
Thyroid Cancer Diagnostics Related to Occupational and Environmental Risk Factors: An Integrated Risk Assessment Approach

 ,
,
Abstract
:1. Introduction
2. Etiology and Pathogenesis Mechanisms
3. Thyroid Cancer Diagnostics: General Approach
3.1. Ultrasonography Diagnosis (US) and Risk Stratification Systems
3.2. US-Guided Fine Needle Aspiration (FNA)
4. Thyroid Cancer Diagnostics: Biomarkers and Methodology
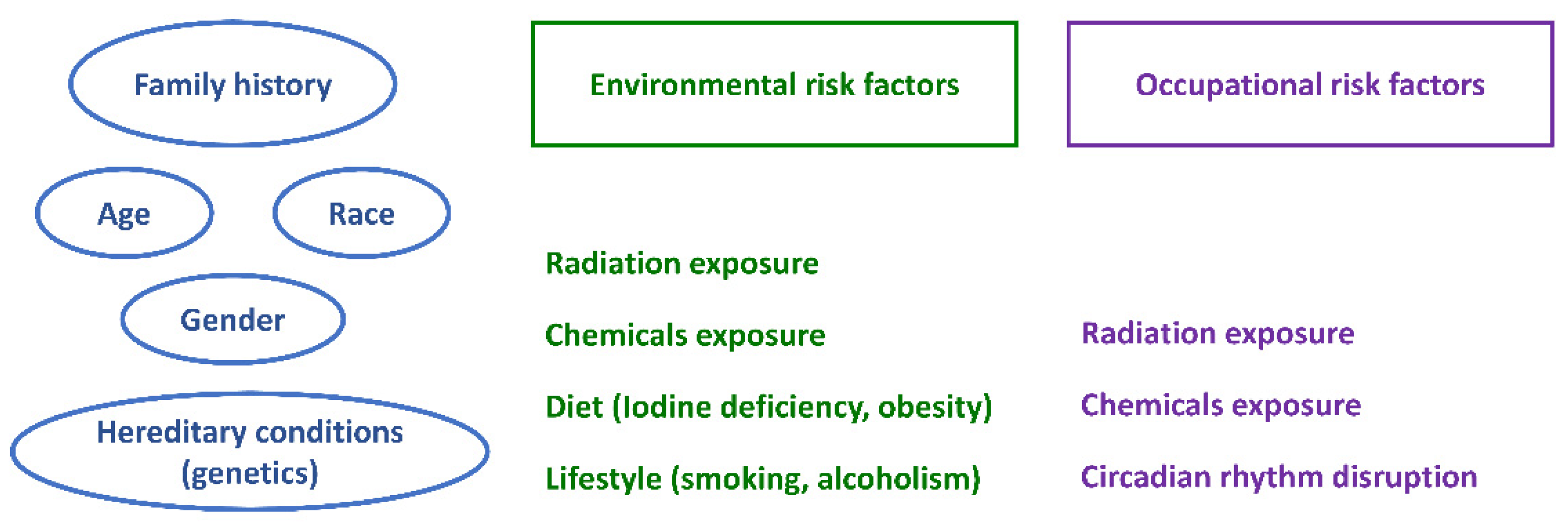
5. Risk Factors Involved in the Pathogenesis of Thyroid Cancer
5.1. Occupational Risk Factors
5.2. Environmental Risk Factors
6. Risk Factors and Risk Assessments: An Integrative Approach
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aschebrook-Kilfoy, B.; Ward, M.H.; Della Valle, C.T.; Friesen, M.C. Occupation, and thyroid cancer. Occup. Environ. Med. 2014, 71, 366–380. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Tamhane, S.; Gharib, H. Thyroid nodule update on diagnosis and management. Clin. Diabetes Endocrinol. 2016, 2, 17–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gharib, H.; Papini, E. Thyroid nodules: Clinical importance, assessment, and treatment. Endocrinol. Metab. Clin. N. Am. 2007, 36, 707–735. [Google Scholar] [CrossRef]
- Granja, F.; Morari, J.; Morari, E.C.; Correa, L.A.C.; Assumpção, L.V.M.; Ward, L.S. Proline homozygosity in codon 72 of p53 is a factor of susceptibility for thyroid cancer. Cancer Lett. 2004, 210, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Arena, A.; Stigliano, A.; Belcastro, E.; Giorda, E.; Rosado, M.M.; Grossi, A.; Assenza, M.R.; Moretti, F.; Fierabracci, A. p53 Activation Effect in the Balance of T Regulatory and Effector Cell Subsets in Patients with Thyroid Cancer and Autoimmunity. Front. Immunol. 2021, 12, 3452. [Google Scholar] [CrossRef]
- Khan, M.S.; Pandith, A.A.; Azad, N.; Hussain, M.; Masoodi, S.R.; Wani, K.A.; Andrabi, K.I.; Mudassar, S. Impact of molecular alterations of BRAF in the pathogenesis of thyroid cancer. Mutagenesis 2014, 29, 131–137. [Google Scholar] [CrossRef] [Green Version]
- Zhao, L.; Wang, L.; Jia, X.; Hu, X.; Pang, P.; Zhao, S.; Wang, Y.; Wang, J.; Zhang, Y.; Lyu, Z. The Coexistence of Genetic Mutations in Thyroid Carcinoma Predicts Histopathological Factors Associated with a Poor Prognosis: A Systematic Review and Network Meta-Analysis. Front. Oncol. 2020, 10, 2316. [Google Scholar] [CrossRef]
- Bonaldi, E.; Gargiuli, C.; De Cecco, L.; Micali, A.; Rizzetti, M.G.; Greco, A.; Borrello, M.G.; Minna, E. BRAF Inhibitors Induce Feedback Activation of RAS Pathway in Thyroid Cancer Cells. Int. J. Mol. Sci. 2021, 22, 5744. [Google Scholar] [CrossRef]
- Guilhen, A.C.T.; Bufalo, N.E.; Morari, E.C.; Leite, J.L.; Assumpcao, L.V.M.; Tincani, A.J.A.; Ward, L.S. Role of the N-Acetyltransferase 2 Detoxification System in Thyroid Cancer Susceptibility. Clin. Cancer Res. 2009, 15, 406–412. [Google Scholar] [CrossRef] [Green Version]
- Bufalo, N.E.; Leite, J.L.; Guilhen, A.C.T.; Morari, E.C.; Granja, F.; Assumpcao, L.V.M.; Ward, L.S. Smoking and susceptibility to thyroid cancer: An inverse association with CYP1A1 allelic variants. Endocr. Relat. Cancer 2006, 13, 1185–1193. [Google Scholar] [CrossRef] [PubMed]
- Baldini, E.; Odorisio, T.; Tuccilli, C.; Persechino, S.; Sorrenti, S.; Catania, A.; Pironi, D.; Carbotta, G.; Giacomelli, L.; Arcieri, S.; et al. Thyroid diseases and skin autoimmunity. Rev. Endocr. Metab. Disord. 2018, 19, 311–323. [Google Scholar] [CrossRef] [PubMed]
- Marqusee, E.; Benson, C.B.; Frates, M.C.; Doubilet, P.M.; Larsen, P.R.; Cibas, E.S.; Mandel, S.J. Usefulness of ultrasonography in the management of nodular thyroid disease. Ann. Intern. Med. 2000, 133, 696–700. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [Green Version]
- Bonjoc, K.J.; Young, H.; Warner, S.; Gernon, T.; Maghami, E.; Chaudhry, A. Thyroid cancer diagnosis in the era of precision imaging. J. Thorac. Dis. 2020, 12, 5128–5139. [Google Scholar] [CrossRef]
- Hagag, P.; Strauss, S.; Weiss, M. Role of ultrasound-guided fine-needle aspiration biopsy in evaluation of nonpalpable thyroid nodules. Thyroid 1998, 8, 989–995. [Google Scholar] [CrossRef]
- Remonti, L.R.; Kramer, C.K.; Leitão, C.B.; Pinto, L.C.F.; Gross, J.L. Thyroid ultrasound features and risk of carcinoma: A systematic review and meta-analysis of observational studies. Thyroid 2015, 25, 538–550. [Google Scholar] [CrossRef] [Green Version]
- Middleton, W.D.; Teefey, S.A.; Reading, C.C.; Langer, J.E.; Beland, M.D.; Szabunio, M.M.; Desser, T.S. Multiinstitutional Analysis of Thyroid Nodule Risk Stratification Using the American College of Radiology Thyroid Imaging Reporting and Data System. Am. J. Roentgenol. 2017, 208, 1331–1341. [Google Scholar] [CrossRef]
- Russ, G.; Bonnema, S.J.; Erdogan, M.F.; Durante, C.; Ngu, R.; Leenhardt, L. European Thyroid Association Guidelines for Ultrasound Malignancy Risk Stratification of Thyroid Nodules in Adults: The EU-TIRADS. Eur. Thyroid J. 2017, 6, 225–237. [Google Scholar] [CrossRef] [Green Version]
- Shin, J.H.; Baek, J.H.; Chung, J.; Ha, E.J.; Kim, J.H.; Lee, Y.H.; Lim, H.K.; Moon, W.J.; Na, D.G.; Park, J.S.; et al. Ultrasonography diagnosis and imaging-based management of thyroid nodules: Revised Korean Society of Thyroid Radiology Consensus Statement and Recommendations. Korean J. Radiol. 2016, 17, 370–395. [Google Scholar] [CrossRef] [Green Version]
- Moon, H.J.; Kwak, J.Y.; Kim, M.J.; Son, E.J.; Kim, E.K. Can vascularity at power Doppler US help predict thyroid malignancy? Radiology 2010, 255, 260–269. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Ma, X.; Wu, N.; Liu, L.; Liu, X.; Zhang, J.; Yang, J.; Niu, T. Shear wave elastography for differentiation of benign and malignant thyroid nodules: A meta-analysis. J. Ultrasound Med. 2013, 32, 2163–2169. [Google Scholar] [CrossRef] [PubMed]
- Cibas, E.S.; Ali, S.Z. The 2017 Bethesda System for Reporting Thyroid Cytopathology. Thyroid 2017, 27, 1341–1346. [Google Scholar] [CrossRef] [PubMed]
- Bongiovanni, M.; Spitale, A.; Faquin, W.C.; Mazzucchelli, L.; Baloch, Z.W. The Bethesda System for Reporting Thyroid Cytopathology: A meta-analysis. Acta Cytol. 2012, 56, 333–339. [Google Scholar] [CrossRef]
- Wu, Y.; Xu, T.; Cao, X.; Zhao, X.; Deng, H.; Wang, J.; Li, X.; Yao, Q.; Ye, X.; Shen, M.; et al. BRAF (V600E) vs. TIRADS in predicting papillary thyroid cancers in Bethesda system I, III, and V nodules. Cancer Biol. Med. 2019, 16, 131–138. [Google Scholar] [CrossRef] [Green Version]
- Koh, J.; Kim, E.K.; Kwak, J.Y.; Yoon, J.H.; Moon, H.J. Repeat fine-needle aspiration can be performed at 6 months or more after initial atypia of undetermined significance or follicular lesion of undetermined significance results for thyroid nodules 10 mm or larger. Eur. Radiol. 2016, 26, 4442–4448. [Google Scholar] [CrossRef]
- Jung, C.K.; Baek, J.H.; Na, D.G.; Oh, Y.L.; Yi, K.H.; Kang, H.C. 2019 Practice guidelines for thyroid core needle biopsy: A report of the Clinical Practice Guidelines Development Committee of the Korean Thyroid Association. J. Pathol. Transl. Med. 2020, 54, 64–86. [Google Scholar] [CrossRef] [Green Version]
- Filetti, S.; Durante, C.; Hart, D.; Leboulleux, S.; Locati, L.D.; Newbold, K.; Papotti, M.G.; Berruti, A.; ESMO Guidelines Committee Cancer. Thyroid cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment, and follow-up. Ann. Oncol. 2019, 30, 1856–1883. [Google Scholar] [CrossRef] [Green Version]
- Coelho, M.; Raposo, L.; Goodfellow, B.J.; Atzori, L.; Jones, J.; Manadas, B. The Potential of Metabolomics in the Diagnosis of Thyroid Cancer. Int. J. Mol. Sci. 2020, 21, 5272. [Google Scholar] [CrossRef]
- Kunavisarut, T. Diagnostic biomarkers of differentiated thyroid cancer. Endocrine 2013, 44, 616–622. [Google Scholar] [CrossRef]
- Hussein, O.; Abdelwahab, K.; Hamdy, O.; Awny, S.; Megahed, N.A.; Hafez, M.T.; Elalfi, A.F.; Abdelaziz, M.; Gaballah, K.; Abdelkhalek, M. Thyroid cancer associated with Hashimoto thyroiditis: Similarities and differences in an endemic area. J. Egypt. Natl. Cancer Inst. 2020, 32, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, S.; Qiu, L.; Wang, Y.; Qin, X.; Liu, H.; He, M.; Zhang, Y.; Li, Z.; Chen, X. Tissue imaging and serum lipidomic profiling for screening potential biomarkers of thyroid tumors by matrix-assisted laser desorption/ionization-Fourier transform ion cyclotron resonance mass spectrometry. Anal. Bioanal. Chem. 2014, 406, 4357–4370. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Song, J.; Koh, T.; Park, O.; Park, J.T.; Lee, W.J. Thyroid cancer among female workers in Korea, 2007–2015. Ann. Occup. Environ. Med. 2018, 30, 48. [Google Scholar] [CrossRef] [PubMed]
- Wojakowska, A.; Chekan, M.; Widlak, P.; Pietrowska, M. Application of Metabolomics in Thyroid Cancer Research. Int. J. Endocrinol. 2015, 2015, 258763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrokhi Yekta, R.; Rezaie Tavirani, M.; Arefi Oskouie, A.; Mohajeri Tehrani, M.R.; Soroush, A.R. The metabolomics and lipidomics window into thyroid cancer research. Biomarkers 2017, 22, 595–603. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, D.R. Metabolomics in Cancer Research and Emerging Applications in Clinical Oncology. CA Cancer J. Clin. 2021, 71, 333–358. [Google Scholar] [CrossRef] [PubMed]
- Abooshahab, R.; Gholami, M.; Sanoie, M.; Azizi, F.; Hedayati, M. Advances in metabolomics of thyroid cancer diagnosis and metabolic regulation. Endocrine 2019, 65, 1–14. [Google Scholar] [CrossRef]
- Du, Y.; Fan, P.; Jiang, Y.; Gu, X.; Yu, J.; Zhang, C. Serum Metabolomics Study of Papillary Thyroid Carcinoma Based on HPLC-Q-TOF-MS/MS. Front. Cell Dev. Biol. 2021, 9, art593510. [Google Scholar] [CrossRef]
- Ishikawa, S.; Tateya, I.; Hayasaka, T.; Masaki, N.; Takizawa, Y.; Ohno, S.; Kojima, T.; Kitani, Y.; Kitamura, M.; Hirano, S.; et al. Increased expression of phosphatidylcholine (16:0/18:1) and (16:0/18:2) in thyroid papillary cancer. PLoS ONE 2012, 7, e48873. [Google Scholar] [CrossRef] [Green Version]
- Peng, S.; Liu, Y.; Lv, W.; Liu, L.; Zhou, Q.; Yang, H.; Ren, J.; Liu, G.; Wang, X.; Zhang, X.; et al. Deep learning-based artificial intelligence model to assist thyroid nodule diagnosis and management: A multicentre diagnostic study. Lancet Digit. Health 2021, 3, e250–e259. [Google Scholar] [CrossRef]
- Nabhan, F.; Dedhia, P.H.; Ringel, M.D. Thyroid Cancer, Recent Advances in Diagnosis and Therapy. Int. J. Cancer 2021, 149, 984–992. [Google Scholar] [CrossRef] [PubMed]
- Rinschen, M.M.; Ivanisevic, J.; Giera, M.; Siuzdak, G. Identification of bioactive metabolites using activity metabolomics. Nat. Rev. Mol. Cell Biol. 2019, 20, 353–367. [Google Scholar] [CrossRef] [PubMed]
- Khatami, F.; Payab, M.; Sarvari, M.; Gilany, K.; Larijani, B.; Arjmand, B.; Tavangar, S.M. Oncometabolites as biomarkers in thyroid cancer: A systematic review. Cancer Manag. Res. 2019, 11, 1829–1841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rovcanin, B.; Stojsavljevic, A.; Kekic, D.; Gopcevic, K.; Manojlovic, D.; Jovanovic, M.; Knezevic, S.; Zivaljevic, V.; Diklic, A.; Paunovic, I. Redox Status and Antioxidative Cofactor Metals Influence Clinical and Pathological Characteristics of Papillary Thyroid Carcinoma and Colloid Goiter. Biol. Trace Elem. Res. 2020, 197, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Hińcza, K.; Kowalik, A.; Kowalska, A. Current Knowledge of Germline Genetic Risk Factors for the Development of Non-Medullary Thyroid Cancer. Genes 2019, 10, 482. [Google Scholar] [CrossRef] [Green Version]
- Malaguarnera, R.; Ledda, C.; Filippello, A.; Frasca, F.; Francavilla, V.C.; Ramaci, T.; Parisi, M.C.; Rapisarda, V.; Piro, S. Thyroid cancer and Circadian Clock Disruption. Cancers 2020, 12, 3109. [Google Scholar] [CrossRef]
- Diamanti-Kandarakis, E.; Bourguignon, J.P.; Giudice, L.C.; Hauser, R.; Prins, G.S.; Soto, A.M.; Zoeller, R.T.; Gore, A.C. Endocrine-disrupting chemicals: An Endocrine Society scientific statement. Endocr. Rev. 2009, 30, 293–342. [Google Scholar] [CrossRef]
- Andrianou, X.D.; Gängler, S.; Piciu, A.; Charisiadis, P.; Zira, C.; Aristidou, K.; Piciu, D.; Hauser, R.; Makris, K.C. Human Exposures to Bisphenol A, Bisphenol F and Chlorinated Bisphenol A Derivatives and Thyroid Function. PLoS ONE 2016, 11, e0155237. [Google Scholar] [CrossRef]
- Deveau, M.; Chen, C.P.; Johanson, G.; Krewski, D.; Maier, A.; Niven, K.J.; Ripple, S.; Schulte, P.A.; Silk, J.; Urbanus, J.H.; et al. The Global Landscape of Occupational Exposure Limits--Implementation of Harmonization Principles to Guide Limit Selection. J. Occup. Environ. Hyg. 2015, 12 (Suppl. 1), S127–S144. [Google Scholar] [CrossRef] [Green Version]
- Manisalidis, I.; Stavropoulou, E.; Stavropoulos, A.; Bezirtzoglou, E. Environmental and Health Impacts of Air Pollution: A Review. Front. Public Health 2020, 8, 14. [Google Scholar] [CrossRef] [Green Version]
- Vermeulen, R.; Schymanski, E.L.; Barabási, A.L.; Miller, G.W. The exposome and health: Where chemistry meets biology. Science 2020, 367, 392–396. [Google Scholar] [CrossRef] [PubMed]
- Leso, V.; Vetrani, I.; De Cicco, L.; Cardelia, A.; Fontana, L.; Buonocore, G.; Iavicoli, I. The Impact of Thyroid Diseases on the Working Life of Patients: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4295. [Google Scholar] [CrossRef] [PubMed]
- Lentz, T.J.; Dotson, G.S.; Williams, P.R.; Maier, A.; Gadagbui, B.; Pandalai, S.P.; Lamba, A.; Hearl, F.; Mumtaz, M. Aggregate Exposure and Cumulative Risk Assessment--Integrating Occupational and Non-occupational Risk Factors. J. Occup. Environ. Hyg. 2015, 12, S112–S126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ba, Y.; Huang, H.; Lerro, C.C.; Li, S.; Zhao, N.; Li, A.; Ma, S.; Udelsman, R.; Zhang, Y. Occupation and Thyroid Cancer. J. Occup. Environ. Med. 2016, 58, 299–305. [Google Scholar] [CrossRef] [Green Version]
- Coppeta, L.; Di Giampaolo, L.; Rizza, S.; Balbi, O.; Baldi, S.; Pietroiusti, A.; Magrini, A. Relationship between the night shift work and thyroid disorders: A systematic review and meta-analysis. Endocr. Regul. 2020, 54, 64–70. [Google Scholar] [CrossRef] [Green Version]
- Khodamoradi, F.; Ghoncheh, M.; Mehri, A.; Hassanipour, S.; Salehiniya, H. Incidence, Mortality, and Risk Factors of Thyroid Cancer In The World: A Review. World Cancer Res. J. 2018, 5, e1093. [Google Scholar]
- Kim, K.H.; Woo, S.H. An Occupational Study in Nurses: Prevalence of Thyroid Nodules and Cancer in Comparison to Health Check-up Female. Clin. Exp. Otorhinolaryngol. 2016, 9, 252–256. [Google Scholar] [CrossRef]
- Zabel, E.W.; Alexander, B.H.; Mongin, S.J.; Doody, M.M.; Sigurdson, A.J.; Linet, M.S.; Freedman, D.M.; Hauptmann, M.; Mabuchi, K.; Ron, E. Thyroid cancer and employment as a radiologic technologist. Int. J. Cancer 2006, 119, 1940–1945. [Google Scholar] [CrossRef]
- Shi, F.; Liu, Y.; Li, M.; Wen, P.; Qian, Q.Q.; Fan, Y.; Huang, R. Analysis of lncRNA and mRNA Transcriptomes Expression in Thyroid Cancer Tissues Among Patients with Exposure of Medical Occupational Radiation. Dose-Response 2019, 17, 1–11. [Google Scholar] [CrossRef]
- Kitahara, C.M.; Preston, D.L.; Neta, G.; Little, M.P.; Doody, M.M.; Simon, S.L.; Sigurdson, A.J.; Alexander, B.H.; Linet, M.S. Occupational radiation exposure and thyroid cancer incidence in a cohort of US radiologic technologists, 1983–2013. Int. J. Cancer 2018, 143, 2145–2149. [Google Scholar] [CrossRef]
- Lee, W.J.; Preston, D.L.; Cha, E.S.; Ko, S.; Lim, H. Thyroid cancer risks among medical radiation workers in South Korea, 1996–2015. Environ. Health 2019, 18, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lope, V.; Pollán, M.; Gustavsson, P.; Plato, N.; Pérez-Gómez, B.; Aragonés, N.; Suárez, B.; Carrasco, J.M.; Rodríguez, S.; Ramis, R.; et al. Occupation and Thyroid Cancer Risk in Sweden. J. Occup. Environ. Med. 2005, 47, 948–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alsen, M.; Sinclair, C.; Cooke, P.; Ziadkhanpour, K.; Genden, E.; van Gerwen, M. Endocrine Disrupting Chemicals and Thyroid Cancer: An Overview. Toxics 2021, 9, 14. [Google Scholar] [CrossRef] [PubMed]
- Fiore, M.; Conti, G.A.; Caltabiano, R.; Buffone, A.; Zuccarello, P.; Cormaci, L.; Cannizzaro, M.A.; Ferrante, M. Role of Emerging Environmental Risk Factors in Thyroid Cancer: A Brief Review. Int. J. Environ. Res. Public Health 2019, 16, 1185. [Google Scholar] [CrossRef] [Green Version]
- Paquet, M.; Shivappa, N.; Hébert, J.R.; Baron-Dubourdieu, D.; Boutron-Ruault, M.-C.; Guénel, P.; Truong, T. Dietary Inflammatory Index and Differentiated Thyroid Carcinoma Risk: A Population-Based Case-Control Study in New Caledonia. Am. J. Epidemiol. 2020, 189, 95–107. [Google Scholar] [CrossRef]
- Kieliszek, M.; Lipinski, B. Pathophysiological significance of protein hydrophobic interac-tions: An emerging hypothesis. Med. Hypotheses 2018, 110, 15–22. [Google Scholar] [CrossRef]
- Correia, M.M.; Chammas, M.C.; Zavariz, J.D.; Arata, A.; Martins, L.C.; Marui, S.; Pereira, L.A. Evaluation of the effects of chronic occupational exposure to metallic mercury on the thyroid parenchyma and hormonal function. Int. Arch. Occup. Environ. Health 2020, 93, 491–502. [Google Scholar] [CrossRef]
- Liu, B.; Chen, Y.; Li, S.; Xu, Y.; Wang, Y. Relationship between urinary metabolites of polycyclic aromatic hydrocarbons and risk of papillary thyroid carcinoma and nodular goiter: A case-control study in non-occupational populations. Environ. Pollut. 2021, 269, 116–158. [Google Scholar] [CrossRef]
- Iribarren, C.; Haselkorn, T.; Tekawa, I.S.; Friedman, G.D. Cohort study of Thyroid Cancer in a San Francisco Bay area population. Int. J. Cancer 2001, 93, 745–750. [Google Scholar] [CrossRef]
- Colbeth, H.L.; Genere, N.; Hall, C.B.; Jaber, N.; Brito, J.P.; El Kawkgi, O.M.; Goldfarb, D.G.; Webber, M.P.; Schwartz, T.M.; Prezant, D.J.; et al. Evaluation of Medical Surveillance and Incidence of Post-September 11, 2001, Thyroid Cancer in World Trade Center–Exposed Firefighters and Emergency Medical Service Workers. JAMA Intern. Med. 2020, 180, 888–895. [Google Scholar] [CrossRef]
- Tuminello, S.; Van Gerwen, M.A.G.; Genden, E.; Crane, M.; Lieberman-Cribbin, W.; Taioli, E. Increased Incidence of Thyroid Cancer among World Trade Center First Responders: A Descriptive Epidemiological Assessment. Int. J. Environ. Res. Public Health 2019, 16, 1258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagano, L.; Caputo, M.; Samà, M.T.; Garbaccio, V.; Zavattaro, M.; Mauri, M.G.; Prodam, F.; Marzullo, P.; Boldorini, R.; Valente, G.; et al. Clinical–pathological changes in differentiated thyroid cancer (DTC) over time (1997–2010): Data from the University Hospital “Maggiore della Carità” in Novara. Endocrine 2012, 42, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Akslen, L.; Nilssen, S.; Kvåle, G. Reproductive factors and risk of thyroid cancer. A prospective study of 63,090 women from Norway. Br. J. Cancer 1992, 65, 772–774. [Google Scholar] [CrossRef] [PubMed]
- Myung, S.K.; Lee, C.W.; Lee, J.; Kim, J.; Kim, H.S. Risk Factors for Thyroid Cancer: A Hospital-Based Case-Control Study in Korean Adults. Cancer Res. Treat. 2017, 49, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Huang, M.; Wang, L.; Ye, W.; Tong, Y.; Wang, H. Obesity and Risk of Thyroid Cancer: Evidence from a Meta-Analysis of 21 Observational Studies. Med. Sci. Monit. 2015, 21, 283–291. [Google Scholar]
- Harrison, J.; Dawson, L. Occupational Health: Meeting the Challenges of the Next 20 Years. Saf. Health Work 2016, 7, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Loomis, D.; Guha, N.; Hall, A.L.; Straif, K. Identifying occupational carcinogens: An update from the IARC Monographs. Occup. Environ. Med. 2018, 75, 593–603. [Google Scholar] [CrossRef] [Green Version]
- Juarez, P.D.; Matthews-Juarez, P.; Hood, D.B.; Im, W.; Levine, R.S.; Kilbourne, B.J.; Langston, M.A.; Al-Hamdan, M.Z.; Crosson, W.L.; Estes, M.G.; et al. The public health exposome: A population-based, exposure science approach to health disparities research. Int. J. Environ. Res. Public Health 2014, 11, 12866–12895. [Google Scholar] [CrossRef]
- Cui, Y.; Balshaw, D.M.; Kwok, R.K.; Thompson, C.L.; Collman, G.W.; Birnbaum, L.S. The Exposome: Embracing the Complexity for Discovery in Environmental Health. Environ. Health Perspect. 2016, 124, A137–A140. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| TI-RADS Category | Meaning | Risk of Malignancy | Size Threshold for FNA (cm) | Size Threshold for Follow-Up (cm) |
|---|---|---|---|---|
| TR 1 | Benign (ACR) No nodule (EU, K) | - | No FNA | No follow-up |
| TR 2 | Not suspicious (ACR) Benign (EU, K) | <2% (ACR) 0% (EU) <3% (K) | No FNA | No follow-up |
| TR 3 | Mildly suspicious (ACR) Low risk (EU, K) | 2–5% (ACR) 2–4% (EU) 3–15% (K) | >2.5 (ACR) >2 (EU) >1.5 (K) | >1.5 (ACR) >1 (EU) |
| TR 4 | Moderately suspicious (ACR) Intermediate risk (EU, K) | 5–20% (ACR) 6–17% (EU) 15–50% (K) | >1.5 (ACR) >1.5 (EU) >1 (K) | >1 (ACR) >0.5 (EU) |
| TR 5 | Highly suspicious (ACR) High risk (EU, K) | >20% (ACR) 26–87% (EU) >60% (K) | >1 (ACR) >1 (EU) >1 (K) | >0.5 (ACR) All (EU) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berinde, G.M.; Socaciu, A.I.; Socaciu, M.A.; Cozma, A.; Rajnoveanu, A.G.; Petre, G.E.; Piciu, D. Thyroid Cancer Diagnostics Related to Occupational and Environmental Risk Factors: An Integrated Risk Assessment Approach. Diagnostics 2022, 12, 318. https://doi.org/10.3390/diagnostics12020318
Berinde GM, Socaciu AI, Socaciu MA, Cozma A, Rajnoveanu AG, Petre GE, Piciu D. Thyroid Cancer Diagnostics Related to Occupational and Environmental Risk Factors: An Integrated Risk Assessment Approach. Diagnostics. 2022; 12(2):318. https://doi.org/10.3390/diagnostics12020318
Chicago/Turabian StyleBerinde, Gabriela Maria, Andreea Iulia Socaciu, Mihai Adrian Socaciu, Andreea Cozma, Armand Gabriel Rajnoveanu, Gabriel Emil Petre, and Doina Piciu. 2022. "Thyroid Cancer Diagnostics Related to Occupational and Environmental Risk Factors: An Integrated Risk Assessment Approach" Diagnostics 12, no. 2: 318. https://doi.org/10.3390/diagnostics12020318