
FDG PET/CT to Predict Recurrence of Early Breast Invasive Ductal Carcinoma

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. FDG PET/CT Imaging
2.3. Analysis of FDG PET/CT Radiomic Features
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
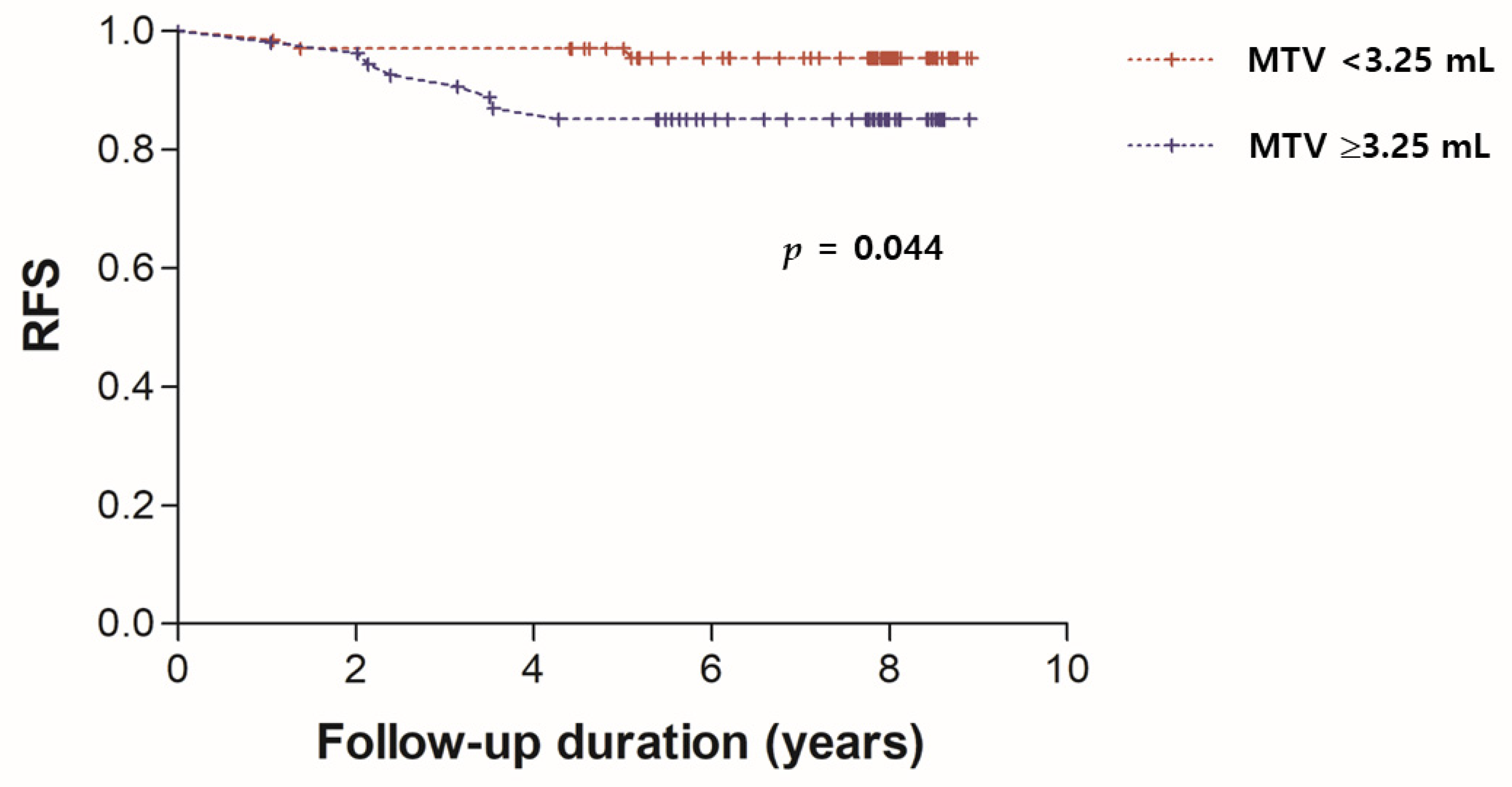
3.2. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sharma, R. Breast cancer incidence, mortality and mortality-to-incidence ratio (MIR) are associated with human development, 1990–2016: Evidence from Global Burden of Disease Study 2016. Breast Cancer 2019, 26, 428–445. [Google Scholar] [CrossRef] [PubMed]
- Mayerhoefer, M.E.; Materka, A.; Langs, G.; Haggstrom, I.; Szczypinski, P.; Gibbs, P.; Cook, G. Introduction to Radiomics. J. Nucl. Med. 2020, 61, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Vitale, I.; Shema, E.; Loi, S.; Galluzzi, L. Intratumoral heterogeneity in cancer progression and response to immunotherapy. Nat. Med. 2021, 27, 212–224. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.; Choi, H.; Paeng, J.C.; Cheon, G.J. Radiomics in Oncological PET/CT: A Methodological Overview. Nucl. Med. Mol. Imaging 2019, 53, 14–29. [Google Scholar] [CrossRef] [PubMed]
- Nioche, C.; Orlhac, F.; Boughdad, S.; Reuze, S.; Goya-Outi, J.; Robert, C.; Pellot-Barakat, C.; Soussan, M.; Frouin, F.; Buvat, I. LIFEx: A Freeware for Radiomic Feature Calculation in Multimodality Imaging to Accelerate Advances in the Characterization of Tumor Heterogeneity. Cancer Res. 2018, 78, 4786–4789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulaner, G.A. PET/CT for Patients with Breast Cancer: Where Is the Clinical Impact? AJR Am. J. Roentgenol. 2019, 213, 254–265. [Google Scholar] [CrossRef] [PubMed]
- Groheux, D.; Cochet, A.; Humbert, O.; Alberini, J.L.; Hindie, E.; Mankoff, D. 18F-FDG PET/CT for Staging and Restaging of Breast Cancer. J. Nucl. Med. 2016, 57 (Suppl. S1), 17S–26S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paydary, K.; Seraj, S.M.; Zadeh, M.Z.; Emamzadehfard, S.; Shamchi, S.P.; Gholami, S.; Werner, T.J.; Alavi, A. The Evolving Role of FDG-PET/CT in the Diagnosis, Staging, and Treatment of Breast Cancer. Mol. Imaging Biol. 2019, 21, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Groheux, D.; Giacchetti, S.; Delord, M.; de Roquancourt, A.; Merlet, P.; Hamy, A.S.; Espie, M.; Hindie, E. Prognostic impact of 18F-FDG PET/CT staging and of pathological response to neoadjuvant chemotherapy in triple-negative breast cancer. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Cochet, A.; Dygai-Cochet, I.; Riedinger, J.M.; Humbert, O.; Berriolo-Riedinger, A.; Toubeau, M.; Guiu, S.; Coutant, C.; Coudert, B.; Fumoleau, P.; et al. 18F-FDG PET/CT provides powerful prognostic stratification in the primary staging of large breast cancer when compared with conventional explorations. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 428–437. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef] [PubMed]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aerts, H.J.; Velazquez, E.R.; Leijenaar, R.T.; Parmar, C.; Grossmann, P.; Carvalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; Rietveld, D.; et al. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat. Commun. 2014, 5, 4006. [Google Scholar] [CrossRef] [PubMed]
- Bi, W.L.; Hosny, A.; Schabath, M.B.; Giger, M.L.; Birkbak, N.J.; Mehrtash, A.; Allison, T.; Arnaout, O.; Abbosh, C.; Dunn, I.F.; et al. Artificial intelligence in cancer imaging: Clinical challenges and applications. CA Cancer J. Clin. 2019, 69, 127–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fornacon-Wood, I.; Mistry, H.; Ackermann, C.J.; Blackhall, F.; McPartlin, A.; Faivre-Finn, C.; Price, G.J.; O’Connor, J.P.B. Reliability and prognostic value of radiomic features are highly dependent on choice of feature extraction platform. Eur. Radiol. 2020, 30, 6241–6250. [Google Scholar] [CrossRef] [PubMed]
- Zwanenburg, A.; Vallieres, M.; Abdalah, M.A.; Aerts, H.J.W.L.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-based Phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Z.; Zhu, G.; Jiang, X.; Zhao, Y.; Zeng, H.; Jing, J.; Ma, X. Survival Prediction in Gallbladder Cancer Using CT Based Machine Learning. Front. Oncol. 2020, 10, 604288. [Google Scholar] [CrossRef]
- Aksu, A.; Karahan Sen, N.P.; Acar, E.; Capa Kaya, G. Evaluating Focal 18F-FDG Uptake in Thyroid Gland with Radiomics. Nucl. Med. Mol. Imaging 2020, 54, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Sollini, M.; Kirienko, M.; Cavinato, L.; Ricci, F.; Biroli, M.; Ieva, F.; Calderoni, L.; Tabacchi, E.; Nanni, C.; Zinzani, P.L.; et al. Methodological framework for radiomics applications in Hodgkin’s lymphoma. Eur. J. Hybrid Imaging 2020, 4, 9. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhao, X.; Zhao, Y.; Zhang, J.; Zhang, Z.; Wang, J.; Wang, Y.; Dai, M.; Han, J. Value of pre-therapy 18F-FDG PET/CT radiomics in predicting EGFR mutation status in patients with non-small cell lung cancer. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1137–1146. [Google Scholar] [CrossRef] [PubMed]
- Kocak, B.; Durmaz, E.S.; Ates, E.; Sel, I.; Turgut Gunes, S.; Kaya, O.K.; Zeynalova, A.; Kilickesmez, O. Radiogenomics of lower-grade gliomas: Machine learning-based MRI texture analysis for predicting 1p/19q codeletion status. Eur. Radiol. 2020, 30, 877–886. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.C.; Chen, C.J.; Hsu, W.L.; Chang, S.M.; Huang, Y.F.; Tyan, Y.C. Prognostic significance of metabolic parameters and textural features on 18F-FDG PET/CT in invasive ductal carcinoma of breast. Sci. Rep. 2019, 9, 10946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groheux, D.; Martineau, A.; Teixeira, L.; Espié, M.; de Cremoux, P.; Bertheau, P.; Merlet, P.; Lemarignier, C. 18FDG-PET/CT for predicting the outcome in ER+/HER2- breast cancer patients: Comparison of clinicopathological parameters and PET image-derived indices including tumor texture analysis. Breast Cancer Res. 2017, 19, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, T.H.; Yoon, J.K.; Kang, D.K.; Kang, S.Y.; Jung, Y.S.; Han, S.; Kim, J.Y.; Yim, H.; An, Y.S. Value of volume-based metabolic parameters for predicting survival in breast cancer patients treated with neoadjuvant chemotherapy. Medicine 2016, 95, e4605. [Google Scholar] [CrossRef] [PubMed]
- Wen, W.; Xuan, D.; Hu, Y.; Li, X.; Liu, L.; Xu, D. Prognostic value of maximum standard uptake value, metabolic tumor volume, and total lesion glycolysis of positron emission tomography/computed tomography in patients with breast cancer: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0225959. [Google Scholar] [CrossRef] [PubMed]
- Kitajima, K.; Miyoshi, Y.; Yamano, T.; Odawara, S.; Higuchi, T.; Yamakado, K. Prognostic value of FDG-PET and DWI in breast cancer. Ann. Nucl. Med. 2018, 32, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Chan, J.; Chew, C.; Schultz, C. PET-SUV Max and Upstaging of Lung Cancer. Heart Lung Circ. 2019, 28, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Semrau, S.; Haderlein, M.; Schmidt, D.; Lell, M.; Wolf, W.; Waldfahrer, F.; Uder, M.; Iro, H.; Kuwert, T.; Fietkau, R. Single-cycle induction chemotherapy followed by chemoradiotherapy or surgery in patients with head and neck cancer: What are the best predictors of remission and prognosis? Cancer 2015, 121, 1214–1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, L.; Gu, P.; Huang, G.; Xue, H.; Wu, S. Prognostic significance of SUV on PET/CT in patients with esophageal cancer: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2009, 21, 1008–1015. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wu, X.; Huang, Y.; Bian, D.; Jiang, L. 18F-FDG PET/CT in lung adenosquamous carcinoma and its correlation with clinicopathological features and prognosis. Ann. Nucl. Med. 2020, 34, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.J.; Chang, S.H.; Lee, T.Y.; Yoon, S.Y.; Cheon, Y.K.; Shim, C.S.; So, Y.; Chung, H.W. Prognostic value of FDG-PET/CT total lesion glycolysis for patients with resectable distal bile duct adenocarcinoma. Anticancer Res. 2015, 35, 6985–6991. [Google Scholar] [PubMed]
- Yoon, H.J.; Kim, Y.; Chung, J.; Kim, B.S. Predicting neo-adjuvant chemotherapy response and progression-free survival of locally advanced breast cancer using textural features of intratumoral heterogeneity on F-18 FDG PET/CT and diffusion-weighted MR imaging. Breast J. 2019, 25, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Molina-García, D.; García-Vicente, A.M.; Pérez-Beteta, J.; Amo-Salas, M.; Martínez-González, A.; Tello-Galán, M.J.; Soriano-Castrejón, Á.; Pérez-García, V.M. Intratumoral heterogeneity in 18F-FDG PET/CT by textural analysis in breast cancer as a predictive and prognostic subrogate. Ann. Nucl. Med. 2018, 32, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.Y.; Franc, B.L.; Harnish, R.J.; Liu, G.; Mitra, D.; Copeland, T.P.; Arasu, V.A.; Kornak, J.; Jones, E.F.; Behr, S.C.; et al. Exploration of PET and MRI radiomic features for decoding breast cancer phenotypes and prognosis. NPJ Breast Cancer 2018, 4, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| Mean age (range) | 60 ± 10 (38–86) |
| Type of surgery | |
| BCS a Simple mastectomy MRM b | 102 4 18 |
| Mean primary tumor size (range) | 1.9 ± 0.9 (0.3–4.7) cm |
| Histologic grade | |
| G1 G2 G3 | 16 58 50 |
| AJCC c anatomic stage | |
| IA IB IIA IIB | 70 0 41 13 |
| AJCC prognostic stage | |
| IA IB IIA IIB IIIA IIIB IIIC | 76 21 17 5 4 0 1 |
| Receptor status | |
| Estrogen receptor (+/−) | 103/21 |
| Progesterone receptor (+/−) | 73/51 |
| HER2 d (+/−) | 24/100 |
| Mean Ki-67 expression (range) | 29 ± 24 (1–95) % |
| Adjuvant chemotherapy (+/−) | 95/29 |
| Adjuvant radiotherapy (+/−) | 101/23 |
| Adjuvant hormonal therapy (+/−) | 107/17 |
| Mean SUVmax e (range) | 5.2 ± 4.5 (0–19.2) |
| Mean MTV f (range) | 3.7 ± 3.2 (0–22.3) ml |
| Mean TLG g (range) | 13.3 ± 22.7 (0–198.5) |
| Mean skewness (range) | 0.69 ± 0.39 (−0.40–1.60) |
| Mean kurtosis (range) | 2.65 ± 1.03 (0–4.99) |
| Mean entropy (range) | 2.57 ± 1.10 (0–4.80) |
| Mean uniformity (range) | 0.18 ± 0.11 (0–0.48) |
| Univariate Analysis | Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Variables | No. of Patients | HR a | 95% CI b | p | HR | 95% CI | p |
| Age | |||||||
| <60 | 64 | 1 | |||||
| ≥60 | 60 | 0.59 | 0.18−1.96 | 0.397 | |||
| Size | |||||||
| ≤2 cm | 80 | 1 | |||||
| >2 cm | 44 | 3.27 | 1.03−12.26 | 0.045 | 0.55 | 0.09−3.44 | 0.519 |
| Histologic grade | |||||||
| I and II | 74 | 1 | |||||
| III | 50 | 1.83 | 0.56−6.23 | 0.31 | |||
| N stage | |||||||
| N0 | 101 | 1 | |||||
| N1 | 23 | 0.42 | 0.12−2.34 | 0.395 | |||
| AJCC c anatomic stage | |||||||
| I | 70 | 1 | |||||
| II | 54 | 0.44 | 0.13−1.44 | 0.174 | |||
| AJCC prognostic stage | |||||||
| I | 97 | 1 | |||||
| ≥II | 27 | 3.16 | 1.04−19.07 | 0.044 | 0.62 | 0.13−3.07 | 0.558 |
| Estrogen receptor | |||||||
| + | 103 | 1 | |||||
| − | 21 | 1.92 | 0.45−11.02 | 0.326 | |||
| Progesterone receptor | |||||||
| + | 73 | 1 | |||||
| − | 51 | 1.77 | 0.54−6.02 | 0.337 | |||
| HER2 d | |||||||
| + | 24 | 1 | |||||
| − | 100 | Undefined | 0.094 | ||||
| Ki-67 | |||||||
| <30% | 75 | 1 | |||||
| ≥30% | 49 | 4.39 | 1.31−14.98 | 0.017 | 2.76 | 0.57−13.37 | 0.208 |
| Adjuvant chemotherapy | |||||||
| − | 29 | 1 | |||||
| + | 95 | Undefined | 0.061 | ||||
| Adjuvant radiotherapy | |||||||
| − | 23 | 1 | |||||
| + | 101 | 1.01 | 0.22−4.64 | 0.995 | |||
| Adjuvant hormonal therapy | |||||||
| − | 17 | 1 | |||||
| + | 107 | 0.38 | 0.04−1.56 | 0.142 | |||
| SUVmax e | |||||||
| <5.0 | 76 | 1 | |||||
| ≥5.0 | 48 | 7.71 | 2.03−23.52 | 0.002 | 6.66 | 0.54−82.84 | 0.14 |
| MTV f | |||||||
| <3.25 mL | 70 | 1 | |||||
| ≥3.25 mL | 54 | 3.59 | 1.04−11.30 | 0.044 | 4.99 | 1.04−24.09 | 0.045 |
| TLG g | |||||||
| <10.5 | 82 | 1 | |||||
| ≥10.5 | 42 | 5.54 | 1.77−22.12 | 0.004 | 2.65 | 0.37−19.03 | 0.332 |
| Skewness | |||||||
| <0.638 | 49 | 1 | |||||
| ≥0.638 | 75 | 1.30 | 0.39−4.40 | 0.663 | |||
| Kurtosis | |||||||
| <2.35 | 36 | 1 | |||||
| ≥2.35 | 88 | 0.69 | 0.18−2.52 | 0.565 | |||
| Entropy | |||||||
| <3.15 | 83 | 1 | |||||
| ≥3.15 | 41 | 5.78 | 1.89−23.99 | 0.003 | 1.41 | 0.163−12.11 | 0.757 |
| Uniformity | |||||||
| <0.1 | 36 | 1 | |||||
| ≥0.1 | 88 | 0.46 | 0.11−1.56 | 0.192 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jo, J.-H.; Chung, H.W.; So, Y.; Yoo, Y.B.; Park, K.S.; Nam, S.E.; Lee, E.J.; Noh, W.C. FDG PET/CT to Predict Recurrence of Early Breast Invasive Ductal Carcinoma. Diagnostics 2022, 12, 694. https://doi.org/10.3390/diagnostics12030694
Jo J-H, Chung HW, So Y, Yoo YB, Park KS, Nam SE, Lee EJ, Noh WC. FDG PET/CT to Predict Recurrence of Early Breast Invasive Ductal Carcinoma. Diagnostics. 2022; 12(3):694. https://doi.org/10.3390/diagnostics12030694
Chicago/Turabian StyleJo, Joon-Hyung, Hyun Woo Chung, Young So, Young Bum Yoo, Kyoung Sik Park, Sang Eun Nam, Eun Jeong Lee, and Woo Chul Noh. 2022. "FDG PET/CT to Predict Recurrence of Early Breast Invasive Ductal Carcinoma" Diagnostics 12, no. 3: 694. https://doi.org/10.3390/diagnostics12030694