
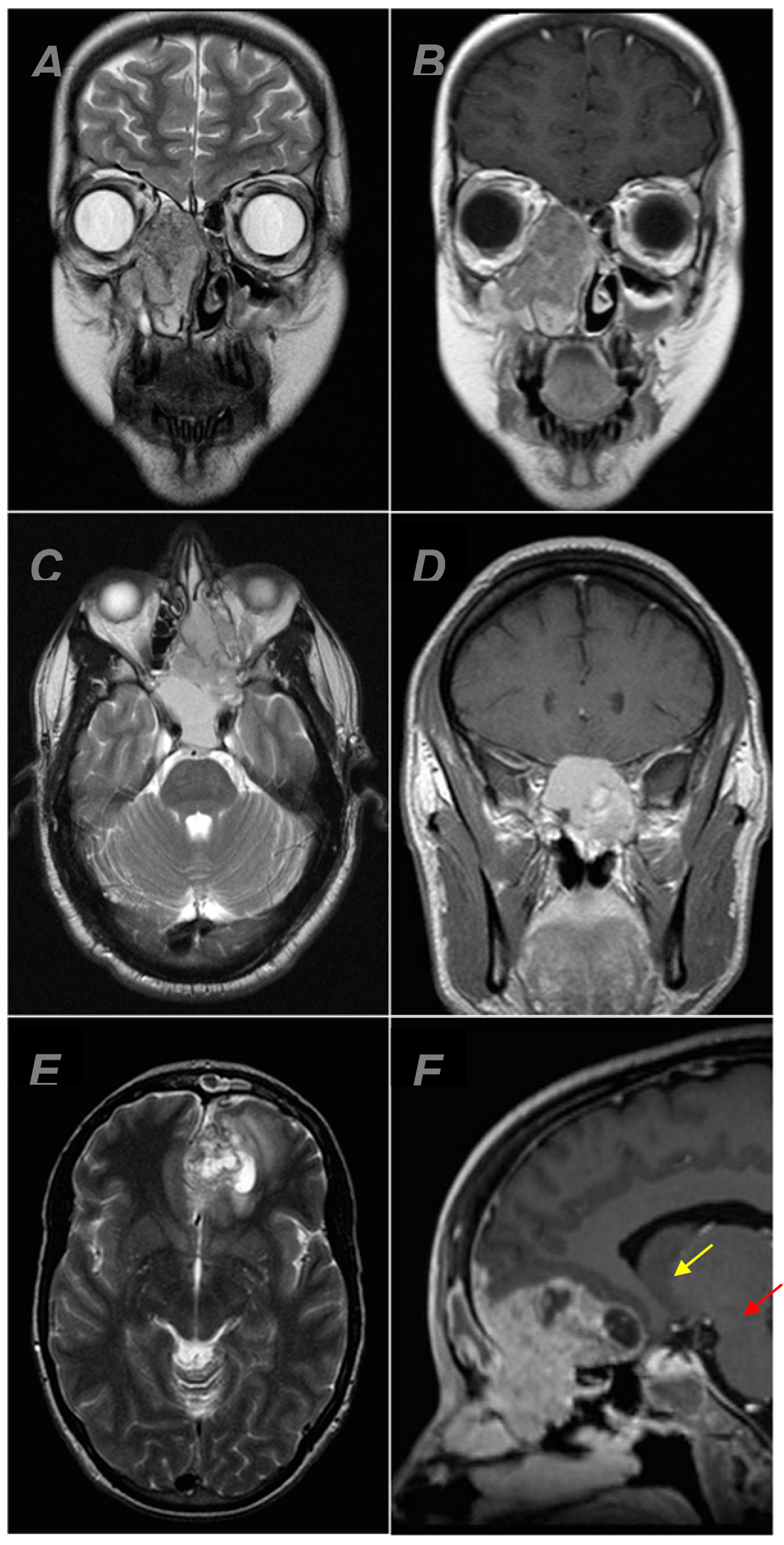
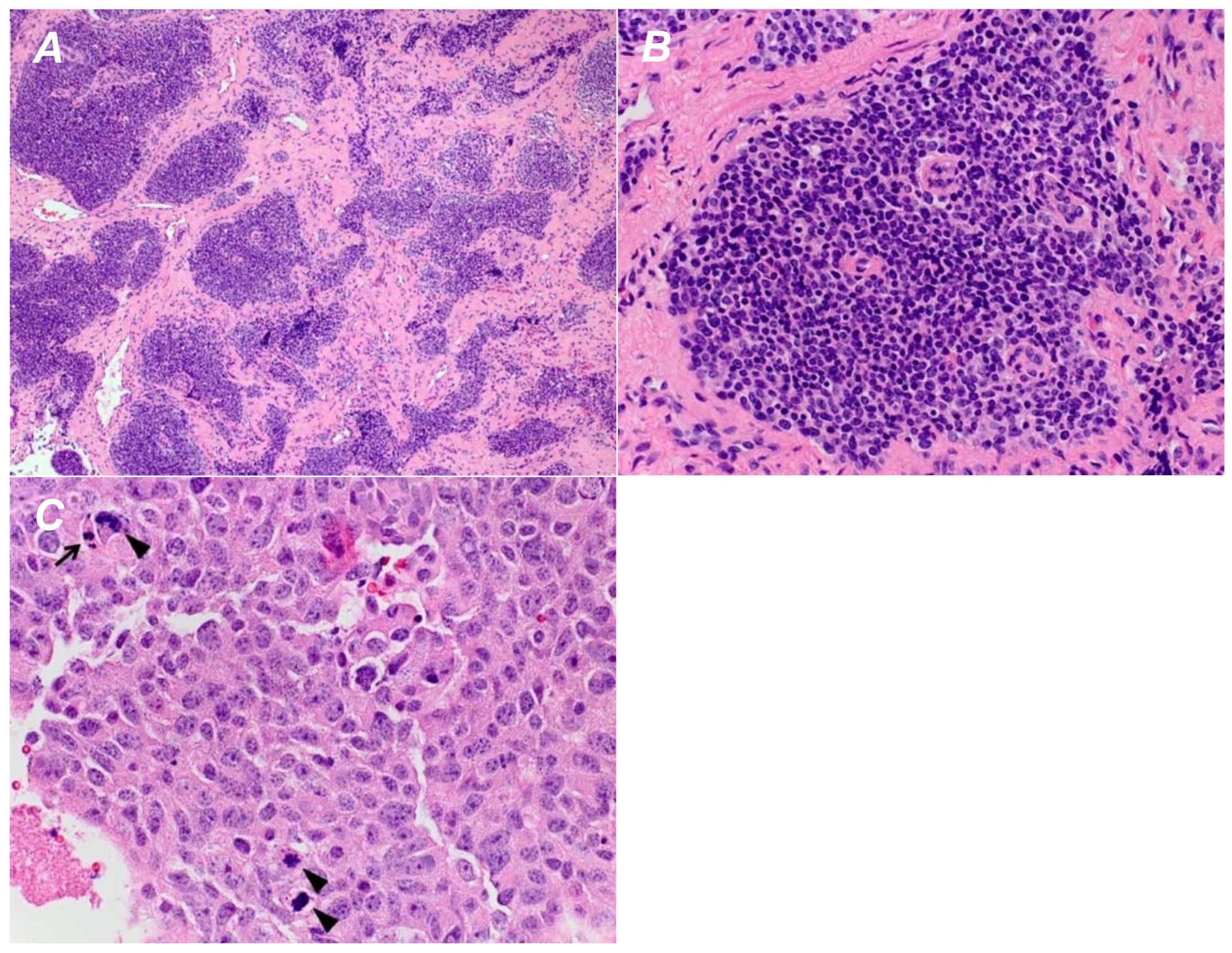
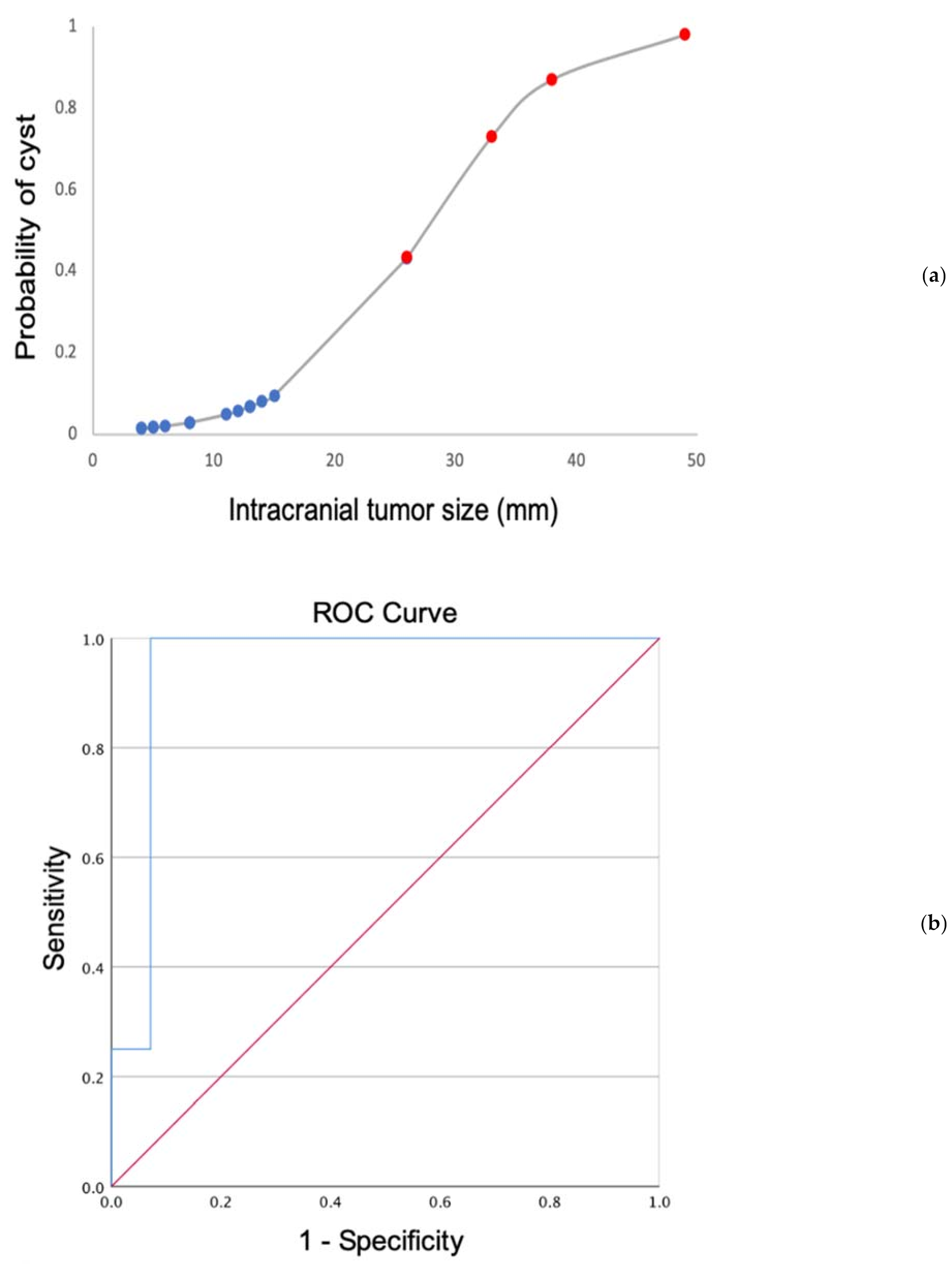
Olfactory Neuroblastoma: Re-Evaluating the Paradigm of Intracranial Extension and Cyst Formation


Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Imaging and Analysis
2.3. Specimen Analysis
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Dulguerov, P.; Allal, A.S.; Calcaterra, T.C. Esthesioneuroblastoma: A meta-analysis and review. Lancet Oncol. 2001, 2, 683–690. [Google Scholar] [CrossRef] [Green Version]
- Connor, S.E.; Umaria, N.; Chavda, S.V. Imaging of giant tumours involving the anterior skull base. Br. J. Radiol. 2001, 74, 662–667. [Google Scholar] [CrossRef] [PubMed]
- Som, P.M.; Lidov, M.; Brandwein, M.; Catalano, P.; Biller, H.F. Sinonasal esthesioneuroblastoma with intracranial extension: Marginal tumor cysts as a diagnostic MR finding. AJNR Am. J. Neuroradiol. 1994, 15, 1259–1262. [Google Scholar] [PubMed]
- Goshtasbi, K.; Abiri, A.; Abouzari, M.; Sahyouni, R.; Wang, B.Y.; Tajudeen, B.A.; Hsu, F.P.K.; Cadena, G.; Kuan, E.C. Hyams grading as a predictor of metastasis and overall survival in esthesioneuroblastoma: A meta-analysis. Int. Forum. Allergy Rhinol. 2019, 28, 22373. [Google Scholar] [CrossRef] [PubMed]
- Bell, D. Sinonasal Neuroendocrine Neoplasms: Current Challenges and Advances in Diagnosis and Treatment, with a Focus on Olfactory Neuroblastoma. Head. Neck. Pathol. 2018, 12, 22–30. [Google Scholar] [CrossRef]
- Iio, M.; Homma, A.; Furuta, Y.; Fukuda, S. Magnetic resonance imaging of olfactory neuroblastoma. Nihon Jibiinkoka Gakkai Kaiho 2006, 109, 142–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kairemo, K.J.; Jekunen, A.P.; Kestilä, M.S.; Ramsay, H.A. Imaging of olfactory neuroblastoma--an analysis of 17 cases. Auris Nasus Larynx 1998, 25, 173–179. [Google Scholar] [CrossRef]
- Yu, T.; Xu, Y.K.; Li, L.; Jia, F.G.; Duan, G.; Wu, Y.K.; Li, H.Y.; Yang, R.M.; Feng, J.; Ye, X.H.; et al. Esthesioneuroblastoma methods of intracranial extension: CT and MR imaging findings. Neuroradiology 2009, 51, 841–850. [Google Scholar] [CrossRef]
- Malouf, G.G.; Casiraghi, O.; Deutsch, E.; Guigay, J.; Temam, S.; Bourhis, J. Low- and high-grade esthesioneuroblastomas display a distinct natural history and outcome. Eur. J. Cancer 2013, 49, 1324–1334. [Google Scholar] [CrossRef]
- Bykowski, J. Sinonasal Undifferentiated Carcinoma. ASNR Published 2010. Available online: http://www.ajnr.org/content/cow/09132010 (accessed on 28 February 2022).
- Seo, E.; Yang, N. P03.23 Sinonasal teratocarcinosarcoma with intracranial extension: Case report and literature review. Neuro-Oncology 2017, 19, iii38–iii39. [Google Scholar] [CrossRef]
- Lee, A.; Goldstein, D.P.; Irish, J.; Gentili, F.; Perez-Ordonez, B. Noncontiguous bilateral esthesioneuroblastoma: A case report. Skull Base. 2007, 17, 405–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, M.-H.; Kuo, Y.-J.; Ho, C.-Y.; Kuan, E.C.; Lan, M.-Y. Metastatic Tumors of the Sinonasal Cavity: A 15-Year Review of 17 Cases. J. Clin. Med. 2019, 8, 539. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | All Patients (n = 31) | |
|---|---|---|
| Gender | females | 13 (41.9%) |
| males | 18 (58.1%) | |
| Age (year) | median | 55 |
| range | 12–79 | |
| Intracranial extension | yes | 18 (58.1%) |
| no | 13 (41.9%) | |
| Cyst formation | yes | 4 (22.2%) |
| no | 14 (77.8%) | |
| Hyams grade | I/II | 20 (80%) |
| III/IV | 5 (20%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dumont, R.A.; Palma Diaz, M.F.; Hsu, W.; Sepahdari, A.R. Olfactory Neuroblastoma: Re-Evaluating the Paradigm of Intracranial Extension and Cyst Formation. Diagnostics 2022, 12, 614. https://doi.org/10.3390/diagnostics12030614
Dumont RA, Palma Diaz MF, Hsu W, Sepahdari AR. Olfactory Neuroblastoma: Re-Evaluating the Paradigm of Intracranial Extension and Cyst Formation. Diagnostics. 2022; 12(3):614. https://doi.org/10.3390/diagnostics12030614
Chicago/Turabian StyleDumont, Rebecca A., Miguel Fernando Palma Diaz, William Hsu, and Ali R. Sepahdari. 2022. "Olfactory Neuroblastoma: Re-Evaluating the Paradigm of Intracranial Extension and Cyst Formation" Diagnostics 12, no. 3: 614. https://doi.org/10.3390/diagnostics12030614