
Renin-Angiotensin-Aldosterone System Inhibitors and Risk of Cancer: A Population-Based Cohort Study Using a Common Data Model

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
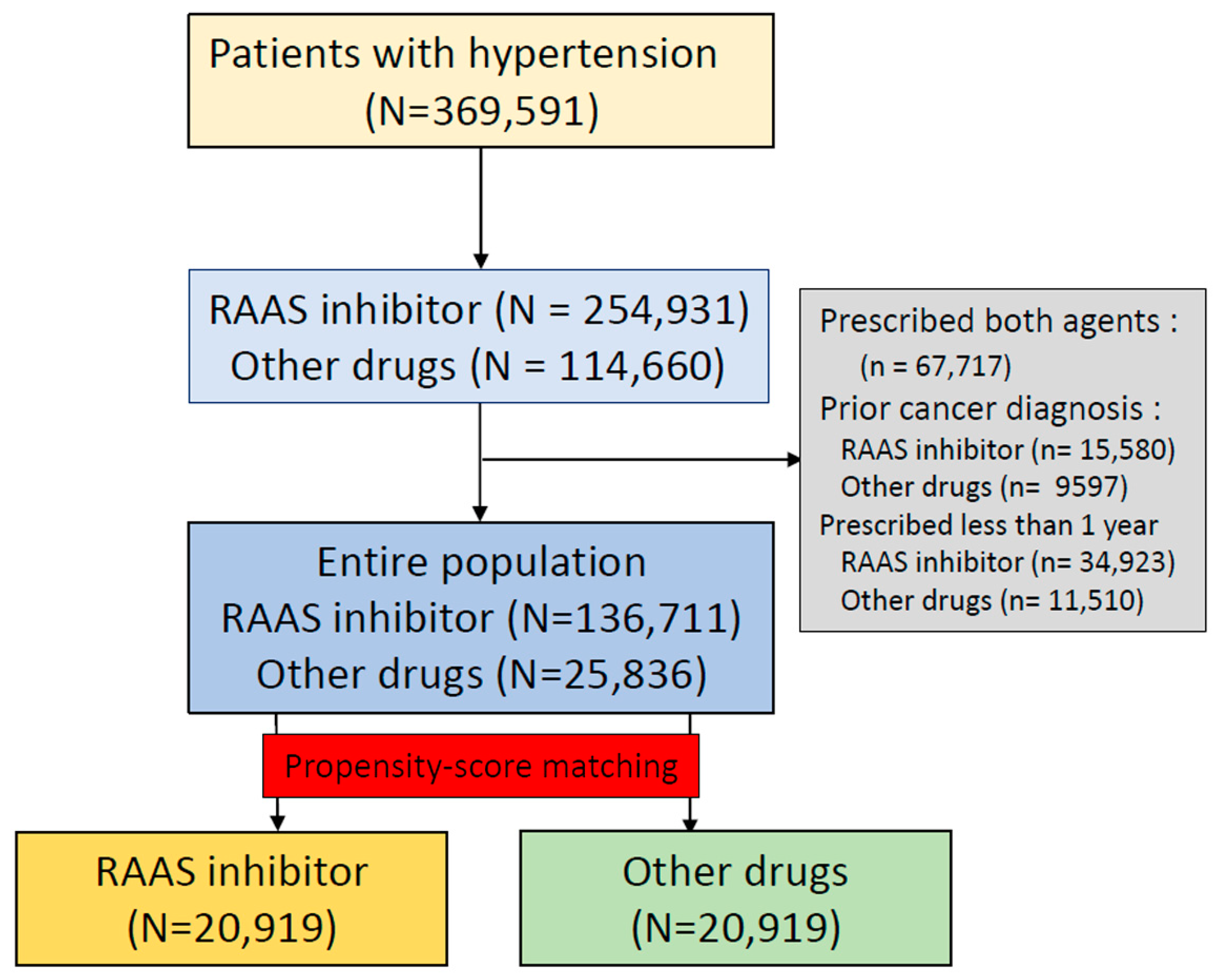
2.1. Data Curation, Cohort Definition, and Outcome
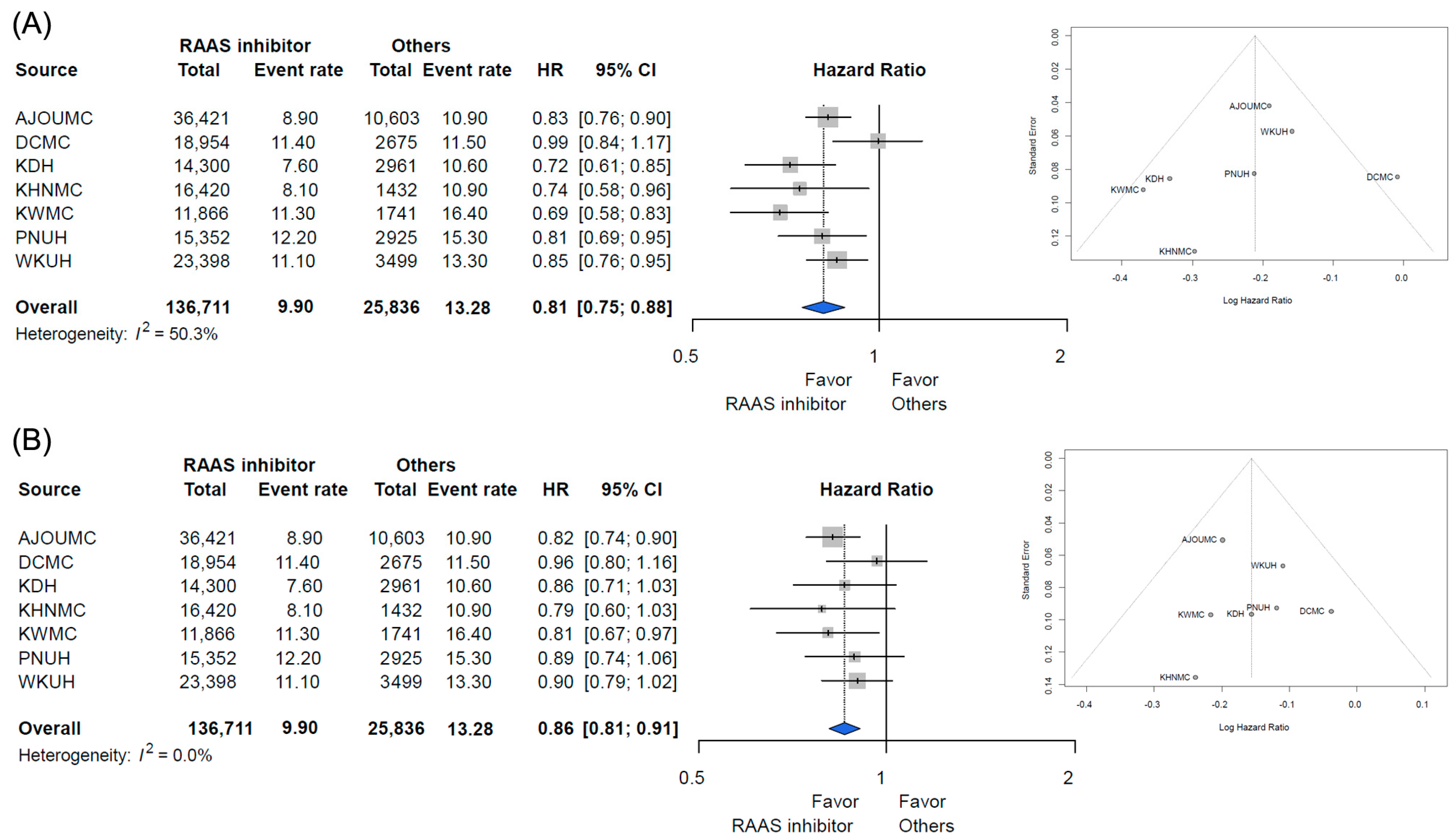
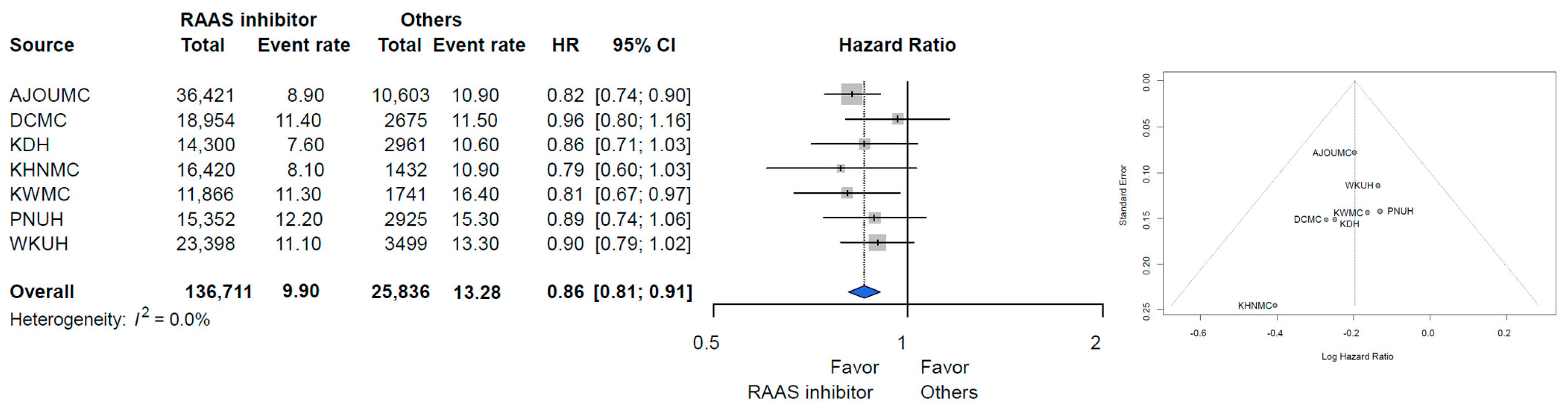
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sipahi, I.; Debanne, S.M.; Rowland, D.Y.; Simon, D.I.; Fang, J.C. Angiotensin-receptor blockade and risk of cancer: Meta-analysis of randomised controlled trials. Lancet Oncol. 2010, 11, 627–636. [Google Scholar] [CrossRef] [Green Version]
- Hanif, K.; Bid, H.K.; Konwar, R. Reinventing the ACE inhibitors: Some old and new implications of ACE inhibition. Hypertens. Res. 2010, 33, 11–21. [Google Scholar] [CrossRef] [Green Version]
- Song, T.; Choi, C.H.; Kim, M.K.; Kim, M.L.; Yun, B.S.; Seong, S.J. The effect of angiotensin system inhibitors (angiotensin-converting enzyme inhibitors or angiotensin receptor blockers) on cancer recurrence and survival: A meta-analysis. Eur. J. Cancer Prev. 2017, 26, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Tadic, M.; Cuspidi, C.; Belyavskiy, E.; Grassi, G. Intriguing relationship between antihypertensive therapy and cancer. Pharmacol. Res. 2019, 141, 501–511. [Google Scholar] [CrossRef] [PubMed]
- Sipahi, I.; Chou, J.; Mishra, P.; Debanne, S.M.; Simon, D.I.; Fang, J.C. Meta-analysis of randomized controlled trials on effect of angiotensin-converting enzyme inhibitors on cancer risk. Am. J. Cardiol. 2011, 108, 294–301. [Google Scholar] [CrossRef]
- Afsar, B.; Afsar, R.E.; Ertuglu, L.A.; Kuwabara, M.; Ortiz, A.; Covic, A.; Kanbay, M. Renin-angiotensin system and cancer: Epidemiology, cell signaling, genetics and epigenetics. Clin. Transl. Oncol. 2021, 23, 682–696. [Google Scholar] [CrossRef] [PubMed]
- You, S.C.; Lee, S.; Cho, S.Y.; Park, H.; Jung, S.; Cho, J.; Yoon, D.; Park, R.W. Conversion of National Health Insurance Service-National Sample Cohort (NHIS-NSC) Database into Observational Medical Outcomes Partnership-Common Data Model (OMOP-CDM). Stud. Health Technol. Inform. 2017, 245, 467–470. [Google Scholar] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Thiers, B.H. Association of ACE Inhibitors and Angiotensin Receptor Blockers with Keratinocyte Cancer Prevention in the Randomized VATTC Trial. Year Book Dermatol. Dermatol. Surg. 2009, 2009, 318–319. [Google Scholar] [CrossRef]
- Ni, H.; Rui, Q.; Zhu, X.; Yu, Z.; Gao, R.; Liu, H. Antihypertensive drug use and breast cancer risk: A meta-analysis of observational studies. Oncotarget 2017, 8, 62545–62560. [Google Scholar] [CrossRef] [Green Version]
- Cao, L.; Zhang, S.; Jia, C.M.; He, W.; Wu, L.T.; Li, Y.Q.; Wang, W.; Li, Z.; Ma, J. Antihypertensive drugs use and the risk of prostate cancer: A meta-analysis of 21 observational studies. BMC Urol. 2018, 18, 17. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Acebo, I.; Dierssen-Sotos, T.; Palazuelos, C.; Perez-Gomez, B.; Lope, V.; Tusquets, I.; Alonso, M.H.; Moreno, V.; Amiano, P.; Molina de la Torre, A.J.; et al. The Use of Antihypertensive Medication and the Risk of Breast Cancer in a Case-Control Study in a Spanish Population: The MCC-Spain Study. PLoS ONE 2016, 11, e0159672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friis, S.; Sorensen, H.T.; Mellemkjaer, L.; McLaughlin, J.K.; Nielsen, G.L.; Blot, W.J.; Olsen, J.H. Angiotensin-converting enzyme inhibitors and the risk of cancer: A population-based cohort study in Denmark. Cancer 2001, 92, 2462–2470. [Google Scholar] [CrossRef]
- Schmidt, S.A.J.; Schmidt, M.; Mehnert, F.; Lemeshow, S.; Sørensen, H.T. Use of antihypertensive drugs and risk of skin cancer. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1545–1554. [Google Scholar] [CrossRef]
- Mitsushige, S.; Yoshio, Y.; Naohito, S.; Takahisa, F. Role of renin-angiotensin system in gastric oncogenesis. J. Gastroenterol. Hepatol. 2012, 27, 442–451. [Google Scholar]
- Gong, Q.; Davis, M.; Chipitsyna, G.; Yeo, C.J.; Arafat, H.A. Blocking angiotensin II Type 1 receptor triggers apoptotic cell death in human pancreatic cancer cells. Pancreas 2010, 39, 581–594. [Google Scholar] [CrossRef]
- Rhodes, D.R.; Ateeq, B.; Cao, Q.; Tomlins, S.A.; Mehra, R.; Laxman, B.; Kalyana-Sundaram, S.; Lonigro, R.J.; Helgeson, B.E.; Bhojani, M.S.; et al. AGTR1 overexpression defines a subset of breast cancer and confers sensitivity to losartan, an AGTR1 antagonist. Proc. Natl. Acad. Sci. USA 2009, 106, 10284–10289. [Google Scholar] [CrossRef] [Green Version]
- Fujimoto, Y.; Sasaki, T.; Tsuchida, A.; Chayama, K. Angiotensin II type 1 receptor expression in human pancreatic cancer and growth inhibition by angiotensin II type 1 receptor antagonist. FEBS Lett. 2001, 495, 197–200. [Google Scholar] [CrossRef]
- Wilop, S.; von Hobe, S.; Crysandt, M.; Esser, A.; Osieka, R.; Jost, E. Impact of angiotensin I converting enzyme inhibitors and angiotensin II type 1 receptor blockers on survival in patients with advanced non-small-cell lung cancer undergoing first-line platinum-based chemotherapy. J. Cancer Res. Clin. Oncol. 2009, 135, 1429–1435. [Google Scholar] [CrossRef]
- Tian, Y.; Schuemie, M.J.; Suchard, M.A. Evaluating large-scale propensity score performance through real-world and synthetic data experiments. Int. J. Epidemiol. 2018, 47, 2005–2014. [Google Scholar] [CrossRef]
- Rhee, C.; Dantes, R.; Epstein, L.; Murphy, D.J.; Seymour, C.W.; Iwashyna, T.J.; Kadri, S.S.; Angus, D.C.; Danner, R.L.; Fiore, A.E.; et al. Incidence and Trends of Sepsis in US Hospitals Using Clinical vs. Claims Data, 2009–2014. JAMA 2017, 318, 1241–1249. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Propensity-Score Stratification | Propensity-Score Matching | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| RAAS Inhibitor (N = 136,711) | Other Drugs (N = 25,836) | SMD | RAAS Inhibitor (N = 136,711) | Other Drugs (N = 25,836) | SMD | RAAS Inhibitor (N = 20,919) | Other Drugs (N = 20,919) | SMD | |
| Age group | |||||||||
| 20–24 | 0.8 | 1 | −0.02 | 0.7 | 0.9 | −0.02 | 0.7 | 0.9 | −0.02 |
| 25–29 | 0.8 | 1.7 | −0.08 | 1.3 | 1.3 | 0.01 | 1.3 | 1.2 | 0.01 |
| 30–34 | 1.5 | 2.4 | −0.07 | 1.8 | 1.9 | −0.01 | 1.7 | 1.8 | −0.01 |
| 35–39 | 3 | 3.7 | −0.04 | 3.2 | 3.5 | −0.02 | 3.2 | 3.4 | −0.02 |
| 45–49 | 7.8 | 6.9 | 0.03 | 7.5 | 7.6 | 0 | 7.3 | 7.4 | 0 |
| 50–54 | 10.7 | 9.2 | 0.05 | 10.4 | 10.4 | 0 | 10.3 | 10.3 | 0 |
| 55–59 | 12.4 | 11.1 | 0.04 | 12.6 | 12.3 | 0.01 | 12.6 | 12.3 | 0.01 |
| 60–64 | 13.2 | 11.9 | 0.04 | 13.4 | 13.3 | 0 | 13.4 | 13.4 | 0 |
| 65–69 | 13.1 | 12.3 | 0.02 | 13.1 | 13.1 | 0 | 13.2 | 13.1 | 0 |
| 70–74 | 12.4 | 12.6 | −0.01 | 12.8 | 12.4 | 0.01 | 12.9 | 12.5 | 0.01 |
| 80–84 | 5.9 | 7 | −0.05 | 5.4 | 5.5 | 0 | 5.5 | 5.6 | 0 |
| 85–89 | 2.4 | 3.1 | −0.04 | 2.1 | 2.2 | 0 | 2.2 | 2.3 | 0 |
| Gender: female | 45.3 | 53.5 | −0.16 | 56.6 | 55.1 | 0.03 | 56.7 | 55.2 | 0.03 |
| Medical history: General | |||||||||
| Acute respiratory disease | 2 | 3.2 | −0.08 | 2.8 | 2.5 | 0.02 | 2.8 | 2.5 | 0.02 |
| Diabetes mellitus | 17.6 | 10.7 | 0.2 | 9.5 | 9.9 | −0.01 | 9.3 | 9.8 | −0.01 |
| Hyperlipidemia | 14.3 | 7.2 | 0.23 | 9.1 | 9.4 | −0.01 | 9.2 | 9.5 | −0.01 |
| Hypertensive disorder | 50.1 | 37.6 | 0.25 | 42.8 | 43.1 | −0.01 | 42.4 | 42.7 | −0.01 |
| Osteoarthritis | 1.5 | 1.7 | −0.02 | 2.3 | 2.1 | 0.01 | 2.3 | 2.1 | 0.01 |
| Pneumonia | 2.9 | 6 | −0.15 | 3.5 | 3.4 | 0.01 | 3.5 | 3.4 | 0.01 |
| Renal impairment | 5.2 | 5.7 | −0.02 | 4.3 | 4.1 | 0.01 | 4.3 | 4.1 | 0.01 |
| Rheumatoid arthritis | 0.4 | 1.9 | −0.14 | 1.8 | 1.5 | 0.02 | 1.7 | 1.4 | 0.02 |
| Visual system disorder | 8.2 | 7.6 | 0.02 | 8.4 | 8.6 | −0.01 | 8.5 | 8.7 | −0.01 |
| Medical history: Cardiovascular disease | |||||||||
| Cerebrovascular disease | 5.9 | 4.1 | 0.08 | 5 | 4.9 | 0 | 5 | 5 | 0 |
| Coronary arteriosclerosis | 5.7 | 1.4 | 0.24 | 2.2 | 2.1 | 0.01 | 2.1 | 2 | 0.01 |
| Heart disease | 34.4 | 11.6 | 0.56 | 14.4 | 14.8 | −0.01 | 14.5 | 14.9 | −0.01 |
| Ischemic heart disease | 18.8 | 4.7 | 0.45 | 7.2 | 7.1 | 0 | 7.1 | 7.1 | 0 |
| Venous thrombosis | 0.4 | 0.8 | −0.05 | 0.5 | 0.5 | 0.01 | 0.5 | 0.5 | 0.01 |
| RAAS Inhibtor | Others | Unadjusted HR (95% CI) | PS Matched Pairs | PS Adjusted HR (95% CI) | |
|---|---|---|---|---|---|
| Breast cancer | 66,701 | 16,930 | 1.02 (0.82–1.26) | 13,157 | 1.07 (0.71–1.63) |
| Colon cancer | 146,043 | 30,543 | 0.82 (0.67–1.00) | 24,216 | 0.80 (0.59–1.08) |
| Gastric cancer | 145,997 | 30,456 | 0.79 (0.68–0.92) | 24,170 | 0.79 (0.62–1.00) |
| Liver cancer | 146,854 | 30,367 | 0.53 (0.46–0.60) | 24,393 | 0.71 (0.53–0.96) |
| Lung cancer | 146,882 | 30,962 | 0.68 (0.52–0.90) | 24,496 | 0.80 (0.55–1.16) |
| Gynecological cancer | 67,139 | 16,993 | 0.79 (0.51–1.24) | 13,230 | 1.48 (0.91–2.40) |
| Pancreaticobiliary cancer | 147,049 | 31,015 | 0.62 (0.54–0.72) | 24,565 | 0.61 (0.45–0.82) |
| Prostate cancer | 78,920 | 13,704 | 0.77 (0.58–1.02) | 10,838 | 1.00 (0.64–1.55) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-H.; Park, J.; Park, R.W.; Shin, S.J.; Kim, J.; Sung, J.D.; Kim, D.J.; Yang, K. Renin-Angiotensin-Aldosterone System Inhibitors and Risk of Cancer: A Population-Based Cohort Study Using a Common Data Model. Diagnostics 2022, 12, 263. https://doi.org/10.3390/diagnostics12020263
Lee S-H, Park J, Park RW, Shin SJ, Kim J, Sung JD, Kim DJ, Yang K. Renin-Angiotensin-Aldosterone System Inhibitors and Risk of Cancer: A Population-Based Cohort Study Using a Common Data Model. Diagnostics. 2022; 12(2):263. https://doi.org/10.3390/diagnostics12020263
Chicago/Turabian StyleLee, Seung-Hwa, Jungchan Park, Rae Woong Park, Seo Jeong Shin, Jinseob Kim, Ji Dong Sung, Dae Jung Kim, and Kwangmo Yang. 2022. "Renin-Angiotensin-Aldosterone System Inhibitors and Risk of Cancer: A Population-Based Cohort Study Using a Common Data Model" Diagnostics 12, no. 2: 263. https://doi.org/10.3390/diagnostics12020263