
SARS-CoV-2 Saliva Mass Screening in Primary Schools: A 10-Week Sentinel Surveillance Study in Munich, Germany

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Conduct
2.2. Ethical Statement
2.3. Eligibility Criteria and Study Procedure
2.4. Laboratory Analysis
2.5. Statistical Analysis
2.6. Contact Tracing
2.7. Online Questionnaire
3. Results
3.1. Study Population
3.2. Detection of SARS-CoV-2 Infection by RT-qPCR
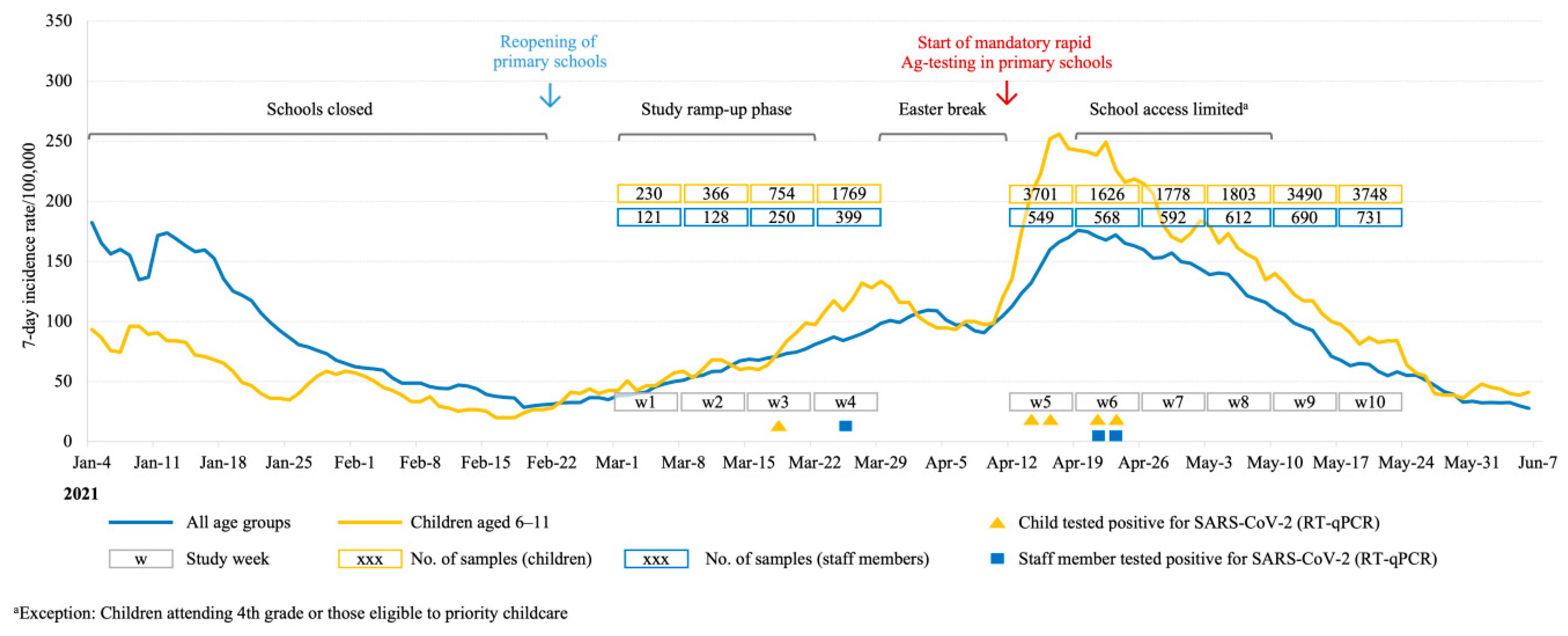
3.3. Background Incidence
3.4. NGS and Distribution of SARS-CoV-2 Variants
3.5. Saliva Volume Measurement
3.6. Infection Control Measure and Evaluation of Study Concept
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hoch, M.; Vogel, S.; Kolberg, L.; Dick, E.; Fingerle, V.; Eberle, U.; Ackermann, N.; Sing, A.; Huebner, J.; Rack-Hoch, A.; et al. Weekly SARS-CoV-2 Sentinel Surveillance in Primary Schools, Kindergartens, and Nurseries, Germany, June–November 2020. Emerg. Infect. Dis. 2021, 27, 2192–2196. [Google Scholar] [CrossRef] [PubMed]
- Ismail, S.A.; Saliba, V.; Lopez Bernal, J.; Ramsay, M.E.; Ladhani, S.N. SARS-CoV-2 infection and transmission in educational settings: A prospective, cross-sectional analysis of infection clusters and outbreaks in England. Lancet Infect. Dis. 2021, 21, 344–353. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. National Center for Immunization and Respiratory Diseases (NCIRD) Division of Viral Diseases. Science Brief: Transmission of SARS-CoV-2 in K-12 schools and Early Care and Education Programs-Updated. 9 July 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/transmission_k_12_schools.html (accessed on 11 November 2021).
- Ladhani, S.N.; Baawuah, F.; Beckmann, J.; Okike, I.O.; Ahmad, S.; Garstang, J.; Brent, A.J.; Brent, B.; Walker, J.; Andrews, N.; et al. SARS-CoV-2 infection and transmission in primary schools in England in June–December, 2020 (sKIDs): An active, prospective surveillance study. Lancet Child Adolesc. Health 2021, 5, 417–427. [Google Scholar] [CrossRef]
- Davies, N.G.; Klepac, P.; Liu, Y.; Prem, K.; Jit, M.; Pearson, C.A.B.; Quilty, B.J.; Kucharski, A.J.; Gibbs, H.; Clifford, S.; et al. Age-dependent effects in the transmission and control of COVID-19 epidemics. Nat. Med. 2020, 26, 1205–1211. [Google Scholar] [CrossRef]
- Viner, R.M.; Russell, S.J.; Croker, H.; Packer, J.; Ward, J.; Stansfield, C.; Mytton, O.; Bonell, C.; Booy, R. School closure and management practices during coronavirus outbreaks including COVID-19: A rapid systematic review. Lancet Child Adolesc. Health 2020, 4, 397–404. [Google Scholar] [CrossRef]
- Creswell, C.; Shum, A.; Pearcey, S.; Skripkauskaite, S.; Patalay, P.; Waite, P. Young people’s mental health during the COVID-19 pandemic. Lancet Child Adolesc. Health 2021, 5, 535–537. [Google Scholar] [CrossRef]
- Racine, N.; McArthur, B.A.; Cooke, J.E.; Eirich, R.; Zhu, J.; Madigan, S. Global Prevalence of Depressive and Anxiety Symptoms in Children and Adolescents During COVID-19: A Meta-analysis. JAMA Pediatr. 2021, 175, 1142–1150. [Google Scholar] [CrossRef] [PubMed]
- United Nations Children’s Fund. COVID-19 and School Closures. One year of educational disruption. March 2021. Available online: https://data.unicef.org/resources/one-year-of-covid-19-and-school-closures/ (accessed on 11 November 2021).
- Ravens-Sieberer, U.; Kaman, A.; Erhart, M.; Devine, J.; Schlack, R.; Otto, C. Impact of the COVID-19 pandemic on quality of life and mental health in children and adolescents in Germany. Eur. Child Adolesc. Psychiatry 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Woolford, S.J.; Sidell, M.; Li, X.; Else, V.; Young, D.R.; Resnicow, K.; Koebnick, C. Changes in Body Mass Index Among Children and Adolescents During the COVID-19 Pandemic. JAMA 2021, 326, 1434–1436. [Google Scholar] [CrossRef] [PubMed]
- Koletzko, B.; Holzapfel, C.; Schneider, U.; Hauner, H. Lifestyle and Body Weight Consequences of the COVID-19 Pandemic in Children: Increasing Disparity. Ann. Nutr. Metab. 2021, 77, 1–3. [Google Scholar] [CrossRef]
- Engzell, P.; Frey, A.; Verhagen, M.D. Learning loss due to school closures during the COVID-19 pandemic. Proc. Natl. Acad. Sci. USA 2021, 118, e2022376118. [Google Scholar] [CrossRef] [PubMed]
- Rubens, J.H.; Akindele, N.P.; Tschudy, M.M.; Sick-Samuels, A.C. Acute covid-19 and multisystem inflammatory syndrome in children. BMJ 2021, 372, n385. [Google Scholar] [CrossRef] [PubMed]
- Bhopal, S.S.; Bagaria, J.; Olabi, B.; Bhopal, R. Children and young people remain at low risk of COVID-19 mortality. Lancet Child Adolesc. Health 2021, 5, e12–e13. [Google Scholar] [CrossRef]
- Molteni, E.; Sudre, C.H.; Canas, L.S.; Bhopal, S.S.; Hughes, R.C.; Chen, L.; Deng, J.; Murray, B.; Kerfoot, E.; Antonelli, M.; et al. Illness characteristics of COVID-19 in children infected with the SARS-CoV-2 Delta variant. medRxiv 2021. [Google Scholar] [CrossRef]
- Hoch, M.; Vogel, S.; Eberle, U.; Kolberg, L.; Gruenthaler, V.; Fingerle, V.; Ackermann, N.; Sing, A.; Liebl, B.; Huebner, J.; et al. Feasibility and Diagnostic Accuracy of Saliva-Based SARS-CoV-2 Screening in Educational Settings and Children Aged <12 Years. Diagnostics 2021, 11, 1797. [Google Scholar] [CrossRef]
- Tan, S.H.; Allicock, O.; Armstrong-Hough, M.; Wyllie, A.L. Saliva as a gold-standard sample for SARS-CoV-2 detection. Lancet Respir. Med. 2021, 9, 562–564. [Google Scholar] [CrossRef]
- Abasiyanik, M.F.; Flood, B.; Lin, J.; Ozcan, S.; Rouhani, S.J.; Pyzer, A.; Trujillo, J.; Zhen, C.; Wu, P.; Jumic, S.; et al. Sensitive detection and quantification of SARS-CoV-2 in saliva. Sci. Rep. 2021, 11, 12425. [Google Scholar] [CrossRef] [PubMed]
- Huang, N.; Pérez, P.; Kato, T.; Mikami, Y.; Okuda, K.; Gilmore, R.C.; Conde, C.D.; Gasmi, B.; Stein, S.; Beach, M.; et al. SARS-CoV-2 infection of the oral cavity and saliva. Nat. Med. 2021, 27, 892–903. [Google Scholar] [CrossRef] [PubMed]
- Villar, L.M.; da Costa, V.D.; Marques, B.C.L.; da Silva, L.L.; Santos, A.C.; Mendonça, A.C.d.F.; Marques, V.A.; do Nascimento, G.P.; Lewis-Ximenez, L.L.; de Paula, V.S. Usefulness of saliva samples for detecting SARS-CoV-2 RNA among liver disease patients. J. Infect. 2021, 82, e4–e5. [Google Scholar] [CrossRef]
- Melo Costa, M.; Benoit, N.; Dormoi, J.; Amalvict, R.; Gomez, N.; Tissot-Dupont, H.; Million, M.; Pradines, B.; Granjeaud, S.; Almeras, L. Salivette, a relevant saliva sampling device for SARS-CoV-2 detection. J. Oral Microbiol. 2021, 13, 1920226. [Google Scholar] [CrossRef] [PubMed]
- Fougère, Y.; Schwob, J.M.; Miauton, A.; Hoegger, F.; Opota, O.; Jaton, K.; Brouillet, R.; Greub, G.; Genton, B.; Gehri, M.; et al. Performance of RT-PCR on Saliva Specimens Compared with Nasopharyngeal Swabs for the Detection of SARS-CoV-2 in Children: A Prospective Comparative Clinical Trial. Pediatr. Infect. Dis. J. 2021, 40, e300–e304. [Google Scholar] [CrossRef] [PubMed]
- Al Suwaidi, H.; Senok, A.; Varghese, R.; Deesi, Z.; Khansaheb, H.; Pokasirakath, S.; Chacko, B.; Abufara, I.; Loney, T.; Alsheikh-Ali, A. Saliva for molecular detection of SARS-CoV-2 in school-age children. Clin. Microbiol. Infect. 2021, 27, 1330–1335. [Google Scholar] [CrossRef]
- Azzi, L. Saliva is the Key Element for Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Mass Screening. Clin. Infect. Dis. 2021, 73, e566–e568. [Google Scholar] [CrossRef] [PubMed]
- Hershow, R.B.; Wu, K.; Lewis, N.M.; Milne, A.T.; Currie, D.; Smith, A.R.; Lloyd, S.; Orleans, B.; Young, E.L.; Freeman, B.; et al. Low SARS-CoV-2 Transmission in Elementary Schools—Salt Lake County, Utah, December 3, 2020–January 31, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 442–448. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Participants, No. (%) | |
|---|---|---|
| Staff | Children | |
| Total No. | 681 | 3752 |
| Age, median,(range) [IQR], y | 41 (14–71) [29–51] | 8 (6–13) [7–9] |
| Sex | ||
| Male | 89 (0.13) | 1826 (0.49) |
| Female | 592 (0.87) | 1926 (0.51) |
| Study Week | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| Participants, No. | ||||||||||
| Total | 341 | 485 | 965 | 2128 | 3194 | 1312 | 1381 | 1374 | 2705 | 2816 |
| Children | 230 | 363 | 741 | 1763 | 2808 | 961 | 1010 | 1005 | 2298 | 2403 |
| Staff members | 111 | 122 | 224 | 365 | 386 | 351 | 371 | 369 | 407 | 413 |
| Saliva samples, No. | ||||||||||
| Total | 351 | 494 | 1004 | 2168 | 4250 | 2194 | 2370 | 2415 | 4180 | 4479 |
| Children (all) | 230 | 366 | 754 | 1769 | 3701 | 1626 | 1778 | 1803 | 3490 | 3748 |
| Children (negative) | 230 | 366 | 753 | 1769 | 3699 | 1623 | 1777 | 1802 | 3490 | 3748 |
| Children (positive) | 0 | 0 | 1 | 0 | 2 | 2 | 0 | 0 | 0 | 0 |
| Children (inconclusive) | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 0 |
| Staff members (all) | 121 | 128 | 250 | 399 | 549 | 568 | 592 | 612 | 690 | 731 |
| Staff members (negative) | 121 | 128 | 250 | 398 | 549 | 566 | 592 | 612 | 690 | 731 |
| Staff members (positive) | 0 | 0 | 0 | 1 | 0 | 2 | 0 | 0 | 0 | 0 |
| Staff members (inconclusive) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Test frequency, No. | ||||||||||
| Children tested once | 230 | 360 | 728 | 1757 | 1923 | 559 | 554 | 495 | 1258 | 1329 |
| Children tested twice | 0 | 3 | 13 | 6 | 878 | 179 | 197 | 258 | 910 | 843 |
| Children tested three times | 0 | 0 | 0 | 0 | 6 | 201 | 228 | 225 | 108 | 205 |
| Children tested four times | 0 | 0 | 0 | 0 | 1 | 4 | 9 | 18 | 22 | 12 |
| Children tested five times | 0 | 0 | 0 | 0 | 0 | 18 | 22 | 9 | 0 | 14 |
| Staff members tested once | 101 | 116 | 200 | 331 | 246 | 218 | 233 | 207 | 222 | 208 |
| Staff members tested twice | 10 | 6 | 22 | 34 | 120 | 74 | 78 | 103 | 107 | 127 |
| Staff members tested three times | 0 | 0 | 2 | 0 | 17 | 44 | 46 | 46 | 58 | 57 |
| Staff members tested four times | 0 | 0 | 0 | 0 | 3 | 5 | 5 | 6 | 20 | 7 |
| Staff members tested five times | 0 | 0 | 0 | 0 | 0 | 10 | 9 | 8 | 0 | 14 |
| Age Group [Years] | n | Mean [μL] | Min [μL] | Max [μL] |
|---|---|---|---|---|
| 6 | 261 | 1495 | 300 | 3150 |
| 7 | 1045 | 1481 | 10 | 3600 |
| 8 | 916 | 1579 | 50 | 4300 |
| 9 | 889 | 1609 | 100 | 3900 |
| 10 | 608 | 1558 | 10 | 3600 |
| 11–13 | 60 | 1523 | 400 | 2750 |
| 6–13 (all children) | 3779 | 1549 | 10 | 4300 |
| 14–71 (all staff) | 736 | 1582 | 50 | 2650 |
| All | 4515 | 1554 | 10 | 4300 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vogel, S.; von Both, U.; Nowak, E.; Ludwig, J.; Köhler, A.; Lee, N.; Dick, E.; Rack-Hoch, A.; Wicklein, B.; Neusser, J.; et al. SARS-CoV-2 Saliva Mass Screening in Primary Schools: A 10-Week Sentinel Surveillance Study in Munich, Germany. Diagnostics 2022, 12, 162. https://doi.org/10.3390/diagnostics12010162
Vogel S, von Both U, Nowak E, Ludwig J, Köhler A, Lee N, Dick E, Rack-Hoch A, Wicklein B, Neusser J, et al. SARS-CoV-2 Saliva Mass Screening in Primary Schools: A 10-Week Sentinel Surveillance Study in Munich, Germany. Diagnostics. 2022; 12(1):162. https://doi.org/10.3390/diagnostics12010162
Chicago/Turabian StyleVogel, Sebastian, Ulrich von Both, Elisabeth Nowak, Janina Ludwig, Alexandra Köhler, Noah Lee, Elisabeth Dick, Anita Rack-Hoch, Bernd Wicklein, Jessica Neusser, and et al. 2022. "SARS-CoV-2 Saliva Mass Screening in Primary Schools: A 10-Week Sentinel Surveillance Study in Munich, Germany" Diagnostics 12, no. 1: 162. https://doi.org/10.3390/diagnostics12010162