
The AIFELL Score as a Predictor of Coronavirus Disease 2019 (COVID-19) Severity and Progression in Hospitalized Patients

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Statistical Analysis
3. Results
3.1. Linear Regression Analysis
3.2. ANOVA with Repeated Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sanches, P.R.S.; Charlie-Silva, I.; Braz, H.L.B.; Bittar, C.; Freitas Calmon, M.; Rahal, P.; Cilli, E.M. Recent Advances in SARS-CoV-2 Spike Protein and RBD Mutations Comparison between New Variants Alpha (B.1.1.7, United Kingdom), Beta (B.1.351, South Africa), Gamma (P.1, Brazil) and Delta (B.1.617.2, India). J. Virus Erad. 2021, 7, 100054. [Google Scholar] [CrossRef] [PubMed]
- Thakur, V.; Ratho, R.K. OMICRON (B.1.1.529): A New SARS-CoV-2 Variant of Concern Mounting Worldwide Fear. J. Med. Virol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Khateeb, J.; Li, Y.; Zhang, H. Emerging SARS-CoV-2 Variants of Concern and Potential Intervention Approaches. Crit. Care 2021, 25, 244. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, A.; McMenamin, J.; Taylor, B.; Robertson, C. SARS-CoV-2 Delta VOC in Scotland: Demographics, Risk of Hospital Admission, and Vaccine Effectiveness. Lancet 2021, 397, 2461–2462. [Google Scholar] [CrossRef]
- Challen, R.; Brooks-Pollock, E.; Read, J.M.; Dyson, L.; Tsaneva-Atanasova, K.; Danon, L. Risk of Mortality in Patients Infected with SARS-CoV-2 Variant of Concern 202012/1: Matched Cohort Study. BMJ 2021, 372, n579. [Google Scholar] [CrossRef]
- Lazarevic, I.; Pravica, V.; Miljanovic, D.; Cupic, M. Immune Evasion of SARS-CoV-2 Emerging Variants: What Have We Learnt so Far? Viruses 2021, 13, 1192. [Google Scholar] [CrossRef]
- Zhang, X.; Wu, S.; Wu, B.; Yang, Q.; Chen, A.; Li, Y.; Zhang, Y.; Pan, T.; Zhang, H.; He, X. SARS-CoV-2 Omicron Strain Exhibits Potent Capabilities for Immune Evasion and Viral Entrance. Signal Transduct. Target. Ther. 2021, 6, 430. [Google Scholar] [CrossRef]
- Rosen, B.; Waitzberg, R.; Israeli, A. Israel’s Rapid Rollout of Vaccinations for COVID-19. Isr. J. Health Policy Res. 2021, 10, 16. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Robertson, C.; Stowe, J.; Tessier, E.; Simmons, R.; Cottrell, S.; Roberts, R.; O’Doherty, M.; et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca Vaccines on COVID-19 Related Symptoms, Hospital Admissions, and Mortality in Older Adults in England: Test Negative Case-Control Study. BMJ 2021, 373, n1088. [Google Scholar] [CrossRef]
- Juthani, P.V.; Gupta, A.; Borges, K.A.; Price, C.C.; Lee, A.I.; Won, C.H.; Chun, H.J. Hospitalisation among Vaccine Breakthrough COVID-19 Infections. Lancet Infect. Dis. 2021, 21, 1485–1486. [Google Scholar] [CrossRef]
- Naaber, P.; Tserel, L.; Kangro, K.; Sepp, E.; Jürjenson, V.; Adamson, A.; Haljasmägi, L.; Rumm, A.P.; Maruste, R.; Kärner, J.; et al. Dynamics of Antibody Response to BNT162b2 Vaccine after Six Months: A Longitudinal Prospective Study. Lancet Reg. Health Eur. 2021, 10, 100208. [Google Scholar] [CrossRef]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine Hesitancy: The next Challenge in the Fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Padma, T.V. COVID Vaccines to Reach Poorest Countries in 2023—Despite Recent Pledges. Nature 2021, 595, 342–343. [Google Scholar] [CrossRef] [PubMed]
- Wadman, M. A Grim Warning from Israel: Vaccination Blunts, but Does Not Defeat Delta. Science 2021, 373, 838–839. [Google Scholar] [CrossRef]
- Cheng, A.; Caruso, D.; McDougall, C. Outpatient Management of COVID-19: Rapid Evidence Review. Am. Fam. Physician 2020, 102, 478–486. [Google Scholar] [PubMed]
- Levenfus, I.; Ullmann, E.; Battegay, E.; Schuurmans, M.M. Triage Tool for Suspected COVID-19 Patients in the Emergency Room: AIFELL Score. Braz. J. Infect. Dis. 2020, 24, 458–461. [Google Scholar] [CrossRef]
- Sahu, K.K.; Borogovac, A.; Cerny, J. COVID-19 Related Immune Hemolysis and Thrombocytopenia. J. Med. Virol. 2021, 93, 1164–1170. [Google Scholar] [CrossRef]
- Bouchla, A.; Kriebardis, A.G.; Georgatzakou, H.T.; Fortis, S.P.; Thomopoulos, T.P.; Lekkakou, L.; Markakis, K.; Gkotzias, D.; Panagiotou, A.; Papageorgiou, E.G.; et al. Red Blood Cell Abnormalities as the Mirror of SARS-CoV-2 Disease Severity: A Pilot Study. Front. Physiol. 2021, 12, 825055. [Google Scholar] [CrossRef]
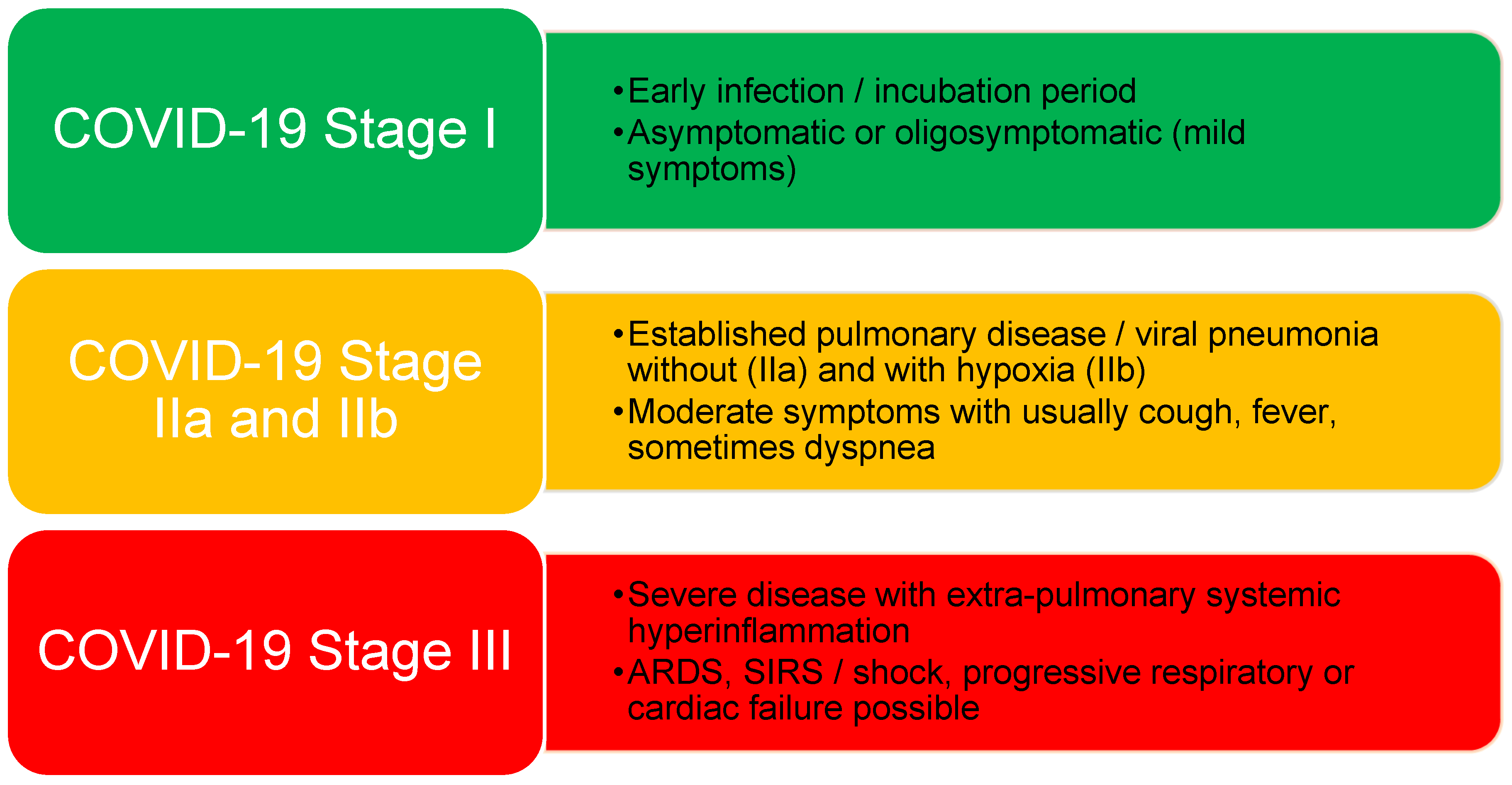
- Siddiqi, H.K.; Mehra, M.R. COVID-19 Illness in Native and Immunosuppressed States: A Clinical-Therapeutic Staging Proposal. J. Heart Lung Transplant. 2020, 39, 405–407. [Google Scholar] [CrossRef] [Green Version]
- Knight, S.R.; Ho, A.; Pius, R.; Buchan, I.; Carson, G.; Drake, T.M.; Dunning, J.; Fairfield, C.J.; Gamble, C.; Green, C.A.; et al. Risk Stratification of Patients Admitted to Hospital with COVID-19 Using the ISARIC WHO Clinical Characterisation Protocol: Development and Validation of the 4C Mortality Score. BMJ 2020, 370, m3339. [Google Scholar] [CrossRef]
- Sun, H.; Jain, A.; Leone, M.J.; Alabsi, H.S.; Brenner, L.N.; Ye, E.; Ge, W.; Shao, Y.-P.; Boutros, C.L.; Wang, R.; et al. CoVA: An Acuity Score for Outpatient Screening That Predicts Coronavirus Disease 2019 Prognosis. J. Infect. Dis. 2021, 223, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Jehi, L.; Ji, X.; Milinovich, A.; Erzurum, S.; Merlino, A.; Gordon, S.; Young, J.B.; Kattan, M.W. Development and Validation of a Model for Individualized Prediction of Hospitalization Risk in 4536 Patients with COVID-19. PLoS ONE 2020, 15, e0237419. [Google Scholar] [CrossRef] [PubMed]
- Chao, H.; Fang, X.; Zhang, J.; Homayounieh, F.; Arru, C.D.; Digumarthy, S.R.; Babaei, R.; Mobin, H.K.; Mohseni, I.; Saba, L.; et al. Integrative Analysis for COVID-19 Patient Outcome Prediction. Med. Image Anal. 2021, 67, 101844. [Google Scholar] [CrossRef]
- Soto-Mota, A.; Marfil-Garza, B.A.; Martínez Rodríguez, E.; Barreto Rodríguez, J.O.; López Romo, A.E.; Alberti Minutti, P.; Alejandre Loya, J.V.; Pérez Talavera, F.E.; Ávila Cervera, F.J.; Velazquez Burciaga, A.; et al. The Low-harm Score for Predicting Mortality in Patients Diagnosed with COVID-19: A Multicentric Validation Study. J. Am. Coll. Emerg. Physicians Open 2020, 1, 1436–1443. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Wang, X.; Zhuang, X.; Wang, H.; Li, A.; Huang, L.; Zhang, X.; Xue, Y.; Wei, F.; Ma, C. Baseline Characteristics and Changes of Biomarkers in Disease Course Predict Prognosis of Patients with COVID-19. Intern. Emerg. Med. 2021, 16, 1165–1172. [Google Scholar] [CrossRef]
- Pilotto, A.; Azzini, M.; Cella, A.; Cenderello, G.; Castagna, A.; Pilotto, A.; Custureri, R.; Dini, S.; Farinella, S.T.; Ruotolo, G.; et al. The Multidimensional Prognostic Index (MPI) for the Prognostic Stratification of Older Inpatients with COVID-19: A Multicenter Prospective Observational Cohort Study. Arch. Gerontol. Geriatr. 2021, 95, 104415. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Ju, M.; Xie, R.; Yu, S.; Zheng, J.; Ma, G.; Liu, K.; Ma, J.; Yu, K.; Tu, G.; et al. Prognostic Accuracy of Early Warning Scores for Clinical Deterioration in Patients With COVID-19. Front. Med. 2021, 7, 1113. [Google Scholar] [CrossRef]
- van Dam, P.M.; Zelis, N.; Stassen, P.; van Twist, D.J.L.; de Leeuw, P.W.; van Kuijk, S.; Buijs, J. Validating the RISE UP Score for Predicting Prognosis in Patients with COVID-19 in the Emergency Department: A Retrospective Study. BMJ Open 2021, 11, e045141. [Google Scholar] [CrossRef]
- Pokeerbux, M.R.; Yelnik, C.M.; Faure, E.; Drumez, E.; Bruandet, A.; Labreuche, J.; Assaf, A.; Goffard, A.; Garabedian, C.; Poissy, J.; et al. National Early Warning Score to Predict Intensive Care Unit Transfer and Mortality in COVID-19 in a French Cohort. Int. J. Clin. Pract. 2021, 75, e14121. [Google Scholar] [CrossRef]
- Thakkar, S.; Arora, S.; Kumar, A.; Jaswaney, R.; Faisaluddin, M.; Ammad Ud Din, M.; Shariff, M.; Barssoum, K.; Patel, H.P.; Nirav, A.; et al. A Systematic Review of the Cardiovascular Manifestations and Outcomes in the Setting of Coronavirus-19 Disease. Clin. Med. Insights Cardiol. 2020, 14, 117954682097719. [Google Scholar] [CrossRef]
- Wijeratne, T.; Gillard Crewther, S.; Sales, C.; Karimi, L. COVID-19 Pathophysiology Predicts That Ischemic Stroke Occurrence Is an Expectation, Not an Exception—A Systematic Review. Front. Neurol. 2021, 11, 1759. [Google Scholar] [CrossRef]
- Izcovich, A.; Ragusa, M.A.; Tortosa, F.; Lavena Marzio, M.A.; Agnoletti, C.; Bengolea, A.; Ceirano, A.; Espinosa, F.; Saavedra, E.; Sanguine, V.; et al. Prognostic Factors for Severity and Mortality in Patients Infected with COVID-19: A Systematic Review. PLoS ONE 2020, 15, e0241955. [Google Scholar] [CrossRef] [PubMed]
- Tang, M.; Yu, X.-X.; Huang, J.; Gao, J.-L.; Cen, F.-L.; Xiao, Q.; Fu, S.-Z.; Yang, Y.; Xiong, B.; Pan, Y.-J.; et al. Clinical Diagnosis of Severe COVID-19: A Derivation and Validation of a Prediction Rule. World J. Clin. Cases 2021, 9, 2994. [Google Scholar] [CrossRef] [PubMed]
- Mosquera-Sulbaran, J.A.; Pedreañez, A.; Carrero, Y.; Callejas, D. C-reactive Protein as an Effector Molecule in Covid-19 Pathogenesis. Rev. Med. Virol. 2021, 31, e2221. [Google Scholar] [CrossRef] [PubMed]
- Pan, F.; Yang, L.; Li, Y.; Liang, B.; Li, L.; Ye, T.; Li, L.; Liu, D.; Gui, S.; Hu, Y.; et al. Factors Associated with Death Outcome in Patients with Severe Coronavirus Disease-19 (COVID-19): A Case-Control Study. Int. J. Med. Sci. 2020, 17, 1281. [Google Scholar] [CrossRef] [PubMed]
- Khinda, J.; Janjua, N.Z.; Cheng, S.; Heuvel, E.R.; Bhatti, P.; Darvishian, M. Association between Markers of Immune Response at Hospital Admission and COVID-19 Disease Severity and Mortality: A Meta-analysis and Meta-regression. J. Med. Virol. 2021, 93, 1078–1098. [Google Scholar] [CrossRef]
- Tjendra, Y.; al Mana, A.F.; Espejo, A.P.; Akgun, Y.; Millan, N.C.; Gomez-Fernandez, C.; Cray, C. Predicting Disease Severity and Outcome in COVID-19 Patients: A Review of Multiple Biomarkers. Arch. Pathol. Lab. Med. 2020, 144, 1465–1474. [Google Scholar] [CrossRef]
- Aziz, M.; Goyal, H.; Haghbin, H.; Lee-Smith, W.M.; Gajendran, M.; Perisetti, A. The Association of “Loss of Smell” to COVID-19: A Systematic Review and Meta-Analysis. Am. J. Med. Sci. 2021, 361, 216–225. [Google Scholar] [CrossRef]
- Wijeratne, T.; Sales, C.A.; Crewther, S.G.; Nguyen, V.; Karimi, L. First Australian Case of Good Recovery of a COVID-19 Patient With Severe Neurological Symptoms Post Prolonged Hospitalization. Cureus 2020, 12, e10366. [Google Scholar] [CrossRef]
- Wijeratne, T.; Wijeratne, C. Clinical Utility of Serial Systemic Immune Inflammation Indices (SSIIi) in the Context of Post COVID-19 Neurological Syndrome (PCNS). J. Neurol. Sci. 2021, 423, 117356. [Google Scholar] [CrossRef]
- Cacciapaglia, G.; Cot, C.; Sannino, F. Multiwave Pandemic Dynamics Explained: How to Tame the next Wave of Infectious Diseases. Sci. Rep. 2021, 11, 6638. [Google Scholar] [CrossRef] [PubMed]
- Schultz, M.J.; Gebremariam, T.H.; Park, C.; Pisani, L.; Sivakorn, C.; Taran, S.; Papali, A. Pragmatic Recommendations for the Use of Diagnostic Testing and Prognostic Models in Hospitalized Patients with Severe COVID-19 in Low- and Middle-Income Countries. Am. J. Trop. Med. Hyg. 2021, 104, 34–47. [Google Scholar] [CrossRef] [PubMed]
- Weinreich, D.M.; Sivapalasingam, S.; Norton, T.; Ali, S.; Gao, H.; Bhore, R.; Musser, B.J.; Soo, Y.; Rofail, D.; Im, J.; et al. REGN-COV2, a Neutralizing Antibody Cocktail, in Outpatients with COVID-19. N. Engl. J. Med. 2021, 384, 238–251. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Gonzalez-Rojas, Y.; Juarez, E.; Crespo Casal, M.; Moya, J.; Falci, D.R.; Sarkis, E.; Solis, J.; Zheng, H.; Scott, N.; et al. Early Treatment for COVID-19 with SARS-CoV-2 Neutralizing Antibody Sotrovimab. N. Engl. J. Med. 2021, 385, 1941–1950. [Google Scholar] [CrossRef]
- Lee, J.Y.; Lee, J.Y.; Ko, J.-H.; Hyun, M.; Kim, H.A.; Cho, S.; Lee, Y.D.; Song, J.; Shin, S.; Peck, K.R. Effectiveness of Regdanvimab Treatment in High-Risk COVID-19 Patients to Prevent Progression to Severe Disease. Front. Immunol. 2021, 12, 4998. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Baseline Characteristics | Mean (Range)/Total Number (Percentage) | SD |
|---|---|---|
| Demographics | ||
| Age (years) | 69 (23–95) | 15.7 |
| Sex (male) | 99 (64.2%) | |
| Clinical | ||
| Temperature (°C) | 38 (35.6–40) | 0.92 |
| SpO2 (%) | 92.3 (60–100) | 6.75 |
| Heart rate (bpm) | 85.7 (57–130) | 15.6 |
| Blood pressure (mmHg) | ||
| Systolic | 135.5 (72–236) | 23.5 |
| Diastolic | 73.7 (40–110) | 13.8 |
| Respiratory rate (cycles/Min) | 23.6 (8–40) | 6.3 |
| Altered smell or taste noted | 16 (10.4%) | |
| Infiltrates documented | 142 (92.2%) | |
| Laboratory | ||
| CRP (mg/L) | 97 (0.6–422) | 79.5 |
| LDH (U/L) | 382 (176–1166) | 176 |
| Lymphocyte count (109 cells/L) | 1.0 (0.1–2.7) | 0.465 |
| Medications administered | ||
| Antibiotics | 70 (45.6%) | |
| Dexamethason | 83 (53.9%) | |
| Remdesivir | 76 (49.4%) | |
| Outcomes | ||
| Ventilation (NIV, intubation) | 30 (19.5%) | |
| Exitus | 14 (9.1%) | |
| COVID-19 severity stages at admission according to Siddiqi & Mehra | ||
| Stage I | 13 (8.4%) | |
| Stage IIa | 35 (22.7%) | |
| Stage IIb | 80 (52%) | |
| Stage III | 26 (16.9%) | |
| Maximum COVID-19 severity stage during hospitalization | ||
| Stage I | 13 (8.4%) | |
| Stage IIa | 16 (10.4%) | |
| Stage IIb | 87 (56.5%) | |
| Stage III | 38 (24.7%) | |
| AIFELL scores at admission | ||
| 0 | 1 (0.66%) | |
| 1 | 1 (0.66%) | |
| 2 | 11 (7.1%) | |
| 3 | 43 (27.9%) | |
| 4 | 66 (42.9%) | |
| 5 | 31 (20.1%) | |
| 6 | 1 (0.66%) |
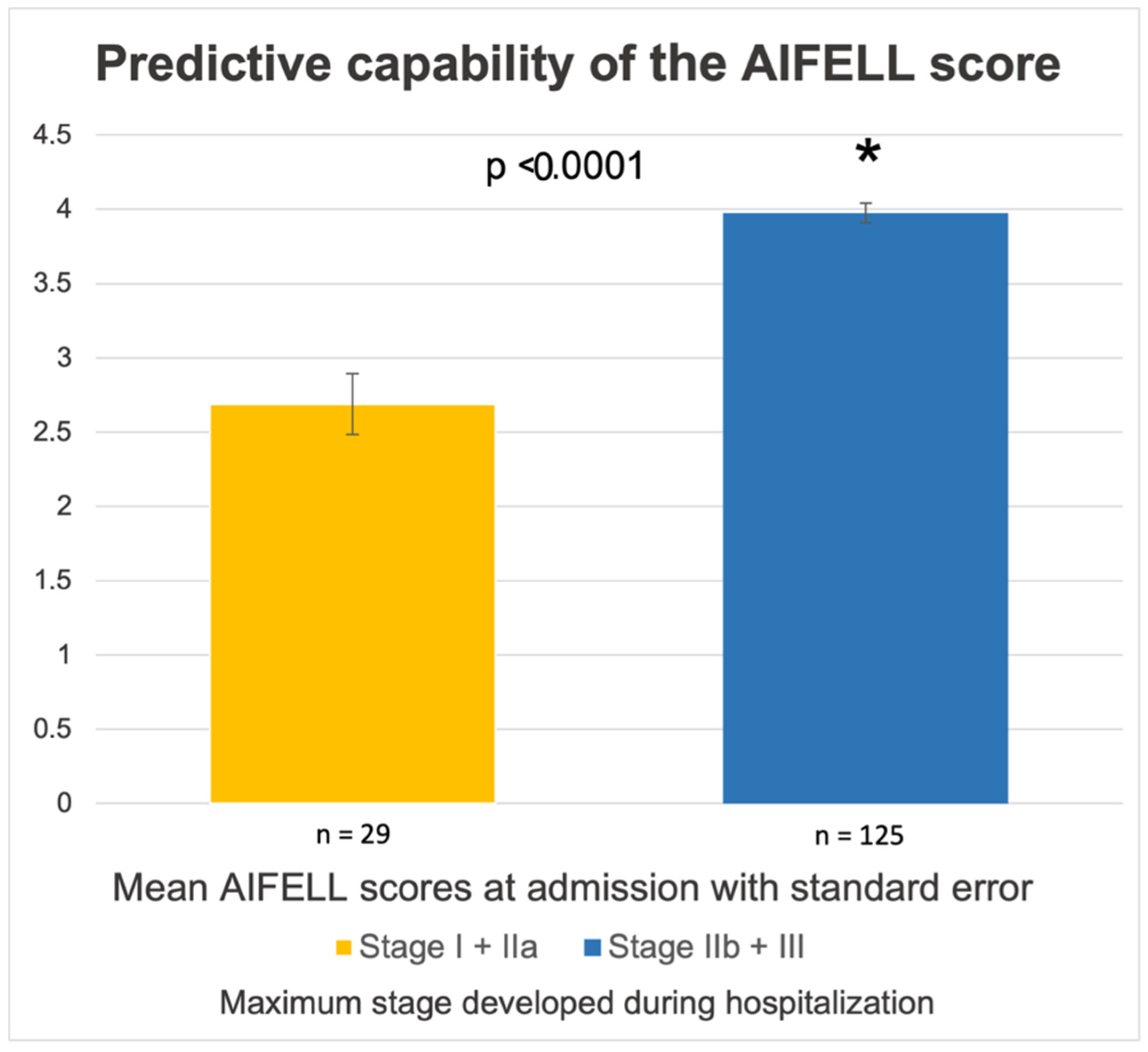
| Maximum COVID-19 Stage during Hospitalization | Average AIFELL Score at Admission | SD | Two-Tailed t-Test | p Value |
| Stage I | 2.08 | 0.86 | Stage I vs. IIa | 0.005 |
| Stage IIa | 3.2 | 0.05 | Stage I vs. II & III | <0.0001 |
| Stage IIb | 3.9 | 0.77 | Stage IIa vs. IIb | 0.002 |
| Stage III | 4.2 | 0.65 | Stage II vs. III | 0.008 |
| TOTAL | 3.73 | 0.96 |
| b | SEB | β | T | p | |
|---|---|---|---|---|---|
| AIFELL score | 0.677 | 0.146 | 0.352 | 4.632 | 0.000 *** |
| Parameter | ANOVA Time Effect | ANOVA Group Effect | ANOVA Time * Group Interaction | |||
|---|---|---|---|---|---|---|
| F | P | F | p | F | p | |
| AIFELL score | 8.101 | 0.005 ** | 19.867 | 0.000 *** | 1.276 | 0.26 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levenfus, I.; Ullmann, E.; Petrowski, K.; Rose, J.; Huber, L.C.; Stüssi-Helbling, M.; Schuurmans, M.M. The AIFELL Score as a Predictor of Coronavirus Disease 2019 (COVID-19) Severity and Progression in Hospitalized Patients. Diagnostics 2022, 12, 604. https://doi.org/10.3390/diagnostics12030604
Levenfus I, Ullmann E, Petrowski K, Rose J, Huber LC, Stüssi-Helbling M, Schuurmans MM. The AIFELL Score as a Predictor of Coronavirus Disease 2019 (COVID-19) Severity and Progression in Hospitalized Patients. Diagnostics. 2022; 12(3):604. https://doi.org/10.3390/diagnostics12030604
Chicago/Turabian StyleLevenfus, Ian, Enrico Ullmann, Katja Petrowski, Jutta Rose, Lars C. Huber, Melina Stüssi-Helbling, and Macé M. Schuurmans. 2022. "The AIFELL Score as a Predictor of Coronavirus Disease 2019 (COVID-19) Severity and Progression in Hospitalized Patients" Diagnostics 12, no. 3: 604. https://doi.org/10.3390/diagnostics12030604