
Evaluation and Comparison of the Predictive Value of 4C Mortality Score, NEWS, and CURB-65 in Poor Outcomes in COVID-19 Patients: A Retrospective Study from a Single Center in Romania

 , , , , , ,
, , , , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants
2.3. Data Sources Measurement and Outcome
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
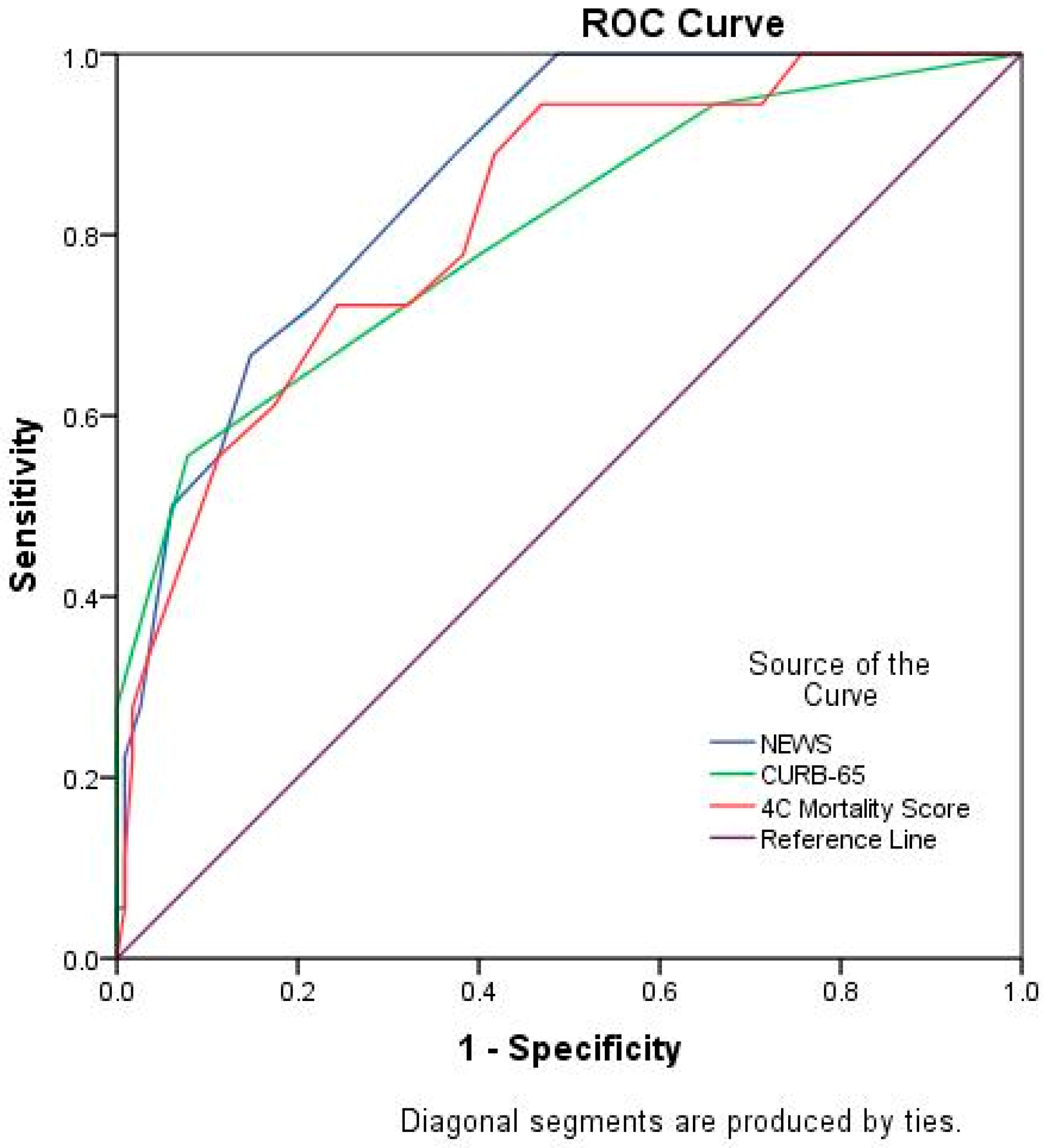
3.2. Comparison of 4C Mortality Score, NEWS and CURB-65 Scores
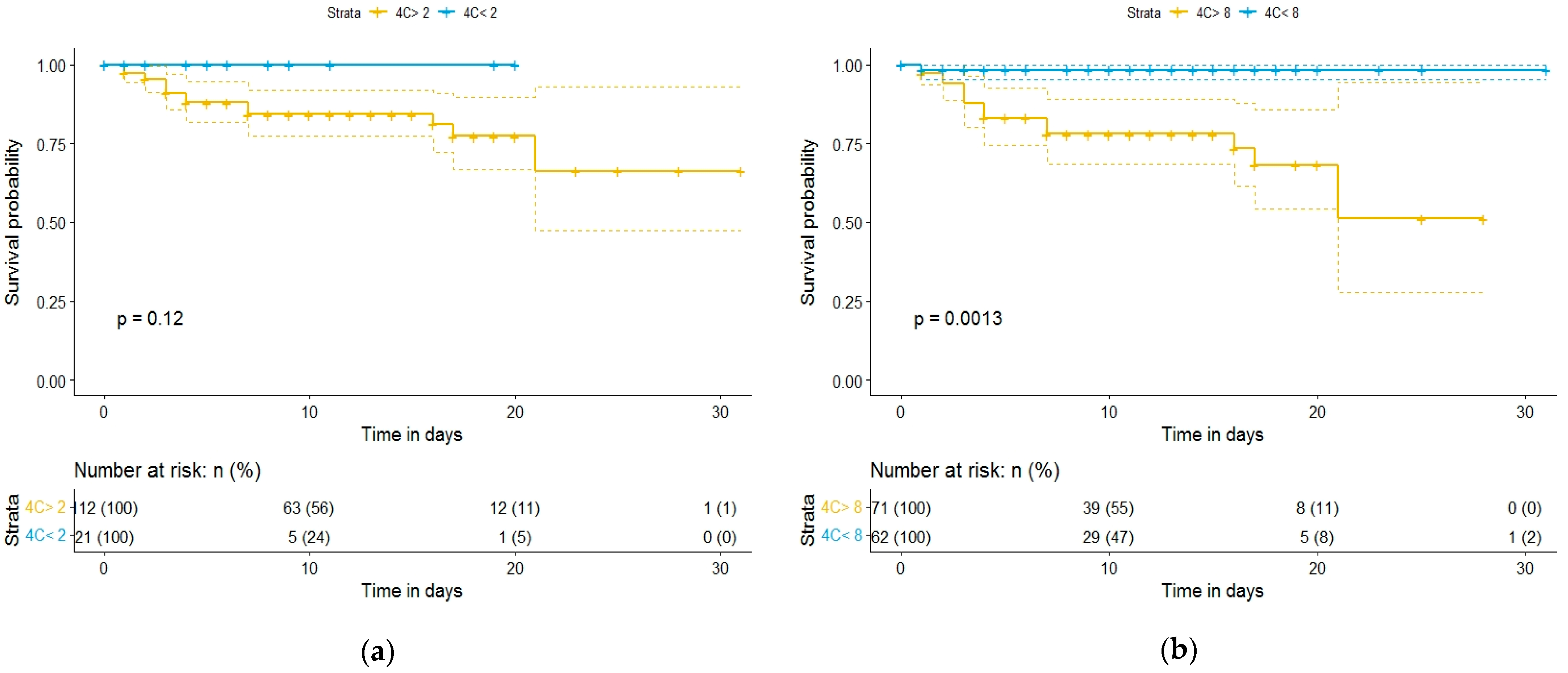
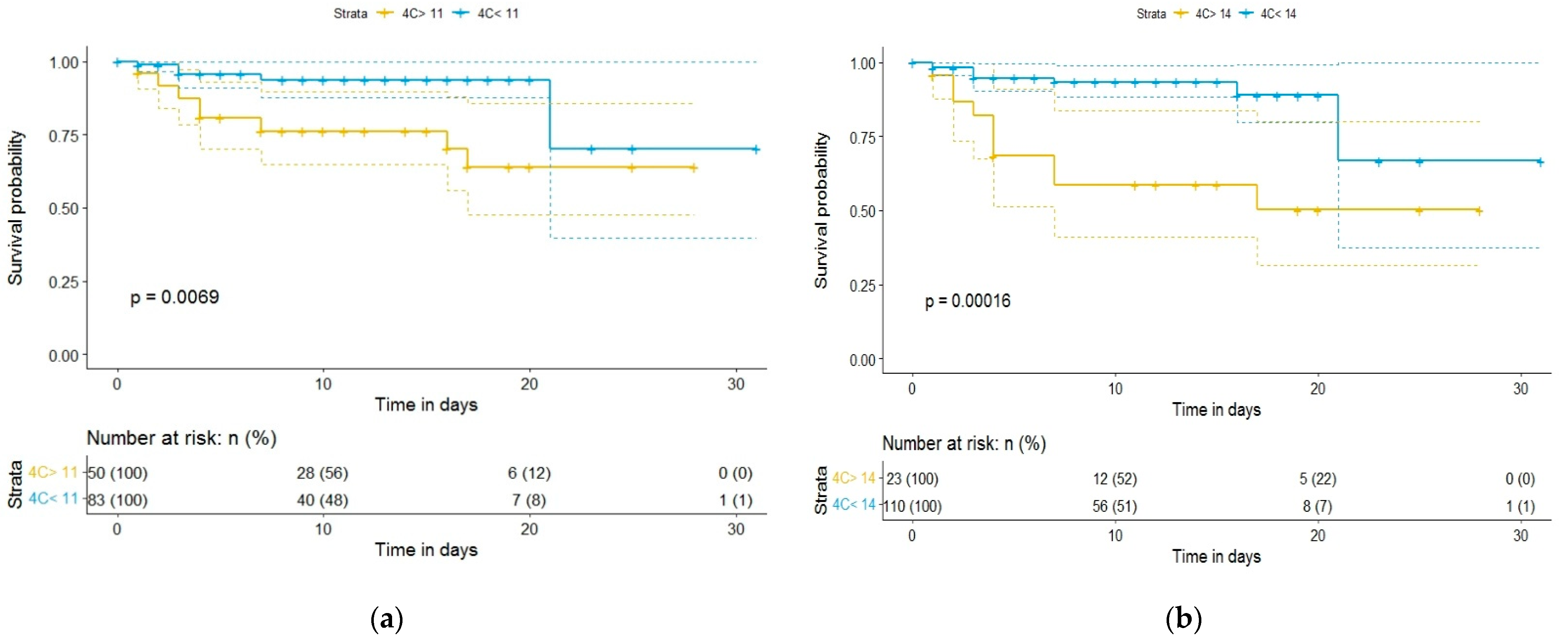
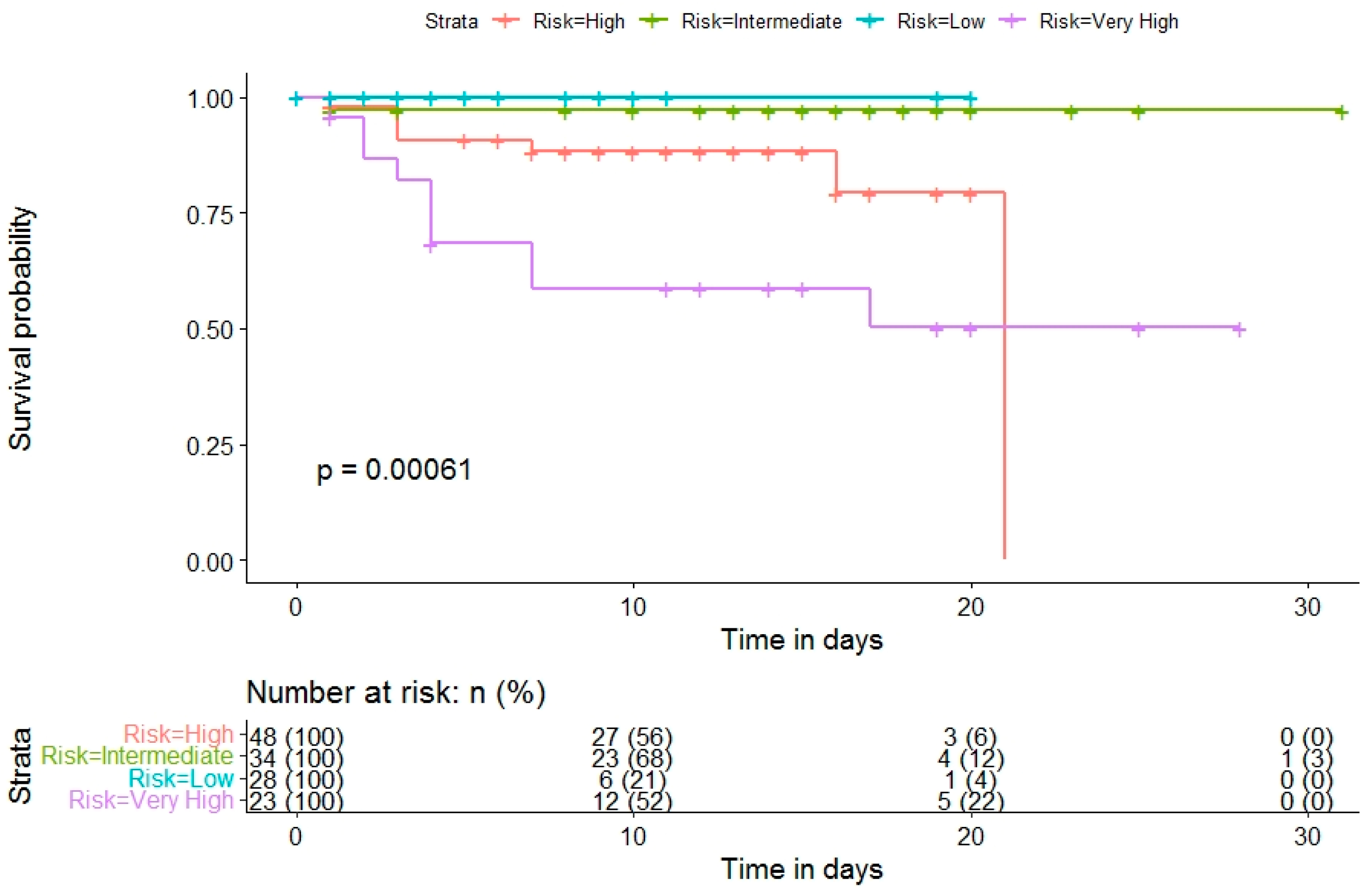
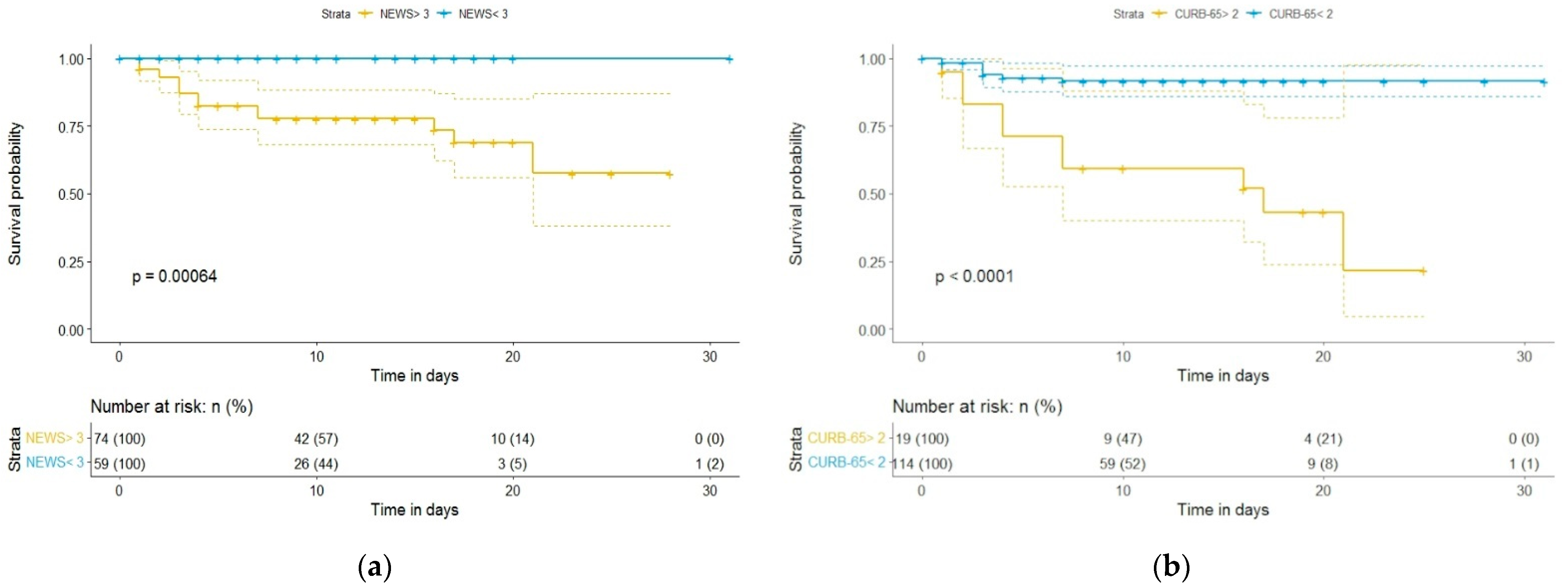
3.3. Association of 4C Mortality Score, NEWS, and CURB-65 Scores with COVID-19 Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Abbreviation | Full Form | Definition |
|---|---|---|
| ARDS | Acute respiratory distress syndrome | A life-threatening lung injury that allows fluid to leak into the lungs. |
| AUC | Area under the ROC curve | A performance measurement for the classification problems at various threshold settings. |
| CAP | Community-acquired pneumonia | An acute infection of the pulmonary parenchyma in someone who has not recently had close contact with the health care system. |
| CKD | Chronic kidney disease | Kidney damage or glomerular filtration rate (GFR) < 60 mL/min/1.73 m2 for 3 months or more, irrespective of cause. |
| COPD | Chronic obstructive pulmonary disease | A type of lung disease marked by permanent damage to tissues in the lungs, making it hard to breathe. |
| COVID-19 | Coronavirus disease 2019 | A respiratory disease caused by SARS-CoV-2, a coronavirus discovered in 2019. |
| ICU | Intensive care unit | The part of a hospital that provides intensive care. |
| IQI | Interquartile range | A measure of statistical dispersion. |
| .NEWS | National Early Warning Score | A tool developed by the Royal College of Physicians which improves the detection and response to clinical deterioration in adult patients. |
| ROC curve | Receiver operating characteristic curve | A graphical plot that illustrates the diagnostic ability of a binary classifier system as its discrimination threshold is varied. |
| WHO | World Health Organization | A specialized agency of the United Nations responsible for international public health. |
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- COVID Live—Coronavirus Statistics—Worldometer. Available online: https://www.worldometers.info/coronavirus/ (accessed on 13 February 2022).
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical Course and Outcomes of Critically Ill Patients with SARS-CoV-2 Pneumonia in Wuhan, China: A Single-Centered, Retrospective, Observational Study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- George, P.M.; Barratt, S.L.; Condliffe, R.; Desai, S.R.; Devaraj, A.; Forrest, I.; Gibbons, M.A.; Hart, N.; Jenkins, R.G.; McAuley, D.F.; et al. Respiratory Follow-up of Patients with COVID-19 Pneumonia. Thorax 2020, 75, 1009–1016. [Google Scholar] [CrossRef] [PubMed]
- Van Dam, P.M.E.L.; Zelis, N.; van Kuijk, S.M.J.; Linkens, A.E.M.J.H.; Brüggemann, R.A.G.; Spaetgens, B.; van der Horst, I.C.C.; Stassen, P.M. Performance of Prediction Models for Short-Term Outcome in COVID-19 Patients in the Emergency Department: A Retrospective Study. Ann. Med. 2021, 53, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, Y.; Azoyan, L.; Szychowiak, P.; Bellamine, A.; Lemaitre, G.; Bernaux, M.; Daniel, C.; Leblanc, J.; Riller, Q.; Steichen, O. External Validation of Prognostic Scores for COVID-19: A Multicenter Cohort Study of Patients Hospitalized in Greater Paris University Hospitals. Intensive Care Med. 2021, 47, 1426–1439. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Pandita, A.; Hardesty, A.; McCarthy, M.; Aridi, J.; Weiss, Z.F.; Beckwith, C.G.; Farmakiotis, D. Validation of Pneumonia Prognostic Scores in a Statewide Cohort of Hospitalised Patients with COVID-19. Int. J. Clin. Pract. 2020, 75, e13926. [Google Scholar] [CrossRef] [PubMed]
- Knight, S.R.; Ho, A.; Pius, R.; Buchan, I.; Carson, G.; Drake, T.M.; Dunning, J.; Fairfield, C.J.; Gamble, C.; Green, C.A.; et al. Risk Stratification of Patients Admitted to Hospital with Covid-19 Using the ISARIC WHO Clinical Characterisation Protocol: Development and Validation of the 4C Mortality Score. BMJ 2020, 370, m3339. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, S.; Matsumoto, S.; Sano, T.; Kitai, T.; Yonetsu, T.; Kohsaka, S.; Torii, S.; Kishi, T.; Komuro, I.; Hirata, K.; et al. External Validation of the 4C Mortality Score for Patients with COVID-19 and Pre-Existing Cardiovascular Diseases/Risk Factors. BMJ Open 2021, 11, e052708. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Zhou, B.; Zhu, M.; Yuan, Y.; Wang, Q.; Zhou, H.; Wang, X.; Lv, T.; Li, S.; Liu, P.; et al. CURB-65 May Serve as a Useful Prognostic Marker in COVID-19 Patients within Wuhan, China: A Retrospective Cohort Study. Epidemiol. Infect. 2020, 148, e241. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, Y.; Corre, F.; Honsel, V.; Curac, S.; Zarrouk, V.; Fantin, B.; Galy, A. Applicability of the CURB-65 Pneumonia Severity Score for Outpatient Treatment of COVID-19. J. Infect. 2020, 81, e96–e98. [Google Scholar] [CrossRef] [PubMed]
- Royal College of Physicians of London. National Early Warning Score (NEWS): Standardising the Assessment of Acute-Illness Severity in the NHS; Royal College of Physicians: London, UK, 2012. [Google Scholar]
- Lim, W.; van der Eerden, M.M.; Laing, R.; Boersma, W.; Karalus, N.; Town, G.; Lewis, S.; Macfarlane, J. Defining Community Acquired Pneumonia Severity on Presentation to Hospital: An International Derivation and Validation Study. Thorax 2003, 58, 377–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Citu, C.; Gorun, F.; Motoc, A.; Sas, I.; Gorun, O.M.; Burlea, B.; Tuta-Sas, I.; Tomescu, L.; Neamtu, R.; Malita, D.; et al. The Predictive Role of NLR, d-NLR, MLR, and SIRI in COVID-19 Mortality. Diagnostics 2022, 12, 122. [Google Scholar] [CrossRef] [PubMed]
- Macedo, A.; Gonçalves, N.; Febra, C. COVID-19 Fatality Rates in Hospitalized Patients: Systematic Review and Meta-Analysis. Ann. Epidemiol. 2021, 57, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Doğanay, F.; Ak, R. Performance of the CURB-65, ISARIC-4C and COVID-GRAM Scores in Terms of Severity for COVID-19 Patients. Int. J. Clin. Pract. 2021, 75, e14759. [Google Scholar] [CrossRef] [PubMed]
- Kostakis, I.; Smith, G.B.; Prytherch, D.; Meredith, P.; Price, C.; Chauhan, A. The Performance of the National Early Warning Score and National Early Warning Score 2 in Hospitalised Patients Infected by the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Resuscitation 2021, 159, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Pokeerbux, M.R.; Yelnik, C.M.; Faure, E.; Drumez, E.; Bruandet, A.; Labreuche, J.; Assaf, A.; Goffard, A.; Garabedian, C.; Poissy, J.; et al. National Early Warning Score to Predict Intensive Care Unit Transfer and Mortality in COVID-19 in a French Cohort. Int. J. Clin. Pract. 2021, 75, e14121. [Google Scholar] [CrossRef] [PubMed]
- Lim, N.T.; Pan, D.; Barker, J. NEWS2 System Requires Modification to Identify Deteriorating Patients with COVID-19. Clin. Med. 2020, 20, e133–e134. [Google Scholar] [CrossRef] [PubMed]
- Jamshidi, M.; Lalbakhsh, A.; Talla, J.; Peroutka, Z.; Hadjilooei, F.; Lalbakhsh, P.; Jamshidi, M.; Spada, L.L.; Mirmozafari, M.; Dehghani, M.; et al. Artificial Intelligence and COVID-19: Deep Learning Approaches for Diagnosis and Treatment. IEEE Access 2020, 8, 109581–109595. [Google Scholar] [CrossRef] [PubMed]
- Jamshidi, M.B.; Talla, J.; Lalbakhsh, A.; Sharifi-Atashgah, M.S.; Sabet, A.; Peroutka, Z. A Conceptual Deep Learning Framework for COVID-19 Drug Discovery. In Proceedings of the 2021 IEEE 12th Annual Ubiquitous Computing, Electronics & Mobile Communication Conference (UEMCON), New York, NY, USA, 1–4 December 2021; IEEE: New York, NY, USA, 2021; pp. 00030–00034. [Google Scholar] [CrossRef]





| Variables | Overall (n = 133) | Survivors (n = 115) | Died (n = 18) | p-Value |
|---|---|---|---|---|
| Demographics | ||||
| Gender (n/%) | ||||
| Female | 65/48.9% | 58/50.4% | 7/38.9% | 0.45 (OR = 1.59) |
| Male | 68/51.1% | 57/ 49.6% | 11/61.1% | |
| Age (years; median (IQR)) | 65 (21) | 62 (20.5) | 70 (15.5) | 0.02 |
| Comorbidities (n/%) | ||||
| Hypertension | 87/65.4% | 72/62.6% | 15/83.3% | 0.11 (OR = 2.96) |
| Diabetes | 59/44.4% | 49/42.6% | 10/55.6% | 0.32 (OR = 1.67) |
| Cardiovascular disease | 44/33.1% | 32/27.8% | 12/66.7% | 0.002 (OR = 5.11) |
| CKD | 69/51.9% | 55/47.8% | 14/77.8% | 0.02 (OR = 3.78) |
| COPD/asthma | 26/19.5% | 20/17.4% | 6/33.3% | 0.12 (OR = 2.35) |
| Cancer | 15/11.3% | 11/9.6% | 4/22.2% | 0.12 (OR = 2.67) |
| Presenting symptoms (n/%) | ||||
| Cough | 77/57.9% | 65/56.5% | 12/66.7% | 0.45 (OR = 1.53) |
| Dyspnea | 69/51.9% | 59/51.3% | 10/55.6% | 0.80 (OR = 1.18) |
| Chest pain | 18/13.5% | 14/12.2% | 4/22.2% | 0.26 (OR = 2.04) |
| Fatigue | 82/61.7% | 68/59.1% | 14/77.8% | 0.19 (OR = 2.40) |
| Myalgia | 33/24.8% | 28/24.3% | 5/27.8% | 0.77 (OR = 1.19) |
| No smell/taste | 18/13.5% | 17/14.8% | 1/5.56% | 0.46 (OR = 0.34) |
| Gastrointestinal symptoms | 52/39.1% | 44/38.3% | 8/44.4% | 0.61 (OR = 1.28) |
| Clinical course (n/%) | ||||
| Mechanic ventilation | 9/6.77% | 2/1.74% | 7/38.9% | <0.001 (OR = 33.8) |
| ICU admission | 10/7.52% | 4/3.48% | 6/33.3% | <0.001 (OR = 13.3) |
| Score | Overall | Survived | Died | p-Value |
|---|---|---|---|---|
| 4C Mortality Score median (IQI) | 9 (9) | 8 (8) | 15 (5.25) | <0.001 |
| Low (0–3) n (%) | 28 (21.1%) | 28 (24.3%) | - | |
| Intermediate (4–8) n (%) | 34 (25.6%) | 33 (28.7%) | 1 (5.56%) | |
| High (9–14) n (%) | 48 (36.1%) | 41 (35.7%) | 7 (38.9%) | |
| Very high (15–21) n (%) | 23 (17.3%) | 13 (11.3%) | 10 (55.6%) | |
| NEWS median (IQI) | 4 (5) | 3 (4) | 8.5 (4.5) | <0.001 |
| CURB-65 median (IQI) | 1 (2) | 1 (2) | 3 (1.75) | <0.001 |
| Score | AUC | p-Value | 95% CI | |
|---|---|---|---|---|
| Lower | Upper | |||
| 4C Mortality score | 0.818 | <0.001 | 0.718 | 0.919 |
| NEWS | 0.861 | <0.001 | 0.784 | 0.939 |
| CURB-65 | 0.801 | <0.001 | 0.681 | 0.922 |
| Cut-Off | Sensitivity (%) | Specificity (%) |
|---|---|---|
| 4C Mortality Score | ||
| >3 | 100% | 24% |
| >8 | 94% | 53% |
| >11 | 72% | 67% |
| >14 | 55% | 88% |
| NEWS | ||
| >3 | 100% | 51% |
| CURB-65 | ||
| >2 | 55% | 92% |
| Score | Odds Ratio | p-Value | 95% CI | |
|---|---|---|---|---|
| Upper | Lower | |||
| 4C Mortality Score | 1.33 | <0.001 | 1.15 | 1.55 |
| NEWS | 1.56 | <0.001 | 1.28 | 1.91 |
| CURB-65 | 3.52 | <0.001 | 1.95 | 6.38 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Citu, C.; Gorun, F.; Motoc, A.; Ratiu, A.; Gorun, O.M.; Burlea, B.; Neagoe, O.; Citu, I.M.; Rosca, O.; Bratosin, F.; et al. Evaluation and Comparison of the Predictive Value of 4C Mortality Score, NEWS, and CURB-65 in Poor Outcomes in COVID-19 Patients: A Retrospective Study from a Single Center in Romania. Diagnostics 2022, 12, 703. https://doi.org/10.3390/diagnostics12030703
Citu C, Gorun F, Motoc A, Ratiu A, Gorun OM, Burlea B, Neagoe O, Citu IM, Rosca O, Bratosin F, et al. Evaluation and Comparison of the Predictive Value of 4C Mortality Score, NEWS, and CURB-65 in Poor Outcomes in COVID-19 Patients: A Retrospective Study from a Single Center in Romania. Diagnostics. 2022; 12(3):703. https://doi.org/10.3390/diagnostics12030703
Chicago/Turabian StyleCitu, Cosmin, Florin Gorun, Andrei Motoc, Adrian Ratiu, Oana Maria Gorun, Bogdan Burlea, Octavian Neagoe, Ioana Mihaela Citu, Ovidiu Rosca, Felix Bratosin, and et al. 2022. "Evaluation and Comparison of the Predictive Value of 4C Mortality Score, NEWS, and CURB-65 in Poor Outcomes in COVID-19 Patients: A Retrospective Study from a Single Center in Romania" Diagnostics 12, no. 3: 703. https://doi.org/10.3390/diagnostics12030703