
SARS-CoV-2 Sero-Surveillance in Greece: Evolution over Time and Epidemiological Attributes during the Pre-Vaccination Pandemic Era

 , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Laboratory Analysis
2.3. Statistical Analysis and Calculation of Indicators
2.3.1. Weighted Prevalence
2.3.2. Effective Sample Size
2.3.3. Estimation of Actual Infections Based on Seroprevalence Data
2.3.4. Calculation of Case Fatality Ratio and Infection Fatality Ratio
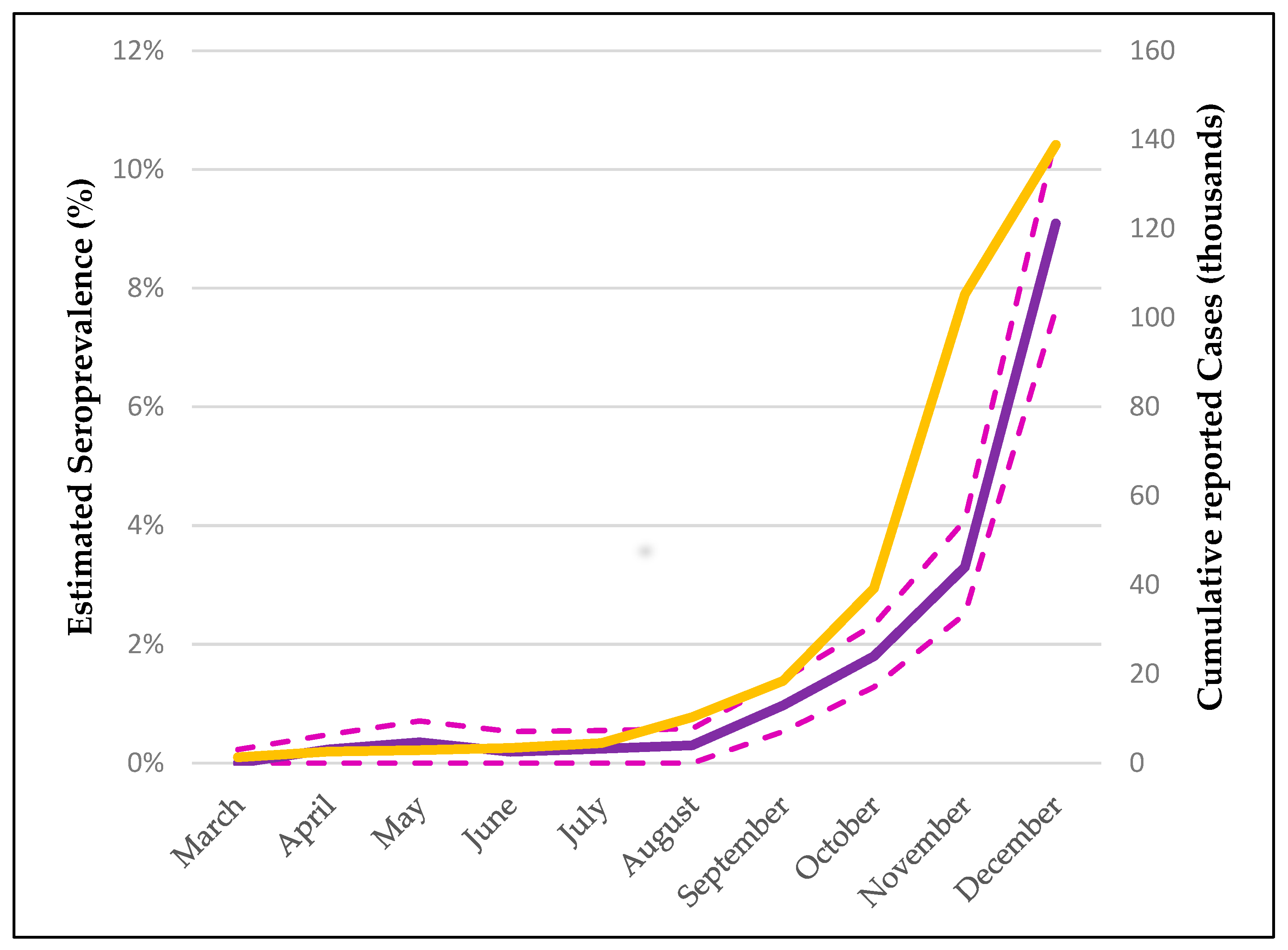
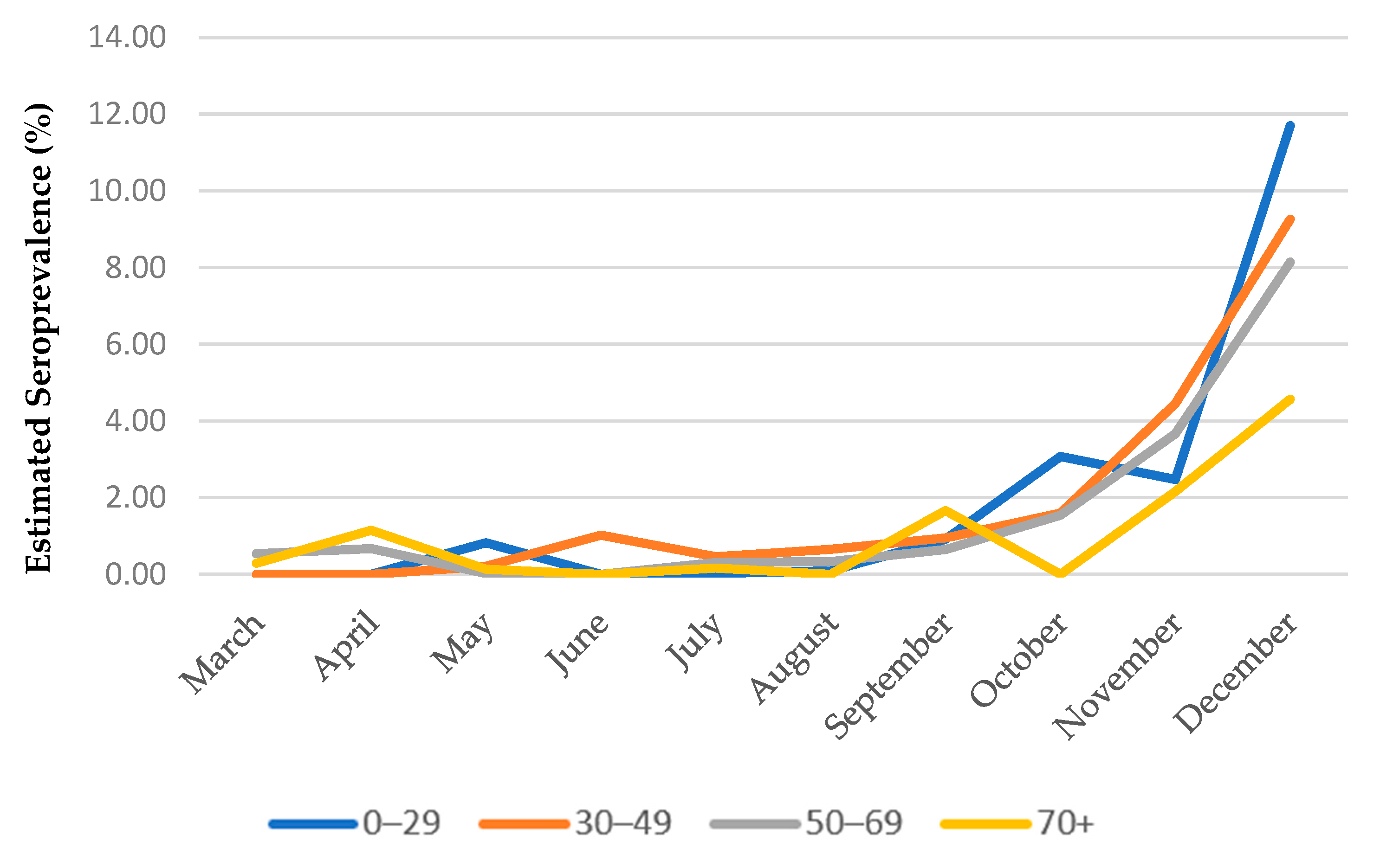
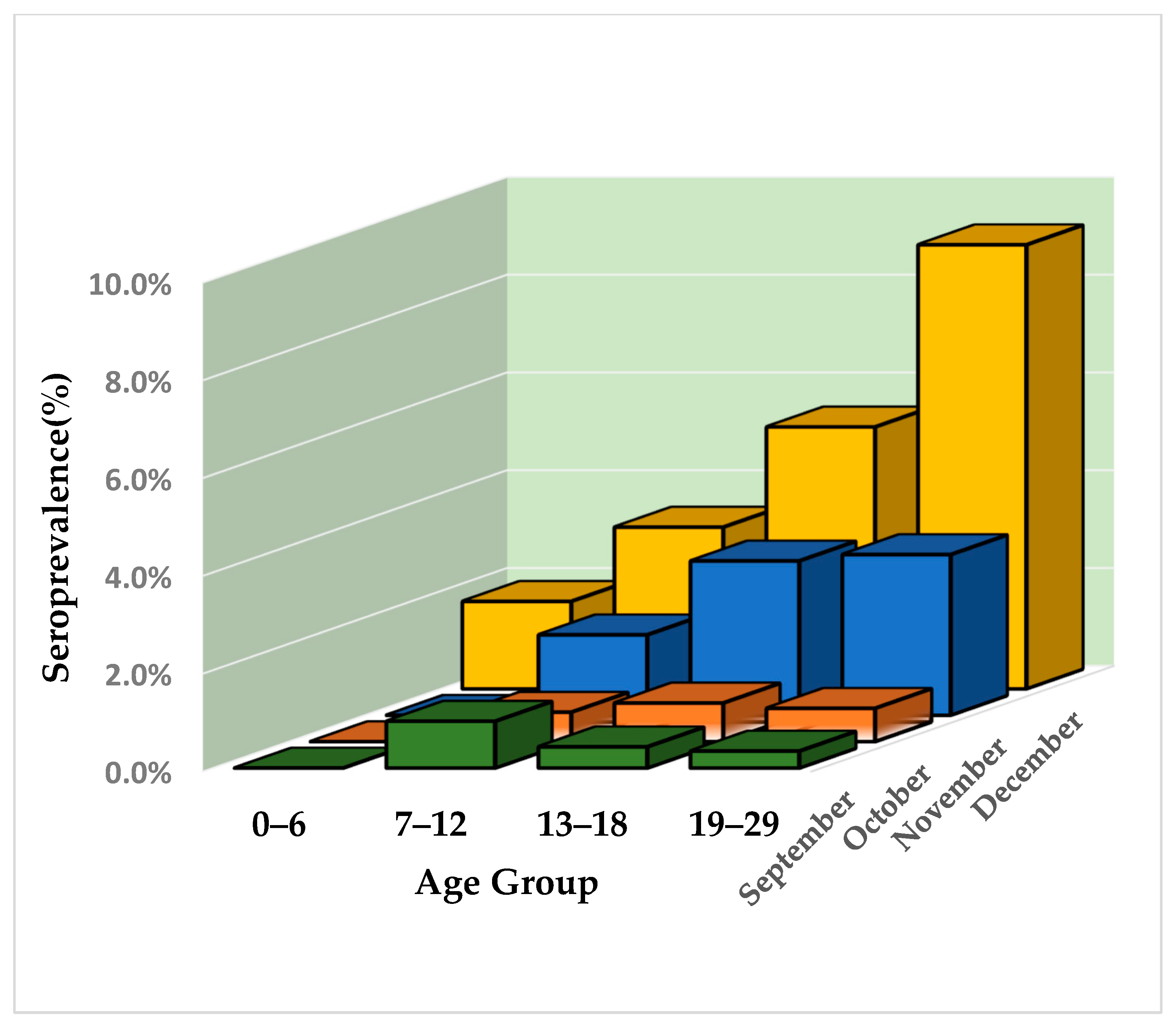
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B

{kind=link}
{kind=link}
{kind=link}
| Probability of Remaining IgG Positive (Months Since Seroconvertion) | Probability of Seroreversion (Months Since Seroconvertion) | ||
|---|---|---|---|
| P1(0) | 100.0% | P2(0) | 0.0% |
| P1(1) | 84.7% | P2(1) | 15.3% |
| P1(2) | 71.8% | P2(2) | 28.2% |
| P1(3) | 60.9% | P2(3) | 39.1% |
| P1(4) | 51.6% | P2(4) | 48.4% |
| P1(5) | 43.7% | P2(5) | 56.3% |
| P1(6) | 37.0% | P2(6) | 63.0% |
| P1(7) | 31.4% | P2(7) | 68.6% |
| P1(8) | 26.6% | P2(8) | 73.4% |
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/region/euro/country/gr (accessed on 18 December 2021).
- Huff, H.V.; Singh, A. Asymptomatic Transmission During the Coronavirus Disease 2019 Pandemic and Implications for Public Health Strategies. Clin. Infect. Dis. 2020, 71, 2752–2756. [Google Scholar] [CrossRef] [PubMed]
- Byambasuren, O.; Dobler, C.C.; Bell, K.; Rojas, D.P.; Clark, J.; McLaws, M.L.; Glasziou, P. Comparison of seroprevalence of SARS-CoV-2 infections with cumulative and imputed COVID-19 cases: Systematic review. PLoS ONE 2021, 16, e0248946. [Google Scholar] [CrossRef] [PubMed]
- European Center for Disease Perevention and Control (ECDC). COVID-19 Surveillance Guidance. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/COVID-19-surveillance-guidance.pdf (accessed on 27 December 2021).
- Arora, R.K.; Joseph, A.; Van Wyk, J.; Rocco, S.; Atmaja, A.; May, E.; Yan, T.; Bobrovitz, N.; Chevrier, J.; Cheng, M.P.; et al. SeroTracker: A global SARS-CoV-2 seroprevalence dashboard. Lancet Infect. Dis. 2021, 21, e75–e76. [Google Scholar] [CrossRef]
- Bogogiannidou, Z.; Speletas, M.; Vontas, A.; Nikoulis, D.J.; Dadouli, K.; Kyritsi, M.A.; Mouchtouri, V.A.; Mina, P.; Anagnostopoulos, L.; Koureas, M.; et al. Repeated leftover serosurvey of sars-cov-2 igg antibodies in greece, may to august 2020. Vaccines 2021, 9, 504. [Google Scholar] [CrossRef] [PubMed]
- Bogogiannidou, Z.; Vontas, A.; Dadouli, K.; Kyritsi, M.A.; Soteriades, S.; Nikoulis, D.J.; Mouchtouri, V.; Koureas, M.; Kazakos, E.I.; Spanos, E.G.; et al. Repeated leftover serosurvey of SARS-CoV-2 IgG antibodies, Greece, March and April 2020. Euro Surveill. Bull. Eur. Sur Les Mal. Transm. Eur. Commun. Dis. Bull. 2020, 25. [Google Scholar] [CrossRef] [PubMed]
- Nardone, A.; Miller, E. Serological surveillance of rubella in Europe: European Sero-Epidemiology Network (ESEN2). Euro Surveill. Bull. Eur. Sur Les Mal. Transm. Eur. Commun. Dis. Bull. 2004, 9, 5–7. [Google Scholar] [CrossRef]
- Naing, N.N. Easy way to learn standardization: Direct and indirect methods. Malays. J. Med. Sci. 2000, 7, 10–15. [Google Scholar]
- Bendavid, E.; Mulaney, B.; Sood, N.; Shah, S.; Bromley-Dulfano, R.; Lai, C.; Weissberg, Z.; Saavedra-Walker, R.; Tedrow, J.; Bogan, A.; et al. COVID-19 antibody seroprevalence in Santa Clara County, California. Int. J. Epidemiol. 2021, 50, 410–419. [Google Scholar] [CrossRef]
- Diggle, P.J. Estimating Prevalence Using an Imperfect Test. Epidemiol. Res. Int. 2011, 2011, 608719. [Google Scholar] [CrossRef] [Green Version]
- European Center for Disease Perevention and Control (ECDC). Immune Responses and Immunity to SARS-CoV-2. Available online: https://www.ecdc.europa.eu/en/covid-19/latest-evidence/immune-responses (accessed on 16 November 2021).
- Self, W.H.; Tenforde, M.W.; Stubblefield, W.B.; Feldstein, L.R.; Steingrub, J.S.; Shapiro, N.I.; Ginde, A.A.; Prekker, M.E.; Brown, S.M.; Peltan, I.D.; et al. Decline in SARS-CoV-2 Antibodies After Mild Infection Among Frontline Health Care Personnel in a Multistate Hospital Network—12 States, April-August 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 1762–1766. [Google Scholar] [CrossRef]
- Rostami, A.; Sepidarkish, M.; Fazlzadeh, A.; Mokdad, A.H.; Sattarnezhad, A.; Esfandyari, S.; Riahi, S.M.; Mollalo, A.; Dooki, M.E.; Bayani, M.; et al. Update on SARS-CoV-2 seroprevalence: Regional and worldwide. Clin. Microbiol. Infect. 2021, 27, 1762–1771. [Google Scholar] [CrossRef] [PubMed]
- Tatsi, E.B.; Dellis, C.; Petridou, E.; Banou, K.; Zachariadou, L.; Syriopoulou, V.; Michos, A. SARS-CoV-2 seroepidemiological study in healthcare workers and discordant results using seven different diagnostic methods. Infection 2021, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Kotsiou, O.S.; Papagiannis, D.; Fradelos, E.C.; Perlepe, G.; Miziou, A.; Siachpazidou, D.S.; Gourgoulianis, K.I. Understanding covid-19 epidemiology and implications for control: The experience from a greek semi-closed community. J. Clin. Med. 2021, 10, 2765. [Google Scholar] [CrossRef] [PubMed]
- Fotis, C.; Meimetis, N.; Tsolakos, N.; Politou, M.; Akinosoglou, K.; Pliaka, V.; Minia, A.; Terpos, E.; Trougakos, I.P.; Mentis, A.; et al. Accurate SARS-CoV-2 seroprevalence surveys require robust multi-antigen assays. Sci. Rep. 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Goldblatt, D.; Johnson, M.; Falup-Pecurariu, O.; Ivaskeviciene, I.; Spoulou, V.; Tamm, E.; Wagner, M.; Zar, H.J.; Bleotu, L.; Ivaskevicius, R.; et al. Cross-sectional prevalence of SARS-CoV-2 antibodies in healthcare workers in paediatric facilities in eight countries. J. Hosp. Infect. 2021, 110, 60–66. [Google Scholar] [CrossRef]
- Psichogiou, M.; Karabinis, A.; Pavlopoulou, I.D.; Basoulis, D.; Petsios, K.; Roussos, S.; Pratikaki, M.; Jahaj, E.; Protopapas, K.; Leontis, K.; et al. Antibodies against SARS-CoV-2 among health care workers in a country with low burden of COVID-19. PLoS ONE 2020, 15, e0243025. [Google Scholar] [CrossRef]
- Vlachoyiannopoulos, P.; Alexopoulos, H.; Apostolidi, I.; Bitzogli, K.; Barba, C.; Athanasopoulou, E.; Dalakas, M.; Tzioufas, A. Anti-SARS-CoV-2 antibody detection in healthcare workers of two tertiary hospitals in Athens, Greece. Clin. Immunol. 2020, 221. [Google Scholar] [CrossRef]
- Tsitsilonis, O.E.; Paraskevis, D.; Lianidou, E.; Pierros, V.; Akalestos, A.; Kastritis, E.; Moutsatsou, P.; Scorilas, A.; Sphicopoulos, T.; Terpos, E.; et al. Seroprevalence of antibodies against SARS-CoV-2 among the personnel and students of the national and kapodistrian university of athens, greece: A preliminary report. Life 2020, 10, 214. [Google Scholar] [CrossRef]
- Bajema, K.L.; Wiegand, R.E.; Cuffe, K.; Patel, S.V.; Iachan, R.; Lim, T.; Lee, A.; Moyse, D.; Havers, F.P.; Harding, L.; et al. Estimated SARS-CoV-2 Seroprevalence in the US as of September 2020. JAMA Intern. Med. 2021, 181, 450–460. [Google Scholar] [CrossRef]
- Ward, H.; Atchison, C.; Whitaker, M.; Donnelly, C.A.; Riley, S.; Ashby, D.; Darzi, A.; Barclay, W.S.; Cooke, G.; Elliott, P.; et al. Increasing SARS-CoV-2 antibody prevalence in England at the start of the second wave: REACT-2 Round 4 cross-sectional study in 160,000 adults. medRxiv 2021. [Google Scholar] [CrossRef]
- Pastor-Barriuso, R.; Pérez-Gómez, B.; Hernán, M.A.; Pérez-Olmeda, M.; Yotti, R.; Oteo-Iglesias, J.; Sanmartín, J.L.; León-Gómez, I.; Fernández-García, A.; Fernández-Navarro, P.; et al. Infection fatality risk for SARS-CoV-2 in community dwelling population of Spain: Nationwide seroepidemiological study. BMJ 2020, 371, m4509. [Google Scholar] [CrossRef] [PubMed]
- Bobrovitz, N.; Arora, R.K.; Cao, C.; Boucher, E.; Liu, M.; Donnici, C.; Yanes-Lane, M.; Whelan, M.; Perlman-Arrow, S.; Chen, J.; et al. Global seroprevalence of SARS-CoV-2 antibodies: A systematic review and metaanalysis. PLoS ONE 2021, 16, e0252617. [Google Scholar] [CrossRef] [PubMed]
- Huang, A.T.; Garcia-Carreras, B.; Hitchings, M.D.T.; Yang, B.; Katzelnick, L.C.; Rattigan, S.M.; Borgert, B.A.; Moreno, C.A.; Solomon, B.D.; Trimmer-Smith, L.; et al. A systematic review of antibody mediated immunity to coronaviruses: Kinetics, correlates of protection, and association with severity. Nat. Commun. 2020, 11, 4704. [Google Scholar] [CrossRef] [PubMed]
- Wold Health Organization (WHO). COVID-19 Disease in Children and Adolescents. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Sci_Brief-Children_and_adolescents-2021.1 (accessed on 18 December 2021).



| Month | Seropositivity | New Infections | Previous Infections (IgG Positive) | Previous Infections (Seroreversed) | Total Infections | Cumulative Cases * | Ratio (Total/Reported) |
|---|---|---|---|---|---|---|---|
| September | 0.97 (0.53–1.41) | 0.72 (0.53–0.92) | 0.57 (0.10–1.18) | 0.20 (0.04–0.40) | 1.17 (0.57–1.81) | 0.104 | 11.25 (5.43–17.37) |
| October | 1.80 (1.28–2.33) | 0.98 (0.83–1.14) | 0.82 (0.45–1.19) | 0.35 (0.12–0.61) | 2.15 (1.40–2.94) | 0.183 | 11.74 (7.63–16.08) |
| November | 3.30 (2.51–4.09) | 1.77 (1.43–2.12) | 1.53 (1.08–1.97) | 0.51 (0.22–0.83) | 3.81 (2.73–4.92) | 0.434 | 8.77 (6.28–11.33) |
| December | 9.09 (7.64–10.55) | 6.29 (5.51–7.08) | 2.80 (2.13–3.47) | 0.95 (0.61–1.32) | 10.04 (8.25–11.87) | 1.047 | 9.59 (7.88–11.33) |
| Central Greece (Thessaly & Central Greece) | Islands | Northern Greece (Macedonia & Thrace & Epirus) | Southern Greece (Western Greece & Peloponnese) | Attica | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Month | p (S3) | 95% CI | p (S3) | 95% CI | p (S3) | 95% CI | p (S3) | 95% CI | p (S3) | 95% CI | |||||
| September | 0.31% | 0.00% | 0.97% | 0.56% | 0.00% | 1.29% | 0.77% | 0.27% | 1.28% | 0.06% | 0.00% | 0.32% | 1.54% | 0.72% | 2.35% |
| October | 0.44% | 0.00% | 0.90% | 0.47% | 0.00% | 1.22% | 0.78% | 0.30% | 1.25% | 0.00% | 0.00% | 0.21% | 2.29% | 1.35% | 3.23% |
| November | 1.30% | 0.67% | 1.94% | 1.69% | 0.58% | 2.80% | 3.68% | 2.76% | 4.60% | 2.76% | 1.76% | 3.77% | 3.40% | 1.70% | 5.09% |
| December | 5.81% | 4.57% | 7.05% | 1.74% | 0.85% | 2.63% | 10.34% | 8.32% | 12.37% | 2.53% | 1.42% | 3.64% | 11.92% | 8.69% | 15.15% |
| Rest of Country | Attica | Thessaloniki | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pos | Total | S3 (%) | 95% CI | Pos | Total | S3 (%) | 95% CI | Pos | Total | S3 (%) | 95% CI | ||||
| September | 39 | 6283 | 0.65 | 0.16 | 1.14 | 19 | 1288 | 1.54 | 0.72 | 2.35 | 1 | 218 | 0.19 | 0.00 | 1.26 |
| October | 46 | 6520 | 1.80 | 1.12 | 2.47 | 31 | 1413 | 2.29 | 1.37 | 3.21 | 1 | 227 | 0.12 | 0.00 | 1.10 |
| November | 123 | 5797 | 3.08 | 2.27 | 3.88 | 20 | 620 | 3.40 | 1.76 | 5.04 | 21 | 652 | 3.76 | 2.09 | 5.44 |
| December | 247 | 5503 | 5.90 | 4.56 | 7.24 | 60 | 603 | 11.92 | 9.03 | 14.82 | 14 | 125 | 12.76 | 6.21 | 19.30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koureas, M.; Bogogiannidou, Z.; Vontas, A.; Kyritsi, M.A.; Mouchtouri, V.A.; Dadouli, K.; Anagnostopoulos, L.; Mina, P.; Matziri, A.; Ntouska, M.; et al. SARS-CoV-2 Sero-Surveillance in Greece: Evolution over Time and Epidemiological Attributes during the Pre-Vaccination Pandemic Era. Diagnostics 2022, 12, 295. https://doi.org/10.3390/diagnostics12020295
Koureas M, Bogogiannidou Z, Vontas A, Kyritsi MA, Mouchtouri VA, Dadouli K, Anagnostopoulos L, Mina P, Matziri A, Ntouska M, et al. SARS-CoV-2 Sero-Surveillance in Greece: Evolution over Time and Epidemiological Attributes during the Pre-Vaccination Pandemic Era. Diagnostics. 2022; 12(2):295. https://doi.org/10.3390/diagnostics12020295
Chicago/Turabian StyleKoureas, Michalis, Zacharoula Bogogiannidou, Alexandros Vontas, Maria A. Kyritsi, Varvara A. Mouchtouri, Katerina Dadouli, Lemonia Anagnostopoulos, Paraskevi Mina, Alexia Matziri, Maria Ntouska, and et al. 2022. "SARS-CoV-2 Sero-Surveillance in Greece: Evolution over Time and Epidemiological Attributes during the Pre-Vaccination Pandemic Era" Diagnostics 12, no. 2: 295. https://doi.org/10.3390/diagnostics12020295