
Personalized Diagnosis in Differentiated Thyroid Cancers by Molecular and Functional Imaging Biomarkers: Present and Future

 ,
,
Abstract
:1. Introduction
2. Functional Imaging Available in Thyroid Carcinomas
3. The Future in Theragnostic: DTC Radionuclide Somatostatin Receptor and Redifferentiation Therapies
NIS Targeted Gene Therapy
4. Molecular Biomarker Diagnosis in Differential Thyroid Carcinoma
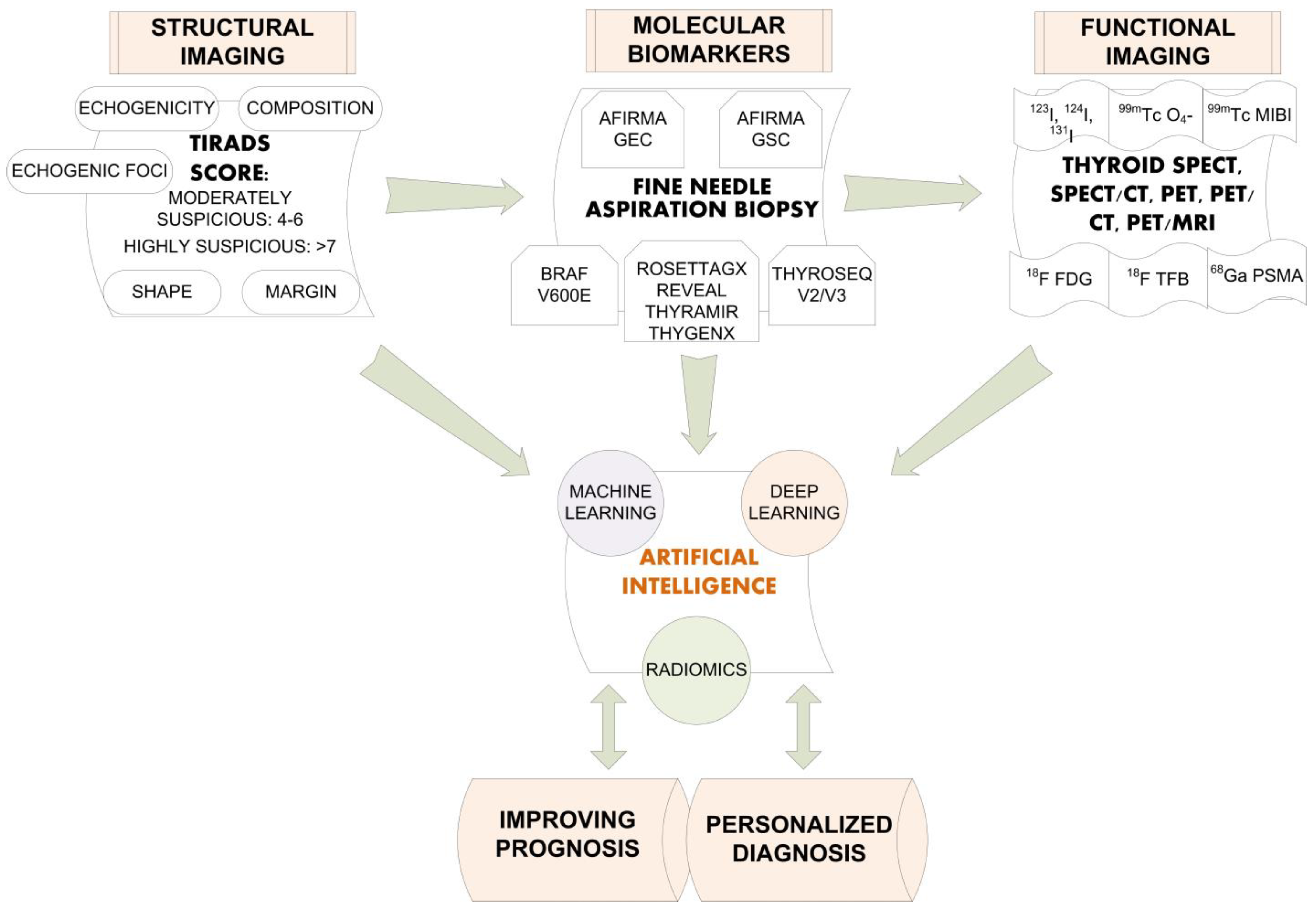
5. Artificial Intelligence in Thyroid Carcinoma

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Accuracy | Sensitivity | Specificity | |
|---|---|---|---|
| Kim et al. 2021 | 85.10% | 81.80% | 86.10% |
| Wu et al. 2021 | 82% | 85% | 78% |
| Jin et al. 2020 | 80.30% | 80.60% | 80.10% |
| Liang et al. 2020 | 75% | 84.90% | 69% |
| Buda et al. 2019 | N/A | 87% | 52% |
| Ko et al. 2019 | 87.30% | 90% | 82% |
| Park et al. 2019 | 86% | 91% | 80% |
| Wang et al. 2019 | 90.30% | 90.50% | 89.90% |
| Li et al. 2019 | 86% | 84% | 87% |
| Chi et al. 2017 | 96.30% | 82.80% | 99.30% |
| Ma et al. 2017 | 83% | 82.40% | 84.90% |
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- American Cancer Society. Available online: https://www.cancer.org/cancer/thyroid-cancer/about/key-statistics.html (accessed on 15 January 2022).
- American Cancer Society. Available online: https://www.cancer.org/cancer/thyroid-cancer/detection-diagnosis-staging/survival-rates.html (accessed on 15 January 2022).
- International Agency for Research on Cancer, World Health Organization. Available online: https://gco.iarc.fr/today/data/factsheets/populations/908-europe-fact-sheets.pdf (accessed on 15 January 2022).
- International Agency for Research on Cancer, World Health Organization. Available online: https://gco.iarc.fr/today/data/factsheets/cancers/32-Thyroid-fact-sheet.pdf (accessed on 15 January 2022).
- Piciu, D. Thyroid cancer incidence 25 years after Chernobyl, in a Romanian cancer center: Is it a public health problem? Curr. Radiopharm. 2013, 6, 249–252. [Google Scholar] [CrossRef] [PubMed]
- Rager, O.; Radojewski, P.; Dumont, R.A.; Treglia, G.; Giovanella, L.; Walter, M.A. Radioisotope imaging for discriminating benign from malignant cytologically indeterminate thyroid nodules. Gland Surg. 2019, 8, S118–S125. [Google Scholar] [CrossRef]
- Giovanella, L.; Avram, A.M.; Iakovou, I.; Kwak, J.; Lawson, S.A.; Lulaj, E.; Luster, M.; Piccardo, A.; Schmidt, M.; Tulchinsky, M.; et al. EANM practice guideline/SNMMI procedure standard for RAIU and thyroid scintigraphy. Eur. J. Pediatr. 2019, 46, 2514–2525. [Google Scholar] [CrossRef] [PubMed]
- Santhanam, P.; Solnes, L.B.; Rowe, S.P. Molecular imaging of advanced thyroid cancer: Iodinated radiotracers and beyond. Med. Oncol. 2017, 34, 189. [Google Scholar] [CrossRef] [PubMed]
- McCready, V.R. Radioiodine—The success story of Nuclear Medicine: 75th Anniversary of the first use of Iodine-131 in humans. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 179–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spanu, A.; Nuvoli, S.; Marongiu, A.; Gelo, I.; Mele, L.; De Vito, A.; Rondini, M.; Madeddu, G. The Diagnostic usefulness of 131I-SPECT/CT at both radioiodine ablation and during long-term follow-up in patients thyroidectomized for differentiated thyroid carcinoma: Analysis of tissue risk factors ascertained at surgery and correlated with metastasis appearance. Diagnostics 2021, 11, 1504. [Google Scholar] [CrossRef] [PubMed]
- Giovanella, L.; Avram, A.M.; Ovčariček, P.P.; Clerc, J. Thyroid functional and molecular imaging. Presse Med. 2022, 51, 104116. [Google Scholar] [CrossRef]
- Kuker, R.; Sztejnberg, M.; Gulec, S. I-124 imaging and dosimetry. I-124 görüntüleme ve dozimetri. Mol. Imaging Radionucl. Ther. 2017, 26, 66–73. [Google Scholar] [CrossRef]
- Wu, D.; Ylli, D.; Heimlich, M.S.L.; Burman, K.D.; Wartofsky, L.; Van Nostrand, D. 124I positron emission tomography/computed tomography versus conventional radioiodine imaging in differentiated thyroid cancer: A review. Thyroid 2019, 29, 1523–1535. [Google Scholar] [CrossRef]
- Jalloul, W.; Tibu, R.; Ionescu, T.M.; Stolniceanu, C.; Grierosu, I.; Tarca, A.; Ionescu, L.; Ungureanu, M.C.; Ciobanu, D.; Ghizdovat, V.; et al. Personalizes nuclear imaging protocol in cases with nodular goiter and parathyroid adenoma. Acta Endocrinol. 2021, 17, 393–398. [Google Scholar]
- Zhang, Y.; Wang, J. Targeting uptake transporters for cancer imaging and treatment. Acta Pharm. Sinica B 2020, 10, 79–90. [Google Scholar] [CrossRef] [PubMed]
- Jauregui-Osoro, M.; Sunassee, K.; Weeks, A.J.; Berry, D.J.; Paul, R.L.; Cleij, M.; Banga, J.P.; O’Doherty, M.J.; Marsden, P.K.; Clarke, S.E.M.; et al. Synthesis and biological evaluation of [18F]tetrafluoroborate: A PET imaging agent for thyroid disease and reporter gene imaging of the sodium/iodide symporter. Eur. J. Pediatr. 2010, 37, 2108–2116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, H.; DeGrado, T.R. [18F]Tetrafluoroborate ([18F]TFB) and its analogs for PET imaging of the sodium/iodide symporter. Theranostics 2018, 8, 3918–3931. [Google Scholar] [CrossRef] [PubMed]
- Doherty, J.O.; Jauregui-Osoro, M.; Brothwood, T.; Szyszko, T.; Marsden, P.K.; Doherty, M.J.O.; Cook, G.; Blower, P.; Lewington, V. 18F-Tetrafluoroborate, a PET probe for imaging sodium/iodide symporter expression: Whole-body biodistribution, safety, and radiation dosimetry in thyroid cancer patients. J. Nucl. Med. 2017, 58, 1666–1671. [Google Scholar] [CrossRef] [Green Version]
- Jiang, H.; Schmit, N.R.; Koenen, A.R.; Bansal, A.; Pandey, M.K.; Glynn, R.B.; Kemp, B.J.; Delaney, K.L.; Dispenzieri, A.; Bakkum-Gamez, J.N.; et al. Safety, pharmacokinetics, metabolism and radiation dosimetry of 18F-tetrafluoroborate (18F-TFB) in healthy human subjects. EJNMMI Res. 2017, 7, 90. [Google Scholar] [CrossRef] [Green Version]
- Dittmann, M.; Carvalho, J.M.G.; Rahbar, K.; Schäfers, M.; Claesener, M.; Riemann, B.; Seifert, R. Incremental diagnostic value of [18F]tetrafluoroborate PET-CT compared to [131I]iodine scintigraphy in recurrent differentiated thyroid cancer. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2639–2646. [Google Scholar] [CrossRef] [Green Version]
- Piccardo, A.; Trimboli, P.; Foppiani, L.; Treglia, G.; Ferrarazzo, G.; Massollo, M.; Bottoni, G.; Giovanella, L. PET/CT in thyroid nodule and differentiated thyroid cancer patients. The evidence-based state of the art. Rev. Endocr. Metab. Disord. 2019, 20, 47–64. [Google Scholar] [CrossRef]
- Signore, G.; Albano, D.; Giovanella, L.; Bertagna, F.; Treglia, G. Evidence-based data about prevalence and risk of malignancy of thyroid incidentalomas detected by different PET radiopharmaceuticals. Curr. Radiopharm. 2020, 13, 89–93. [Google Scholar] [CrossRef]
- Shie, P.; Cardarelli, R.; Sprawls, K.; Fulda, K.G.; Taur, A. Systematic review: Prevalence of malignant incidental thyroid nodules identified on fluorine-18 fluorodeoxyglucose positron emission tomography. Nucl. Med. Commun. 2009, 30, 742–748. [Google Scholar] [CrossRef]
- Soelberg, K.K.; Bonnema, S.J.; Brix, T.H.; Hegedüs, L. Risk of malignancy in thyroid incidentalomas detected by18F-fluorodeoxyglucose positron emission tomography: A systematic review. Thyroid 2012, 22, 918–925. [Google Scholar] [CrossRef]
- Bertagna, F.; Treglia, G.; Piccardo, A.; Giubbini, R. Diagnostic and clinical significance of F-18-FDG-PET/CT thyroid incidentalomas. J. Clin. Endocrinol. Metab. 2012, 97, 3866–3875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treglia, G.; Bertagna, F.; Sadeghi, R.; Verburg, F.A.; Ceriani, L.; Giovanella, L. Focal thyroid incidental uptake detected by 18F-fluorodeoxyglucose positron emission tomography. Meta-analysis on prevalence and malignancy risk. Nuklearmedizi 2013, 52, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Qu, N.; Zhang, L.; Lu, Z.-W.; Wei, W.-J.; Zhang, Y.; Ji, Q.-H. Risk of malignancy in focal thyroid lesions identified by 18F-fluorodeoxyglucose positron emission tomography or positron emission tomography/computed tomography: Evidence from a large series of studies. Tumor Biol. 2014, 35, 6139–6147. [Google Scholar] [CrossRef] [PubMed]
- Nayan, S.; Ramakrishna, J.; Gupta, M.K. The proportion of malignancy in incidental thyroid lesions on 18-FDG PET study: A systematic review and meta-analysis. Otolaryngol. Head. Neck Surg. 2014, 151, 190–200. [Google Scholar] [CrossRef] [PubMed]
- de Leijer, J.F.; Metman, M.J.H.; van der Hoorn, A.; Brouwers, A.H.; Kruijff, S.; van Hemel, B.M.; Links, T.P.; Westerlaan, H.E. Focal thyroid incidentalomas on 18F-FDG PET/CT: A systematic review and meta-analysis on prevalence, risk of malignancy and inconclusive fine needle aspiration. Front. Endocrinol. 2021, 12, 723394. [Google Scholar] [CrossRef] [PubMed]
- Scappaticcio, L.; Piccardo, A.; Treglia, G.; Poller, D.N.; Trimboli, P. The dilemma of 18F-FDG PET/CT thyroid incidentaloma: What we should expect from FNA. A systematic review and meta-analysis. Endocrine 2021, 73, 540–549. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Zhai, H.; Lu, Y. Is fluorine-18 fluorodeoxyglucose positron emission tomography useful for the thyroid nodules with indeterminate fine needle aspiration biopsy? A meta-analysis of the literature. J. Otolaryngol. Head Neck Surg. 2013, 42, 38. [Google Scholar] [CrossRef] [Green Version]
- Vriens, D.; Adang, E.M.M.; Netea-Maier, R.T.; Smit, J.W.A.; De Wilt, J.H.W.; Oyen, W.J.G.; De Geus-Oei, L.F. Cost-effectiveness of FDG-PET/CT for cytologically indeterminate thyroid nodules: A decision analytic approach. J. Clin. Endocrinol. Metab. 2014, 99, 3263–3274. [Google Scholar] [CrossRef] [Green Version]
- Castellana, M.; Trimboli, P.; Piccardo, A.; Giovanella, L.; Treglia, G. Performance of 18F-FDG PET/CT in Selecting thyroid nodules with indeterminate fine-needle aspiration cytology for surgery. A systematic review and a meta-analysis. J. Clin. Med. 2019, 8, 1333. [Google Scholar] [CrossRef] [Green Version]
- Wan, Q.; Shen, J.; Li, L.; Ji, B.; Wang, R.; Zheng, X. Comparison of 18F-FDG-PET and 18F-FDG-PET/CT for the diagnostic performance in thyroid nodules with indeterminate cytology: A meta-analysis. Medicine 2020, 99, e20446. [Google Scholar] [CrossRef]
- Dong, M.-J.; Liu, Z.-F.; Zhao, K.; Ruan, L.-X.; Wang, G.-L.; Yang, S.-Y.; Sun, F.; Luo, X.-G. Value of 18F-FDG-PET/PET-CT in differentiated thyroid carcinoma with radioiodine-negative whole-body scan: A meta-analysis. Nucl. Med. Commun. 2009, 30, 639–650. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.E.; Chen, Q.; Elashoff, D.; Abemayor, E.; John, M.S. Positron emission tomography and positron emission tomography-CT evaluation for recurrent papillary thyroid carcinoma: Meta-analysis and literature review. Head Neck 2011, 33, 562–565. [Google Scholar] [CrossRef] [PubMed]
- Caetano, R.; Bastos, C.R.G.; De Oliveira, I.A.G.; Da Silva, R.M.; Fortes, C.P.D.D.; Pepe, V.L.E.; Reis, L.G.; Braga, J.U. Accuracy of positron emission tomography and positron emission tomography-CT in the detection of differentiated thyroid cancer recurrence with negative131I whole-body scan results: A meta-analysis. Head Neck 2015, 38, 316–327. [Google Scholar] [CrossRef]
- Haslerud, T.M.; Brauckhoff, K.; Reisæter, L.A.R.; Lein, R.K.; Heinecke, A.; Varhaug, J.E.; Biermann, M. F18-FDG-PET for recurrent differentiated thyroid cancer: A systematic meta-analysis. Acta Radiol. 2016, 57, 1193–1200. [Google Scholar] [CrossRef] [Green Version]
- Schütz, F.; Lautenschläger, C.; Lorenz, K.; Haerting, J. Positron Emission Tomography (PET) and PET/CT in thyroid cancer: A systematic review and meta-analysis. Eur. Thyroid J. 2018, 7, 13–20. [Google Scholar] [CrossRef]
- Kim, S.K.; So, Y.; Chung, H.W.; Yoo, Y.B.; Park, K.S.; Hwang, T.S.; Kim, B.; Lee, W.W. Analysis of predictability of F-18 fluorodeoxyglucose- PET/CT in the recurrence of papillary thyroid carcinoma. Cancer Med. 2016, 5, 2756–2762. [Google Scholar] [CrossRef] [PubMed]
- Qichang, W.; Lin, B.; Gege, Z.; Youjia, Z.; Qingjie, M.; Renjie, W.; Bin, J.; Wan, Q.; Bai, L.; Zhao, G.; et al. Diagnostic performance of 18F-FDG-PET/CT in DTC patients with thyroglobulin elevation and negative iodine scintigraphy: A meta-analysis. Eur. J. Endocrinol. 2019, 181, 93–102. [Google Scholar] [CrossRef]
- Treglia, G.; Caldarella, C.; Saggiorato, E.; Ceriani, L.; Orlandi, F.; Salvatori, M.; Giovanella, L. Diagnostic performance of 99mTc-MIBI scan in predicting the malignancy of thyroid nodules: A meta-analysis. Endocrine 2013, 44, 70–78. [Google Scholar] [CrossRef]
- Erdil, T.Y.; Özker, K.; Kabasakal, L.; Kanmaz, B.; Sönmezoglu, K.; Atasoy, K.; Turoglu, H.T.; Uslu, I.; Isitman, A.T.; Onsel, C. Correlation of technetium-99m MIBI and thallium-201 retention in solitary cold thyroid nodules with postoperative histopathology. Eur. J. Nucl. Med. 2000, 27, 713–720. [Google Scholar] [CrossRef]
- Campennì, A.; Siracusa, M.; Ruggeri, R.M.; Laudicella, R.; Pignata, S.A.; Baldari, S.; Giovanella, L. Differentiating malignant from benign thyroid nodules with indeterminate cytology by 99mTc-MIBI scan: A new quantitative method for improving diagnostic accuracy. Sci. Rep. 2017, 7, 6147. [Google Scholar] [CrossRef] [Green Version]
- Saggiorato, E.; Angusti, T.; Rosas, R.; Martinese, M.; Finessi, M.; Arecco, F.; Trevisiol, E.; Bergero, N.; Puligheddu, B.; Volante, M.; et al. 99mTc-MIBI imaging in the presurgical characterization of thyroid follicular neoplasms: Relationship to multidrug resistance protein expression. J. Nucl. Med. 2009, 50, 1785–1793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertagna, F.; Albano, D.; Giovanella, L.; Bonacina, M.; Durmo, R.; Giubbini, R.; Treglia, G. 68Ga-PSMA PET thyroid incidentalomas. Hormones 2019, 18, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Piek, M.W.; de Vries, L.H.; Donswijk, M.L.; de Keizer, B.; de Boer, J.P.; Lodewijk, L.; van Leeuwaarde, R.S.; Vriens, M.R.; Hartemink, K.J.; van der Ploeg, I.M.C. Retrospective analysis of PSMA PET/CT thyroid incidental uptake in adults: Incidence, diagnosis, and treatment/outcome in a tertiary cancer referral center and University Medical Center. Eur. J. Nucl. Med. Mol. Imaging 2022, 1–9, Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Gossili, F.; Petersen, L.J.; Zacho, H.D. The frequency of thyroid incidental findings and risk of malignancy detected by 68Ga-labeled prostate-specific membrane antigen PET/CT in prostate cancer. Hell J. Nucl. Med. 2020, 23, 240–245. [Google Scholar] [PubMed]
- Lawhn-Heath, C.; Yom, S.S.; Liu, C.; Villanueva-Meyer, J.E.; Aslam, M.; Smith, R.; Narwal, M.; Juarez, R.; Behr, S.C.; Pampaloni, M.H.; et al. Gallium-68 prostate-specific membrane antigen ([68Ga]Ga-PSMA-11) PET for imaging of thyroid cancer: A feasibility study. EJNMMI Res. 2020, 10, 128. [Google Scholar] [CrossRef] [PubMed]
- Pitalua-Cortes, Q.; García-Perez, F.O.; Vargas-Ahumada, J.; Gonzalez-Rueda, S.; Gomez-Argumosa, E.; Ignacio-Alvarez, E.; Soldevilla-Gallardo, I.; Torres-Agredo, L. Head-to-head comparison of 68Ga-PSMA-11 and 131I in the follow-up of well-differentiated metastatic thyroid cancer: A new potential theragnostic agent. Front. Endocrinol. 2021, 12, 794759. [Google Scholar] [CrossRef] [PubMed]
- Santhanam, P.; Russell, J.; Rooper, L.M.; Ladenson, P.W.; Pomper, M.G.; Rowe, S.P. The prostate-specific membrane antigen (PSMA)-targeted radiotracer 18F-DCFPyL detects tumor neovasculature in metastatic, advanced, radioiodine-refractory, differentiated thyroid cancer. Med. Oncol. 2020, 37, 98. [Google Scholar] [CrossRef]
- Albano, D.; Durmo, R.; Bertagna, F.; Giubbini, R. 18F-choline PET/CT incidental thyroid uptake in patients studied for prostate cancer. Endocrine 2019, 63, 531–536. [Google Scholar] [CrossRef]
- Salavati, A.; Puranik, A.; Kulkarni, H.R.; Budiawan, H.; Baum, R.P. Peptide Receptor Radionuclide Therapy (PRRT) of medullary and nonmedullary thyroid cancer using radiolabeled somatostatin analogues. Semin. Nucl. Med. 2016, 46, 215–224. [Google Scholar] [CrossRef]
- Schrell, U.; Buchfelder, M.; Hensen, J.; Wendler, J.; Gramatzki, M.; Wolf, F.; Becker, W. Somatostatin receptor expression in the thyroid demonstrated with 111In-octreotide scintigraphy. Nuklearmedizin 1995, 34, 100–103. [Google Scholar] [CrossRef]
- Liu, H.; Wang, X.; Yang, R.; Zeng, W.; Peng, D.; Li, J.; Wang, H. Recent development of nuclear molecular imaging in thyroid cancer. BioMed Res. Int. 2018, 2018, 2149532. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, H.; England, J.A.; Rafferty, A.; Jesudason, V.; Bedford, K.; Karsai, L.; Atkin, S.L. Somatostatin receptor expression in thyroid disease. Int. J. Exp. Pathol. 2013, 94, 226–229. [Google Scholar] [CrossRef] [PubMed]
- Rogoza, O.; Megnis, K.; Kudrjavceva, M.; Gerina-Berzina, A.; Rovite, V. Role of somatostatin signalling in neuroendocrine tumours. Int. J. Mol. Sci. 2022, 23, 1447. [Google Scholar] [CrossRef]
- Czepczyński, R.; Matysiak-Grześ, M.; Gryczyńska, M.; Bączyk, M.; Wyszomirska, A.; Stajgis, M.; Ruchała, M. Peptide receptor radionuclide therapy of differentiated thyroid cancer: Efficacy and toxicity. Arch. Immunol. Ther. Exp. 2015, 63, 147–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Versari, A.; Sollini, M.; Frasoldati, A.; Fraternali, A.; Filice, A.; Froio, A.; Asti, M.; Fioroni, F.; Cremonini, N.; Putzer, D.; et al. Differentiated thyroid cancer: A new perspective with radiolabeled somatostatin analogues for imaging and treatment of patients. Thyroid 2014, 24, 715–726. [Google Scholar] [CrossRef] [PubMed]
- Maghsoomi, Z.; Emami, Z.; Malboosbaf, R.; Malek, M.; Khamseh, M.E. Efficacy and safety of peptide receptor radionuclide therapy in advanced radioiodine-refractory differentiated thyroid cancer and metastatic medullary thyroid cancer: A systematic review. BMC Cancer 2021, 21, 579. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.Y.; Kim, Y.-I. Peptide receptor radionuclide therapy in patients with differentiated thyroid cancer: A meta-analysis. Clin. Nucl. Med. 2020, 45, 604–610. [Google Scholar] [CrossRef]
- Roll, W.; Riemann, B.; Schäfers, M.; Stegger, L.; Vrachimis, A. 177Lu-DOTATATE therapy in radioiodine-refractory differentiated thyroid cancer: A single center experience. Clin. Nucl. Med. 2018, 43, e346–e351. [Google Scholar] [CrossRef]
- Basu, S.; Parghane, R.V.; Naik, C. Clinical efficacy of 177 Lu-DOTATATE peptide receptor radionuclide therapy in thyroglobulin-elevated negative iodine scintigraphy: A “not-so-promising” result compared to GEP-NETs. World J. Nucl. Med. 2020, 19, 205–210. [Google Scholar] [CrossRef]
- De Vries, L.H.; Lodewijk, L.; Braat, A.J.A.T.; Krijger, G.C.; Valk, G.D.; Lam, M.G.E.H.; Rinkes, I.H.M.B.; Vriens, M.R.; De Keizer, B. 68Ga-PSMA PET/CT in radioactive iodine-refractory differentiated thyroid cancer and first treatment results with 177Lu-PSMA-617. EJNMMI Res. 2020, 10, 1–8. [Google Scholar] [CrossRef]
- Bychkov, A.; Vutrapongwatana, U.; Tepmongkol, S.; Keelawat, S. PSMA expression by microvasculature of thyroid tumors—Potential implications for PSMA theranostics. Sci. Rep. 2017, 7, 5202. [Google Scholar] [CrossRef] [PubMed]
- Assadi, M.; Ahmadzadehfar, H. 177Lu-DOTATATE and177Lu-prostate-specific membrane antigen therapy in a patient with advanced metastatic radioiodine-refractory differentiated thyroid cancer after failure of tyrosine kinase inhibitors treatment. World J. Nucl. Med. 2019, 18, 406–408. [Google Scholar] [CrossRef] [PubMed]
- Uijen, M.J.M.; Derks, Y.H.W.; Merkx, R.I.J.; Schilham, M.G.M.; Roosen, J.; Privé, B.M.; van Lith, S.A.M.; van Herpen, C.M.L.; Gotthardt, M.; Heskamp, S.; et al. PSMA radioligand therapy for solid tumors other than prostate cancer: Background, opportunities, challenges, and first clinical reports. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 4350–4368. [Google Scholar] [CrossRef] [PubMed]
- Buffet, C.; Wassermann, J.; Hecht, F.; Leenhardt, L.; Dupuy, C.; Groussin, L.; Lussey-Lepoutre, C. Redifferentiation of radioiodine-refractory thyroid cancers. Endocr. Relat. Cancer 2020, 27, R113–R132. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.M.; Ahn, B.-C. Molecular mechanisms of radioactive iodine refractoriness in differentiated thyroid cancer: Impaired sodium iodide symporter (NIS) expression owing to altered signaling pathway activity and intracellular localization of NIS. Theranostics 2021, 11, 6251–6277. [Google Scholar] [CrossRef]
- Rothenberg, S.M.; McFadden, D.G.; Palmer, E.L.; Daniels, G.H.; Wirth, L.J. Redifferentiation of iodine-refractory BRAF V600E-mutant metastatic papillary thyroid cancer with dabrafenib. Clin. Cancer Res. 2015, 21, 1028–1035. [Google Scholar] [CrossRef] [Green Version]
- Dunn, L.A.; Sherman, E.J.; Baxi, S.S.; Tchekmedyian, V.; Grewal, R.K.; Larson, S.M.; Pentlow, K.S.; Haque, S.; Tuttle, R.M.; Sabra, M.M.; et al. Vemurafenib redifferentiation of BRAF mutant, RAI-refractory thyroid cancers. J. Clin. Endocrinol. Metab. 2019, 104, 1417–1428. [Google Scholar] [CrossRef]
- Ho, A.L.; Grewal, R.K.; Leboeuf, R.; Sherman, E.J.; Pfister, D.G.; Deandreis, D.; Pentlow, K.S.; Zanzonico, P.B.; Haque, S.; Gavane, S.; et al. Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer. N. Engl. J. Med. 2013, 368, 623–632. [Google Scholar] [CrossRef] [Green Version]
- Rosenbaum-Krumme, S.J.; Freudenberg, L.S.; Jentzen, W.; Bockisch, A.; Nagarajah, J. Effects of rosiglitazone on radioiodine negative and progressive differentiated thyroid carcinoma as assessed by 124I PET/CT imaging. Clin. Nucl. Med. 2012, 37, e47–e52. [Google Scholar] [CrossRef]
- Pak, K.; Shin, S.; Kim, S.-J.; Kim, I.-J.; Chang, S.; Koo, P.; Kwak, J.; Kim, J.-H. Response of retinoic acid in patients with radioactive iodine-refractory thyroid cancer: A meta-analysis. Oncol. Res. Treat. 2018, 41, 100–104. [Google Scholar] [CrossRef]
- Huillard, O.; Tenenbaum, F.; Clerc, J.; Goldwasser, F.; Groussin, L. Restoring radioiodine uptake in BRAF V600E-mutated papillary thyroid cancer. J. Endocr. Soc. 2017, 1, 285–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaber, T.; Waguespack, S.G.; Cabanillas, M.E.; Elbanan, M.; Vu, T.; Dadu, R.; Sherman, S.I.; Amit, M.; Santos, E.B.; Zafereo, M.; et al. Targeted therapy in advanced thyroid cancer to resensitize tumors to radioactive iodine. J. Clin. Endocrinol. Metab. 2018, 103, 3698–3705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iravani, A.; Solomon, B.; Pattison, D.A.; Jackson, P.; Kumar, A.S.R.; Kong, G.; Hofman, M.S.; Akhurst, T.; Hicks, R.J. Mitogen-activated protein kinase pathway inhibition for redifferentiation of radioiodine refractory differentiated thyroid cancer: An evolving protocol. Thyroid 2019, 29, 1634–1645. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, M.I.; Junit, S.M.; Ng, K.L.; Jayapalan, J.; Karikalan, B.; Hashim, O.H. Papillary thyroid cancer: Genetic alterations and molecular biomarker investigations. Int. J. Med Sci. 2019, 16, 450–460. [Google Scholar] [CrossRef] [Green Version]
- Bongiovanni, M.; Spitale, A.; Faquin, W.C.; Mazzucchelli, L.; Baloch, Z.W. The bethesda system for reporting thyroid cytopathology: A meta-analysis. Acta Cytol. 2012, 56, 333–339. [Google Scholar] [CrossRef]
- Valderrabano, P.; Khazai, L.; Thompson, Z.J.; Sharpe, S.C.; Tarasova, V.D.; Otto, K.J.; Hallanger-Johnson, J.E.; Wadsworth, J.T.; Wenig, B.M.; Chung, C.H.; et al. Cancer risk associated with nuclear atypia in cytologically indeterminate thyroid nodules: A systematic review and meta-analysis. Thyroid 2018, 28, 210–219. [Google Scholar] [CrossRef]
- Titov, S.; Demenkov, P.S.; Lukyanov, S.A.; Sergiyko, S.V.; Katanyan, G.A.; Veryaskina, Y.A.; Ivanov, M.K. Preoperative detection of malignancy in fine-needle aspiration cytology (FNAC) smears with indeterminate cytology (Bethesda III, IV) by a combined molecular classifier. J. Clin. Pathol. 2020, 73, 722–727. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The american thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [Green Version]
- Silaghi, C.A.; Lozovanu, V.; Georgescu, C.E.; Georgescu, R.D.; Susman, S.; Năsui, B.A.; Dobrean, A.; Silaghi, H. Thyroseq v3, Afirma GSC, and microRNA panels versus previous molecular tests in the preoperative diagnosis of indeterminate thyroid nodules: A systematic review and meta-analysis. Front. Endocrinol. 2021, 12, 649522. [Google Scholar] [CrossRef]
- Agarwal, S.; Bychkov, A.; Jung, C.-K. Emerging biomarkers in thyroid practice and research. Cancers 2021, 14, 204. [Google Scholar] [CrossRef]
- Patel, K.N.; Angell, T.E.; Babiarz, J.; Barth, N.M.; Blevins, T.; Duh, Q.-Y.; Ghossein, R.A.; Harrell, R.M.; Huang, J.; Kennedy, G.C.; et al. Performance of a genomic sequencing classifier for the preoperative diagnosis of cytologically indeterminate thyroid nodules. JAMA Surg. 2018, 153, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Steward, D.L.; Carty, S.E.; Sippel, R.S.; Yang, S.P.; Sosa, J.A.; Sipos, J.A.; Figge, J.J.; Mandel, S.; Haugen, B.R.; Burman, K.D.; et al. Performance of a multigene genomic classifier in thyroid nodules with indeterminate cytology: A prospective blinded multicenter study. JAMA Oncol. 2019, 5, 204–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lithwick-Yanai, G.; Dromi, N.; Shtabsky, A.; Morgenstern, S.; Strenov, Y.; Feinmesser, M.; Kravtsov, V.; Leon, M.E.; Hajdúch, M.; Ali, S.Z.; et al. Multicentre validation of a microRNA-based assay for diagnosing indeterminate thyroid nodules utilising fine needle aspirate smears. J. Clin. Pathol. 2017, 70, 500–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Labourier, E.; Shifrin, A.; Busseniers, A.E.; Lupo, M.A.; Manganelli, M.L.; Andruss, B.; Wylie, D.; Beaudenon-Huibregtse, S. Molecular testing for miRNA, mRNA, and DNA on fine-needle aspiration improves the preoperative diagnosis of thyroid nodules with indeterminate cytology. J. Clin. Endocrinol. Metab. 2015, 100, 2743–2750. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Pan, B.; Xu, L.; Fang, D.; Ma, X.; Lu, H. The diagnostic performance of afirma gene expression classifier for the indeterminate thyroid nodules: A meta-analysis. BioMed Res. Int. 2019, 2019, 7150527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polavarapu, P.; Fingeret, A.; Yuil-Valdes, A.; Olson, D.; Patel, A.; Shivaswamy, V.; Matthias, T.D.; Goldner, W. Comparison of Afirma GEC and GSC to nodules without molecular testing in cytologically indeterminate thyroid nodules. J. Endocr. Soc. 2021, 5, bvab148. [Google Scholar] [CrossRef]
- Sciacchitano, S.; Lavra, L.; Ulivieri, A.; Magi, F.; De Francesco, G.P.; Bellotti, C.; Salehi, L.B.; Trovato, M.; Drago, C.; Bartolazzi, A. Comparative analysis of diagnostic performance, feasibility and cost of different test-methods for thyroid nodules with indeterminate cytology. Oncotarget 2017, 8, 49421–49442. [Google Scholar] [CrossRef]
- Borowczyk, M.; Szczepanek-Parulska, E.; Olejarz, M.; Więckowska, B.; Verburg, F.A.; Dębicki, S.; Budny, B.; Janicka-Jedyńska, M.; Ziemnicka, K.; Ruchała, M. Correction to: Evaluation of 167 Gene Expression Classifier (GEC) and ThyroSeq v2 diagnostic accuracy in the preoperative assessment of indeterminate thyroid nodules: Bivariate/HROC meta-analysis. Endocr. Pathol. 2019, 30, 16. [Google Scholar] [CrossRef] [Green Version]
- Vargas-Salas, S.; Martínez, J.R.; Urra, S.; Domínguez, J.M.; Mena, N.; Uslar, T.; Lagos, M.; Henríquez, M.; González, H.E. Genetic testing for indeterminate thyroid cytology: Review and meta-analysis. Endocr. Relat. Cancer 2018, 25, R163–R177. [Google Scholar] [CrossRef] [Green Version]
- Vuong, H.G.; Nguyen, T.P.X.; Hassell, L.A.; Jung, C.K. Diagnostic performances of the Afirma Gene Sequencing Classifier in comparison with the Gene Expression Classifier: A meta-analysis. Cancer Cytopathol. 2021, 129, 182–189. [Google Scholar] [CrossRef]
- Fnais, N.; Soobiah, C.; Al-Qahtani, K.; Hamid, J.S.; Perrier, L.; Straus, S.E.; Tricco, A.C. Diagnostic value of fine needle aspiration BRAFV600E mutation analysis in papillary thyroid cancer: A systematic review and meta-analysis. Hum. Pathol. 2015, 46, 1443–1454. [Google Scholar] [CrossRef] [PubMed]
- Ngo, H.T.T.; Nguyen, T.P.X.; Vu, T.H.; Jung, C.K.; Hassell, L.; Kakudo, K.; Vuong, H.G. Impact of molecular testing on the management of indeterminate thyroid nodules among western and asian countries: A systematic review and meta-analysis. Endocr. Pathol. 2021, 32, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Geng, H.; Liu, X.; Cao, M.; Zhang, X. A meta-analysis of circulating microRNAs in the diagnosis of papillary thyroid carcinoma. PLoS ONE 2021, 16, e0251676. [Google Scholar] [CrossRef] [PubMed]
- Ye, W.; Hannigan, B.; Zalles, S.; Mehrotra, M.; Barkoh, B.A.; Williams, M.D.; Cabanillas, M.E.; Edeiken-Monroe, B.; Roy-Chowdhuri, S.; Duose, D.; et al. Centrifuged supernatants from FNA provide a liquid biopsy option for clinical next-generation sequencing of thyroid nodules. Cancer Cytopathol. 2019, 127, 146–160. [Google Scholar] [CrossRef] [Green Version]
- Ablordeppey, K.K.; Timmaraju, V.A.; Song-Yang, J.W.; Yaqoob, S.; Narick, C.; Mireskandari, A.; Finkelstein, S.D.; Kumar, G. Development and analytical validation of an expanded mutation detection panel for next-generation sequencing of thyroid nodule aspirates. J. Mol. Diagn. 2020, 22, 355–367. [Google Scholar] [CrossRef] [Green Version]
- Morris, L.G.T. Molecular profiling of thyroid nodules—Are these findings meaningful, or merely measurable? A review. JAMA Otolaryngol. Head. Neck Surg. 2020, 146, 845–850. [Google Scholar] [CrossRef]
- Arosemena, M.; Thekkumkattil, A.; Valderrama, M.I.L.; Kuker, R.A.; Castillo, R.P.; Sidani, C.; Gonzalez, M.L.; Casula, S.; Kargi, A.Y. American thyroid association sonographic risk and afirma gene expression classifier alone and in combination for the diagnosis of thyroid nodules with bethesda category III cytology. Thyroid 2020, 30, 1613–1619. [Google Scholar] [CrossRef]
- Peng, S.; Liu, Y.; Lv, W.; Liu, L.; Zhou, Q.; Yang, H.; Ren, J.; Liu, G.; Wang, X.; Zhang, X.; et al. Deep learning-based artificial intelligence model to assist thyroid nodule diagnosis and management: A multicentre diagnostic study. Lancet Digit. Health 2021, 3, e250–e259. [Google Scholar] [CrossRef]
- Bini, F.; Pica, A.; Azzimonti, L.; Giusti, A.; Ruinelli, L.; Marinozzi, F.; Trimboli, P. Artificial intelligence in thyroid field—A comprehensive review. Cancers 2021, 13, 4740. [Google Scholar] [CrossRef]
- Park, V.Y.; Han, K.; Seong, Y.K.; Park, M.H.; Kim, E.-K.; Moon, H.J.; Yoon, J.H.; Kwak, J.Y. Diagnosis of thyroid nodules: Performance of a deep learning convolutional neural network model vs. radiologists. Sci. Rep. 2019, 9, 17843. [Google Scholar] [CrossRef]
- Kim, G.R.; Lee, E.; Kim, H.R.; Yoon, J.H.; Park, V.Y.; Kwak, J.Y. Convolutional neural network to stratify the malignancy risk of thyroid nodules: Diagnostic performance compared with the american college of radiology thyroid imaging reporting and data system implemented by experienced radiologists. Am. J. Neuroradiol. 2021, 42, 1513–1519. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.-G.; Lv, W.-Z.; Yin, R.; Xu, J.-W.; Yan, Y.-J.; Chen, R.-X.; Wang, J.-Y.; Zhang, B.; Cui, X.-W.; Dietrich, C.F. Deep learning based on ACR TI-RADS can improve the differential diagnosis of thyroid nodules. Front. Oncol. 2021, 11, 575166. [Google Scholar] [CrossRef] [PubMed]
- Jin, Z.; Zhu, Y.; Zhang, S.; Xie, F.; Zhang, M.; Zhang, Y.; Tian, X.; Zhang, J.; Luo, Y.; Cao, J. Ultrasound Computer-Aided Diagnosis (CAD) based on the Thyroid Imaging Reporting and Data System (TI-RADS) to distinguish benign from malignant thyroid nodules and the diagnostic performance of radiologists with different diagnostic experience. Med. Sci. Monit. 2020, 26, e918452. [Google Scholar] [CrossRef]
- Liang, X.; Yu, J.; Liao, J.; Chen, Z. Convolutional Neural network for breast and thyroid nodules diagnosis in ultrasound imaging. BioMed Res. Int. 2020, 2020, 1763803. [Google Scholar] [CrossRef]
- Buda, M.; Wildman-Tobriner, B.; Hoang, J.K.; Thayer, D.; Tessler, F.N.; Middleton, W.D.; Mazurowski, M.A. Management of thyroid nodules seen on US images: Deep learning may match performance of radiologists. Radiology 2019, 292, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Ko, S.Y.; Lee, J.H.; Yoon, J.H.; Na, H.; Hong, E.; Han, K.; Jung, I.; Kim, E.; Moon, H.J.; Park, V.Y.; et al. Deep convolutional neural network for the diagnosis of thyroid nodules on ultrasound. Head Neck 2018, 41, 885–891. [Google Scholar] [CrossRef]
- Wang, L.; Yang, S.; Yang, S.; Zhao, C.; Tian, G.; Gao, Y.; Chen, Y.; Lu, Y. Automatic thyroid nodule recognition and diagnosis in ultrasound imaging with the YOLOv2 neural network. World J. Surg. Oncol. 2019, 17, 12. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Zhang, S.; Zhang, Q.; Wei, X.; Pan, Y.; Zhao, J.; Xin, X.; Qin, C.; Wang, X.; Li, J.; et al. Diagnosis of thyroid cancer using deep convolutional neural network models applied to sonographic images: A retrospective, multicohort, diagnostic study. Lancet Oncol. 2019, 20, 193–201. [Google Scholar] [CrossRef]
- Chi, J.; Walia, E.; Babyn, P.; Wang, J.; Groot, G.; Eramian, M. Thyroid nodule classification in ultrasound images by fine-tuning deep convolutional neural network. J. Digit. Imaging 2017, 30, 477–486. [Google Scholar] [CrossRef]
- Ma, J.; Wu, F.; Zhu, J.; Xu, D.; Kong, D. A pre-trained convolutional neural network based method for thyroid nodule diagnosis. Ultrasonics 2017, 73, 221–230. [Google Scholar] [CrossRef]
- Yang, P.; Pi, Y.; He, T.; Sun, J.; Wei, J.; Xiang, Y.; Jiang, L.; Li, L.; Yi, Z.; Zhao, Z.; et al. Automatic differentiation of thyroid scintigram by deep convolutional neural network: A dual center study. BMC Med. Imaging 2021, 21, 179. [Google Scholar] [CrossRef] [PubMed]





| Authors (Publication Year) | Number of Studies | Number of Patients | Pooled Prevalence (95%CI) | Pooled Risk of Malignancy (95%CI) |
|---|---|---|---|---|
| Shie et al. (2009) [23] | 18 | 55,160 | 1% | 33.2% |
| Soelberg et al. (2012) [24] | 22 | 125,754 | 1.6% | 34.8% |
| Bertagna et al. (2012) [25] | 27 | 147,505 | 2.46% (1.68–3.39) | 34.6% (29.3–40.2) |
| Treglia et al. (2013) [26] | 34 | 215,057 | 1.92% (1.87–1.99) | 36.2% (33.8–38.6) |
| Qu et al. (2014) [27] | 29 | 196,298 | 2.9% | NR |
| Nayan et al. (2014) [28] | 31 | 197,296 | 1.9% | 20% (15.3–25) |
| de Leijer JF et al.(2021) [29] | 61 | 660,037 | 2.22% | 12.6% |
| Scappaticcio L et al. (2021) [30] | 15 | 2304 | NR | 19% (13–25) |
| Authors (Publication Year) | Number of Studies | Number of Patients | Prevalence of Malignancy | Sensitivity (95%CI) | Specificity (95%CI) | NPV (95%CI) | PPV (95%CI) |
|---|---|---|---|---|---|---|---|
| Wang et al. (2013) [31] | 7 | 267 | 26.2% (19.6–40) | 89% (79–95) | 55% (48–62) | NR | [1]NR |
| Vriens et al. (2014) [32] | 6 | 225 | 25.8% (13.6–41.7) | 95% (86–99) | 48% (40–56) | 96% (90–99) | 39% (31–47) |
| Castellana M. et al. (2019) [33] | 8 | 431 | NR | 74% (58–84) | 58% (48–67) | 74% (41–100) | 34% (25–44) |
| Qichang et al. (2019) [34] | 13 | 634 | 24% (4–50) | 63% | 65% | 55% | 44% |
| Authors (Publication Year) | Number of Studies | Number of Patients | Sensitivity (95%CI) | Specificity (95%CI) |
|---|---|---|---|---|
| Dong et al. (2009) [35] | 6 | 165 | 93% (87–97) | 84% (72–92) |
| Miller et al. (2011) * [36] | 11 | 498 | 82% (69–94) | 84% (77–92) |
| Caetano et al. (2016) [37] | 7 | 260 | 93% (84–97) | 81% (69–90) |
| Haslerud et al. (2016) [38] | 17 | 905 | 80% (73–86) | 75% (63–85) |
| Schütz et al. (2018) [39] | 11 | NR | 94% (87–98) | 78% (52–92) |
| Kim et al. (2018) [40] | 9 | 515 | 84% (77–89) | 78% (67–86) |
| Qichang et al. (2019) [41] | 17 | 1195 | 86% | 84% |
| Afirma Gene Sequencing Classifier (GSC) [85] | ThyroSeq v3 [86] | RosettaGX Reveal [87] | ThyraMir [88] | |
|---|---|---|---|---|
| Sensitivity | 91% | 94% | 74% | 89% |
| Specificity | 68% | 82% | 74% | 85% |
| Negative predictive value | 96% | 97% | 94% | 92% |
| Positive predictive value | 47% | 66% | 43% | 74% |
| Author/Year | No. of Studies | No. of Thyroid Nodules | Sensitivity | Specificity | Negative Predictive Value | Positive Predictive Value | |
|---|---|---|---|---|---|---|---|
| Afirma Gene Expression Classifier (GEC) | Sciacchitano et al. 2017 [91] | 2 | 210 | 90% | 52% | 94% | 37% |
| Borowczyk et al. 2018 [92] | 16 | 1086 | 98% | 12% | 91% | 45% | |
| Vargas-Salas et al. 2018 [93] | 19 | 1371 | 92% | 27% | 91% | 30% | |
| Liu et al. 2019 [89] | 18 | 3290 | 95.5% | 22.1% | 88.2% | 44.3% | |
| Vuong et al. 2020 [94] | 7 | 1947 | 93.6% | 25.1% | 86.1% | 41.6% | |
| Silaghi et al. 2021 [83] | 25 | 4538 | 97% | 19% | 91% | 39% | |
| Afirma Gene Sequencing Classifier (GSC) | Vuong et al. 2020 [94] | 7 | 807 | 94.3% | 43% | 90% | 63.1% |
| Silaghi et al. 2021 [83] | 4 | 635 | 95% | 51% | 91% | 60% | |
| ThyroSeq v2 | Borowczyk et al. 2018 [92] | 5 | 459 | 84% | 78% | 93% | 58% |
| Vargas-Salas et al. 2018 [93] | 5 | 350 | 86% | 79% | 94% | 58% | |
| Sciacchitano et al. 2017 [91] | 9 | 143 | 90% | 93% | 96% | 83% | |
| Silaghi et al. 2021 [83] | 9 | 1549 | 86% | 75% | 95% | 51% | |
| ThyroSeq v3 | Silaghi et al. 2021 [83] | 4 | 603 | 99% | 64% | 96% | 78% |
| ThyGenX | Sciacchitano et al. 2017 [91] | 8 | 1141 | 51% | 93% | 86% | 70% |
| Vargas-Salas et al. 2018 [93] | 1 | 109 | 89% | 85% | 96% | 66% | |
| Silaghi et al. 2021 [83] | 3 | 141 | 94.3% | 61.4% | N/A | N/A | |
| RosettaGX Reveal | Vargas-Salas et al. 2018 [93] | 1 | 150 | 74% | 74% | 90% | 49 |
| Silaghi et al. 2021 [83] | 3 | 234 | 85.2–100% | 69.2–85.7% | N/A | N/A | |
| ThyraMir | Sciacchitano et al. 2017 [91] | 2 | 109 | 89% | 85% | 94% | 74% |
| Silaghi et al. 2021 [83] | 1 | 105 | 50% | 91.9% | N/A | N/A | |
| BRAF V600E | Sciacchitano et al. 2017 [91] | 24 | 2625 | 41% | 100% | 68% | 99% |
| Fnais et al. 2015 [95] | 9 | 262 | 52% | 100% | N/A | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teodoriu, L.; Leustean, L.; Ungureanu, M.-C.; Bilha, S.; Grierosu, I.; Matei, M.; Preda, C.; Stefanescu, C. Personalized Diagnosis in Differentiated Thyroid Cancers by Molecular and Functional Imaging Biomarkers: Present and Future. Diagnostics 2022, 12, 944. https://doi.org/10.3390/diagnostics12040944
Teodoriu L, Leustean L, Ungureanu M-C, Bilha S, Grierosu I, Matei M, Preda C, Stefanescu C. Personalized Diagnosis in Differentiated Thyroid Cancers by Molecular and Functional Imaging Biomarkers: Present and Future. Diagnostics. 2022; 12(4):944. https://doi.org/10.3390/diagnostics12040944
Chicago/Turabian StyleTeodoriu, Laura, Letitia Leustean, Maria-Christina Ungureanu, Stefana Bilha, Irena Grierosu, Mioara Matei, Cristina Preda, and Cipriana Stefanescu. 2022. "Personalized Diagnosis in Differentiated Thyroid Cancers by Molecular and Functional Imaging Biomarkers: Present and Future" Diagnostics 12, no. 4: 944. https://doi.org/10.3390/diagnostics12040944