
Quantification of Abdominal Muscle Mass and Diagnosis of Sarcopenia with Cross-Sectional Imaging in Patients with Polycystic Kidney Disease: Correlation with Total Kidney Volume

Abstract
:1. Introduction
2. Materials and Methods
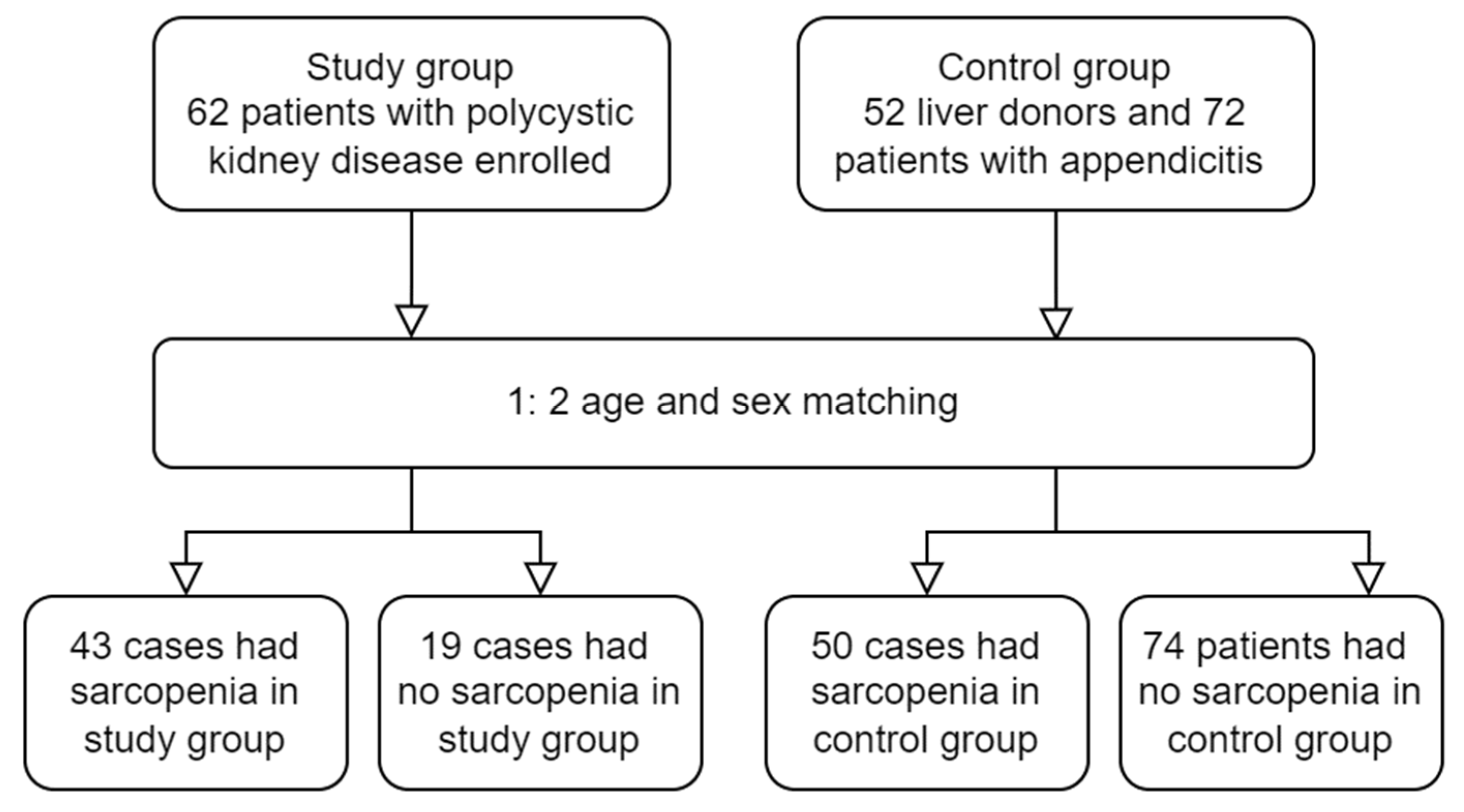
2.1. Patient and Study Design
2.2. Study Variables and Imaging Acquisition
2.3. Imaging Processing
2.4. Statistical Analysis
3. Results
3.1. Clinical and Laboratory Assessment
3.2. Correlation between Body Composition Analysis and TKV
3.3. Sarcopenia Assessment
3.4. Internal Validation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pereira, R.A.; Cordeiro, A.C.; Avesani, C.M.; Carrero, J.J.; Lindholm, B.; Amparo, F.C.; Amodeo, C.; Cuppari, L.; Kamimura, M.A. Sarcopenia in Chronic Kidney Disease on Conservative Therapy: Prevalence and Association with Mortality. Nephrol. Dial. Transplant. 2015, 30, 1718–1725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greiber, S.; Mitch, W.E. Mechanisms for Protein Catabolism in Uremia: Metabolic Acidosis and Activation of Proteolytic Pathways. Miner. Electrolyte Metab. 1992, 18, 233–236. [Google Scholar] [PubMed]
- Isoyama, N.; Qureshi, A.R.; Avesani, C.M.; Lindholm, B.; Bàràny, P.; Heimbürger, O.; Cederholm, T.; Stenvinkel, P.; Carrero, J.J. Comparative Associations of Muscle Mass and Muscle Strength with Mortality in Dialysis Patients. Clin. J. Am. Soc. Nephrol. 2014, 9, 1720–1728. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-K.; Kim, S.G.; Oh, J.-E.; Lee, Y.-K.; Noh, J.-W.; Kim, H.J.; Song, Y.R. Impact of Sarcopenia on Long-Term Mortality and Cardiovascular Events in Patients Undergoing Hemodialysis. Korean J. Intern. Med. 2019, 34, 599–607. [Google Scholar] [CrossRef]
- Cederholm, T.; Bosaeus, I.; Barazzoni, R.; Bauer, J.; Van Gossum, A.; Klek, S.; Muscaritoli, M.; Nyulasi, I.; Ockenga, J.; Schneider, S.M.; et al. Diagnostic Criteria for Malnutrition—An ESPEN Consensus Statement. Clin. Nutr. 2015, 34, 335–340. [Google Scholar] [CrossRef]
- Cesari, M.; Fielding, R.A.; Pahor, M.; Goodpaster, B.; Hellerstein, M.; Van Kan, G.A.; Anker, S.D.; Rutkove, S.; Vrijbloed, J.W.; Isaac, M.; et al. Biomarkers of Sarcopenia in Clinical Trials—Recommendations from the International Working Group on Sarcopenia. J. Cachexia Sarcopenia Muscle 2012, 3, 181–190. [Google Scholar] [CrossRef] [Green Version]
- Zillikens, M.C.; Van den Berg, J.W.; Wilson, J.H.; Swart, G.R. Whole-Body and Segmental Bioelectrical-Impedance Analysis in Patients with Cirrhosis of the Liver: Changes after Treatment of Ascites. Am. J. Clin. Nutr. 1992, 55, 621–625. [Google Scholar] [CrossRef]
- Guañabens, N.; Monegal, A.; Muxi, A.; Martinez-Ferrer, A.; Reyes, R.; Caballería, J.; Del Río, L.; Peris, P.; Pons, F.; Parés, A. Patients with Cirrhosis and Ascites Have False Values of Bone Density: Implications for the Diagnosis of Osteoporosis. Osteoporos. Int. 2012, 23, 1481–1487. [Google Scholar] [CrossRef]
- Woodrow, G.; Oldroyd, B.; Turney, J.H.; Smith, M.A. Influence of Changes in Peritoneal Fluid on Body-Composition Measurements by Dual-Energy X-Ray Absorptiometry in Patients Receiving Continuous Ambulatory Peritoneal Dialysis. Am. J. Clin. Nutr. 1996, 64, 237–241. [Google Scholar] [CrossRef] [Green Version]
- Yu, S.; Visvanathan, T.; Field, J.; Ward, L.C.; Chapman, I.; Adams, R.; Wittert, G.; Visvanathan, R. Lean Body Mass: The Development and Validation of Prediction Equations in Healthy Adults. BMC Pharmacol. Toxicol. 2013, 14, 53. [Google Scholar] [CrossRef] [Green Version]
- Boer, P. Estimated Lean Body Mass as an Index for Normalization of Body Fluid Volumes in Humans. Am. J. Physiol. Ren. Physiol. 1984, 247, F632–F636. [Google Scholar] [CrossRef] [PubMed]
- Bhatla, B.; Moore, H.; Emerson, P.; Keshaviah, P.; Prowant, B.; Nolph, K.D.; Singh, A. Lean Body Mass Estimation by Creatinine Kinetics, Bioimpedance, and Dual Energy X-ray Absorptiometry in Patients on Continuous Ambulatory Peritoneal Dialysis. ASAIO J. 1995, 41, M442–M446. [Google Scholar] [CrossRef] [PubMed]
- Mourtzakis, M.; Prado, C.M.; Lieffers, J.R.; Reiman, T.; McCargar, L.J.; Baracos, V.E. A Practical and Precise Approach to Quantification of Body Composition in Cancer Patients Using Computed Tomography Images Acquired during Routine Care. Appl. Physiol. Nutr. Metab. 2008, 33, 997–1006. [Google Scholar] [CrossRef] [PubMed]
- Ubara, Y.; Tagami, T.; Sawa, N.; Katori, H.; Yokota, M.; Takemoto, F.; Inoue, S.; Kuzuhara, K.; Hara, S.; Yamada, A. Renal Contraction Therapy for Enlarged Polycystic Kidneys by Transcatheter Arterial Embolization in Hemodialysis Patients. Am. J. Kidney Dis. 2002, 39, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Suwabe, T.; Ubara, Y.; Sekine, A.; Ueno, T.; Yamanouchi, M.; Hayami, N.; Hoshino, J.; Kawada, M.; Hiramatsu, R.; Hasegawa, E.; et al. Effect of Renal Transcatheter Arterial Embolization on Quality of Life in Patients with Autosomal Dominant Polycystic Kidney Disease. Nephrol. Dial. Transplant. 2017, 32, 1176–1183. [Google Scholar] [CrossRef] [Green Version]
- Sakuhara, Y.; Nishio, S.; Morita, K.; Abo, D.; Hasegawa, Y.; Yuasa, N.; Mochizuki, T.; Soyama, T.; Oba, K.; Shirato, H.; et al. Transcatheter Arterial Embolization with Ethanol Injection in Symptomatic Patients with Enlarged Polycystic Kidneys. Radiology 2015, 277, 277–285. [Google Scholar] [CrossRef] [Green Version]
- Pei, Y.; Obaji, J.; Dupuis, A.; Paterson, A.D.; Magistroni, R.; Dicks, E.; Parfrey, P.; Cramer, B.; Coto, E.; Torra, R.; et al. Unified Criteria for Ultrasonographic Diagnosis of ADPKD. J. Am. Soc. Nephrol. 2009, 20, 205–212. [Google Scholar] [CrossRef] [Green Version]
- Higashihara, E.; Nutahara, K.; Okegawa, T.; Tanbo, M.; Hara, H.; Miyazaki, I.; Kobayasi, K.; Nitatori, T. Kidney Volume Estimations with Ellipsoid Equations by Magnetic Resonance Imaging in Autosomal Dominant Polycystic Kidney Disease. Nephron 2015, 129, 253–262. [Google Scholar] [CrossRef] [Green Version]
- Guiu, B.; Petit, J.M.; Loffroy, R.; Ben Salem, D.; Aho, S.; Masson, D.; Hillon, P.; Krause, D.; Cercueil, J.P. Quantification of Liver Fat Content: Comparison of Triple-Echo Chemical Shift Gradient-Echo Imaging and in Vivo Proton MR Spectroscopy1. Radiology 2009, 250, 95. [Google Scholar] [CrossRef]
- Gomez-Perez, S.L.; Haus, J.M.; Sheean, P.; Patel, B.; Mar, W.; Chaudhry, V.; McKeever, L.; Braunschweig, C. Measuring Abdominal Circumference and Skeletal Muscle from a Single Cross-Sectional Computed Tomography Image A Step-by-Step Guide for Clinicians Using National Institutes of Health ImageJ. J. Parenter. Enter. Nutr. 2016, 40, 308–318. [Google Scholar] [CrossRef] [Green Version]
- Prado, C.M.M.; Lieffers, J.R.; McCargar, L.J.; Reiman, T.; Sawyer, M.B.; Martin, L.; Baracos, V.E. Prevalence and Clinical Implications of Sarcopenic Obesity in Patients with Solid Tumours of the Respiratory and Gastrointestinal Tracts: A Population-Based Study. Lancet Oncol. 2008, 9, 629–635. [Google Scholar] [CrossRef]
- Whittle, M.; Simões, R. Hereditary Polycystic Kidney Disease: Genetic Diagnosis and Counseling. Rev. Assoc. Med. Bras. 2014, 60, 98–102. [Google Scholar] [CrossRef] [Green Version]
- Grantham, J.J.; Torres, V.E.; Chapman, A.B.; Guay-Woodford, L.M.; Bae, K.T.; King Jr, B.F.; Wetzel, L.H.; Baumgarten, D.A.; Kenney, P.J.; Harris, P.C.; et al. Volume Progression in Polycystic Kidney Disease. N. Engl. J. Med. 2006, 354, 2122–2130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, S.S.; Molnar, M.Z.; Tayek, J.A.; Ix, J.H.; Noori, N.; Benner, D.; Heymsfield, S.; Kopple, J.D.; Kovesdy, C.P.; Kalantar-Zadeh, K. Serum Creatinine as a Marker of Muscle Mass in Chronic Kidney Disease: Results of a Cross-Sectional Study and Review of Literature. J. Cachexia Sarcopenia Muscle 2013, 4, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.W.; Lien, Y.C.; Wu, H.Y.; Yen, C.J.; Pan, C.C.; Hung, T.W.; Su, C.T.; Chiang, C.K.; Cheng, H.T.; Hung, K.Y. Lean Body Mass Predicts Long-Term Survival in Chinese Patients on Peritoneal Dialysis. PLoS ONE 2013, 8, e54976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paris, M.T.; Tandon, P.; Heyland, D.K.; Furberg, H.; Premji, T.; Low, G.; Mourtzakis, M. Automated Body Composition Analysis of Clinically Acquired Computed Tomography Scans Using Neural Networks. Clin. Nutr. 2020, 39, 3049–3055. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group (n) | PKD (62) | Control (124) | p Value |
|---|---|---|---|
| Age (years) | 50.40 ± 12.20 | 50.18 ± 12.09 | 0.905 |
| Female/Male | 37/25 | 74/50 | 0.999 |
| BW (kg) | 64.80 ± 17.08 | 63.84 ± 15.32 | 0.697 |
| BH (cm) | 164.17 ± 9.68 | 162.53 ± 8.02 | 0.223 |
| BMI (kg/m2) | 23.75 ± 4.27 | 23.97 ± 4.31 | 0.742 |
| Underweight/Normal/ Overweight/Obese | 6/35/16/5 | 10/162/51/25 | 0.472 |
| Albumin (g/dL) | 4.4 ± 0.3 | 4.4 ± 0.6 | 0.686 |
| Bilirubin (mg/dL) | 0.71 ± 0.25 | 0.75 ± 0.40 | 0.522 |
| AST (U/L) | 21 ± 8 | 20 ± 9 | 0.832 |
| Platelet (K/µL) | 212 ± 47 | 223 ± 68 | 0.323 |
| Triglyceride (mg/dL) | 111 ± 50 | 109 ± 66 | 0.917 |
| Total cholesterol (mg/dL) | 173 ± 30 | 178 ± 35 | 0.513 |
| Creatinine (mg/dL) | 2.32 ± 2.95 | 0.78 ± 0.22 | <0.001 * |
| eGFR (mL/min/1.73 m2) | 66.04 ± 36.72 | 101.00 ± 23.53 | <0.001 * |
| Estimated TKV (mL) | 1869 ± 1967 | 309 ± 76 | <0.001 * |
| TAM area (cm2) | 111.12 ± 37.85 | 122.23 ± 34.65 | 0.047 * |
| VAT area (cm2) | 77.20 ± 67.62 | 108.58 ± 101.24 | 0.013 * |
| SAT area (cm2) | 125.94 ± 60.84 | 134.81 ± 69.86 | 0.396 |
| TAM index (cm2/m2) | 39.65 ± 11.44 | 45.68 ± 10.05 | <0.001 * |
| VAT index (cm2/m2) | 27.62 ± 22.20 | 40.15 ± 35.57 | 0.004 * |
| SAT index (cm2/m2) | 46.23 ± 20.77 | 51.20 ± 25.73 | 0.189 |
| TAM-defined sarcopenia | 43 | 50 | <0.001 * |
| Correlation with Estimated TKV | Correlation Coefficient (r) | p Value |
|---|---|---|
| TAM area (cm2) | −0.031 | 0.679 |
| VAT area (cm2) | −0.007 | 0.924 |
| SAT area (cm2) | −0.049 | 0.503 |
| TAM index (cm2/m2) | −0.217 | 0.003 * |
| VAT index (cm2/m2) | −0.027 | 0.714 |
| SAT index (cm2/m2) | −0.097 | 0.186 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Factors | OR | 95% CI | p | OR | 95% CI | p |
| Age (year) | 1.025 | 1.000–1.050 | 0.047 * | 1.027 | 0.999–1.055 | 0.055 |
| Gender | 1.796 | 0.993–3.249 | 0.395 | |||
| BMI (kg/m2) | 0.854 | 0.787–0.926 | <0.001 * | 0.795 | 0.721–0.877 | <0.001 * |
| Albumin (g/dL) | 0.935 | 0.361–2.422 | 0.890 | |||
| Bilirubin (mg/dL) | 0.900 | 0.325–2.494 | 0.839 | |||
| Creatinine (mg/dL) | 1.389 | 1.041–1.854 | 0.025 * | 1.054 | 0.728–1.527 | 0.779 |
| eGFR (mL/min/1.73 m2) | 1.043 | 0.994–1.096 | 0.089 | |||
| Estimated TKV (mL) | 1.001 | 1.000–1.001 | 0.004 * | 1.001 | 1.000–1.001 | 0.013 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, C.-H.; Lai, T.-S.; Chen, Y.-M.; Chen, C.-M.; Yang, S.-C.; Liang, P.-C. Quantification of Abdominal Muscle Mass and Diagnosis of Sarcopenia with Cross-Sectional Imaging in Patients with Polycystic Kidney Disease: Correlation with Total Kidney Volume. Diagnostics 2022, 12, 755. https://doi.org/10.3390/diagnostics12030755
Wu C-H, Lai T-S, Chen Y-M, Chen C-M, Yang S-C, Liang P-C. Quantification of Abdominal Muscle Mass and Diagnosis of Sarcopenia with Cross-Sectional Imaging in Patients with Polycystic Kidney Disease: Correlation with Total Kidney Volume. Diagnostics. 2022; 12(3):755. https://doi.org/10.3390/diagnostics12030755
Chicago/Turabian StyleWu, Chih-Horng, Tai-Shuan Lai, Yung-Ming Chen, Chyi-Mong Chen, Shun-Chung Yang, and Po-Chin Liang. 2022. "Quantification of Abdominal Muscle Mass and Diagnosis of Sarcopenia with Cross-Sectional Imaging in Patients with Polycystic Kidney Disease: Correlation with Total Kidney Volume" Diagnostics 12, no. 3: 755. https://doi.org/10.3390/diagnostics12030755