
Radiomics of Biliary Tumors: A Systematic Review of Current Evidence

 , , , , and
, , , , and
Abstract
:1. Introduction
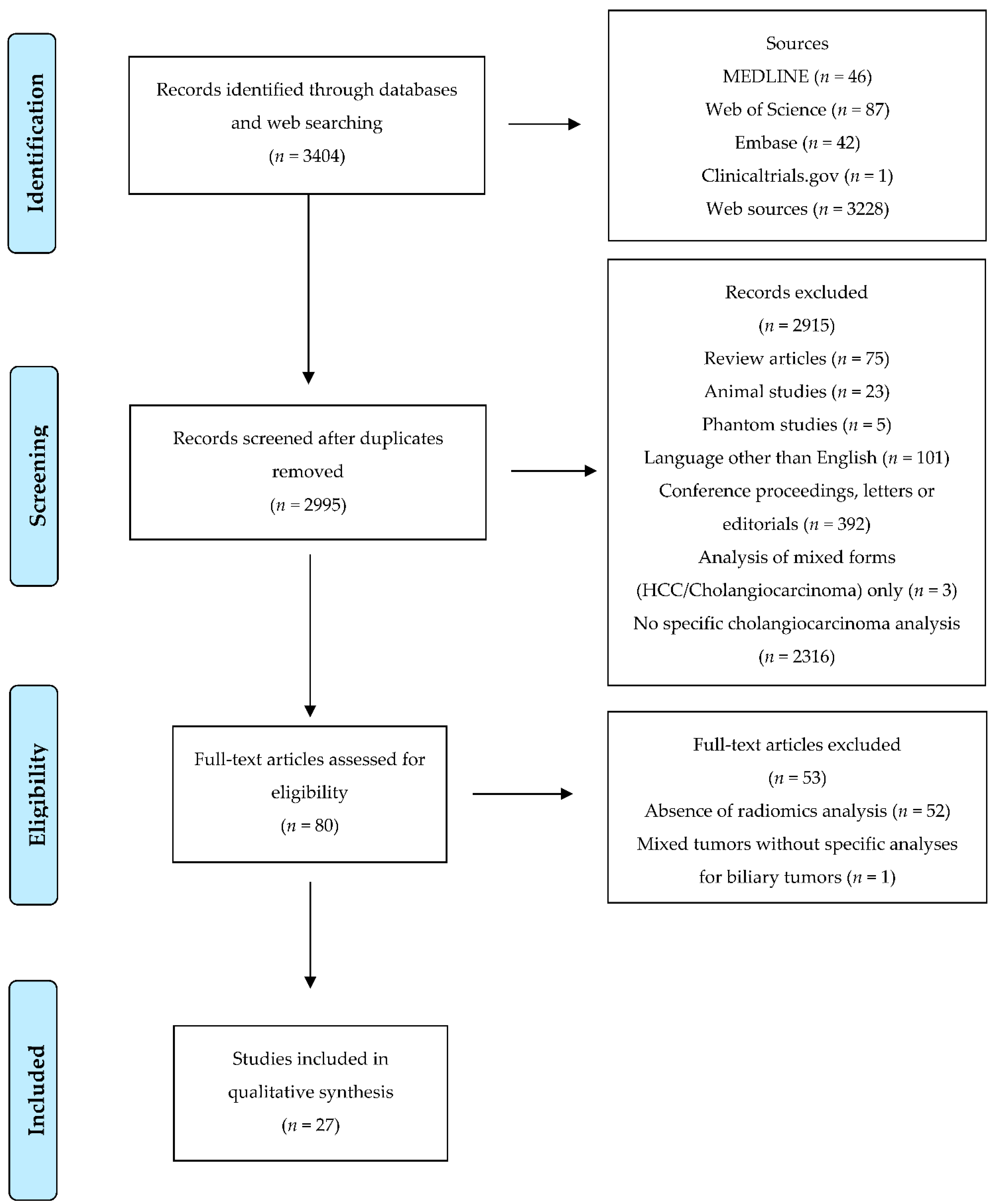
2. Materials and Methods
2.1. Quality Assessment
2.2. Data Collection
3. Results
3.1. Prediction of Pathology Data
3.2. Prediction of Survival
3.2.1. Overall Survival
3.2.2. Recurrence-Free Survival
3.2.3. Early Recurrence
3.3. Differential Diagnosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rizvi, S.; Khan, S.A.; Hallemeier, C.L.; Kelley, R.K.; Gores, G.J. Cholangiocarcinoma-evolving concepts and therapeutic strategies. Nat. Rev. Clin. Oncol. 2018, 15, 95–111. [Google Scholar] [CrossRef] [Green Version]
- Banales, J.M.; Marin, J.J.; Lamarca, A.; Rodrigues, P.M.; Khan, S.A.; Roberts, L.R.; Cardinale, V.; Carpino, G.; Andersen, J.B.; Braconi, C.; et al. Cholangiocarcinoma 2020: The next horizon in mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 557–588. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferro, V.; Gorgen, A.; Roayaie, S.; dit Busset, M.D.; Sapisochin, G. Liver resection and transplantation for intrahepatic cholangiocarcinoma. J. Hepatol. 2020, 72, 364–377. [Google Scholar] [CrossRef] [Green Version]
- Torzilli, G.; Viganò, L.; Fontana, A.; Procopio, F.; Terrone, A.; Cimino, M.M.; Donadon, M.; Del Fabbro, D. Oncological outcome of R1 vascular margin for mass-forming cholangiocarcinoma. A single center observational cohort analysis. HPB 2020, 22, 570–577. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, T.; Ebata, T.; Nagino, M. Advanced hilar cholangiocarcinoma: An aggressive surgical approach for the treatment of advanced hilar cholangiocarcinoma: Perioperative management, extended procedures, and multidisciplinary approaches. Surg. Oncol. 2020, 33, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Hickman, L.; Contreras, C. Gallbladder Cancer: Diagnosis, Surgical Management, and Adjuvant Therapies. Surg. Clin. 2019, 99, 337–355. [Google Scholar]
- Guo, X.; Shen, W. Latest evidence on immunotherapy for cholangiocarcinoma (Review). Oncol. Lett. 2020, 20, 381. [Google Scholar] [CrossRef]
- EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [CrossRef] [Green Version]
- Viganò, L.; Lleo, A.; Muglia, R.; Gennaro, N.; Samà, L.; Colapietro, F.; Roncalli, M.; Aghemo, A.; Chiti, A.; Di Tommaso, L.; et al. Intrahepatic cholangiocellular carcinoma with radiological enhancement patterns mimicking hepatocellular carcinoma. Updates Surg. 2020, 72, 413–421. [Google Scholar] [CrossRef]
- Li, R.; Cai, P.; Ma, K.S.; Ding, S.Y.; Guo, D.Y.; Yan, X.C. Dynamic enhancement patterns of intrahepatic cholangiocarcinoma in cirrhosis on contrast-enhanced computed tomography: Risk of misdiagnosis as hepatocellular carcinoma. Sci. Rep. 2016, 6, 26772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novikov, A.; Kowalski, T.E.; Loren, D.E. Practical Management of Indeterminate Biliary Strictures. Gastrointest. Endosc. Clin. 2019, 29, 205–214. [Google Scholar] [CrossRef]
- Martinez, N.S.; Trindade, A.J.; Sejpal, D.V. Determining the Indeterminate Biliary Stricture: Cholangioscopy and Beyond. Curr. Gastroenterol. Rep. 2020, 22, 58. [Google Scholar] [CrossRef] [PubMed]
- Mavros, M.N.; Economopoulos, K.P.; Alexiou, V.G.; Pawlik, T.M. Treatment and Prognosis for Patients With Intrahepatic Cholangiocarcinoma: Systematic Review and Meta-analysis. JAMA Surg. 2014, 149, 565–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsukamoto, M.; Yamashita, Y.I.; Imai, K.; Umezaki, N.; Yamao, T.; Okabe, H.; Nakagawa, S.; Hashimoto, D.; Chikamoto, A.; Ishiko, T.; et al. Predictors of Cure of Intrahepatic Cholangiocarcinoma After Hepatic Resection. Anticancer Res. 2017, 37, 6971–6975. [Google Scholar]
- Conci, S.; Ruzzenente, A.; Vigano, L.; Ercolani, G.; Fontana, A.; Bagante, F.; Bertuzzo, F.; Dore, A.; Pinna, A.D.; Torzilli, G.; et al. Patterns of Distribution of Hepatic Nodules (Single, Satellites or Multifocal) in Intrahepatic Cholangiocarcinoma: Prognostic Impact After Surgery. Ann. Surg. Oncol. 2018, 25, 3719–3727. [Google Scholar] [CrossRef] [PubMed]
- Sollini, M.; Antunovic, L.; Chiti, A.; Kirienko, M. Towards clinical application of image mining: A systematic review on artificial intelligence and radiomics. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2656–2672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambin, P.; Leijenaar, R.T.; Deist, T.M.; Peerlings, J.; De Jong, E.E.; Van Timmeren, J.; Sanduleanu, S.; Larue, R.T.; Even, A.J.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef]
- Ferro, M.; de Cobelli, O.; Vartolomei, M.D.; Lucarelli, G.; Crocetto, F.; Barone, B.; Sciarra, A.; Del Giudice, F.; Muto, M.; Maggi, M.; et al. Prostate Cancer Radiogenomics-From Imaging to Molecular Characterization. Int. J. Mol. Sci. 2021, 22, 9971. [Google Scholar] [CrossRef]
- Song, J.; Yin, Y.; Wang, H.; Chang, Z.; Liu, Z.; Cui, A. A review of original articles published in the emerging field of radiomics. Eur. J. Radiol. 2020, 127, 108991. [Google Scholar] [CrossRef]
- Fiz, F.; Viganò, L.; Gennaro, N.; Costa, G.; La Bella, L.; Boichuk, A.; Cavinato, L.; Sollini, M.; Politi, L.S.; Chiti, A.; et al. Radiomics of Liver Metastases: A Systematic Review. Cancers 2020, 12, 2881. [Google Scholar] [CrossRef]
- Costa, G.; Cavinato, L.; Masci, C.; Fiz, F.; Sollini, M.; Politi, L.S.; Chiti, A.; Balzarini, L.; Aghemo, A.; di Tommaso, L.; et al. Virtual Biopsy for Diagnosis of Chemotherapy-Associated Liver Injuries and Steatohepatitis: A Combined Radiomic and Clinical Model in Patients with Colorectal Liver Metastases. Cancers 2021, 13, 3077. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 372, n71. [Google Scholar]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Sadot, E.; Simpson, A.L.; Do, R.K.; Gonen, M.; Shia, J.; Allen, P.J.; D’Angelica, M.I.; DeMatteo, R.P.; Kingham, T.P.; Jarnagin, W.R. Cholangiocarcinoma: Correlation between Molecular Profiling and Imaging Phenotypes. PLoS ONE 2015, 10, e0132953. [Google Scholar]
- Ji, G.W.; Zhu, F.P.; Zhang, Y.D.; Liu, X.S.; Wu, F.Y.; Wang, K.; Xia, Y.X.; Zhang, Y.D.; Jiang, W.J.; Li, X.C.; et al. A radiomics approach to predict lymph node metastasis and clinical outcome of intrahepatic cholangiocarcinoma. Eur. Radiol. 2019, 29, 3725–3735. [Google Scholar] [CrossRef]
- King, M.J.; Hectors, S.; Lee, K.M.; Omidele, O.; Babb, J.S.; Schwartz, M.; Tabrizian, P.; Taouli, B.; Lewis, S. Outcomes assessment in intrahepatic cholangiocarcinoma using qualitative and quantitative imaging features. Cancer Imaging 2020, 20, 43. [Google Scholar] [CrossRef]
- Yang, C.; Huang, M.; Li, S.; Chen, J.; Yang, Y.; Qin, N.; Huang, D.; Shu, J. Radiomics model of magnetic resonance imaging for predicting pathological grading and lymph node metastases of extrahepatic cholangiocarcinoma. Cancer Lett. 2020, 470, 1–7. [Google Scholar] [CrossRef]
- Zhang, J.; Wu, Z.; Zhang, X.; Liu, S.; Zhao, J.; Yuan, F.; Shi, Y.; Song, B. Machine learning: An approach to preoperatively predict PD-1/PD-L1 expression and outcome in intrahepatic cholangiocarcinoma using MRI biomarkers. ESMO Open 2020, 5, e000910. [Google Scholar] [CrossRef]
- Peng, Y.T.; Zhou, C.Y.; Lin, P.; Wen, D.Y.; Wang, X.D.; Zhong, X.Z.; Pan, D.H.; Que, Q.; Li, X.; Chen, L.; et al. Preoperative Ultrasound Radiomics Signatures for Noninvasive Evaluation of Biological Characteristics of Intrahepatic Cholangiocarcinoma. Acad. Radiol. 2020, 27, 785–797. [Google Scholar] [CrossRef]
- Yao, X.; Huang, X.; Yang, C.; Hu, A.; Zhou, G.; Ju, M.; Lei, J.; Shu, J. A Novel Approach to Assessing Differentiation Degree and Lymph Node Metastasis of Extrahepatic Cholangiocarcinoma: Prediction Using a Radiomics-Based Particle Swarm Optimization and Support Vector Machine Model. JMIR Med. Inform. 2020, 8, e23578. [Google Scholar] [CrossRef]
- Liu, X.; Khalvati, F.; Namdar, K.; Fischer, S.; Lewis, S.; Taouli, B.; Haider, M.A.; Jhaveri, K.S. Can machine learning radiomics provide pre-operative differentiation of combined hepatocellular cholangiocarcinoma from hepatocellular carcinoma and cholangiocarcinoma to inform optimal treatment planning? Eur. Radiol. 2021, 31, 244–255. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Huang, Z.; Cao, L.; Zhang, Z.; Wei, Y.; Zhang, X.; Song, B. Differentiation combined hepatocellular and cholangiocarcinoma from intrahepatic cholangiocarcinoma based on radiomics machine learning. Ann. Transl. Med. 2020, 8, 119. [Google Scholar] [CrossRef] [PubMed]
- Lewis, S.; Peti, S.; Hectors, S.J.; King, M.; Rosen, A.; Kamath, A.; Putra, J.; Thung, S.; Taouli, B. Volumetric quantitative histogram analysis using diffusion-weighted magnetic resonance imaging to differentiate HCC from other primary liver cancers. Abdom. Radiol. 2019, 44, 912–922. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Ma, X.; Liang, M.; Li, D.; Ma, P.; Wang, S.; Wu, Z.; Zhao, X. Prediction for early recurrence of intrahepatic mass-forming cholangiocarcinoma: Quantitative magnetic resonance imaging combined with prognostic immunohistochemical markers. Cancer Imaging 2019, 19, 49. [Google Scholar] [CrossRef] [Green Version]
- Liang, W.; Xu, L.; Yang, P.; Zhang, L.; Wan, D.; Huang, Q.; Niu, T.; Chen, F. Novel Nomogram for Preoperative Prediction of Early Recurrence in Intrahepatic Cholangiocarcinoma. Front. Oncol. 2018, 8, 360. [Google Scholar] [CrossRef]
- Peng, Y.; Lin, P.; Wu, L.; Wan, D.; Zhao, Y.; Liang, L.; Ma, X.; Qin, H.; Liu, Y.; Li, X.; et al. Ultrasound-Based Radiomics Analysis for Preoperatively Predicting Different Histopathological Subtypes of Primary Liver Cancer. Front. Oncol. 2020, 10, 1646. [Google Scholar] [CrossRef]
- Chu, H.; Liu, Z.; Liang, W.; Zhou, Q.; Zhang, Y.; Lei, K.; Tang, M.; Cao, Y.; Chen, S.; Peng, S.; et al. Radiomics using CT images for preoperative prediction of futile resection in intrahepatic cholangiocarcinoma. Eur. Radiol. 2021, 31, 2368–2376. [Google Scholar] [CrossRef]
- Xu, L.; Yang, P.; Liang, W.; Liu, W.; Wang, W.; Luo, C.; Wang, J.; Peng, Z.; Xing, L.; Huang, M.; et al. A radiomics approach based on support vector machine using MR images for preoperative lymph node status evaluation in intrahepatic cholangiocarcinoma. Theranostics 2019, 9, 5374–5385. [Google Scholar] [CrossRef]
- Xue, B.; Wu, S.; Zheng, M.; Jiang, H.; Chen, J.; Jiang, Z.; Tian, T.; Tu, Y.; Zhao, H.; Shen, X.; et al. Development and Validation of a Radiomic-Based Model for Prediction of Intrahepatic Cholangiocarcinoma in Patients With Intrahepatic Lithiasis Complicated by Imagologically Diagnosed Mass. Front. Oncol. 2020, 10, 598253. [Google Scholar] [CrossRef]
- Zhang, J.; Wu, Z.; Zhao, J.; Liu, S.; Zhang, X.; Yuan, F.; Shi, Y.; Song, B. Intrahepatic cholangiocarcinoma: MRI texture signature as predictive biomarkers of immunophenotyping and survival. Eur. Radiol. 2021, 31, 3661–3672. [Google Scholar] [CrossRef]
- Xu, L.; Yang, P.; Yen, E.A.; Wan, Y.; Jiang, Y.; Cao, Z.; Shen, X.; Wu, Y.; Wang, J.; Luo, C.; et al. A multi-organ cancer study of the classification performance using 2D and 3D image features in radiomics analysis. Phys. Med. Biol. 2019, 64, 215009. [Google Scholar] [CrossRef] [PubMed]
- Mosconi, C.; Cucchetti, A.; Bruno, A.; Cappelli, A.; Bargellini, I.; De Benedittis, C.; Lorenzoni, G.; Gramenzi, A.; Tarantino, F.P.; Parini, L.; et al. Radiomics of cholangiocarcinoma on pretreatment CT can identify patients who would best respond to radioembolisation. Eur. Radiol. 2020, 30, 4534–4544. [Google Scholar] [CrossRef] [PubMed]
- Qin, H.; Hu, X.; Zhang, J.; Dai, H.; He, Y.; Zhao, Z.; Yang, J.; Xu, Z.; Hu, X.; Chen, Z. Machine-learning radiomics to predict early recurrence in perihilar cholangiocarcinoma after curative resection. Liver Int. 2021, 41, 837–850. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Mao, Y.; Chen, J.; Qiu, Y.; Guan, Y.; Wang, Z.; He, J. Value of contrast-enhanced CT texture analysis in predicting IDH mutation status of intrahepatic cholangiocarcinoma. Sci. Rep. 2021, 11, 6933. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Zhang, W.; Fan, C.L.; Zhang, J.; Yuan, F.; Liu, S.Y.; Li, F.Y.; Song, B. Development and validation of preoperative magnetic resonance imaging-based survival predictive nomograms for patients with perihilar cholangiocarcinoma after radical resection: A pilot study. Eur. J. Radiol. 2021, 138, 109631. [Google Scholar] [CrossRef]
- Xue, B.; Wu, S.; Zhang, M.; Hong, J.; Liu, B.; Xu, N.; Zeng, Q.; Tang, K.; Zheng, X. A radiomic-based model of different contrast-enhanced CT phase for differentiate intrahepatic cholangiocarcinoma from inflammatory mass with hepatolithiasis. Abdom. Radiol. 2021, 46, 3835–3844. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhou, G.; Zhang, J.; Xu, C.; Wang, X.; Xu, P. Radiomics signature on dynamic contrast-enhanced MR images: A potential imaging biomarker for prediction of microvascular invasion in mass-forming intrahepatic cholangiocarcinoma. Eur. Radiol. 2021, 31, 6846–6855. [Google Scholar] [CrossRef]
- Ji, G.W.; Zhang, Y.D.; Zhang, H.; Zhu, F.P.; Wang, K.; Xia, Y.X.; Zhang, Y.D.; Jiang, W.J.; Li, X.C.; Wang, X.H. Biliary Tract Cancer at CT: A Radiomics-based Model to Predict Lymph Node Metastasis and Survival Outcomes. Radiology 2019, 290, 90–98. [Google Scholar] [CrossRef] [Green Version]
- Park, H.J.; Park, B.; Park, S.Y.; Choi, S.H.; Rhee, H.; Park, J.H.; Cho, E.S.; Yeom, S.K.; Park, S.; Park, M.S.; et al. Preoperative prediction of postsurgical outcomes in mass-forming intrahepatic cholangiocarcinoma based on clinical, radiologic, and radiomics features. Eur. Radiol. 2021, 31, 8638–8648. [Google Scholar] [CrossRef]
- Choi, T.W.; Kim, J.H.; Park, S.J.; Ahn, S.J.; Joo, I.; Han, J.K. Risk stratification of gallbladder polyps larger than 10 mm using high-resolution ultrasonography and texture analysis. Eur. Radiol. 2018, 28, 196–205. [Google Scholar] [CrossRef]
- Fiz, F.; Costa, G.; Gennaro, N.; la Bella, L.; Boichuk, A.; Sollini, M.; Politi, L.S.; Balzarini, L.; Torzilli, G.; Chiti, A.; et al. Contrast Administration Impacts CT-Based Radiomics of Colorectal Liver Metastases and Non-Tumoral Liver Parenchyma Revealing the “Radiological” Tumour Microenvironment. Diagnostics 2021, 11, 1162. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, T.; Ouhmich, F.; Gonzalez-Cabrera, C.; Felli, E.; Saviano, A.; Agnus, V.; Savadjiev, P.; Baumert, T.F.; Pessaux, P.; Marescaux, J.; et al. Radiomics in hepatocellular carcinoma: A quantitative review. Hepatol. Int. 2019, 13, 546–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.Y.; Lee, K.S.; Seo, B.K.; Cho, K.R.; Woo, O.H.; Song, S.E.; Kim, E.K.; Lee, H.Y.; Kim, J.S.; Cha, J. Radiomic machine learning for predicting prognostic biomarkers and molecular subtypes of breast cancer using tumor heterogeneity and angiogenesis properties on MRI. Eur. Radiol. 2022, 32, 650–660. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.; Henry, A.; Scarsbrook, A. The value of MR textural analysis in prostate cancer. Clin. Radiol. 2019, 74, 876–885. [Google Scholar] [CrossRef]
- Jin, K.P.; Sheng, R.F.; Yang, C.; Zeng, M.S. Combined arterial and delayed enhancement patterns of MRI assist in prognostic prediction for intrahepatic mass-forming cholangiocarcinoma (IMCC). Abdom. Radiol. 2022, 47, 640–650. [Google Scholar] [CrossRef]
- Ciresa, M.; De Gaetano, A.M.; Pompili, M.; Saviano, A.; Infante, A.; Montagna, M.; Guerra, A.; Giuga, M.; Vellone, M.; Ardito, F.; et al. Enhancement patterns of intrahepatic mass-forming cholangiocarcinoma at multiphasic computed tomography and magnetic resonance imaging and correlation with clinicopathologic features. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 2786–2797. [Google Scholar]
- Iavarone, M.; Piscaglia, F.; Vavassori, S.; Galassi, M.; Sangiovanni, A.; Venerandi, L.; Forzenigo, L.V.; Golfieri, R.; Bolondi LColombo, M. Contrast enhanced CT-scan to diagnose intrahepatic cholangiocarcinoma in patients with cirrhosis. J. Hepatol. 2013, 58, 1188–1193. [Google Scholar] [CrossRef]
- Zhao, Y.J.; Chen, W.X.; Wu, D.S.; Zhang, W.Y.; Zheng, L.R. Differentiation of mass-forming intrahepatic cholangiocarcinoma from poorly differentiated hepatocellular carcinoma: Based on the multivariate analysis of contrast-enhanced computed tomography findings. Abdom. Radiol. 2016, 41, 978–989. [Google Scholar] [CrossRef]
- Tsunematsu, S.; Chuma, M.; Kamiyama, T.; Miyamoto, N.; Yabusaki, S.; Hatanaka, K.; Mitsuhashi, T.; Kamachi, H.; Yokoo, H.; Kakisaka, T.; et al. Intratumoral artery on contrast-enhanced computed tomography imaging: Differentiating intrahepatic cholangiocarcinoma from poorly differentiated hepatocellular carcinoma. Abdom. Imaging 2015, 40, 1492–1499. [Google Scholar] [CrossRef]
- Rimola, J.; Forner, A.; Reig, M.; Vilana, R.; de Lope, C.R.; Ayuso, C.; Bruix, J. Cholangiocarcinoma in cirrhosis: Absence of contrast washout in delayed phases by magnetic resonance imaging avoids misdiagnosis of hepatocellular carcinoma. Hepatology 2009, 50, 791–798. [Google Scholar] [CrossRef]
- Huang, B.; Wu, L.; Lu, X.Y.; Xu, F.; Liu, C.F.; Shen, W.F.; Jia, N.Y.; Cheng, H.Y.; Yang, Y.F.; Shen, F. Small Intrahepatic Cholangiocarcinoma and Hepatocellular Carcinoma in Cirrhotic Livers May Share Similar Enhancement Patterns at Multiphase Dynamic MR Imaging. Radiology 2016, 281, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Mansour, J.C.; Aloia, T.A.; Crane, C.H.; Heimbach, J.K.; Nagino, M.; Vauthey, J.N. Hilar Cholangiocarcinoma: Expert consensus statement. HPB 2015, 17, 691–699. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| # | Author | Year | Patients | Tumor Site | Imaging Modality | Analyzed Series | Second-Order Features | Study Design | Validation | Surgery | Analyzed Outcome | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Diagnosis | Pathology | Prognosis | |||||||||||
| 1 | Sadot E [24] | 2015 | 25 | ICC | CT | PVP | Y | R | N | N | N | Y | N |
| 2 | Choi TW [50] | 2018 | 136 | GB polyps | US | - | Y | R | N | Y | Y | N | N |
| 3 | Liang W [35] | 2018 | 209 | ICC | MRI | AP | Y | R | Y | Y | N | N | Y |
| 4 | Xu L [38] | 2019 | 148 | ICC | MRI | T1-weighted contrast-enhanced | Y | R | Y | Y | N | Y | N |
| 5 | Xu L [41] | 2019 | 332 | ICC | CT/MRI | NR | Y | R | Y | Y | N | Y | Y |
| 6 | Ji GW [48] | 2019 | 274 | Mixed | CT | PVP | Y | R | Y | Y | N | Y | Y |
| 7 | Lewis S [33] | 2019 | 17 | ICC | MRI | DWI | N | R | N | N | Y | N | N |
| 8 | Zhao L [34] | 2019 | 47 | ICC | MRI | T2 fat suppr, AP, PVP, LP | Y | R | Y | Y | N | N | Y |
| 9 | Ji GW [25] | 2019 | 155 | ICC | CT | AP | Y | R | Y | Y | N | Y | Y |
| 10 | King MJ [26] | 2020 | 73 | ICC | CT/MRI | CT: AP, PVP MRI: AP, PVP, EP, LP, DWI | Y | R | N | Y | N | Y | Y |
| 11 | Yang C [27] | 2020 | 100 | EBDT | MRI | T1WI, T2WI, DWI | Y | R | Y | Y | N | Y | N |
| 12 | Zhang J [28] | 2020 | 98 | ICC | MRI | AP, PVP | Y | R | Y | Y | N | Y | Y |
| 13 | Peng Y [29] | 2020 | 128 | ICC | US | - | Y | R | Y | Y | N | Y | N |
| 14 | Yao X [30] | 2020 | 110 | EBDT | MRI | T1WI, T2WI, DWI, ADC | Y | R | Y | Y | N | Y | N |
| 15 | Zhang J [32] | 2020 | 123 | ICC | CT | AP, PVP | Y | R | Y | Y | Y | N | N |
| 16 | Peng Y [36] | 2020 | 89 | ICC | US | - | Y | R | Y | Y | Y | N | N |
| 17 | Mosconi C [42] | 2020 | 55 | ICC | CT | AP, PVP, LP | Y | R | N | N | N | N | Y |
| 18 | Zhang J [40] | 2021 | 78 | ICC | MRI | AP, PVP, unenhanced T1W1, T2WI, DWI | Y | R | N | Y | N | Y | N |
| 19 | Qin H [43] | 2021 | 274 | PHCC | CT | AP, PVP, DP, EP | Y | R | Y | Y | N | N | Y |
| 20 | Chu H [37] | 2021 | 203 | ICC | CT | PVP | Y | R | Y | Y | N | N | Y |
| 21 | Liu X [31] | 2021 | 24 | ICC | CT/MRI | 4 CT phases + 9 MRI phases | Y | R | N | N | Y | N | N |
| 22 | Xue B [39] | 2021 | 53 | ICC | CT | AP | Y | R | Y | Y | Y | N | N |
| 23 | Zhu Y [44] | 2021 | 138 | ICC | CT | Basal, AP, PVP, LP | Y | R | Y | Y | N | Y | N |
| 24 | Zhao J [45] | 2021 | 184 | PHCC | MRI | AP and PVP | Y | R | Y | Y | N | N | Y |
| 25 | Xue B [46] | 2021 | 61 | ICC | CT | AP and PVP | Y | R | Y | Y | Y | N | N |
| 26 | Zhou Y [47] | 2021 | 126 | ICC | MRI | T2 fat suppr, T1 in-phase and opposed phase, DWI, basal, AP, PVP, DP | Y | R | Y | Y | N | Y | N |
| 27 | Park HJ [49] | 2021 | 345 | ICC | CT | AP, PVP | Y | R | Y | Y | N | N | Y |
| First Author | Patient Selection Bias Risk | Index Test Bias Risk | Reference Standard Bias Risk | Flow and Timing Bias Risk | Patient Selection Applicability | Index Test Applicability | Reference Standard Applicability |
|---|---|---|---|---|---|---|---|
| Sadot E, 2015 [24] | L | U | U | L | L | L | L |
| Choi TW, 2018 [50] | L | L | L | U | L | L | L |
| Liang W, 2018 [35] | H | L | L | U | L | L | L |
| Xu L, 2019 [38] | H | L | L | U | L | L | L |
| Xu L, 2019 [41] | U | U | U | U | L | U | L |
| Ji GW, 2019 [48] | H | L | L | L | H | L | L |
| Lewis S, 2019 [33] | H | L | L | H | L | H | L |
| Zhao L, 2019 [34] | H | L | L | U | L | L | L |
| Ji GW, 2019 [25] | L | L | L | L | L | L | H |
| King MJ, 2020 [26] | H | L | L | H | L | H | L |
| Yang C, 2020 [27] | L | L | L | U | L | L | L |
| Zhang J, 2020 [28] | H | U | U | L | L | L | L |
| Peng Y, 2020 [29] | H | U | U | L | L | H | L |
| Yao X, 2020 [30] | L | L | L | L | L | L | L |
| Zhang J, 2020 [32] | H | L | L | U | L | L | L |
| Peng Y, 2020 [36] | H | U | U | L | L | H | L |
| Mosconi C, 2020 [42] | L | L | L | L | H | L | L |
| Zhang J, 2021 [40] | H | U | U | L | L | L | L |
| Qin H, 2021 [43] | U | L | L | L | H | L | L |
| Chu H, 2021 [37] | H | U | U | L | L | L | L |
| Liu X, 2021 [31] | L | L | L | L | L | H | L |
| Xue B, 2020 [39] | L | L | L | U | L | U | L |
| Zhu Y, 2021 [44] | H | L | L | L | L | L | L |
| Zhao J, 2021 [45] | L | L | L | L | L | L | L |
| Xue B, 2021 [46] | L | L | L | L | L | L | L |
| Zhou Y, 2021 [47] | H | U | U | L | H | L | L |
| Park HJ, 2021 [49] | H | L | L | U | L | L | L |
| Radiomic model | Combined Model | |||||||
|---|---|---|---|---|---|---|---|---|
| Author Diagnosis | Imaging N° Patients | Radiomic Features | AUC (95% CI) Training/Validation | Accuracy (95% CI) Training/Validation | Variables | AUC (95% CI) Training/Validation | Accuracy (95% CI) Training/Validation | |
| Lymph Node Metastases | ||||||||
| Ji GW, 2019 [25] ICC | CT N = 155 | Score (kurtosis, GLDM_SDE, GLCM_Contrast, RLNU, and GLNU) | 0.823 (0.739–0.907)/0.871 (0.775–0.968) | Radiomics + Ca19-9 + N status at CT | 0.846 (0.768–0.925)/0.892 (0.810–0.975) | |||
| Yang C, 2020 [27] EBDT | MRI N = 100 | Signature (no details) | 0.880/0.900 | 0.814/0.833 | ||||
| Yao X, 2020 [30] EBDT | MRI N = 110 | Signature (no details) | 0.904/0.889 | 0.836/0.812 | ||||
| Xu L, 2019 [38] ICC | MRI N = 148 | Score (GLCM, GLSZM wavelet transforms) | 0.788 (0.698–0.862)/0.787 (0.634–0.898) | 0.736/0.691 | Radiomics + Ca19-9 + N status at MRI | 0.842 (0.758–0.906)/0.870 (0.730–0.953) | 0.726/0.786 | |
| Xu L, 2019 [41] ICC | CT/MRI N = 332 | Signature (no significant features) | 0.704/0.729 | |||||
| Ji GW, 2019 [48] Mixed BT | CT N = 274 | Signature (shape_MinorAxis, firstorder_Skewness, glszm_ZoneEntropy) | 0.790 (0.730–0.860)/0.770 (0.660–0.880) | Radiomics + N status at CT | 0.810 (0.750–0.870)/0.800 (0.700–0.900) | |||
| Tumor grading | ||||||||
| King MJ, 2020 [26] ICC | CT/MRI N = 73 | No association | ||||||
| Yang C, 2020 [27] EBDT | MRI N = 100 | Signature (no details) | 0.780/0.800 | 0.699/0.710 | ||||
| Peng Y 2020 [29] ICC | US N = 128 | Score (kurtosis, skewness) | 0.732/0.712 | 0.735/0.722 | ||||
| Yao X, 2020 [30] EBDT | MRI N = 110 | Signature (no details) | 0.891/0.846 | 0.826/0.809 | ||||
| Microscopic vascular invasion | ||||||||
| Peng Y, 2020 [29] ICC | US N = 128 | Score (IQRs) | 0.699/0.756 | 0.848/0.684 | ||||
| Zhou Y, 2021 [47] ICC | MRI N = 126 | Score (GLDM, ZP, GLRLM, skewness, and mean) | 0.873 (0.796–0.950)/0.850 (0.709–0.991) | 0.863/0.868 | ||||
| Radiomics | Combined Model | |||||||
|---|---|---|---|---|---|---|---|---|
| Author Diagnosis | Imaging N° pts | Signature/Parameter | C-Index (95% CI) Training/Validation | HR (95% CI) | Data | Details | C-Index (95% CI) Training/Validation | Comparison |
| Overall Survival | ||||||||
| Ji GW, 2019 [25] ICC | CT N = 155 | Score (kurtosis, GLDM_SDE, GLCM_Contrast, RLNU, GLNU) | 3.650 (1.950–6.830) | |||||
| King MJ,2020 [26] ICC | CT/MRI N = 73 | Measure of correlation and ADCmin | NR | NR | ||||
| Zhang J, 2020 [28] ICC | MRI N = 98 | AP: LRE, LRHGE, LRLGE, RLNU, SRE | 0.673 | 3.721 (2.210–6.265) | Radiomics + Clinical | Imaging classification (Parenchymal/ductal) CEA | 0.721 (0.658–0.783) | Combined better than radiomic and pathology (PD-1, PD-L1, CEA) |
| Zhang J, 2021 [40] ICC | MRI N = 78 | AP: wavelet-HLH_firstorder_Median | 0.700 (0.570–0.820) | |||||
| Mosconi C, 2020 [42] ICC | CT N = 55 | No association | ||||||
| Zhao J, 2021 [45] PHCC | MRI N = 184 | Score: AP (Kurtosis, Correlation, Homogeneity, GLNU, HGRE, Surfac/Volume) PVP (Correlation, SRHGE) | 0.877 (0.774–0.979)/0.756 (0.615–0.897) | Radiomics + Clinical Radiological | CEA, N stage at imaging, invasion of hepatic artery at imaging | 0.962 (0.905–1)/ 0.814 (0.569–1) | Combined better than clinical and radiomic (clinical similar to radiomic) | |
| Ji GW, 2019 [48] Mixed BT | CT N = 274 | Score (GLSZM_Zone Entropy, Skewness, Minor Axis) | 3.370 (1.920–5.910) | |||||
| Park HJ, 2021 [49] ICC | CT N = 345 | Score (GLCM_Entropy, GLDZM_HGE, Mean) | Radiomics + Clinical Radiological | Tumor contour, multiplicity, periductal tumor infiltration, extrahepatic organ invasion, suspicion of LN metastases | 0.750/0.680 | Combined better than clinical-radiological | ||
| Recurrence-free Survival | ||||||||
| Ji GW, 2019 [25] ICC | CT N = 155 | Score (kurtosis, GLDM_SDE, GLCM_Contrast, RLNU, GLNU | 2.770 (1.580–4.840) | |||||
| King MJ,2020 [26] ICC | CT/MRI N = 73 | MRI variance | 0.550 (0.310–0.970) | |||||
| Mosconi C, 2020 [42] ICC | CT N = 55 | Signature (mean, kurtosis, skewness, GLCM_Homogeneity, GLCM_Dissimilarity) | 0.460 (0.220–0.950) | |||||
| Ji GW, 2019 [48] Mixed BT | CT N = 274 | Score (GLSZM_Zone Entropy, Skewness, Minor Axis) | 1.980 (1.260–3.120) | |||||
| Park HJ, 2021 [49] ICC | CT N = 345 | Score (GLCM_Entropy, GLDZM_HGE, Mean) | 0.690 (0.660–0.750)/0.680 (0.610–0.740) | Radiomics + Clinical Radiological | Tumor contour, multiplicity, periductal tumor infiltration, extrahepatic organ invasion, suspicion of LN metastases | 0.750 (0.720–0.790)/0.710 (0.640–0.770) | Combined better than radiomic and clinical-radiologic. Clinical-radiological similar to radiomic | |
| Author Diagnosis | Imaging N° pts | Radiomics | Combined Model | |||||
|---|---|---|---|---|---|---|---|---|
| Signature/Parameter | AUC (95% CI) Training/Validation | Accuracy (95% CI) Training/Validation | Data | AUC (95% CI) Training/Validation | Accuracy (95% CI) Training/Validation | Comparison | ||
| Zhao L, 2019 [34] ICC | MRI N = 47 | Radiomic model (AP skewness; PVP variance; AP_Cluster-Shade_AllDirection_offset7_SD; AP_GLCMEntropy_angle45_offset7) | 0.889 (0.783–0.996) | 0.809 | Radiomics + Enhancement pattern, VEGFR | 0.949 (0.894–1.000) | 0.872 (0.743–0.952) | Combined better than clinical, radiomics and pathological models |
| Liang W, 2018 [35] ICC | MRI N = 209 | Radiomics score (LRE, HGZE, Mean, GLCM_energy, and SZE) | 0.820 (0.740–0.880)/ 0.750 (0.680–0.810) * 0.770 (0.650–0.860) ** | Radiomics + TNM | 0.900 (0.830–0.940)/ 0.840 (0.780–0.890) * 0.860 (0.760–0.930) ** | Combined better than radiomic model | ||
| Xu L, 2019 [41] ICC | CT/MRI N = 332 | Score (not detailed) | 0.742 (0.666–0.809)/ 0.789 (0.655/0.889) | 0.749/0.743 | ||||
| Qin H, 2021 [43] PHCC | CT N = 274 | AP: S(3,3)AngScMom, motion_S(5,5)SumEntrp, disk_135dr_RLNonUni PP: S(5,-5)SumEntrp, motion_S(2,-2)SumEntrp, motion_S(0,4)Correlat VP: motion_S(0,5)DifVarnc, motion_S(2,-2)DifVarnc, disk_S(3,3)Entropy | 0.805/ 0.719 * 0.714 ** | 0.737 0.671 * 0.649 ** | Radiomics + Grading, N status, CA 19-9, Enhancement pattern | 0.883/ 0.867 * 0.861 ** | 0.826/ 0.757 * 0.757 ** | Combined better than clinical and radiomic models |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiz, F.; Jayakody Arachchige, V.S.; Gionso, M.; Pecorella, I.; Selvam, A.; Wheeler, D.R.; Sollini, M.; Viganò, L. Radiomics of Biliary Tumors: A Systematic Review of Current Evidence. Diagnostics 2022, 12, 826. https://doi.org/10.3390/diagnostics12040826
Fiz F, Jayakody Arachchige VS, Gionso M, Pecorella I, Selvam A, Wheeler DR, Sollini M, Viganò L. Radiomics of Biliary Tumors: A Systematic Review of Current Evidence. Diagnostics. 2022; 12(4):826. https://doi.org/10.3390/diagnostics12040826
Chicago/Turabian StyleFiz, Francesco, Visala S Jayakody Arachchige, Matteo Gionso, Ilaria Pecorella, Apoorva Selvam, Dakota Russell Wheeler, Martina Sollini, and Luca Viganò. 2022. "Radiomics of Biliary Tumors: A Systematic Review of Current Evidence" Diagnostics 12, no. 4: 826. https://doi.org/10.3390/diagnostics12040826