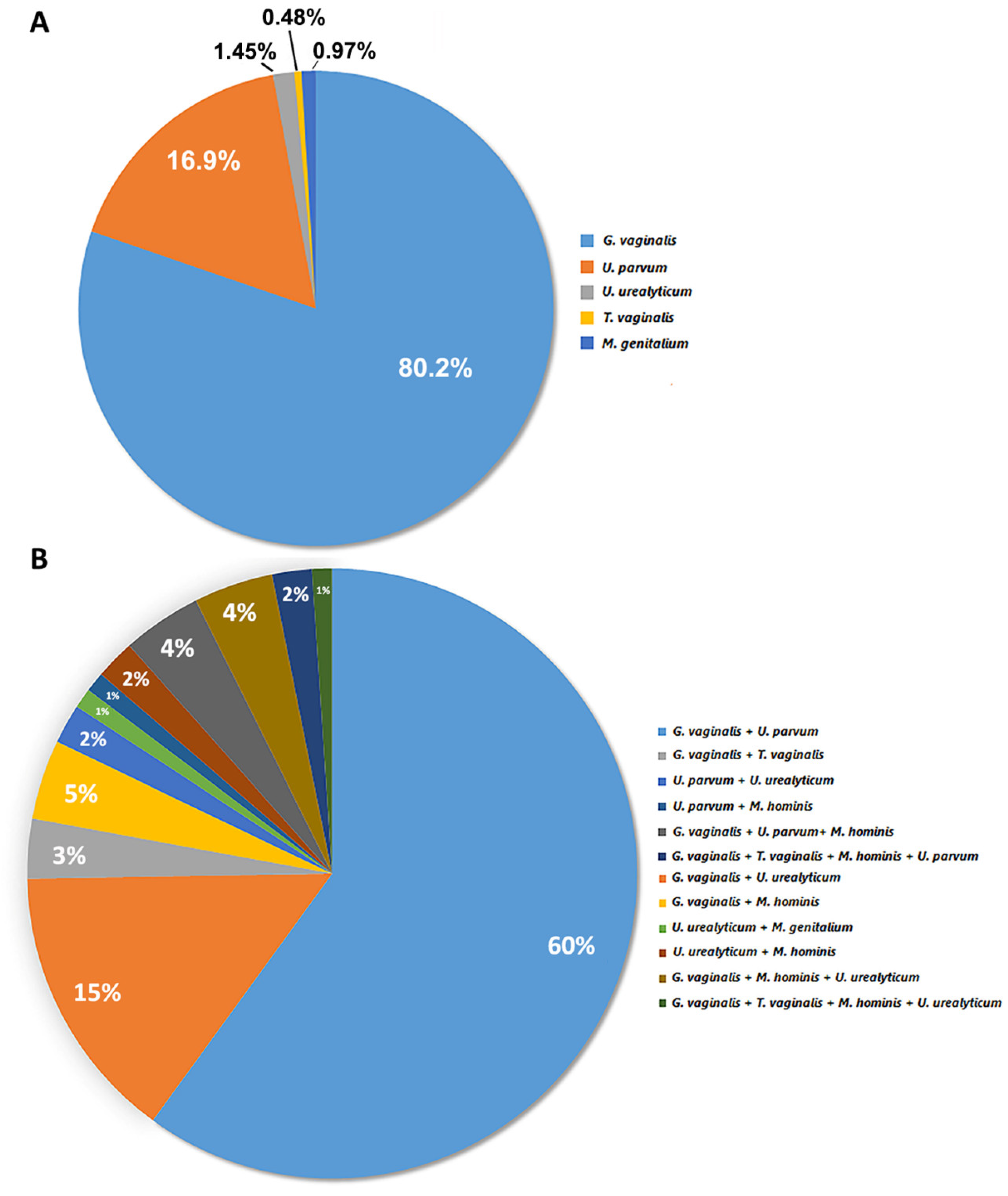
| Double infections | G. vaginalis + U. parvum | 57 (60%) |
| G. vaginalis + U. urealyticum | 14 (15%) | |
| Other | 13 (14%) | |
| Triple infections | G. vaginalis + U. parvum + M. hominis | 4 (4%) |
| G. vaginalis + U. urealyticum + M. hominis | 4 (4%) | |
| Quadruple infections | G. vaginalis + T. vaginalis+ M. hominis + U. parvum | 2 (2%) |
| G. vaginalis + T. vaginalis + M. hominis + U. urealyticum | 1 (1%) | |
| Total samples | 95 (100%) |
| Microorganisms | SF N (%) | SM N (%) | Chi-Square Fisher’s Exact Test |
|---|---|---|---|
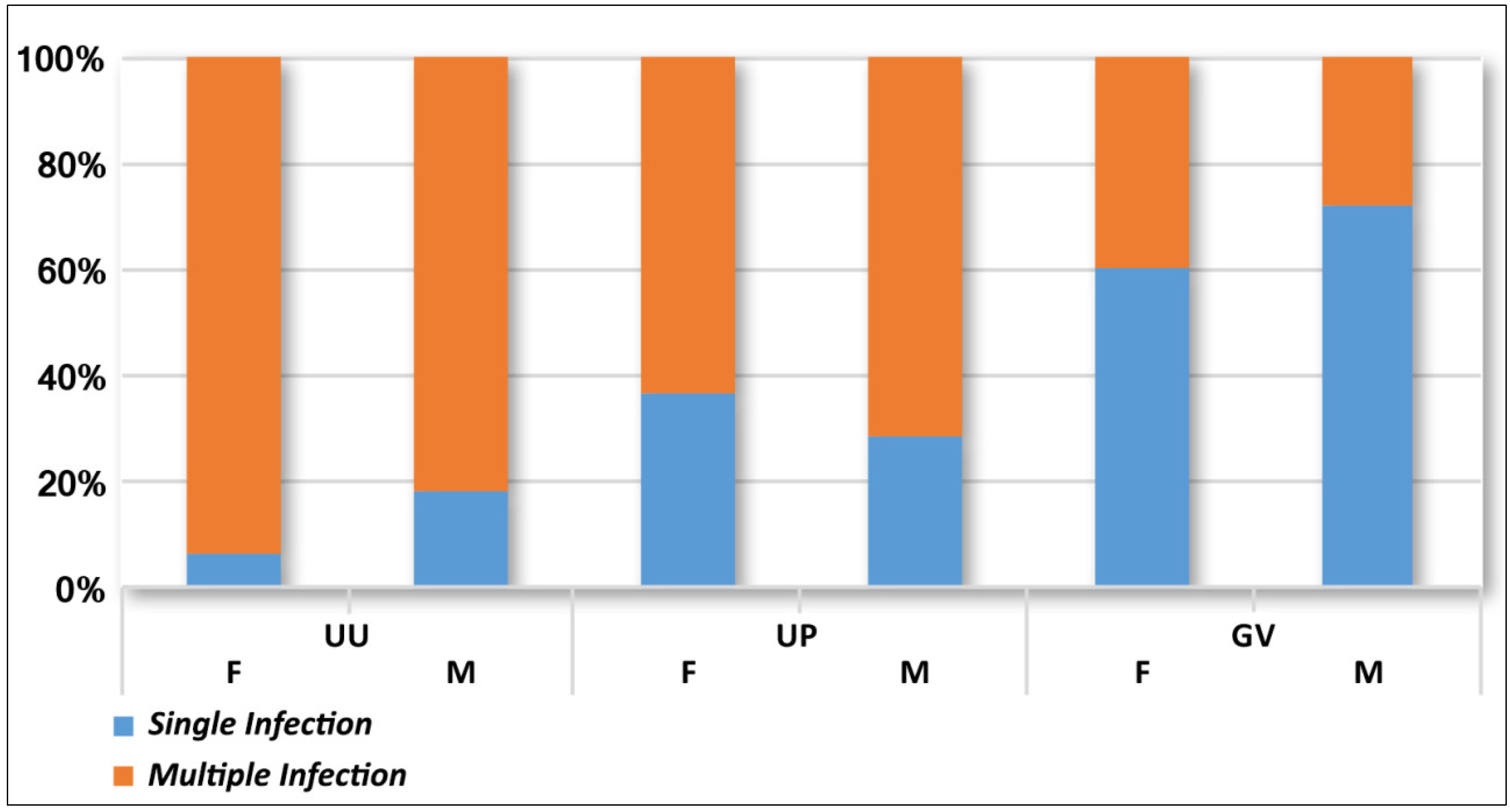
| U. urealyticum | 1 (0.27%) | 2 (0.56%) | n.a. |
| U. parvum | 27 (7.43%) | 8 (2.25%) | <0.001 |
| G. vaginalis | 96 (26.44%) | 70 (19.77%) | <0.05 |
| Multiple Infection | 66 (18.18%) | 29 (8.19%) | <0.001 |
| Positive | 190 (52.34%) | 112 (31.63%) | <0.001 |
| Negative | 173 (47.65%) | 242 (68.36%) | |
| Total samples | 363 (100%) | 354 (100%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scaglione, E.; Mantova, G.; Caturano, V.; Fanasca, L.; Carraturo, F.; Farina, F.; Pagliarulo, C.; Vitiello, M.; Pagliuca, C.; Salvatore, P.; et al. Molecular Epidemiology of Genital Infections in Campania Region: A Retrospective Study. Diagnostics 2022, 12, 1798. https://doi.org/10.3390/diagnostics12081798
Scaglione E, Mantova G, Caturano V, Fanasca L, Carraturo F, Farina F, Pagliarulo C, Vitiello M, Pagliuca C, Salvatore P, et al. Molecular Epidemiology of Genital Infections in Campania Region: A Retrospective Study. Diagnostics. 2022; 12(8):1798. https://doi.org/10.3390/diagnostics12081798
Chicago/Turabian StyleScaglione, Elena, Giuseppe Mantova, Valeria Caturano, Luca Fanasca, Francesca Carraturo, Fabrizio Farina, Caterina Pagliarulo, Mariateresa Vitiello, Chiara Pagliuca, Paola Salvatore, and et al. 2022. "Molecular Epidemiology of Genital Infections in Campania Region: A Retrospective Study" Diagnostics 12, no. 8: 1798. https://doi.org/10.3390/diagnostics12081798