
Predictors for COVID-19 Complete Remission with HRCT Pattern Evolution: A Monocentric, Prospective Study

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. Study Variables and Scores
2.3. Ethics
2.4. Statistical Analysis
3. Results
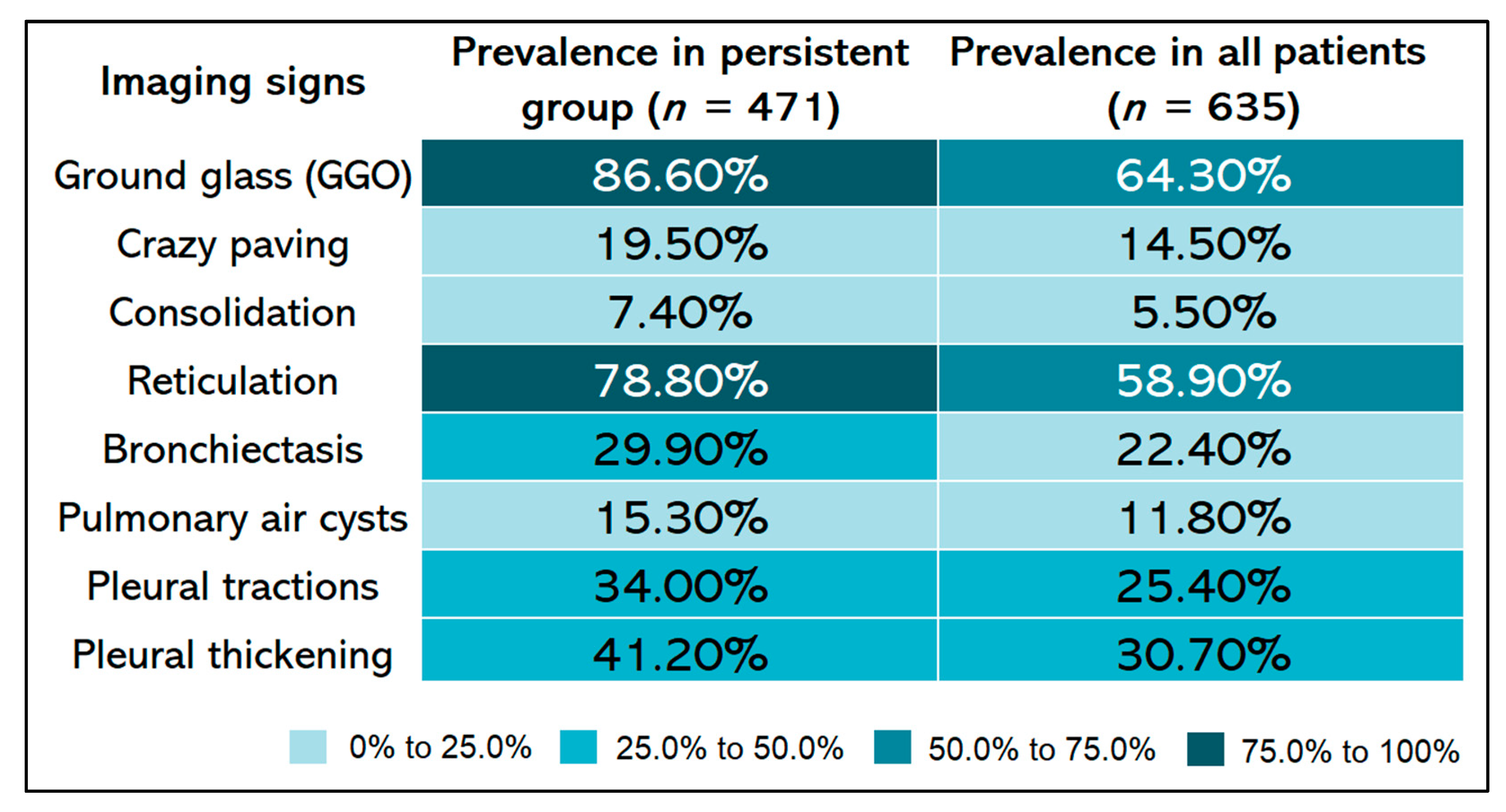
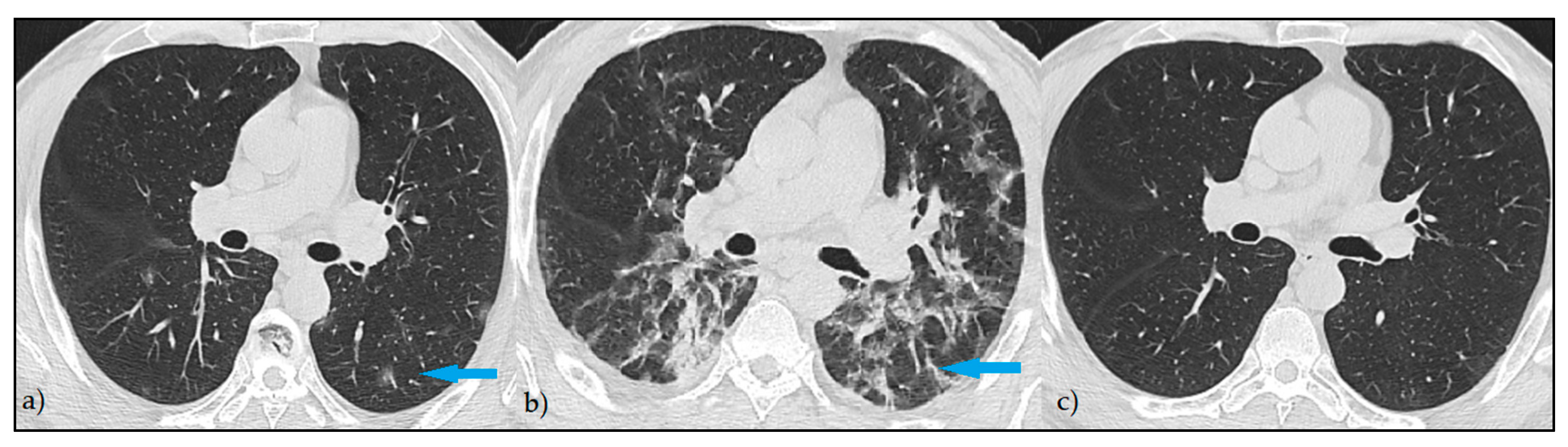
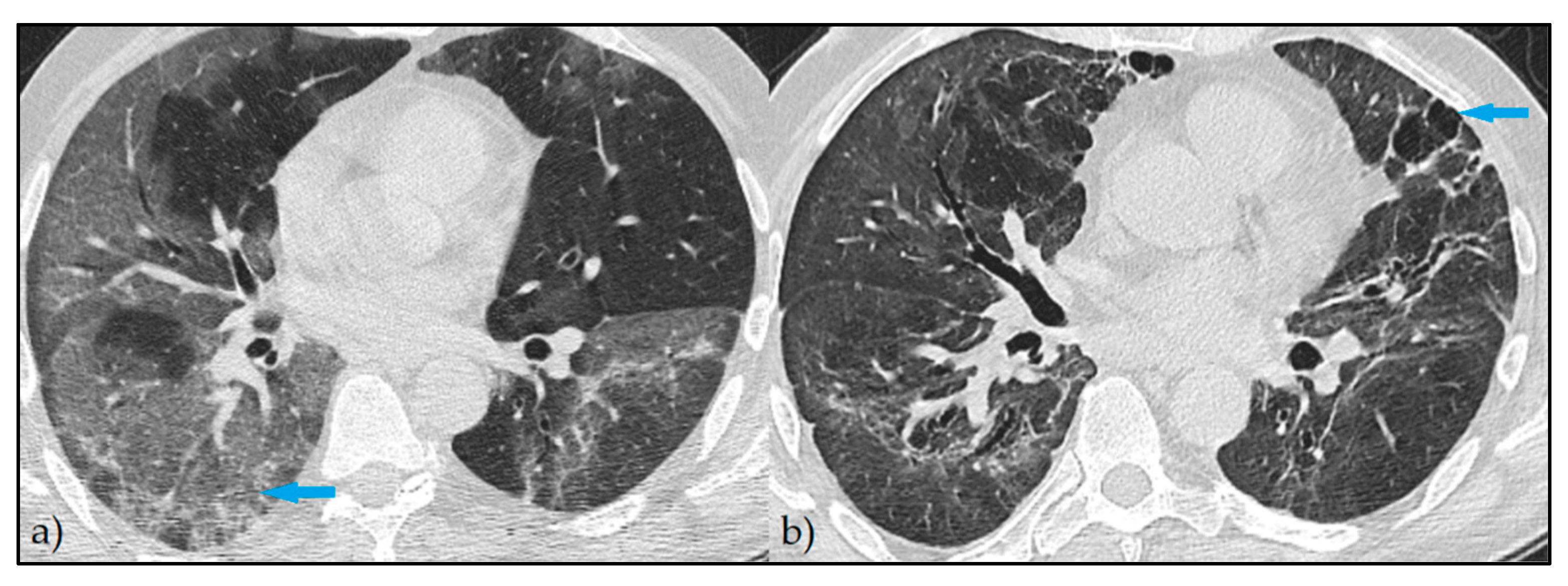
3.1. Imaging Studies
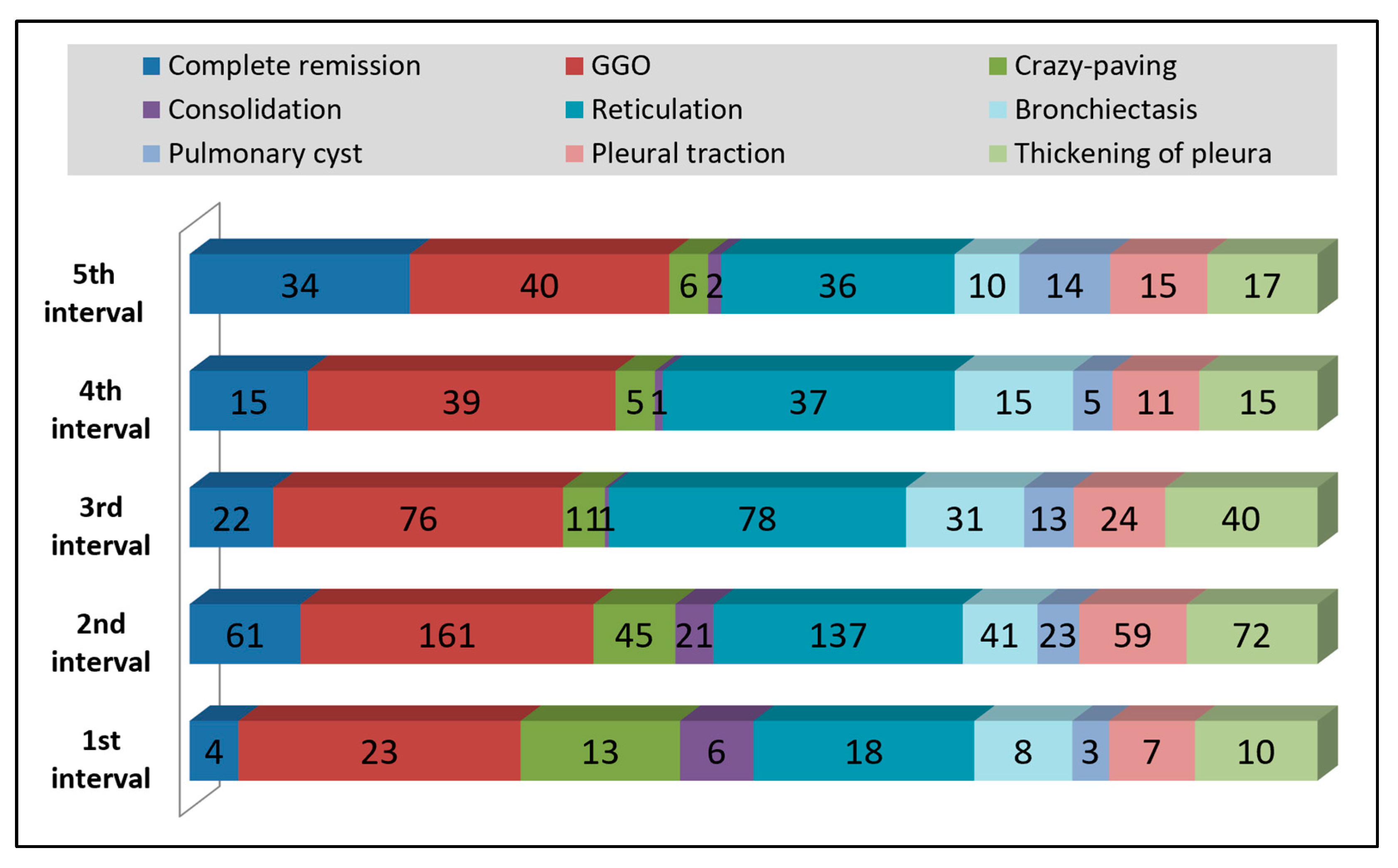
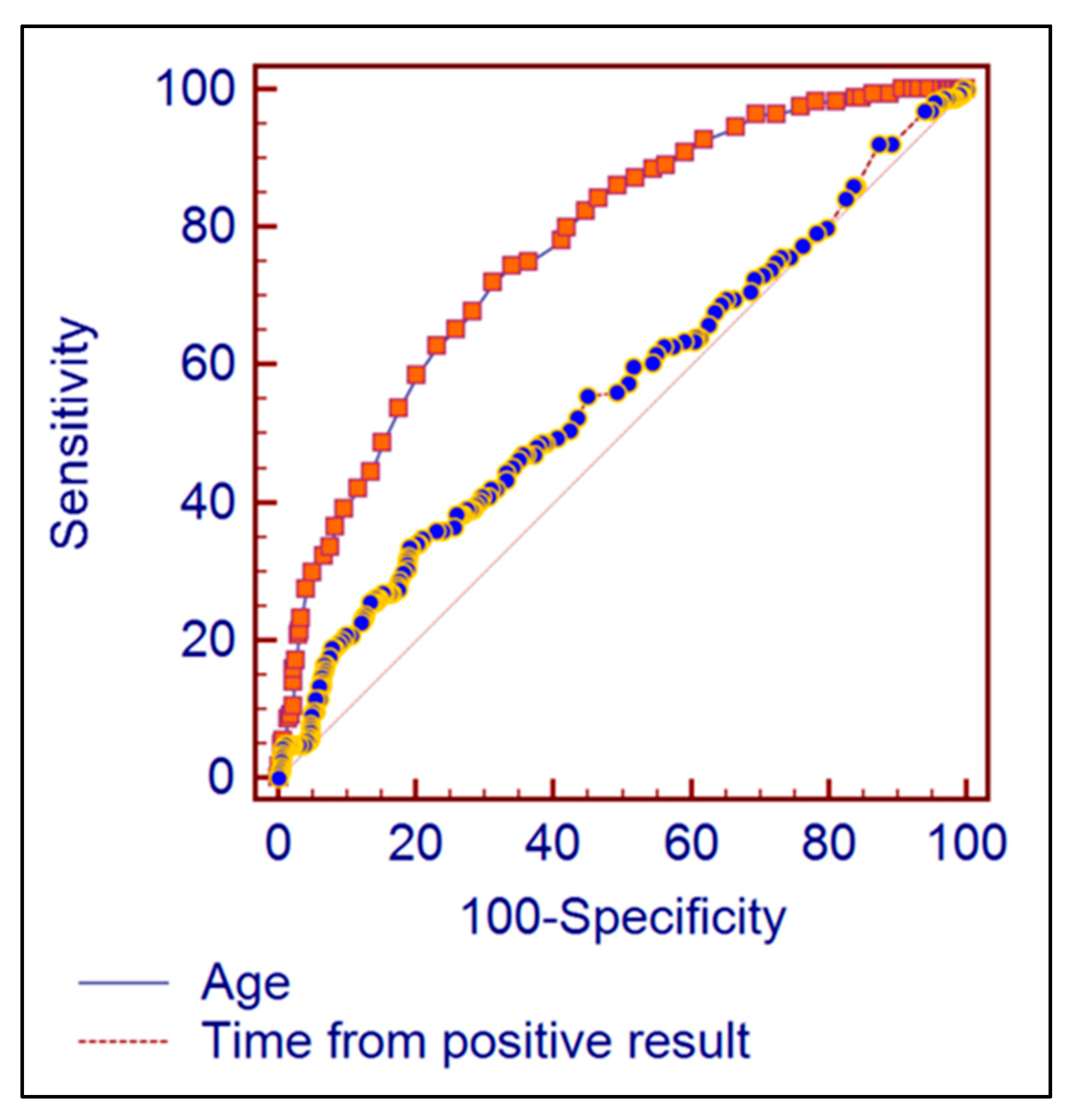
3.2. Time Intervals and Age Group Analysis
4. Discussion
4.1. Current Observations and Literature Findings
4.2. Limitations and Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mohanty, S.K.; Satapathy, A.; Naidu, M.M.; Mukhopadhyay, S.; Sharma, S.; Barton, L.M.; Stroberg, E.; Duval, E.J.; Pradhan, D.; Tzankovet, A.; et al. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) and coronavirus disease 19 (COVID-19)—anatomic pathology perspective on current knowledge. Diagn. Pathol. 2020, 15, 103. [Google Scholar] [CrossRef] [PubMed]
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Adam, D. The pandemic’s true death toll: Millions more than official counts. Nature 2022, 601, 312–315. [Google Scholar] [CrossRef] [PubMed]
- Lopes-Pacheco, M.; Silva, P.L.; Cruz, F.F.; Battaglini, D.; Robba, C.; Pelosi, P.; Morales, M.M.; Neves, C.C.; Rocco, P.R.M. Pathogenesis of Multiple Organ Injury in COVID-19 and Potential Therapeutic Strategies. Front. Physiol. 2021, 12, 593223. [Google Scholar] [CrossRef] [PubMed]
- Mokhtari, T.; Hassani, F.; Ghaffari, N.; Ebrahimi, B.; Yarahmadi, A.; Hassanzadeh, G. COVID-19 and multiorgan failure: A narrative review on potential mechanisms. J. Mol. Histol. 2020, 51, 613–628. [Google Scholar] [CrossRef]
- Vadász, I.; Husain-Syed, F.; Dorfmüller, P.; Roller, F.C.; Tello, K.; Hecker, M.; Morty, R.E.; Gattenlöhner, S.; Walmrath, H.D.; Grimminger, F.; et al. Severe organising pneumonia following COVID-19. Thorax 2021, 76, 201–204. [Google Scholar] [CrossRef]
- Pannone, G.; Caponio, V.C.A.; De Stefano, I.S.; Ramunno, M.A.; Meccariello, M.; Agostinone, A.; Pedicillo, M.C.; Troiano, G.; Zhurakivska, K.; Cassano, T.; et al. Lung histopathological findings in COVID-19 disease—A systematic review. Infect. Agent. Cancer 2021, 16, 34. [Google Scholar] [CrossRef]
- Matthay, M.A.; Zemans, R.L. The acute respiratory distress syndrome: Pathogenesis and treatment. Annu. Rev. Pathol. 2011, 6, 147–163. [Google Scholar] [CrossRef] [Green Version]
- Poerio, A.; Carlicchi, E.; Lotrecchiano, L.; Praticò, C.; Mistè, G.; Scavello, S.; Morsiani, M.; Zompatori, M.; Ferrari, R. Evolution of COVID-19 Pulmonary Fibrosis-Like Residual Changes Over Time—Longitudinal Chest CT up to 9 Months After Disease Onset: A Single-Center Case Series. SN Compr. Clin. Med. 2022, 4, 57. [Google Scholar] [CrossRef]
- de Paula, C.B.V.; Nagashima, S.; Liberalesso, V.; Collete, M.; da Silva, F.P.G.; Oricil, A.G.G.; Barbosa, G.S.; da Silva, G.V.C.; Wiedmer, D.B.; Dezidério, F.d.; et al. COVID-19: Immunohistochemical Analysis of TGF-β Signaling Pathways in Pulmonary Fibrosis. Int. J. Mol. Sci. 2021, 23, 168. [Google Scholar] [CrossRef]
- Rai, D.K.; Sharma, P.; Kumar, R. Post COVID 19 pulmonary fibrosis. Is it real threat? Indian J. Tuberc. 2021, 68, 330–333. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Shen, C.; Wang, L.; Majumder, S.; Zhang, D.; Deen, M.J.; Li, Y.; Qing, L.; Zhang, Y.; Chen, C.; et al. Pulmonary fibrosis and its related factors in discharged patients with new corona virus pneumonia: A cohort study. Respir. Res. 2021, 22, 203. [Google Scholar] [CrossRef] [PubMed]
- Yazdi, N.A.; Ghadery, A.H.; SeyedAlinaghi, S.; Jafari, F.; Jafari, S.; Hasannezad, M.; Koochak, H.E.; Salehi, M.; Manshadi, S.A.D.; Meidani, M.; et al. Predictors of the chest CT score in COVID-19 patients: A cross-sectional study. Virol. J. 2021, 18, 225. [Google Scholar] [CrossRef] [PubMed]
- Guan, X.; Yao, L.; Tan, Y.; Shen, Z.; Zheng, H.; Zhou, H.; Gao, Y.; Li, Y.; Ji, W.; Zhang, H.; et al. Quantitative and semiquantitative CT assessments of lung lesion burden in COVID-19 pneumonia. Sci. Rep. 2021, 11, 5148. [Google Scholar] [CrossRef]
- Yang, R.; Li, X.; Liu, H.; Zhen, Y.; Zhang, X.; Xiong, Q.; Luo, Y.; Gao, C.; Zeng, W. Chest CT Severity Score: An Imaging Tool for Assessing Severe COVID-19. Radiol. Cardiothorac. Imaging 2020, 30, e200047. [Google Scholar] [CrossRef] [Green Version]
- Solomon, J.J.; Heyman, B.; Ko, J.P.; Condos, R.; Lynch, D.A. CT of Post-Acute Lung Complications of COVID-19. Radiology 2021, 301, E383–E395. [Google Scholar] [CrossRef]
- Han, X.; Fan, Y.; Alwalid, O.; Li, N.; Jia, X.; Yuan, M.; Li, Y.; Cao, Y.; Gu, J.; Wu, H.; et al. Six-month Follow-up Chest CT Findings after Severe COVID-19 Pneumonia. Radiology 2021, 299, E177–E186. [Google Scholar] [CrossRef]
- Liu, X.; Zhou, H.; Zhou, Y.; Wu, X.; Zhao, Y.; Lu, Y.; Tan, W.; Yuan, M.; Ding, X.; Zou, J.; et al. Temporal radiographic changes in COVID-19 patients: Relationship to disease severity and viral clearance. Sci. Rep. 2020, 10, 10263. [Google Scholar] [CrossRef]
- Chen, C.; Wang, X.; Dong, J.; Nie, D.; Chen, Q.; Yang, F.; Chen, W. Temporal lung changes in high-resolution chest computed tomography for coronavirus disease 2019. J. Int. Med. Res. 2020, 48, 300060520950990. [Google Scholar] [CrossRef]
- Yasin, R.; Gouda, W. Chest X-ray findings monitoring COVID-19 disease course and severity. Egypt. J. Radiol. Nucl. Med. 2020, 51, 193. [Google Scholar] [CrossRef]
- Ozturk, S.; Ozturk, E.K.; Kaya, S.Y. Clinical and radiological characteristics of COVID-19 patients without comorbidities: A single-center study. Wien. Klin. Wochenschr. 2021, 133, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Dong, C.; Hu, Y.; Li, C.; Ren, Q.; Zhang, X.; Shi, H.; Zhou, M. Temporal Changes of CT Findings in 90 Patients with COVID-19 Pneumonia: A Longitudinal Study. Radiology 2020, 296, E55–E64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irizato, N.; Matsuura, H.; Okada, A.; Ueda, K.; Yamamura, H. Serial computed tomography findings of Coronavirus disease 2019 (COVID-19) pneumonia treated with favipiravir and steroid therapy: Report of 11 cases. Bull. Natl. Res. Cent. 2021, 45, 92. [Google Scholar] [CrossRef] [PubMed]
- Yin, X.; Xi, X.; Min, X.; Feng, Z.; Li, B.; Cai, W.; Fan, C.; Wang, L.; Xia, L. Long-term chest CT follow-up in COVID-19 Survivors: 102-361 days after onset. Ann. Transl. Med. 2021, 9, 1231. [Google Scholar] [CrossRef]
- Vijayakumar, B.; Tonkin, J.; Devaraj, A.; Philip, K.E.J.; Orton, C.M.; Desai, S.R.; Shah, P.L. CT Lung Abnormalities after COVID-19 at 3 Months and 1 Year after Hospital Discharge. Radiology 2022, 303, 444–454. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scores | Categories |
|---|---|
| Lung lobe score | |
| 0 | No lobar involvement |
| 1 | <5% |
| 2 | 5–25% |
| 3 | 25–50% |
| 4 | 50–75% |
| 5 | >75% |
| CT Severity Score | |
| <10 | Mild |
| 10–20 | Moderate |
| >20 | Severe |
| Interval | Period | Frequency |
|---|---|---|
| 1st Interval | <30 days | 5.68% |
| 2nd Interval | 30–60 days | 46.02% |
| 3rd Interval | 60–90 days | 21.78% |
| 4th Interval | 90–120 days | 10.98% |
| 5th Interval | >120 days | 15.53% |
| HRCT Findings | 1st Interval (n = 33) | 2nd Interval (n = 267) | 3rd Interval (n = 154) | 4th Interval (n = 76) | 5th Interval (n = 105) | p-Value * |
|---|---|---|---|---|---|---|
| Complete remission (n = 164) | 13 (7.9%) | 59 (36.0%) | 33 (20.1%) | 20 (12.2%) | 39 (23.8%) | 0.014 |
| Ground-glass opacities (n = 408) | 47 (11.5%) | 164 (40.2%) | 101 (24.8%) | 47 (11.5%) | 49 (12.0%) | 0.014 |
| Crazy paving (n = 92) | 21 (22.8%) | 44 (47.8%) | 17 (18.5%) | 3 (3.3%) | 7 (7.6%) | <0.001 |
| Condensing (n = 35) | 11 (31.4%) | 20 (57.1%) | 2 (5.7%) | 1 (2.9%) | 1 (2.9%) | <0.001 |
| Trabeculation (n = 374) | 35 (9.4%) | 145 (38.8%) | 100 (26.7%) | 45 (12.0%) | 49 (13.1%) | 0.121 |
| Bronchiectasis (n = 142) | 14 (9.9%) | 47 (33.1%) | 43 (30.3%) | 17 (12.0%) | 21 (14.8%) | 0.311 |
| Pulmonary cysts (n = 75) | 5 (6.7%) | 29 (38.7%) | 17 (22.7%) | 7 (9.3%) | 17 (22.7%) | 0.390 |
| Tractions (n = 161) | 16 (9.9%) | 65 (40.4%) | 39 (24.2%) | 18 (11.2%) | 23 (14.3%) | 0.984 |
| Pleural thickening (n = 195) | 18 (9.2%) | 79 (40.5%) | 52 (26.7%) | 19 (9.7%) | 27 (13.8%) | 0.633 |
| HRCT total score | 10.5 ± 8.0 | 6.4 ± 6.0 | 7.2 ± 6.4 | 7.1 ± 6.7 | 4.9 ± 6.1 | <0.001 |
| HRCT Findings | 18–40 Years | 40–65 Years | >65 Years | p-Value * |
|---|---|---|---|---|
| Complete remission (n = 164) | 55 (33.5%) | 103 (62.8%) | 6 (3.7%) | <0.001 |
| Ground-glass opacities (n = 408) | 29 (7.1%) | 245 (60.0%) | 134 (32.8%) | <0.001 |
| Crazy paving (n = 92) | 3 (3.3%) | 42 (45.7%) | 47 (51.1%) | 0.008 |
| Condensing (n = 35) | 2 (5.7%) | 14 (40.0%) | 19 (54.3%) | <0.001 |
| Trabeculation (n = 374) | 24 (6.4%) | 229 (61.2%) | 121 (32.4%) | <0.001 |
| Bronchiectasis (n = 142) | 5 (3.5%) | 80 (56.3%) | 57 (40.1%) | <0.001 |
| Pulmonary cysts (n = 75) | 0 (0.0%) | 39 (52.0%) | 36 (48.0%) | 0.030 |
| Tractions (n = 161) | 10 (6.2%) | 97 (60.2%) | 54 (33.5%) | <0.001 |
| Pleural thickening (n = 195) | 11 (5.6%) | 110 (56.4%) | 74 (37.9%) | <0.001 |
| HRCT total score | 2.7 ± 4.8 | 6.1 ± 6.1 | 10.6 ± 6.0 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manolescu, D.; Timar, B.; Bratosin, F.; Rosca, O.; Citu, C.; Oancea, C. Predictors for COVID-19 Complete Remission with HRCT Pattern Evolution: A Monocentric, Prospective Study. Diagnostics 2022, 12, 1397. https://doi.org/10.3390/diagnostics12061397
Manolescu D, Timar B, Bratosin F, Rosca O, Citu C, Oancea C. Predictors for COVID-19 Complete Remission with HRCT Pattern Evolution: A Monocentric, Prospective Study. Diagnostics. 2022; 12(6):1397. https://doi.org/10.3390/diagnostics12061397
Chicago/Turabian StyleManolescu, Diana, Bogdan Timar, Felix Bratosin, Ovidiu Rosca, Cosmin Citu, and Cristian Oancea. 2022. "Predictors for COVID-19 Complete Remission with HRCT Pattern Evolution: A Monocentric, Prospective Study" Diagnostics 12, no. 6: 1397. https://doi.org/10.3390/diagnostics12061397