
Modified Glasgow Prognostic Score as a Predictor of Recurrence in Patients with High Grade Non-Muscle Invasive Bladder Cancer Undergoing Intravesical Bacillus Calmette–Guerin Immunotherapy

 , , , ,
, , , ,  ,
,  , , , , , ,
, , , , , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Follow-Up
2.2. Statistical Methods
3. Results
3.1. Clinical and Pathological Features for the Whole Cohort of Patients
3.2. Association of Clinical and Pathologic Features with mGPS in 1382 Patients Treated with BCG after Primary HG/G3 T1 NMIBC Included in Follow-Up
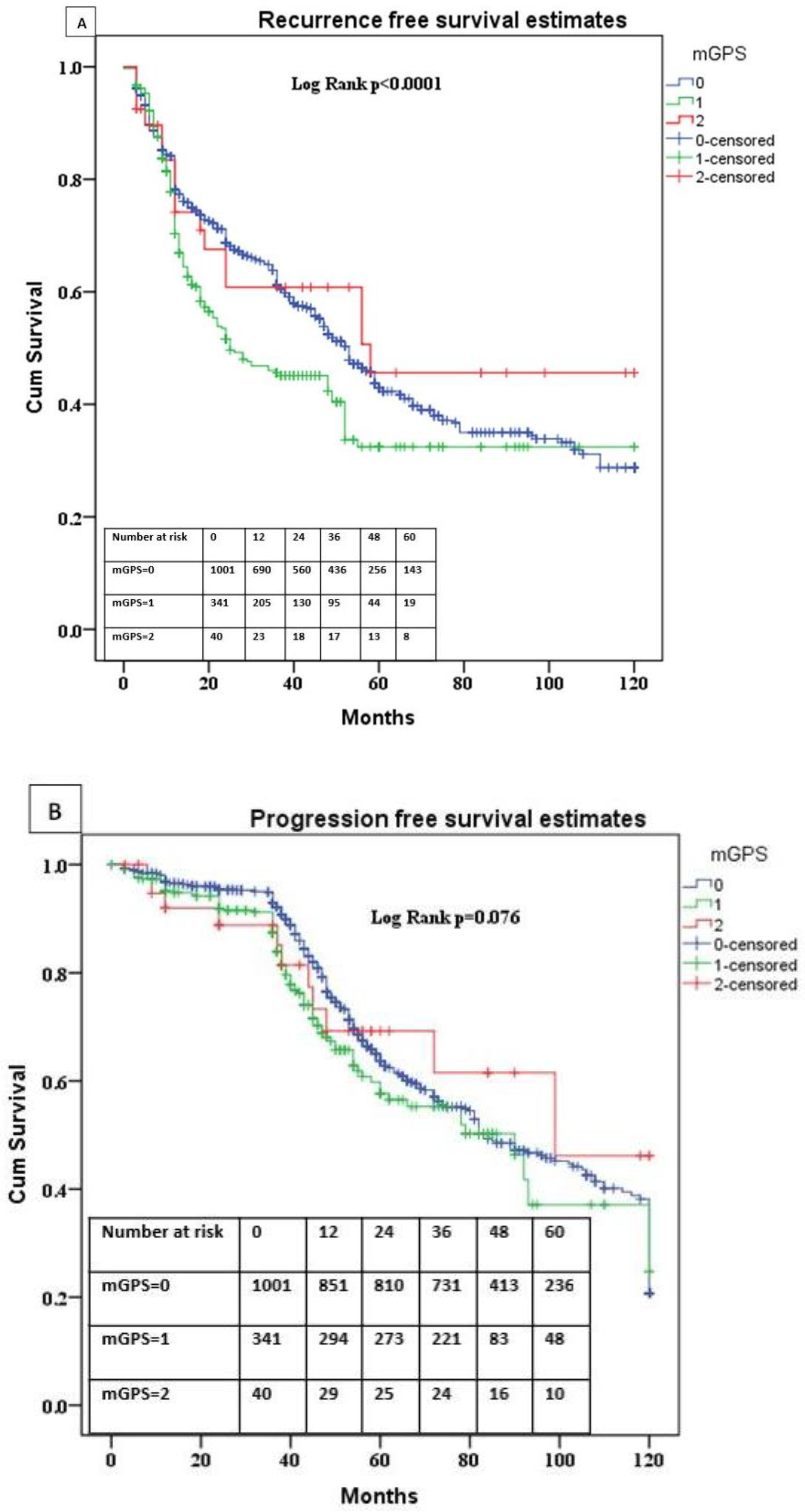
3.3. Association of mGPS with Recurrence and Progression
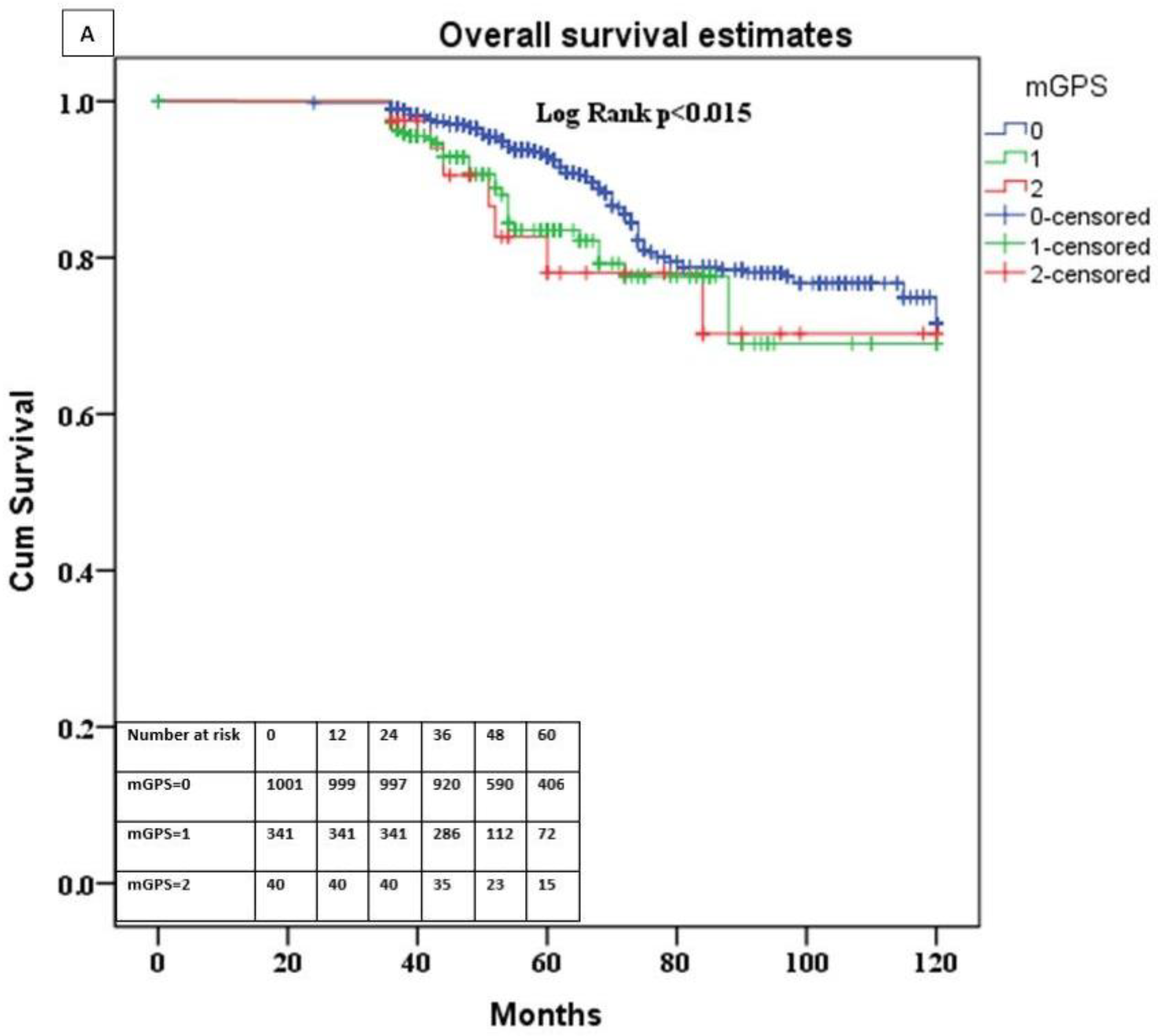
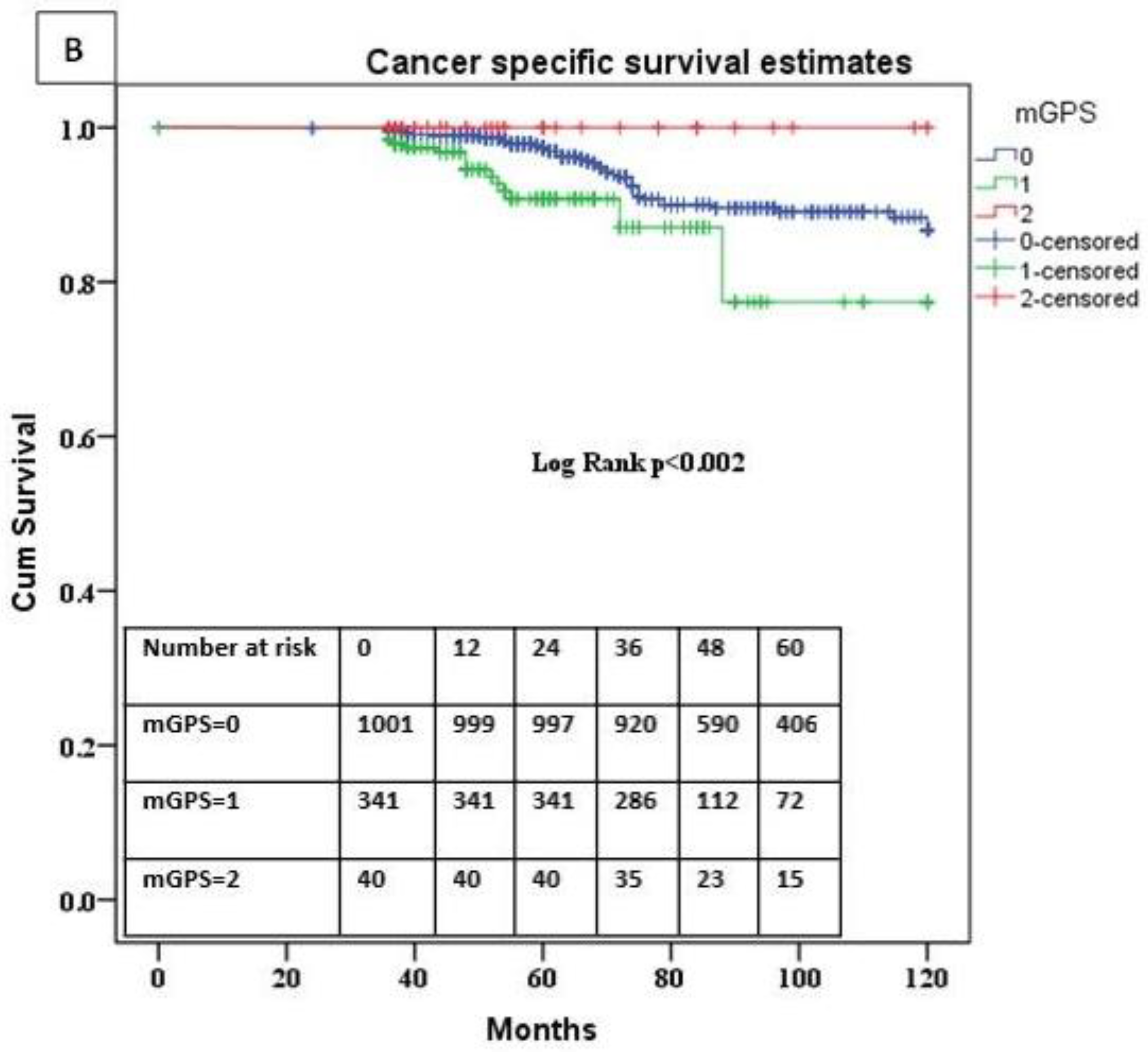
3.4. Association of the mGPS with Overall and Cancer-Specific Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Thun, M.; Linet, M.S.; Cerhan, J.R.; Haiman, C.A.; Schottenfeld, D. Cancer Epidemiology and Prevention; Oxford University Press: Oxford, UK, 2017; ISBN 0-19-023867-4. [Google Scholar]
- Antoni, S.; Ferlay, J.; Soerjomataram, I.; Znaor, A.; Jemal, A.; Bray, F. Bladder Cancer Incidence and Mortality: A Global Overview and Recent Trends. Eur. Urol. 2017, 71, 96–108. [Google Scholar] [CrossRef]
- Sylvester, R.J.; van der Meijden, A.P.M.; Oosterlinck, W.; Witjes, J.A.; Bouffioux, C.; Denis, L.; Newling, D.W.W.; Kurth, K. Predicting Recurrence and Progression in Individual Patients with Stage Ta T1 Bladder Cancer Using EORTC Risk Tables: A Combined Analysis of 2596 Patients from Seven EORTC Trials. Eur. Urol. 2006, 49, 466–477. [Google Scholar] [CrossRef] [PubMed]
- Rieken, M.; Shariat, S.F.; Kluth, L.; Crivelli, J.J.; Abufaraj, M.; Foerster, B.; Mari, A.; Ilijazi, D.; Karakiewicz, P.I.; Babjuk, M.; et al. Comparison of the EORTC Tables and the EAU Categories for Risk Stratification of Patients with Nonmuscle-Invasive Bladder Cancer. Urol. Oncol. 2018, 36, 8.e17–8.e24. [Google Scholar] [CrossRef]
- Fernandez-Gomez, J.; Madero, R.; Solsona, E.; Unda, M.; Martinez-Piñeiro, L.; Gonzalez, M.; Portillo, J.; Ojea, A.; Pertusa, C.; Rodriguez-Molina, J.; et al. Predicting Nonmuscle Invasive Bladder Cancer Recurrence and Progression in Patients Treated with Bacillus Calmette-Guerin: The CUETO Scoring Model. J. Urol. 2009, 182, 2195–2203. [Google Scholar] [CrossRef]
- Cambier, S.; Sylvester, R.J.; Collette, L.; Gontero, P.; Brausi, M.A.; van Andel, G.; Kirkels, W.J.; Silva, F.C.D.; Oosterlinck, W.; Prescott, S.; et al. EORTC Nomograms and Risk Groups for Predicting Recurrence, Progression, and Disease-Specific and Overall Survival in Non-Muscle-Invasive Stage Ta-T1 Urothelial Bladder Cancer Patients Treated with 1–3 Years of Maintenance Bacillus Calmette-Guérin. Eur. Urol. 2016, 69, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Uhlig, A.; Strauss, A.; Seif Amir Hosseini, A.; Lotz, J.; Trojan, L.; Schmid, M.; Uhlig, J. Gender-Specific Differences in Recurrence of Non-Muscle-Invasive Bladder Cancer: A Systematic Review and Meta-Analysis. Eur. Urol. Focus 2018, 4, 924–936. [Google Scholar] [CrossRef]
- Ferro, M.; Vartolomei, M.D.; Russo, G.I.; Cantiello, F.; Farhan, A.R.A.; Terracciano, D.; Cimmino, A.; Di Stasi, S.; Musi, G.; Hurle, R.; et al. An Increased Body Mass Index Is Associated with a Worse Prognosis in Patients Administered BCG Immunotherapy for T1 Bladder Cancer. World J. Urol. 2019, 37, 507–514. [Google Scholar] [CrossRef]
- Vartolomei, M.D.; Porav-Hodade, D.; Ferro, M.; Mathieu, R.; Abufaraj, M.; Foerster, B.; Kimura, S.; Shariat, S.F. Prognostic Role of Pretreatment Neutrophil-to-Lymphocyte Ratio (NLR) in Patients with Non-Muscle-Invasive Bladder Cancer (NMIBC): A Systematic Review and Meta-Analysis. Urol. Oncol. 2018, 36, 389–399. [Google Scholar] [CrossRef]
- Vartolomei, M.D.; Ferro, M.; Cantiello, F.; Lucarelli, G.; Di Stasi, S.; Hurle, R.; Guazzoni, G.; Busetto, G.M.; De Berardinis, E.; Damiano, R.; et al. Validation of Neutrophil-to-Lymphocyte Ratio in a Multi-Institutional Cohort of Patients with T1G3 Non-Muscle-Invasive Bladder Cancer. Clin. Genitourin. Cancer 2018, 16, 445–452. [Google Scholar] [CrossRef]
- Lenis, A.T.; Asanad, K.; Blaibel, M.; Donin, N.M.; Chamie, K. Association between Metabolic Syndrome and Recurrence of Nonmuscle Invasive Bladder Cancer Following Bacillus Calmette-Guérin Treatment. Urol. Pract. 2018, 5, 132–138. [Google Scholar] [CrossRef] [Green Version]
- Werntz, R.P.; Smith, Z.L.; Packiam, V.T.; Smith, N.; Steinberg, G.D. The Impact of Lymphovascular Invasion on Risk of Upstaging and Lymph Node Metastasis at the Time of Radical Cystectomy. Eur. Urol. Focus 2020, 6, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Muppa, P.; Gupta, S.; Frank, I.; Boorjian, S.A.; Karnes, R.J.; Thompson, R.H.; Thapa, P.; Tarrell, R.F.; Herrera Hernandez, L.P.; Jimenez, R.E.; et al. Prognostic Significance of Lymphatic, Vascular and Perineural Invasion for Bladder Cancer Patients Treated by Radical Cystectomy. Pathology 2017, 49, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Chou, W.-C.; Yeh, K.-Y.; Peng, M.-T.; Chen, J.-S.; Wang, H.-M.; Lin, Y.-C.; Liu, C.-T.; Li, S.-H.; Chang, P.-H.; Wang, C.-H.; et al. Development and Validation of a Prognostic Score to Predict Survival in Adult Patients with Solid Tumors and Bone Marrow Metastases. Medicine 2015, 94, e966. [Google Scholar] [CrossRef] [PubMed]
- Hilmy, M.; Campbell, R.; Bartlett, J.M.S.; McNicol, A.-M.; Underwood, M.A.; McMillan, D.C. The Relationship between the Systemic Inflammatory Response, Tumour Proliferative Activity, T-Lymphocytic Infiltration and COX-2 Expression and Survival in Patients with Transitional Cell Carcinoma of the Urinary Bladder. Br. J. Cancer 2006, 95, 1234–1238. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, S.; Saito, K.; Koga, F.; Yokoyama, M.; Kageyama, Y.; Masuda, H.; Kobayashi, T.; Kawakami, S.; Kihara, K. C-Reactive Protein Level Predicts Prognosis in Patients with Muscle-Invasive Bladder Cancer Treated with Chemoradiotherapy. BJU Int. 2008, 101, 978–981. [Google Scholar] [CrossRef] [PubMed]
- Gakis, G.; Todenhöfer, T.; Renninger, M.; Schilling, D.; Sievert, K.-D.; Schwentner, C.; Stenzl, A. Development of a New Outcome Prediction Model in Carcinoma Invading the Bladder Based on Preoperative Serum C-Reactive Protein and Standard Pathological Risk Factors: The TNR-C Score. BJU Int. 2011, 108, 1800–1805. [Google Scholar] [CrossRef] [PubMed]
- Miyake, M.; Morizawa, Y.; Hori, S.; Marugami, N.; Iida, K.; Ohnishi, K.; Gotoh, D.; Tatsumi, Y.; Nakai, Y.; Inoue, T.; et al. Integrative Assessment of Pretreatment Inflammation-, Nutrition-, and Muscle-Based Prognostic Markers in Patients with Muscle-Invasive Bladder Cancer Undergoing Radical Cystectomy. Oncology 2017, 93, 259–269. [Google Scholar] [CrossRef]
- Kikuchi, K.; Nakamura, R.; Segawa, T.; Oikawa, H.; Ariga, H. Modified Glasgow Prognostic Score Can Predict Survival of Muscle Invasive Bladder Cancer Patients after Radiotherapy. J. Radiat. Res. 2020, 61, 616–621. [Google Scholar] [CrossRef]
- Guo, Y.; Cai, K.; Mao, S.; Zhang, J.; Wang, L.; Zhang, Z.; Liu, M.; Zhang, W.; Wu, Y.; Yan, Y.; et al. Preoperative C-Reactive Protein/Albumin Ratio Is a Significant Predictor of Survival in Bladder Cancer Patients after Radical Cystectomy: A Retrospective Study. Cancer Manag. Res. 2018, 10, 4789–4804. [Google Scholar] [CrossRef] [Green Version]
- Qayyum, T.; McArdle, P.; Hilmy, M.; Going, J.; Orange, C.; Seywright, M.; Horgan, P.; Underwood, M.; Edwards, J. A Prospective Study of the Role of Inflammation in Bladder Cancer. Curr. Urol. 2013, 6, 189–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuettfort, V.M.; D’Andrea, D.; Quhal, F.; Mostafaei, H.; Laukhtina, E.; Mori, K.; König, F.; Rink, M.; Abufaraj, M.; Karakiewicz, P.I.; et al. A Panel of Systemic Inflammatory Response Biomarkers for Outcome Prediction in Patients Treated with Radical Cystectomy for Urothelial Carcinoma. BJU Int. 2021, 129, 182–193. [Google Scholar] [CrossRef] [PubMed]
- Albisinni, S.; Moussa, I.; Aoun, F.; Quackels, T.; Assenmacher, G.; Peltier, A.; Roumeguère, T. The Impact of Postoperative Inflammatory Biomarkers on Oncologic Outcomes of Bladder Cancer. Prog. Urol. 2019, 29, 270–281. [Google Scholar] [CrossRef] [PubMed]
- Mbeutcha, A.; Shariat, S.F.; Rieken, M.; Rink, M.; Xylinas, E.; Seitz, C.; Lucca, I.; Mathieu, R.; Rouprêt, M.; Briganti, A.; et al. Prognostic Significance of Markers of Systemic Inflammatory Response in Patients with Non-Muscle-Invasive Bladder Cancer. Urol. Oncol. 2016, 34, 483.e17–483.e24. [Google Scholar] [CrossRef]
- Kimura, S.; D’ Andrea, D.; Soria, F.; Foerster, B.; Abufaraj, M.; Vartolomei, M.D.; Iwata, T.; Karakiewicz, P.I.; Rink, M.; Gust, K.M.; et al. Prognostic Value of Modified Glasgow Prognostic Score in Non-Muscle-Invasive Bladder Cancer. Urol. Oncol. 2019, 37, 179.e19–179.e28. [Google Scholar] [CrossRef]
- Ferro, M.; Di Mauro, M.; Cimino, S.; Morgia, G.; Lucarelli, G.; Abu Farhan, A.R.; Vartolomei, M.D.; Porreca, A.; Cantiello, F.; Damiano, R.; et al. Systemic Combining Inflammatory Score (SCIS): A New Score for Prediction of Oncologic Outcomes in Patients with High-Risk Non-Muscle-Invasive Urothelial Bladder Cancer. Transl. Androl. Urol. 2021, 10, 626–635. [Google Scholar] [CrossRef]
- Babjuk, M.; Böhle, A.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Hernández, V.; Kaasinen, E.; Palou, J.; Rouprêt, M.; et al. EAU Guidelines on Non-Muscle-Invasive Urothelial Carcinoma of the Bladder: Update 2016. Eur. Urol. 2017, 71, 447–461. [Google Scholar] [CrossRef]
- Proctor, M.J.; Horgan, P.G.; Talwar, D.; Fletcher, C.D.; Morrison, D.S.; McMillan, D.C. Optimization of the Systemic Inflammation-Based Glasgow Prognostic Score: A Glasgow Inflammation Outcome Study. Cancer 2013, 119, 2325–2332. [Google Scholar] [CrossRef]
- Kamat, A.M.; Sylvester, R.J.; Böhle, A.; Palou, J.; Lamm, D.L.; Brausi, M.; Soloway, M.; Persad, R.; Buckley, R.; Colombel, M.; et al. Definitions, End Points, and Clinical Trial Designs for Non-Muscle-Invasive Bladder Cancer: Recommendations from the International Bladder Cancer Group. J. Clin. Oncol. 2016, 34, 1935–1944. [Google Scholar] [CrossRef]
- Babjuk, M.; Burger, M.; Compérat, E.M.; Gontero, P.; Mostafid, A.H.; Palou, J.; van Rhijn, B.W.G.; Rouprêt, M.; Shariat, S.F.; Sylvester, R.; et al. European Association of Urology Guidelines on Non-Muscle-Invasive Bladder Cancer (TaT1 and Carcinoma In Situ)—2019 Update. Eur. Urol. 2019, 76, 639–657. [Google Scholar] [CrossRef]
- Ferro, M.; De Cobelli, O.; Buonerba, C.; Di Lorenzo, G.; Capece, M.; Bruzzese, D.; Autorino, R.; Bottero, D.; Cioffi, A.; Matei, D.V.; et al. Modified Glasgow Prognostic Score Is Associated with Risk of Recurrence in Bladder Cancer Patients after Radical Cystectomy: A Multicenter Experience. Medicine 2015, 94, e1861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuk, H.D.; Jeong, C.W.; Kwak, C.; Kim, H.H.; Ku, J.H. Elevated Neutrophil to Lymphocyte Ratio Predicts Poor Prognosis in Non-Muscle Invasive Bladder Cancer Patients: Initial Intravesical Bacillus Calmette-Guerin Treatment after Transurethral Resection of Bladder Tumor Setting. Front. Oncol. 2018, 8, 642. [Google Scholar] [CrossRef] [PubMed]
- Wigner, P.; Grębowski, R.; Bijak, M.; Saluk-Bijak, J.; Szemraj, J. The Interplay between Oxidative Stress, Inflammation and Angiogenesis in Bladder Cancer Development. Int. J. Mol. Sci. 2021, 22, 4483. [Google Scholar] [CrossRef] [PubMed]
- Andrade, D.L.; Moretti, T.B.C.; Neto, W.A.; Benedetti, J.; Reis, L.O. Smoke Load Prognostic Impact on Bacillus Calmette-Guérin (BCG) Treated Non-Muscle Invasive Bladder Cancer. Int. Urol. Nephrol. 2020, 52, 1471–1476. [Google Scholar] [CrossRef]
- Abern, M.R.; Owusu, R.A.; Anderson, M.R.; Rampersaud, E.N.; Inman, B.A. Perioperative Intravesical Chemotherapy in Non-Muscle-Invasive Bladder Cancer: A Systematic Review and Meta-Analysis. J. Natl. Compr. Cancer Netw. 2013, 11, 477–484. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Overall Cohort (n = 1382) | |
|---|---|
| Age (years) | 69.87 ± 9.71 |
| Gender (males/females) | 1115/267 = 80.7%/19.3% |
| BMI (kg/m2) | 26.8 ± 3.79 |
| Smoking status | |
| Yes | 784 (56.7%) |
| No | 598 (43.3%) |
| Number of cigarettes/day | 10 (0–65) |
| Number of years of smoking | 20 (0–70) |
| Multifocality-yes | 605 (43.8%) |
| Tumor size > 3 cm | 887 (64.2%) |
| Concomitant CIS | 224 (16.2%) |
| LVI | 212 (15.3%) |
| LVI at re-TURB | 85 (6.2%) |
| ESR (mm/h) | 12 (1–109) |
| CRP (mg/dL) | 2 (0.01–125.0) |
| Albumin (g/dL) | 4.17 ± 0.52 |
| mGPS | |
| 0 | 1001 (72.4%) |
| 1 | 341 (24.7%) |
| 2 | 40 (2.9%) |
| mGPS 0 | mGPS 1 | mGPS 2 | p Value | |
|---|---|---|---|---|
| Total, n (%) | 1001 (72.4%) | 341 (24.7%) | 40 (2.9%) | - |
| Age (years) Mean (SD) | 69.97 ± 9.68 | 69.74 ± 9.62 | 68.65 ± 11.24 | 0.56 * |
| Gender, n (%) | ||||
| Male | 810 (72.6%) | 277 (24.8%) | 28 (2.5%) | 0.20 ** |
| Female | 191 (71.8%) | 63 (23.7%) | 12 (4.5%) | |
| Smoking status | ||||
| Yes | 285 (73.1%) | 89 (22.8%) | 16 (4.1%) | 0.001 ** |
| No | 404 (67.6%) | 180 (30.1%) | 14 (2.3%) | |
| Multifocality, n (%) | ||||
| Unifocal | 587 (75.5%) | 170 (21.9%) | 20 (2.6%) | 0.014 ** |
| Multifocal | 414 (68.4%) | 171 (28.3%) | 20 (3.3%) | |
| Size, n (%) | ||||
| <3 cm | 381 (77.0%) | 99 (20.0%) | 15 (3.0%) | 0.011 ** |
| ≥3 cm | 620 (69.9%) | 242 (27.3%) | 25 (2.8%) | |
| Concomitant CIS, n (%) | ||||
| Yes | 165 (73.7%) | 54 (24.1%) | 5 (2.2%) | 0.76 ** |
| No | 836 (72.2%) | 287 (24.8%) | 35 (3.0%) | |
| Survival outcomes | ||||
| Recurrence, n (%) | ||||
| Yes | 470 (71.3%) | 173 (26.3%) | 16 (2.4%) | 0.30 ** |
| No | 531 (73.4%) | 168 (23.2%) | 24 (3.3%) | |
| Progression, n (%) | ||||
| Yes | 332 (75.3%) | 98 (22.2%) | 11 (2.5%) | 0.27 ** |
| No | 669 (71.1%) | 243 (25.8%) | 29 (3.1%) | |
| Death | 113 (72.4%) | 36 (23.1%) | 7 (4.5%) | 0.43 ** |
| Death due to BC | 47 (70.1%) | 20 (29.9%) | 0 (0.0%) | 0.22 ** |
| Variables | Recurrence-Free Survival | |||||
|---|---|---|---|---|---|---|
| Univariable | Multivariable | |||||
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Age cont. | 0.840 | 0.716–0.986 | 0.033 | 1.167 | 0.965–1.411 | 0.112 |
| Gender (male vs. female) | 1.074 | 0.980–1.177 | 0.125 | 0.82 | 0.656–1.022 | 0.078 |
| Size (<3 vs. ≥3) cm | 1.154 | 1.082–1.355 | 0.042 | 0.984 | 0.815–1.189 | 0.870 |
| Multifocality (single vs. multiple) | 1.177 | 1.009–1.373 | 0.038 | 1.146 | 0.953–1.379 | 0.147 |
| Concomitant CIS (no vs. yes) | 1.138 | 0.932–1.389 | 0.201 | 0.906 | 0.715–1.149 | 0.416 |
| NLR | 6.864 | 5.234–9.002 | 0.001 | 7.471 | 5.394–10.346 | 0.0001 |
| ESR (mm/h) | 0.911 | 0.768–1.080 | 0.282 | 0.706 | 0.628–0.924 | 0.006 |
| mGPS | ||||||
| 0 | ref | |||||
| 1 | 1.403 | 1.177–1.673 | 0.0001 | 1.417 | 1.187–1.692 | 0.0001 |
| 2 | 0.853 | 0.518–1.404 | 0.531 | 1.239 | 0.813–2.328 | 0.321 |
| Variables | Progression-Free Survival | |||||
|---|---|---|---|---|---|---|
| Univariable | Multivariable | |||||
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Age cont. | 0.749 | 0.585–0.959 | 0.022 | 1.085 | 0.859–1.370 | 0.493 |
| Gender (male vs. female) | 0.960 | 0.849–1.085 | 0.509 | 0.864 | 0.649–1.149 | 0.314 |
| Size (<3 vs. ≥3) cm | 1.136 | 0.934–1.382 | 0.201 | 1.078 | 0.862–1.347 | 0.512 |
| Multifocality (single vs. multiple) | 1.195 | 0.987–1.447 | 0.067 | 1.217 | 0.976–1.518 | 0.081 |
| Concomitant CIS (no vs. yes) | 1.243 | 1.068–1.595 | 0.044 | 1.065 | 0.798–1.422 | 0.667 |
| NLR | 1.010 | 0.827–1.240 | 0.904 | 1.014 | 0.800–1.285 | 0.909 |
| ESR (mm/h) | 1.173 | 0.969–1.421 | 0.102 | 0.692 | 0.532–0.874 | 0.003 |
| mGPS | ||||||
| 0 | ref | |||||
| 1 | 1.324 | 1.044–1.663 | 0.015 | 1.361 | 1.072–1.727 | 0.011 |
| 2 | 0.869 | 0.477–1.586 | 0.648 | 0.899 | 0.492–1.645 | 0.731 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferro, M.; Tătaru, O.S.; Musi, G.; Lucarelli, G.; Abu Farhan, A.R.; Cantiello, F.; Damiano, R.; Hurle, R.; Contieri, R.; Busetto, G.M.; et al. Modified Glasgow Prognostic Score as a Predictor of Recurrence in Patients with High Grade Non-Muscle Invasive Bladder Cancer Undergoing Intravesical Bacillus Calmette–Guerin Immunotherapy. Diagnostics 2022, 12, 586. https://doi.org/10.3390/diagnostics12030586
Ferro M, Tătaru OS, Musi G, Lucarelli G, Abu Farhan AR, Cantiello F, Damiano R, Hurle R, Contieri R, Busetto GM, et al. Modified Glasgow Prognostic Score as a Predictor of Recurrence in Patients with High Grade Non-Muscle Invasive Bladder Cancer Undergoing Intravesical Bacillus Calmette–Guerin Immunotherapy. Diagnostics. 2022; 12(3):586. https://doi.org/10.3390/diagnostics12030586
Chicago/Turabian StyleFerro, Matteo, Octavian Sabin Tătaru, Gennaro Musi, Giuseppe Lucarelli, Abdal Rahman Abu Farhan, Francesco Cantiello, Rocco Damiano, Rodolfo Hurle, Roberto Contieri, Gian Maria Busetto, and et al. 2022. "Modified Glasgow Prognostic Score as a Predictor of Recurrence in Patients with High Grade Non-Muscle Invasive Bladder Cancer Undergoing Intravesical Bacillus Calmette–Guerin Immunotherapy" Diagnostics 12, no. 3: 586. https://doi.org/10.3390/diagnostics12030586