
Chest CT Total Severity Score on Admission to Predict In-Hospital Mortality in COVID-19 Patients with Acute and Chronic Renal Impairment

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
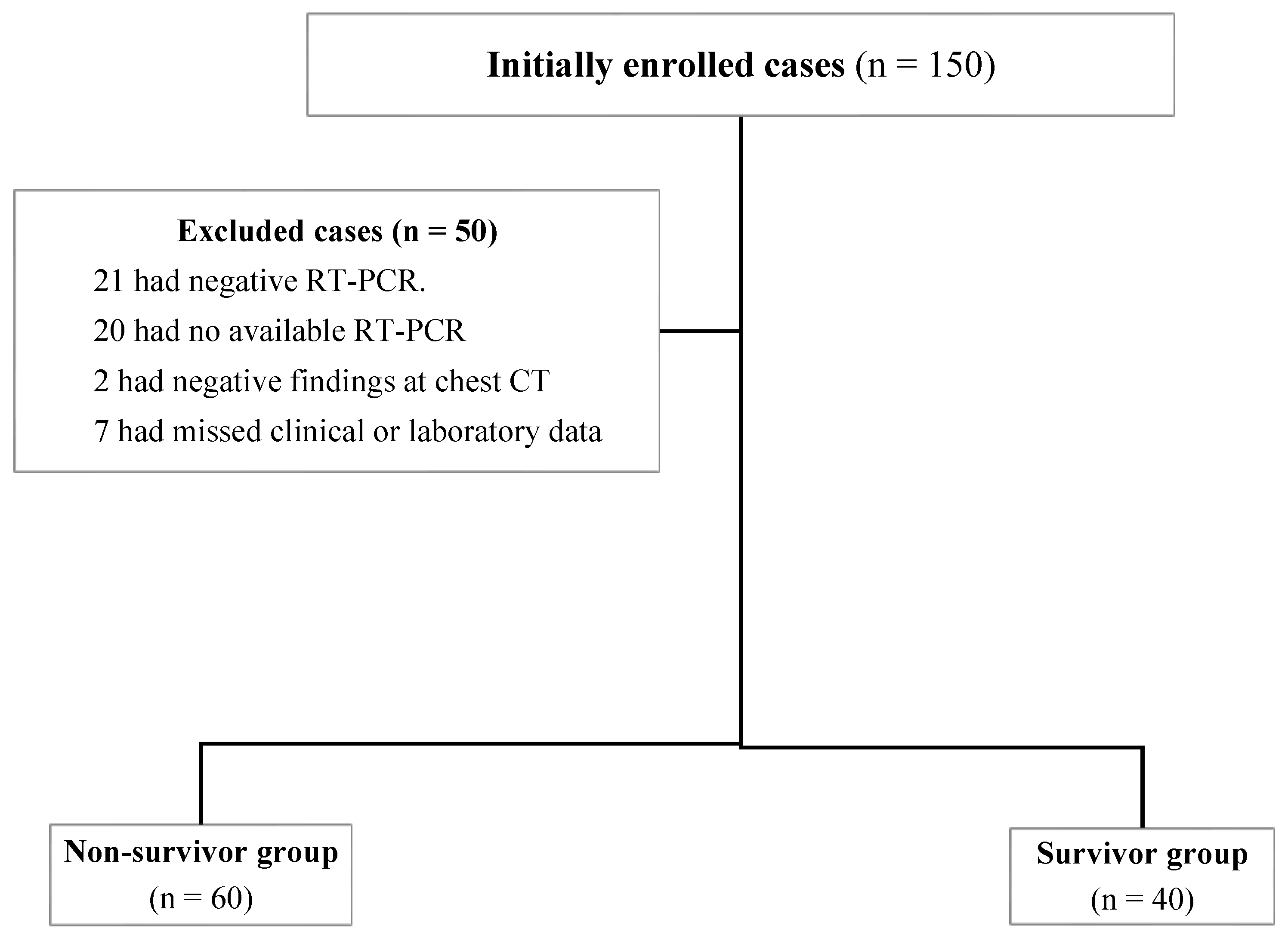
2.1. Patients
2.2. Clinical and Laboratory Data
2.3. Chest CT Acquisition
2.4. Qualitative CT Image Analysis
2.5. Quantitative CT Image Analysis
3. Statistical Analysis
4. Results
4.1. Demographic, Clinical and Laboratory Characteristics
4.2. CT Chest Features
4.3. Determinants of Mortality
4.4. TSS to Predict Mortality
4.5. Interobserver Agreement
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ARDS | acute respiratory distress syndrome |
| ARI | acute renal impairment |
| CBC | complete blood count |
| CKD | chronic kidney disease |
| COVID-19 | coronavirus disease of 2019 |
| Cr | creatinine |
| CRP | C-reactive protein |
| CT | computed tomography |
| ESR | erythrocyte sedimentation rate |
| GGOs | ground-glass opacities |
| ICU | intensive care unit |
| LDH | lactate dehydrogenase |
| LFTs | liver function tests |
| MV | mechanical ventilation |
| RT-PCR | Reverse transcription polymerase chain reaction assay |
| ROC | receiver operating characteristic |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2 |
| TSS | total severity score |
References
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization Declares Global Emergency: A Review of the 2019 Novel Coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Esposito, C.; Masieri, L.; Castagnetti, M.; Crocetto, F.; Escolino, M. Letter to the Editor: Robot-Assisted and Minimally Invasive Pediatric Surgery and Urology During the COVID-19 Pandemic: A Short Literature Review. J. Laparoendosc. Adv. Surg Tech. A 2020, 30, 915–918. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Vaira, L.A.; Hopkins, C.; Salzano, G.; Petrocelli, M.; Melis, A.; Cucurullo, M.; Ferrari, M.; Gagliardini, L.; Pipolo, C.; Deiana, G.; et al. Olfactory and Gustatory Function Impairment in COVID-19 Patients: Italian Objective Multicenter-Study. Head Neck 2020, 42, 1560–1569. [Google Scholar] [CrossRef]
- Chen, R.; Yu, Y.-L.; Li, W.; Liu, Y.; Lu, J.-X.; Chen, F.; Zhou, Q.; Xia, Z.-Y.; Gao, L.; Meng, Q.-T.; et al. Gastrointestinal Symptoms Associated with Unfavorable Prognosis of COVID-19 Patients: A Retrospective Study. Front. Med. 2020, 7, 608259. [Google Scholar] [CrossRef]
- Guarneri, C.; Venanzi Rullo, E.; Gallizzi, R.; Ceccarelli, M.; Cannavò, S.P.; Nunnari, G. Diversity of Clinical Appearance of Cutaneous Manifestations in the Course of COVID-19. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e449–e450. [Google Scholar] [CrossRef]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological Findings of COVID-19 Associated with Acute Respiratory Distress Syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Bertsimas, D.; Lukin, G.; Mingardi, L.; Nohadani, O.; Orfanoudaki, A.; Stellato, B.; Wiberg, H.; Gonzalez-Garcia, S.; Parra-Calderón, C.L.; Robinson, K.; et al. COVID-19 Mortality Risk Assessment: An International Multi-Center Study. PLoS ONE 2020, 15, e0243262. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical Course and Risk Factors for Mortality of Adult Inpatients with COVID-19 in Wuhan, China: A Retrospective Cohort Study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- COVID-19 Recommendations for Older Adults. Available online: https://www.cdc.gov/aging/covid19-guidance.html (accessed on 17 May 2022).
- Ferrer, R. COVID-19 Pandemic: The Greatest Challenge in the History of Critical Care. Med. Intensiva 2020, 44, 323–324. [Google Scholar] [CrossRef]
- Iacobucci, G. COVID-19: All Non-Urgent Elective Surgery Is Suspended for at Least Three Months in England. BMJ 2020, 368, m1106. [Google Scholar] [CrossRef]
- Lai, A.G.; Pasea, L.; Banerjee, A.; Hall, G.; Denaxas, S.; Chang, W.H.; Katsoulis, M.; Williams, B.; Pillay, D.; Noursadeghi, M.; et al. Estimated Impact of the COVID-19 Pandemic on Cancer Services and Excess 1-Year Mortality in People with Cancer and Multimorbidity: Near Real-Time Data on Cancer Care, Cancer Deaths and a Population-Based Cohort Study. BMJ Open 2020, 10, e043828. [Google Scholar] [CrossRef]
- Di Lorenzo, G.; Buonerba, L.; Ingenito, C.; Crocetto, F.; Buonerba, C.; Libroia, A.; Sciarra, A.; Ragone, G.; Sanseverino, R.; Iaccarino, S.; et al. Clinical Characteristics of Metastatic Prostate Cancer Patients Infected with COVID-19 in South Italy. Oncology 2020, 98, 743–747. [Google Scholar] [CrossRef]
- CKD is a Key Risk Factor for COVID-19 Mortality. Nature Reviews Nephrology. Available online: https://www.nature.com/articles/s41581-020-00349-4 (accessed on 17 May 2022).
- Ajaimy, M.; Melamed, M.L. COVID-19 in Patients with Kidney Disease. CJASN 2020, 15, 1087–1089. [Google Scholar] [CrossRef]
- Naicker, S.; Yang, C.-W.; Hwang, S.-J.; Liu, B.-C.; Chen, J.-H.; Jha, V. The Novel Coronavirus 2019 Epidemic and Kidneys. Kidney Int. 2020, 97, 824–828. [Google Scholar] [CrossRef]
- Koo, H.J.; Lim, S.; Choe, J.; Choi, S.-H.; Sung, H.; Do, K.-H. Radiographic and CT Features of Viral Pneumonia. Radiographics 2018, 38, 719–739. [Google Scholar] [CrossRef]
- Pan, Y.; Guan, H. Imaging Changes in Patients with 2019-NCov. Eur. Radiol. 2020, 30, 3612–3613. [Google Scholar] [CrossRef]
- Lei, J.; Li, J.; Li, X.; Qi, X. CT Imaging of the 2019 Novel Coronavirus (2019-NCoV)—Pneumonia. Radiology 2020, 295, 18. [Google Scholar] [CrossRef]
- Elmokadem, A.H.; Mounir, A.M.; Ramadan, Z.A.; Elsedeiq, M.; Saleh, G.A. Comparison of Chest CT Severity Scoring Systems for COVID-19. Eur. Radiol. 2022, 32, 3501–3512. [Google Scholar] [CrossRef]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 Novel Coronavirus (2019-NCoV) by Real-Time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef]
- Hansell, D.M.; Bankier, A.A.; MacMahon, H.; McLoud, T.C.; Müller, N.L.; Remy, J. Fleischner Society: Glossary of Terms for Thoracic Imaging. Radiology 2008, 246, 697–722. [Google Scholar] [CrossRef]
- Li, K.; Fang, Y.; Li, W.; Pan, C.; Qin, P.; Zhong, Y.; Liu, X.; Huang, M.; Liao, Y.; Li, S. CT Image Visual Quantitative Evaluation and Clinical Classification of Coronavirus Disease (COVID-19). Eur. Radiol. 2020, 30, 4407–4416. [Google Scholar] [CrossRef]
- Gasparini, M.; Khan, S.; Patel, J.M.; Parekh, D.; Bangash, M.N.; Stϋmpfle, R.; Shah, A.; Baharlo, B.; Soni, S. Collaborators Renal Impairment and Its Impact on Clinical Outcomes in Patients Who Are Critically Ill with COVID-19: A Multicentre Observational Study. Anaesthesia 2021, 76, 320–326. [Google Scholar] [CrossRef]
- Chu, K.H.; Tsang, W.K.; Tang, C.S.; Lam, M.F.; Lai, F.M.; To, K.F.; Fung, K.S.; Tang, H.L.; Yan, W.W.; Chan, H.W.H.; et al. Acute Renal Impairment in Coronavirus-Associated Severe Acute Respiratory Syndrome. Kidney Int. 2005, 67, 698–705. [Google Scholar] [CrossRef]
- Holman, N.; Knighton, P.; Kar, P.; O’Keefe, J.; Curley, M.; Weaver, A.; Barron, E.; Bakhai, C.; Khunti, K.; Wareham, N.J.; et al. Risk Factors for COVID-19-Related Mortality in People with Type 1 and Type 2 Diabetes in England: A Population-Based Cohort Study. Lancet Diabetes Endocrinol. 2020, 8, 823–833. [Google Scholar] [CrossRef]
- Zahid, U.; Ramachandran, P.; Spitalewitz, S.; Alasadi, L.; Chakraborti, A.; Azhar, M.; Mikhalina, G.; Sherazi, A.; Narh, J.T.; Khattar, P.; et al. Acute Kidney Injury in COVID-19 Patients: An Inner City Hospital Experience and Policy Implications. Am. J. Nephrol. 2020, 51, 786–796. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Garcia-Tsao, G.; Biggins, S.W.; Kamath, P.S.; Wong, F.; McGeorge, S.; Shaw, J.; Pearson, M.; Chew, M.; Fagan, A.; et al. Comparison of Mortality Risk in Patients with Cirrhosis and COVID-19 Compared with Patients with Cirrhosis Alone and COVID-19 Alone: Multicentre Matched Cohort. Gut 2021, 70, 531–536. [Google Scholar] [CrossRef]
- Qi, X.; Liu, Y.; Wang, J.; Fallowfield, J.A.; Wang, J.; Li, X.; Shi, J.; Pan, H.; Zou, S.; Zhang, H.; et al. Clinical Course and Risk Factors for Mortality of COVID-19 Patients with Pre-Existing Cirrhosis: A Multicentre Cohort Study. Gut 2021, 70, 433–436. [Google Scholar] [CrossRef]
- Moon, A.M.; Webb, G.J.; Aloman, C.; Armstrong, M.J.; Cargill, T.; Dhanasekaran, R.; Genescà, J.; Gill, U.S.; James, T.W.; Jones, P.D.; et al. High Mortality Rates for SARS-CoV-2 Infection in Patients with Pre-Existing Chronic Liver Disease and Cirrhosis: Preliminary Results from an International Registry. J. Hepatol. 2020, 73, 705–708. [Google Scholar] [CrossRef]
- Boregowda, U.; Aloysius, M.M.; Perisetti, A.; Gajendran, M.; Bansal, P.; Goyal, H. Serum Activity of Liver Enzymes Is Associated with Higher Mortality in COVID-19: A Systematic Review and Meta-Analysis. Front. Med. 2020, 7, 431. [Google Scholar] [CrossRef]
- Kishaba, T.; Tamaki, H.; Shimaoka, Y.; Fukuyama, H.; Yamashiro, S. Staging of Acute Exacerbation in Patients with Idiopathic Pulmonary Fibrosis. Lung 2014, 192, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Bartziokas, K.; Kostikas, K. Lactate Dehydrogenase, COVID-19 and Mortality. Med. Clin. 2021, 156, 37. [Google Scholar] [CrossRef] [PubMed]
- Rubin, G.D.; Ryerson, C.J.; Haramati, L.B.; Sverzellati, N.; Kanne, J.P.; Raoof, S.; Schluger, N.W.; Volpi, A.; Yim, J.-J.; Martin, I.B.K.; et al. The Role of Chest Imaging in Patient Management during the COVID-19 Pandemic: A Multinational Consensus Statement from the Fleischner Society. Radiology 2020, 296, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Ding, X.; Xu, J.; Zhou, J.; Long, Q. Chest CT Findings of COVID-19 Pneumonia by Duration of Symptoms. Eur. J. Radiol. 2020, 127, 109009. [Google Scholar] [CrossRef]
- Salehi, S.; Abedi, A.; Balakrishnan, S.; Gholamrezanezhad, A. Coronavirus Disease 2019 (COVID-19): A Systematic Review of Imaging Findings in 919 Patients. Am. J. Roentgenol. 2020, 215, 87–93. [Google Scholar] [CrossRef]
- Pan, F.; Ye, T.; Sun, P.; Gui, S.; Liang, B.; Li, L.; Zheng, D.; Wang, J.; Hesketh, R.L.; Yang, L.; et al. Time Course of Lung Changes at Chest CT during Recovery from Coronavirus Disease 2019 (COVID-19). Radiology 2020, 295, 715–721. [Google Scholar] [CrossRef]
- Fang, Y.; Zhang, H.; Xie, J.; Lin, M.; Ying, L.; Pang, P.; Ji, W. Sensitivity of Chest CT for COVID-19: Comparison to RT-PCR. Radiology 2020, 296, E115–E117. [Google Scholar] [CrossRef]
- Bai, H.X.; Hsieh, B.; Xiong, Z.; Halsey, K.; Choi, J.W.; Tran, T.M.L.; Pan, I.; Shi, L.-B.; Wang, D.-C.; Mei, J.; et al. Performance of Radiologists in Differentiating COVID-19 from Non-COVID-19 Viral Pneumonia at Chest CT. Radiology 2020, 296, E46–E54. [Google Scholar] [CrossRef]
- Li, K.; Wu, J.; Wu, F.; Guo, D.; Chen, L.; Fang, Z.; Li, C. The Clinical and Chest CT Features Associated with Severe and Critical COVID-19 Pneumonia. Invest. Radiol. 2020, 55, 327–331. [Google Scholar] [CrossRef]
- Tian, S.; Xiong, Y.; Liu, H.; Niu, L.; Guo, J.; Liao, M.; Xiao, S.-Y. Pathological Study of the 2019 Novel Coronavirus Disease (COVID-19) through Postmortem Core Biopsies. Mod. Pathol. 2020, 33, 1007–1014. [Google Scholar] [CrossRef]
- Colombi, D.; Villani, G.D.; Maffi, G.; Risoli, C.; Bodini, F.C.; Petrini, M.; Morelli, N.; Anselmi, P.; Milanese, G.; Silva, M.; et al. Qualitative and Quantitative Chest CT Parameters as Predictors of Specific Mortality in COVID-19 Patients. Emerg. Radiol. 2020, 27, 701–710. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable Mean ± SD, n (%), Median (Min-Max) |
Total (n = 100) |
Non-Survivor Group (n = 60) |
Survivor Group (n = 40) | P |
|---|---|---|---|---|
| Demographic data | ||||
| Age (years) | 60±15 | 62.38±12.64 | 58.68±17.92 | 0.261 |
| Gender | 0.060 | |||
| Male | 54 | 37 (61.7) | 17 (42.5) | |
| Female | 46 | 23 (38.3) | 23 (57.5) | |
| Type of renal impairment | 0.033 | |||
| Acute | 53 | 37 (61.7) | 16 (40) | |
| Chronic | 47 | 23 (38.3) | 24 (60) | |
| Associated comorbidities | ||||
| Diabetes Miletus | 16 | 10 (16.7) | 6 (15) | 0.824 |
| Hypertension | 23 | 13 (21.7) | 10 (25) | 0.698 |
| Ischemic heart disease | 6 | 2 (3.3) | 4 (10) | 0.214 |
| liver cirrhosis | 10 | 9 (15) | 1 (2.5) | 0.047 |
| Stroke | 2 | 2 (3.3) | 0 | 0.515 |
| Atrial fibrillation | 2 | 2 (3.3) | 0 | 0.515 |
| Systemic lupus erythematosus | 2 | 2 (3.3) | 0 | 0.515 |
| Chronic anemia | 16 | 9 (15) | 7 (17.5) | 0.738 |
| Bronchial asthma | 1 | 0 | 1 (2.5) | 0.400 |
| Clinical presentation of COVID-19 infection | ||||
| Fever | 75 | 41 (68.3) | 34 (85) | 0.059 |
| Dyspnea | 86 | 51 (85) | 35 (87.5) | 0.724 |
| Cough | 65 | 39 (65) | 26 (65) | 1 |
| Vomiting | 1 | 0 | 1 (2.5) | 0.400 |
| Acute confusional state | 6 | 5 (8.3) | 1 (2.5) | 0.397 |
| Vital data | ||||
| Temperature (°C) | 38.34 ± 0.93 | 38.56 ± 0.93 | 38.01 ± 0.83 | 0.003 |
| Systolic blood pressure (mmHg) | 128.83 ± 26.42 | 123.67 ± 27.37 | 136.57 ± 23.15 | 0.016 |
| Diastolic blood pressure (mmHg) | 79.08 ± 13.67 | 76.23 ± 14.01 | 83.36 ± 12.07 | 0.010 |
| Respiratory rate (/min) | 29 (14–50) | 30 (14–50) | 25.66 (15–34) | 0.000 |
| Laboratory findings | ||||
| White blood cells (× 109/L) | 9.45 (2.10–34.60) | 9.65 (2.10–34.60) | 9.35 (4.20–24.26) | 0.992 |
| Neutrophils (× 109/L) | 8 (1.38–31) | 8.76 (1.38–31) | 7.05 (2.2–20) | 0.595 |
| Lymphocytes (× 109/L) | 0.99 (0.2–5) | 0.91 (0.2–2.7) | 1.2 (0.4–5) | 0.067 |
| Platelets (× 109/L) | 182 (26–617) | 165 (26–617) | 235 (45–491) | 0.014 |
| Creatinine (mg/dL) | 5.19 (2–21.76) | 5.09 (2–21.76) | 6 (2–21.07) | 0.964 |
| eGFR (mL/min/1.73 m2) | 10.2 (1.79–43.37) | 10.81 (1.79–43.37) | 8.79 (1.87–28.45) | 0.744 |
| ALT (U/L) | 26.5 (9–1004) | 35.5 (11–1004) | 22 (9–447) | 0.030 |
| AST (U/L) | 37 (11–1897) | 49 (15–1897) | 27 (11–512) | 0.007 |
| Bilirubin (mg/dL) | 0.7 (0.17–6.17) | 0.8 (0.32–6.17) | 0.56 (0.17–3) | 0.012 |
| Albumin (g/dL) | 3.14 (1.80–4.47) | 3 (1.8–4.2) | 3.3 (1.9–4.47) | 0.010 |
| LDH (U/L) | 632 (101.01–2636) | 744 (150–2300) | 440 (101–2636) | 0.001 |
| ESR (mm/hr) | 60.26 (2–138) | 59.5 (2–138) | 62.29 (18–125) | 0.984 |
| D dimer (ng/mL) | 709.03 (102.59–2237.94) | 849.11 (135.11–2237.94) | 594.45 (102.59–2194.59) | 0.082 |
| CRP (mg/L) | 96 (3–366) | 96.43 (12–366) | 54.15 (3–234) | 0.003 |
| Arterial blood gases | ||||
| PH | 7.31 ± 0.099 | 7.31 ± 0.101 | 7.31 ± 0.09 | 0.76 |
| PCO2 (mmHg) | 33.01 ± 11.84 | 33.06 ± 11.97 | 32.94 ± 11.84 | 0.864 |
| HCO3 (mEq/L) | 19.4 (8.40–37.20) | 19.9 (8.4–28.6) | 18.95 (11.7–37.2) | 0.861 |
| Sodium (mEq/L) | 133.95 ± 12.61 | 131.23 ± 10.30 | 135.77 ± 13.71 | 0.077 |
| Potassium (mmol/L) | 4.22 ± 1.09 | 4.21 ± 1.08 | 4.25 ± 1.12 | 0.853 |
| SO2 (%) | 91 (60–98) | 88 (60–97) | 94 (75–98) | 0.001 |
| Hospitalization | 94 | 58 (96.7) | 36 (90) | 0.169 |
| Total duration of hospital stay (days) | 6 (1–19) | 6.5 (1–17) | 6 (2–19) | 0.628 |
| ICU admission | 83 | 57 (95) | 26 (65) | 0.000 |
| Need for dialysis | 49 | 27 (45) | 22 (55) | 0.327 |
| Need for O2 supply | 90 | 57 (95) | 33 (82.5) | 0.005 |
| Invasive mechanical ventilation | 26 | 23 (38.3) | 3 (7.5) | <0.001 |
| Variable n (%), Median (Min-Max) | Total (n = 100) n | Non-Survivor Group (n = 60) n (%) | Survivor Group (n = 40) n (%) | P |
|---|---|---|---|---|
| CT chest findings | ||||
| Ground-glass opacities | 100 | 60 (100) | 40 (100) | - |
| Consolidation | 71 | 54 (90) | 17 (42.5) | <0.001 |
| Crazy paving pattern | 17 | 17 (28.3) | 0 | <0.001 |
| Pleural effusion | 49 | 34 (56.7) | 15 (37.5) | 0.060 |
| Pulmonary nodules | 7 | 6 (10) | 1 (2.5) | 0.238 |
| Bronchial dilatation | 1 | 1 (1.7) | 0 | 1 |
| Mediastinal lymphadenopathy | 3 | 1 (1.7) | 2 (5) | 0.562 |
| Pericardial effusion | 4 | 2 (3.3) | 2 (5) | 1 |
| Predominant pattern | ||||
| Ground-glass opacities | 64 | 26 (43.3) | 38 (95) | <0.001 |
| Consolidation | 34 | 32 (53.3) | 2 (5) | |
| Crazy paving pattern | 2 | 2 (3.3) | 0 | |
| Laterality | ||||
| Unilateral | 2 | 0 | 2 (5) | 0.158 |
| Bilateral | 98 | 60 (100) | 38 (95) | |
| CT chest total severity score | 10 (3–19) | 12 (6–19) | 6 (3–14) | <0.001 |
| Variable | OR | 95% CI | P |
|---|---|---|---|
| Demographic data | |||
| Age | 1.017 | (0.990–1.044) | 0.227 |
| Gender | |||
| Female | Ref | ||
| Male | 2.176 | 0.964–4.916 | 0.061 |
| Clinical data | |||
| Systolic blood pressure | 0.981 | 0.965–0.997 | 0.019 |
| Respiratory rate | 1.149 | 1.057–1.248 | 0.001 |
| Laboratory finding | |||
| Bilirubin | 2.532 | 1.099–5.836 | 0.029 |
| LDH | 1.001 | 1.000–1.003 | 0.018 |
| CRP | 1.010 | 1.002–1.017 | 0.012 |
| ICU admission | 0.033 | 0.004–0.261 | 0.001 |
| Need for O2 supply | 0.083 | 0.010–0.702 | 0.022 |
| Simple face mask | 0.474 | 0.100–2.241 | 0.346 |
| Reservoir mask | 1.588 | 0.454–5.558 | 0.469 |
| Noninvasive ventilation | 7.800 | 0.957–63.55 | 0.055 |
| Invasive mechanical ventilation | 7.667 | 2.118–27.755 | 0.002 |
| CT chest findings | |||
| Consolidation | 0.082 | 0.029–0.235 | <0.001 |
| Pleural effusion | 2.179 | 0.961–4.943 | 0.062 |
| Pulmonary nodules | 4.333 | 0.501–37.451 | 0.183 |
| Mediastinal lymphadenopathy | 0.322 | 0.028–3.676 | 0.362 |
| Pericardial effusion | 0.655 | 0.088–4.852 | 0.679 |
| CT chest total severity score | 2.082 | 1.579–2.745 | <0.001 |
| Independent Variable | Exp(B) | P |
|---|---|---|
| Constant | 0.000 | 0.012 |
| SBP | 0.977 | 0.244 |
| RR | 1.085 | 0.327 |
| Bilirubin | 1.894 | 0.336 |
| LDH | 0.999 | 0.400 |
| CRP | 1.020 | 0.046 |
| ICU | 34.484 | 0.040 |
| TSS | 2.485 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tharwat, S.; Saleh, G.A.; Saleh, M.; Mounir, A.M.; Abdelzaher, D.G.; Salah, A.M.; Nassar, M.K. Chest CT Total Severity Score on Admission to Predict In-Hospital Mortality in COVID-19 Patients with Acute and Chronic Renal Impairment. Diagnostics 2022, 12, 1529. https://doi.org/10.3390/diagnostics12071529
Tharwat S, Saleh GA, Saleh M, Mounir AM, Abdelzaher DG, Salah AM, Nassar MK. Chest CT Total Severity Score on Admission to Predict In-Hospital Mortality in COVID-19 Patients with Acute and Chronic Renal Impairment. Diagnostics. 2022; 12(7):1529. https://doi.org/10.3390/diagnostics12071529
Chicago/Turabian StyleTharwat, Samar, Gehad A. Saleh, Marwa Saleh, Ahmad M. Mounir, Dina G. Abdelzaher, Ahmed M Salah, and Mohammed Kamal Nassar. 2022. "Chest CT Total Severity Score on Admission to Predict In-Hospital Mortality in COVID-19 Patients with Acute and Chronic Renal Impairment" Diagnostics 12, no. 7: 1529. https://doi.org/10.3390/diagnostics12071529