
Comparison of Two RNA Extraction Methods for the Molecular Detection of SARS-CoV-2 from Nasopharyngeal Swab Samples


Abstract
:1. Introduction
2. Materials and Methods
2.1. Samples and RNA Extraction
2.2. Quantitative Real-Time PCR
2.3. Statistical Analysis
3. Results
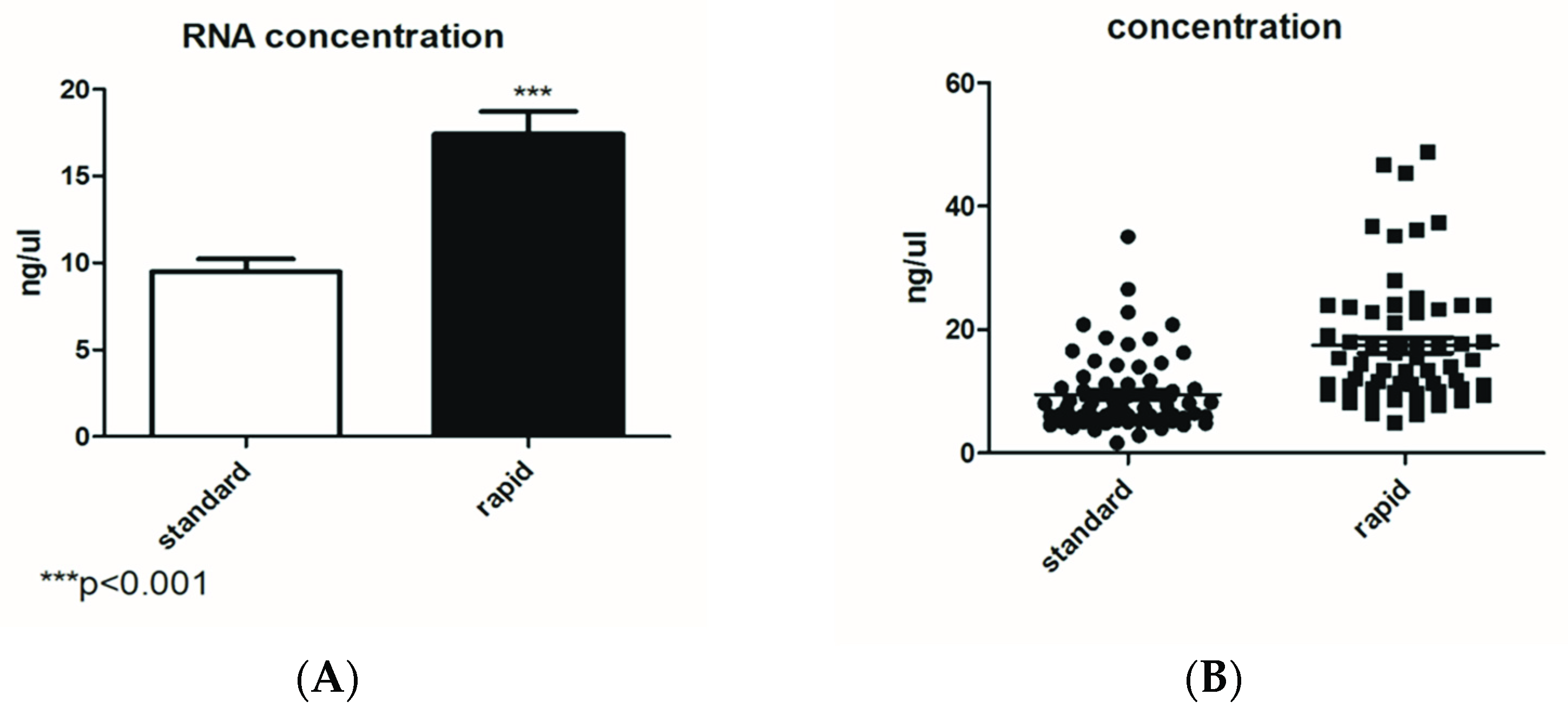
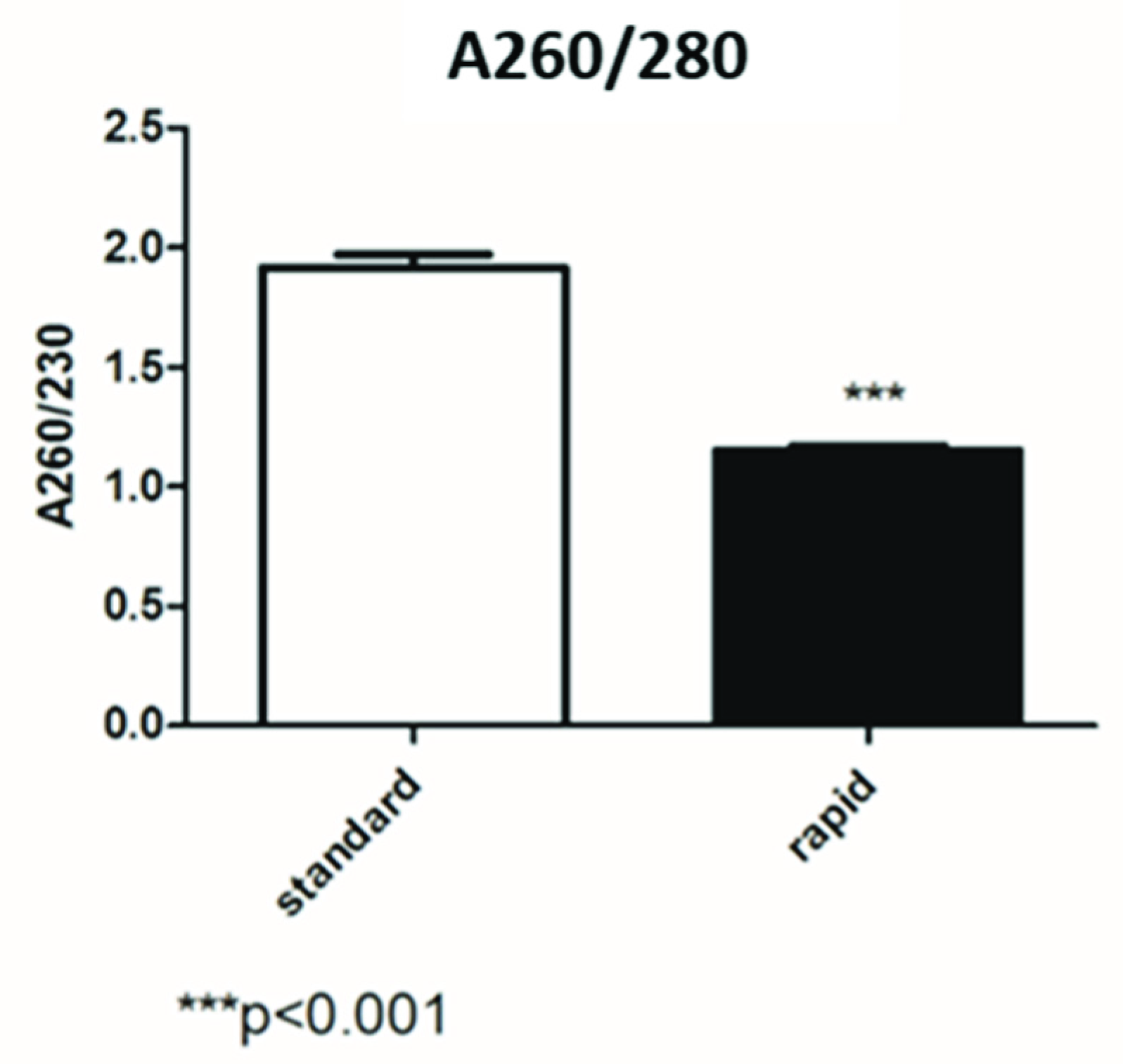
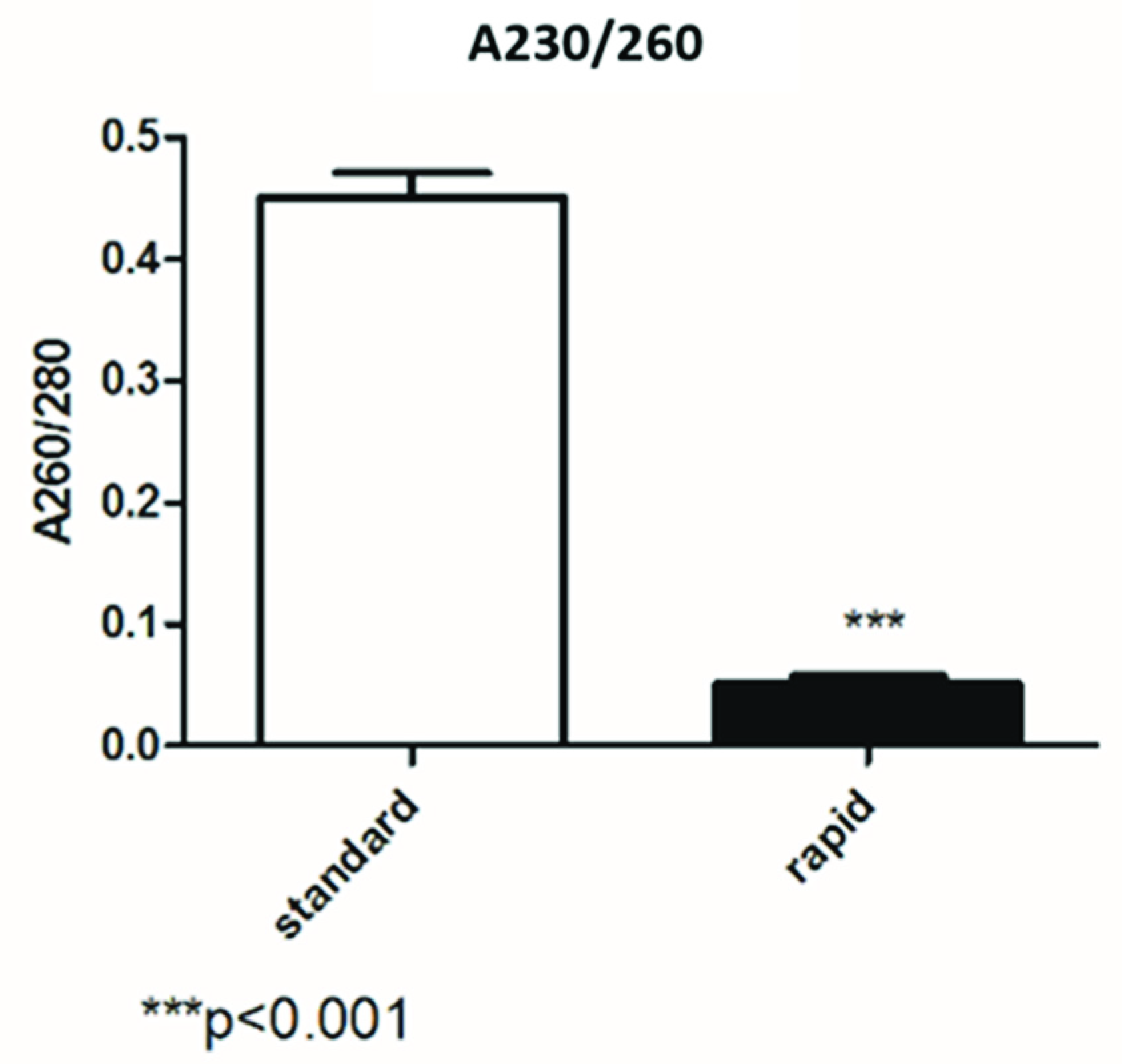
3.1. Comparison between Standard and Rapid Extraction by Nanodrop Analysis
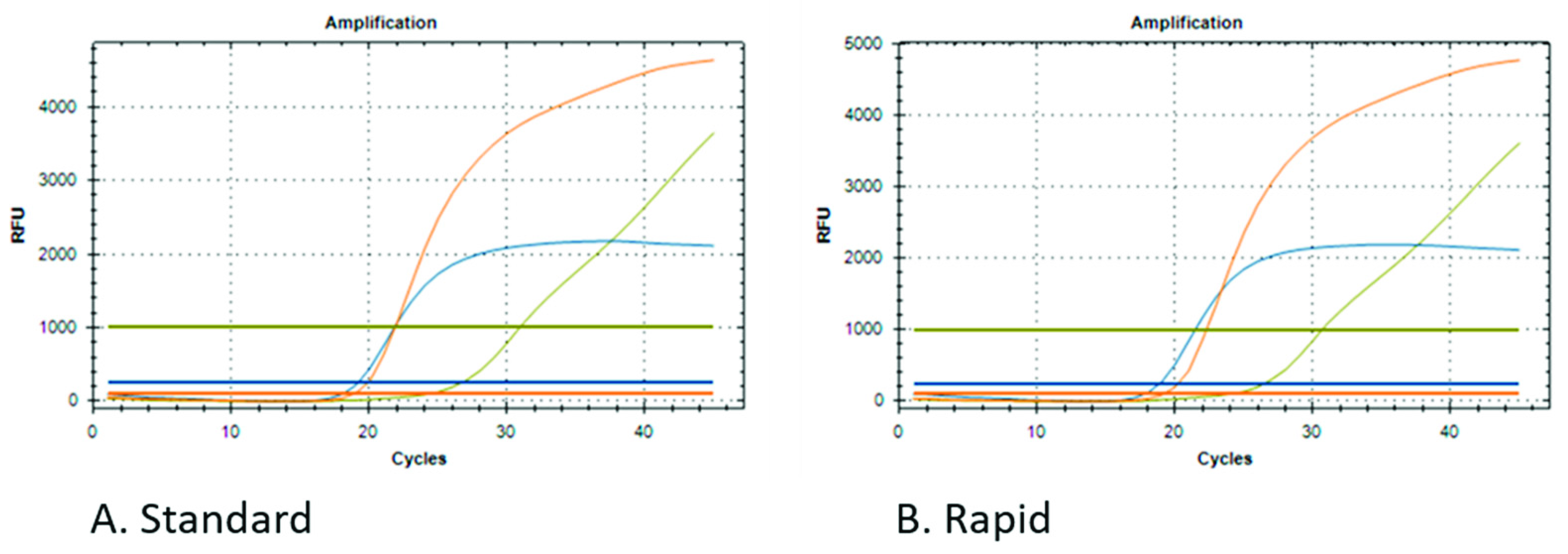
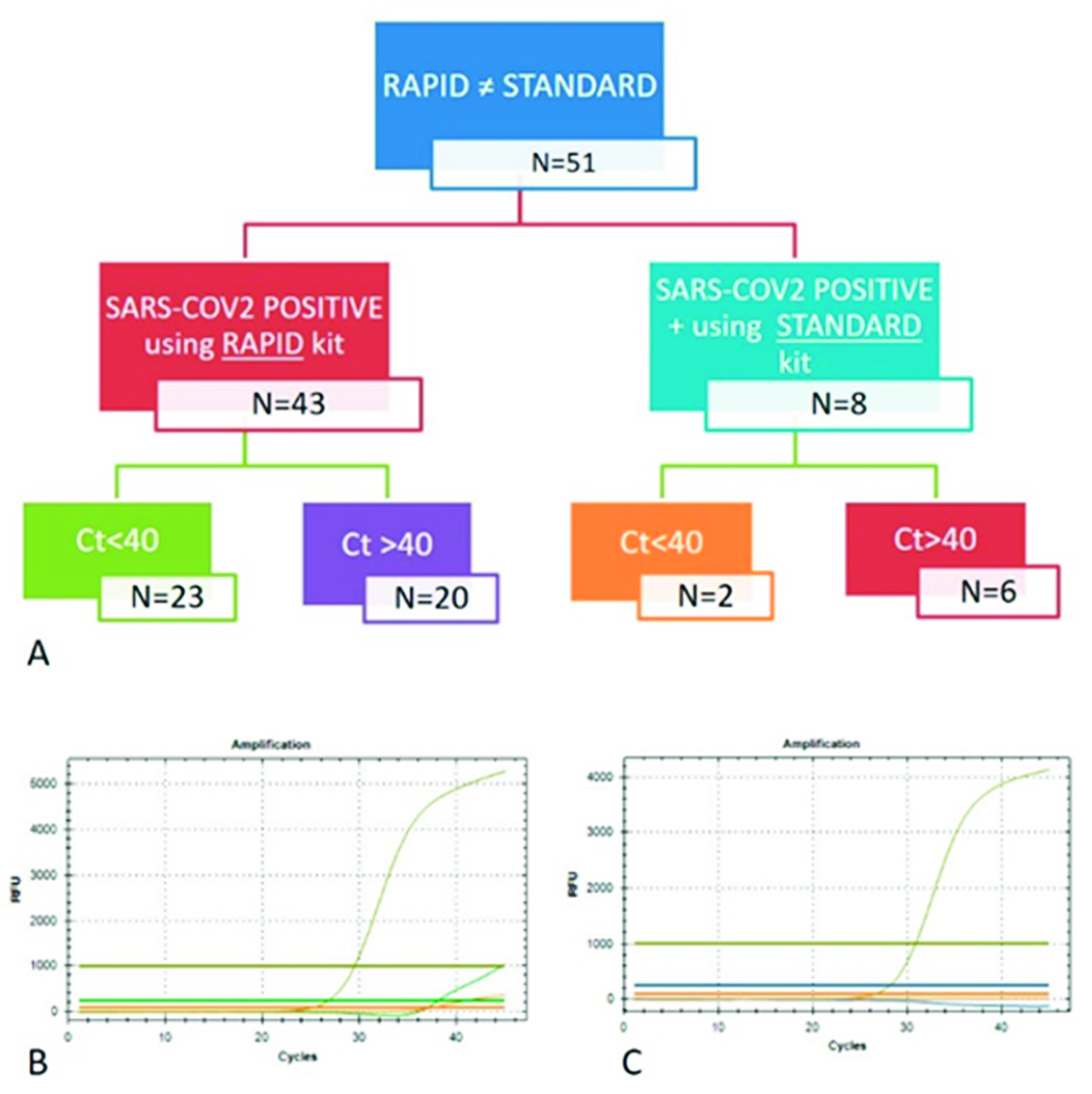
3.2. Comparison between qPCR Data from Different RNA Extraction Kits
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. China Novel Coronavirus Investigating and Research Team. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Cascella, M.; Rajnik, M.; Aleem, A.; Dulebohn, S.C.; Di Napoli, R. Features, evaluation and treatment coronavirus (COVID-19). In Statpearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Flower, T.G.; Buffalo, C.Z.; Hooy, R.M.; Allaire, M.; Ren, X.; Hurley, J.H. Structure of SARS-CoV-2 ORF8, a rapidly evolving immune evasion protein. Proc. Natl. Acad. Sci. USA 2021, 118, e2021785118. [Google Scholar] [CrossRef] [PubMed]
- Laurent-Rolle, M.; Morrison, J.; Rajsbaum, R.; Macleod, J.M.L.; Pisanelli, G.; Pham, A.; Ayllon, J.; Miorin, L.; Martinez, C.; tenOever, B.R.; et al. The interferon signaling antagonist function of yellow fever virus NS5 protein is activated by type I interferon. Cell Host Microbe 2014, 16, 314–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, Y.; Xin, L.; Shi, Y.; Zhang, T.H.; Wu, N.C.; Dai, L.; Gong, D.; Brar, G.; Shu, S.; Luo, J.; et al. Genome-wide identification of interferon-sensitive mutations enables influenza vaccine design. Science 2018, 359, 290–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, Y.; Schneider, T.; Leong, M.; Aravind, L.; Zhang, D. Novel Immunoglobulin Domain Proteins Provide Insights into Evolution and Pathogenesis of SARS-CoV-2-Related Viruses. DmBio 2020, 11, e00760-20. [Google Scholar] [CrossRef] [PubMed]
- Gordon, D.E.; Hiatt, J.; Bouhaddou, M.; Rezelj, V.V.; Ulferts, S.; Braberg, H.; Jureka, A.S.; Obernier, K.; Guo, J.Z.; Batra, J.; et al. Zoonomia Consortium, Comparative host-coronavirus protein interaction networks reveal pan-viral disease mechanisms. QCRG Struct. Biol. Consort. 2020, 370, eabe9403. [Google Scholar]
- Gong, Y.N.; Tsao, K.C.; Hsiao, M.J.; Huang, C.G.; Huang, P.N.; Huang, P.W.; Lee, K.M.; Liu, Y.C.; Yang, S.L.; Kuo, R.L.; et al. SARS-CoV-2 genomic surveillance in Taiwan revealed novel ORF8-deletion mutant and clade possibly associated with infections in Middle East. Emerg. Microbes Infect. 2020, 9, 1457–1466. [Google Scholar] [CrossRef] [PubMed]
- Zinzula, L. Lost in deletion: The enigmatic ORF8 protein of SARS-CoV-2. Biochem. Biophys. Res. Commun. 2021, 538, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Hachim, A.; Kavian, N.; Cohen, C.A.; Chin, A.W.; Chu, D.K.; Mok, C.K.; Tsang, O.T.; Yeung, Y.C.; Perera, R.A.; Poon, L.L.; et al. ORF8 and ORF3b antibodies are accurate serological markers of early and late SARS-CoV-2 infection. Nat. Immunol. 2020, 21, 1293–1301. [Google Scholar] [CrossRef] [PubMed]
- Naqvi, A.A.T.; Fatima, K.; Mohammad, T.; Fatima, U.; Singh, I.K.; Singh, A.; Atif, S.M.; Hariprasad, G.; Hasan, G.M.; Hassan, M.I. Insights into SARS-CoV-2 genome, structure, evolution, pathogenesis and therapies: Structural genomics approach. Biochim. Biophys. Acta Mol. Basis Dis. 2020, 1866, 165878. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chen, Y.; Li, Y.; Huang, F.; Luo, B.; Yuan, Y.; Xia, B.; Ma, X.; Yang, T.; Yu, F.; et al. The ORF8 protein of SARS-CoV-2 mediates immune evasion through potently downregulating MHC-I. Proc. Natl. Acad. Sci. USA 2021, 118, e2024202118. [Google Scholar] [CrossRef] [PubMed]
- Venkataraman, S.; Prasad, B.V.; Selvarajan, R. RNA Dependent RNA Polymerases: Insights from Structure, Function and Evolution. Viruses 2018, 10, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machitani, M.; Yasukawa, M.; Nakashima, J.; Furuichi, Y.; Masutomi, K. RNA-dependent RNA polymerase, RdRP, a promising therapeutic target for cancer and potentially COVID-19. Cancer Sci. 2020, 111, 3976–3984. [Google Scholar] [CrossRef] [PubMed]
- WHO: World Health Organization. Available online: https://www.who.int/publications/i/item/antigen-detection-in-the-diagnosis-of-sars-cov-2infection-using-rapid-immunoassays (accessed on 11 September 2020).
- Fleige, S.; Pfaffl, M.W. RNA integrity and the effect on the real-time qRT-PCR performance. Mol. Asp. Med. 2006, 27, 126–139. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, A.; Duyvejonck, H.; Van Belleghem, J.D.; Gryp, T.; Van Simaey, L.; Vermeulen, S.; Van Mechelen, E.; Vaneechoutte, M. Comparison of procedures for RNA-extraction from peripheral blood mononuclear cells. PLoS ONE 2020, 15, e0229423. [Google Scholar] [CrossRef] [Green Version]
- Komiazyk, M.; Walory, J.; Kozinska, A.; Wasko, I.; Baraniak, A. Impact of the Nucleic Acid Extraction Method and the RT-qPCR Assay on SARS-CoV-2 Detection in Low-Viral Samples. Diagnostics 2021, 11, 2247. [Google Scholar] [CrossRef]
- Ambrosi, C.; Prezioso, C.; Checconi, P.; Scribano, D.; Sarshar, M.; Capannari, M.; Tomino, C.; Fini, M.; Garaci, E.; Palamara, A.T.; et al. SARS-CoV-2: Comparative analysis of different RNA extraction methods. J. Virol. Methods 2021, 287, 114008. [Google Scholar] [CrossRef] [PubMed]
- Silva, L.M.; Riani, L.R.; Silvério, M.S.; Pereira-Júnior, O.D.S.; Pittella, F. Comparison of Rapid Nucleic Acid Extraction Methods for SARS-CoV-2 Detection by RT-qPCR. Diagnostics 2022, 12, 601. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time | ||||
|---|---|---|---|---|
| Standard | Fast | |||
| Step | Well | Name | ||
| 1 | 1 | lysis | 10:00:00 (mixing) | no |
| 2 | 6 | beads | 00:45 (mixing and magnet) | 00:15 (magnet) |
| 3 | 1 | binding | 10:35 (mixing and magnet) | 03:35 (mixing and magnet) |
| 4 | 2 | wash 1 | 02:30 (mixing and magnet) | 00:50 (mixing and magnet) |
| 5 | 3 | wash 2 | 01:30 (mixing and magnet) | 00:50 (mixing and magnet) |
| 6 | 4 | wash 3 | 01:30 (mixing and magnet) | no |
| 7 | 5 | elution | 07:35 (waiting, mixing and magnet) | 03:25 (waiting, mixing and magnet) |
| 8 | 6 | discard | 00:30 (mixing and magnet) | 00:00 |
| total time | 35 min | 9 min | ||
| Protocols | Standard | Rapid |
|---|---|---|
| Methods | Magnetic beads | Magnetic beads |
| Sample volume | 20–1000 μL | 10–300 μL |
| Elution volume | 80 μL | 70 μL |
| Processing time | 35 min | 9 min |
| Proteinase K | Yes | No |
| IC Ct | ||
|---|---|---|
| Kit | Average | Standard Deviation |
| Standard | 28.79 | 1.48 |
| Rapid | 28.5 | 1.53 |
| STANDARD | RAPID | ||
|---|---|---|---|
| POS | NEG | POS | NEG |
| 99 | 535 | 134 | 500 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scarabotto, A.; Balestro, S.; Gagliardi, S.; Trotti, R. Comparison of Two RNA Extraction Methods for the Molecular Detection of SARS-CoV-2 from Nasopharyngeal Swab Samples. Diagnostics 2022, 12, 1561. https://doi.org/10.3390/diagnostics12071561
Scarabotto A, Balestro S, Gagliardi S, Trotti R. Comparison of Two RNA Extraction Methods for the Molecular Detection of SARS-CoV-2 from Nasopharyngeal Swab Samples. Diagnostics. 2022; 12(7):1561. https://doi.org/10.3390/diagnostics12071561
Chicago/Turabian StyleScarabotto, Anna, Simona Balestro, Stella Gagliardi, and Rosa Trotti. 2022. "Comparison of Two RNA Extraction Methods for the Molecular Detection of SARS-CoV-2 from Nasopharyngeal Swab Samples" Diagnostics 12, no. 7: 1561. https://doi.org/10.3390/diagnostics12071561