
Deep Learning Classifies Low- and High-Grade Glioma Patients with High Accuracy, Sensitivity, and Specificity Based on Their Brain White Matter Networks Derived from Diffusion Tensor Imaging
 and
and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Data Acquisition
2.2. Imaging Protocol
2.3. Data Processing
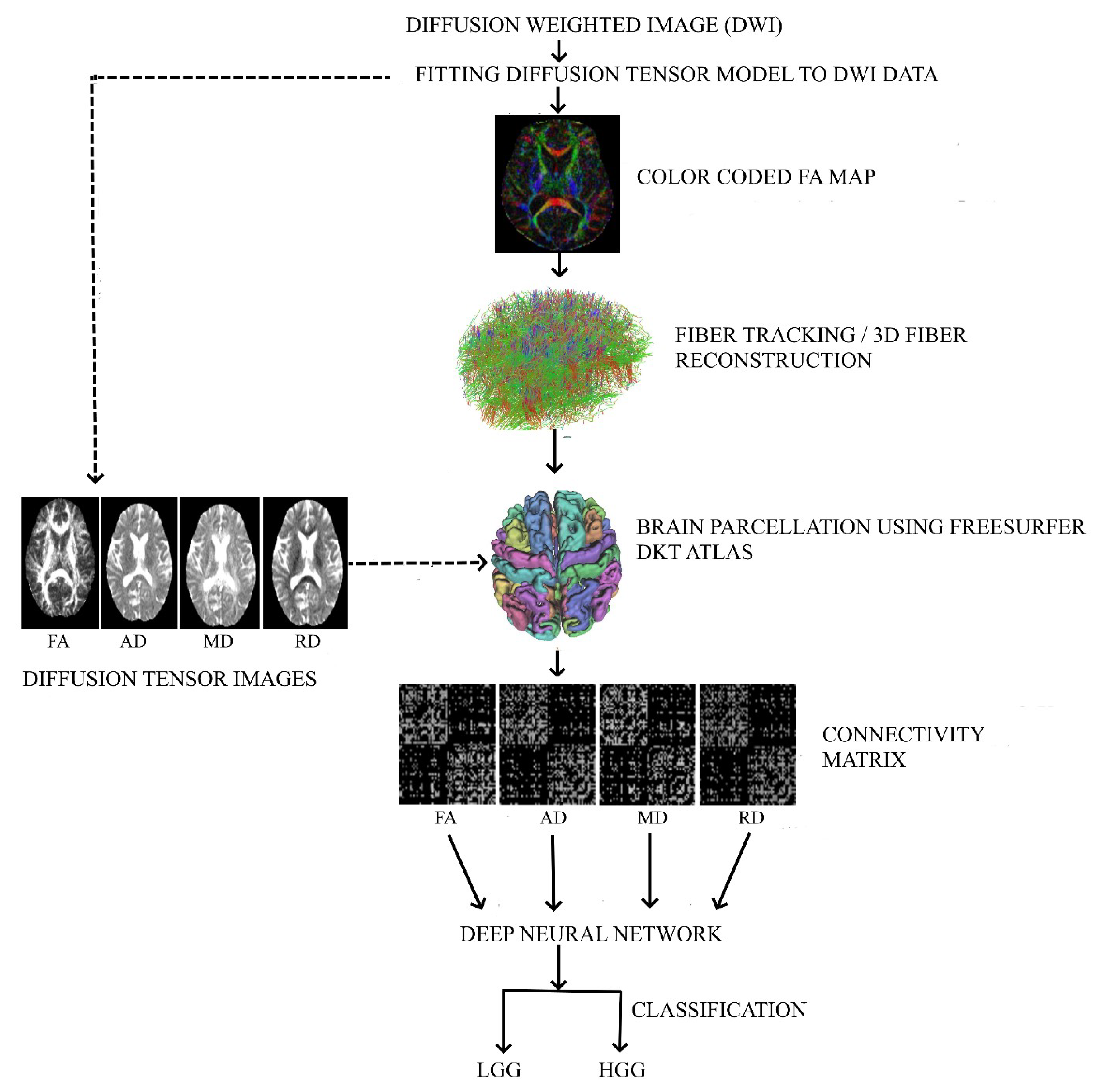
2.3.1. Diffusion Tensor Image Processing
2.3.2. Deep Neural Network Model to Classify LGG and HGG
2.3.3. Deep Neural Network Architecture for Connectivity Matrix as Images
2.3.4. Deep Neural Network Architecture Considering the Connectivity Matrix as a Matrix
3. Results
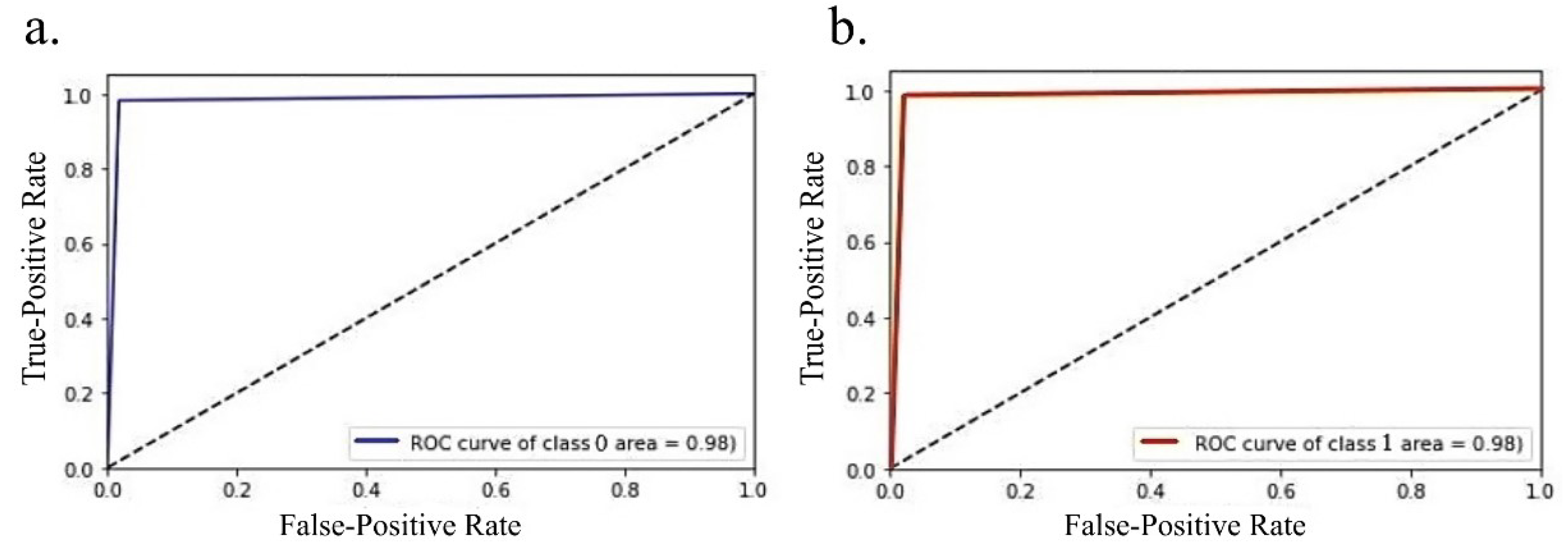
3.1. Performance of the DNN Model on Connectivity Matrix as Image
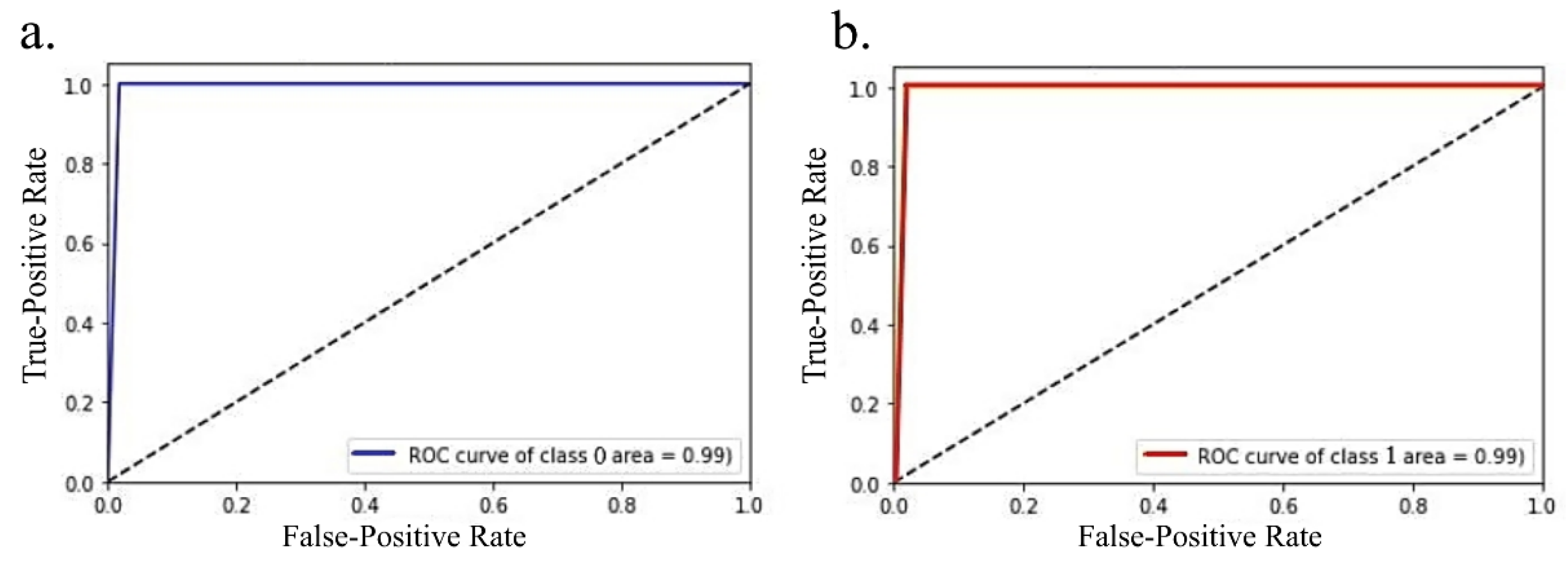
3.2. Performance of the DNN Model on the Connectivity Matrix as it is
3.3. GRAD-CAM Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yuan, W.; Holland, S.K.; Jones, B.V.; Crone, K.; Mangano, F.T. Characterization of abnormal diffusion properties of supratentorial brain tumors: A preliminary diffusion tensor imaging study. J. Neurosurg. Pediatr. 2008, 1, 263–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharifi, G.; Pajavand, A.M.; Nateghinia, S.; Meybodi, T.E.; Hasooni, H. Glioma Migration Through the Corpus Callosum and the Brainstem Detected by Diffusion and Magnetic Resonance Imaging: Initial Findings. Front. Hum. Neurosci. 2019, 13, 472. [Google Scholar] [CrossRef] [PubMed]
- Duffau, H. White Matter Tracts and Diffuse Lower-Grade Gliomas: The Pivotal Role of Myelin Plasticity in the Tumor Pathogenesis, Infiltration Patterns, Functional Consequences and Therapeutic Management. Front. Oncol. 2022, 12, 855587. [Google Scholar] [CrossRef] [PubMed]
- Gauvain, K.M.; McKinstry, R.C.; Mukherjee, P.; Perry, A.; Neil, J.J.; Kaufman, B.A.; Hayashi, R.J. Evaluating pediatric brain tumor cellularity with diffusion-tensor imaging. AJR Am. J. Roentgenol. 2001, 177, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Koob, M.; Girard, N.; Ghattas, B.; Fellah, S.; Confort-Gouny, S.; Figarella-Branger, D.; Scavarda, D. The diagnostic accuracy of multiparametric MRI to determine pediatric brain tumor grades and types. J. Neurooncol. 2016, 127, 345–353. [Google Scholar] [CrossRef] [PubMed]
- El-Serougy, L.; Abdel Razek, A.A.; Ezzat, A.; Eldawoody, H.; El-Morsy, A. Assessment of diffusion tensor imaging metrics in differentiating low-grade from high-grade gliomas. Neuroradiol. J. 2016, 29, 400–407. [Google Scholar] [CrossRef] [Green Version]
- Kubota, T.; Yamada, K.; Kizu, O.; Hirota, T.; Ito, H.; Ishihara, K.; Nishimura, T. Relationship between contrast enhancement on fluid-attenuated inversion recovery MR sequences and signal intensity on T2-weighted MR images: Visual evaluation of brain tumors. J. Magn. Reson. Imaging 2005, 21, 694–700. [Google Scholar] [CrossRef]
- Essig, M.; Metzner, R.; Bonsanto, M.; Hawighorst, H.; Debus, J.; Tronnier, V.; Knopp, M.V.; van Kaick, G. Postoperative fluid-attenuated inversion recovery MR imaging of cerebral gliomas: Initial results. Eur. Radiol. 2001, 11, 2004–2010. [Google Scholar] [CrossRef]
- Yang, Y.; Yan, L.F.; Zhang, X.; Nan, H.Y.; Hu, Y.C.; Han, Y.; Zhang, J.; Liu, Z.C.; Sun, Y.Z.; Tian, Q.; et al. Optimizing Texture Retrieving Model for Multimodal MR Image-Based Support Vector Machine for Classifying Glioma. J. Magn. Reson Imaging 2019, 49, 1263–1274. [Google Scholar] [CrossRef]
- Ding, J.; Zhao, R.; Qiu, Q.; Chen, J.; Duan, J.; Cao, X.; Yin, Y. Developing and validating a deep learning and radiomic model for glioma grading using multiplanar reconstructed magnetic resonance contrast-enhanced T1-weighted imaging: A robust, multi-institutional study. Quant. Imaging Med. Surg. 2022, 12, 1517–1528. [Google Scholar] [CrossRef]
- Jiang, L.; Xiao, C.Y.; Xu, Q.; Sun, J.; Chen, H.; Chen, Y.C.; Yin, X. Analysis of DTI-Derived Tensor Metrics in Differential Diagnosis between Low-grade and High-grade Gliomas. Front. Aging Neurosci. 2017, 9, 271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piyapittayanan, S.; Chawalparit, O.; Tritakarn, S.O.; Witthiwej, T.; Sangruchi, T.; Nunta-Aree, S.; Sathornsumetee, S.; Itthimethin, P.; Komoltri, C. Value of diffusion tensor imaging in differentiating high-grade from low-grade gliomas. J. Med. Assoc. Thai 2013, 96, 716–721. [Google Scholar] [PubMed]
- Inoue, T.; Ogasawara, K.; Beppu, T.; Ogawa, A.; Kabasawa, H. Diffusion tensor imaging for preoperative evaluation of tumor grade in gliomas. Clin. Neurol. Neurosurg. 2005, 107, 174–180. [Google Scholar] [CrossRef]
- Yeh, F.C.; Verstynen, T.D.; Wang, Y.; Fernandez-Miranda, J.C.; Tseng, W.Y. Deterministic diffusion fiber tracking improved by quantitative anisotropy. PLoS ONE 2013, 8, e80713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeh, F.C. Shape analysis of the human association pathways. Neuroimage 2020, 223, 117329. [Google Scholar] [CrossRef] [PubMed]
- Yasaka, K.; Kamagata, K.; Ogawa, T.; Hatano, T.; Takeshige-Amano, H.; Ogaki, K.; Andica, C.; Akai, H.; Kunimatsu, A.; Uchida, W.; et al. Parkinson’s disease: Deep learning with a parameter-weighted structural connectome matrix for diagnosis and neural circuit disorder investigation. Neuroradiology 2021, 63, 1451–1462. [Google Scholar] [CrossRef]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-CAM: Visual Explanations from Deep Networks via Gradient-Based Localization. Int. J. Comput. Vis. 2020, 128, 336–359. [Google Scholar] [CrossRef] [Green Version]
- Timpe, J.C.; Rowe, K.C.; Matsui, J.; Magnotta, V.A.; Denburg, N.L. White matter integrity, as measured by diffusion tensor imaging, distinguishes between impaired and unimpaired older adult decision-makers: A preliminary investigation. J. Cogn. Psychol. 2011, 23, 760–767. [Google Scholar] [CrossRef]
- Aung, W.Y.; Mar, S.; Benzinger, T.L. Diffusion tensor MRI as a biomarker in axonal and myelin damage. Imaging Med. 2013, 5, 427–440. [Google Scholar] [CrossRef] [Green Version]
- Alexander, A.L.; Lee, J.E.; Lazar, M.; Field, A.S. Diffusion tensor imaging of the brain. Neurotherapeutics 2007, 4, 316–329. [Google Scholar] [CrossRef]
- Liu, D.; Liu, Y.; Hu, X.; Hu, G.; Yang, K.; Xiao, C.; Hu, J.; Li, Z.; Zou, Y.; Chen, J.; et al. Alterations of white matter integrity associated with cognitive deficits in patients with glioma. Brain Behav. 2020, 10, e01639. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Tao, L.; Qian, Z.; Wu, J.; Liu, H.; Yu, Y.; Song, J.; Wang, S.; Sun, J. Altered brain anatomical networks and disturbed connection density in brain tumor patients revealed by diffusion tensor tractography. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 2007–2019. [Google Scholar] [CrossRef] [PubMed]
- Zhong, L.; Li, T.; Shu, H.; Huang, C.; Michael Johnson, J.; Schomer, D.F.; Liu, H.L.; Feng, Q.; Yang, W.; Zhu, H. (TS)(2)WM: Tumor Segmentation and Tract Statistics for Assessing White Matter Integrity with Applications to Glioblastoma Patients. Neuroimage 2020, 223, 117368. [Google Scholar] [CrossRef]
- Cortez-Conradis, D.; Favila, R.; Isaac-Olive, K.; Martinez-Lopez, M.; Rios, C.; Roldan-Valadez, E. Diagnostic performance of regional DTI-derived tensor metrics in glioblastoma multiforme: Simultaneous evaluation of p, q, L, Cl, Cp, Cs, RA, RD, AD, mean diffusivity and fractional anisotropy. Eur. Radiol. 2013, 23, 1112–1121. [Google Scholar] [CrossRef] [PubMed]
- Jutten, K.; Mainz, V.; Gauggel, S.; Patel, H.J.; Binkofski, F.; Wiesmann, M.; Clusmann, H.; Na, C.H. Diffusion Tensor Imaging Reveals Microstructural Heterogeneity of Normal-Appearing White Matter and Related Cognitive Dysfunction in Glioma Patients. Front. Oncol. 2019, 9, 536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, F.; Zhang, X.; Li, M.; Wang, R.; Wang, H.T.; Zhu, F.; Lu, D.J.; Zhao, H.; Li, J.W.; Xu, Y.; et al. Axial diffusivity and tensor shape as early markers to assess cerebral white matter damage caused by brain tumors using quantitative diffusion tensor tractography. CNS Neurosci. Ther. 2012, 18, 667–673. [Google Scholar] [CrossRef] [PubMed]





 ) shows frontal lobe regions, black (
) shows frontal lobe regions, black ( ) shows temporal regions, yellow (
) shows temporal regions, yellow ( ) shows cingulate cortex, and blue (
) shows cingulate cortex, and blue ( ) shows parietal regions of the brain. The chord plot was developed using the HoloViews package (Python version 3.9.7). The color of the arcs/ribbons in the chord plot only shows whether the connections are present among different brain ROIs and do not depict the connection strength. left- left brain hemisphere, right- right brain hemisphere.
) shows frontal lobe regions, black () shows temporal regions, yellow () shows cingulate cortex, and blue () shows parietal regions of the brain. The chord plot was developed using the HoloViews package (Python version 3.9.7). The color of the arcs/ribbons in the chord plot only shows whether the connections are present among different brain ROIs and do not depict the connection strength. left- left brain hemisphere, right- right brain hemisphere.
) shows parietal regions of the brain. The chord plot was developed using the HoloViews package (Python version 3.9.7). The color of the arcs/ribbons in the chord plot only shows whether the connections are present among different brain ROIs and do not depict the connection strength. left- left brain hemisphere, right- right brain hemisphere.
) shows frontal lobe regions, black () shows temporal regions, yellow () shows cingulate cortex, and blue () shows parietal regions of the brain. The chord plot was developed using the HoloViews package (Python version 3.9.7). The color of the arcs/ribbons in the chord plot only shows whether the connections are present among different brain ROIs and do not depict the connection strength. left- left brain hemisphere, right- right brain hemisphere.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PREDICTED | |||
|---|---|---|---|
| ACTUAL | GROUP | LGG | HGG |
| LGG | 54 | 1 | |
| HGG | 1 | 54 | |
| Group | TP | TN | FP | FN | Precision | Recall | Specificity | F1-Score |
|---|---|---|---|---|---|---|---|---|
| LGG | 54 | 54 | 1 | 1 | 0.9818 | 0.9818 | 0.9818 | 0.9818 |
| HGG | 54 | 54 | 1 | 1 | 0.9818 | 0.9818 | 0.9818 | 0.9818 |
| PREDICTED | |||
|---|---|---|---|
| ACTUAL | GROUP | LGG | HGG |
| LGG | 55 | 0 | |
| HGG | 1 | 54 | |
| Group | TP | TN | FP | FN | Precision | Recall | Specificity | F1-score |
|---|---|---|---|---|---|---|---|---|
| LGG | 55 | 54 | 1 | 0 | 0.9821 | 1 | 0.9818 | 0.9909 |
| HGG | 54 | 55 | 0 | 1 | 1 | 0.9818 | 1 | 0.9908 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vidyadharan, S.; Prabhakar Rao, B.V.V.S.N.; Perumal, Y.; Chandrasekharan, K.; Rajagopalan, V. Deep Learning Classifies Low- and High-Grade Glioma Patients with High Accuracy, Sensitivity, and Specificity Based on Their Brain White Matter Networks Derived from Diffusion Tensor Imaging. Diagnostics 2022, 12, 3216. https://doi.org/10.3390/diagnostics12123216
Vidyadharan S, Prabhakar Rao BVVSN, Perumal Y, Chandrasekharan K, Rajagopalan V. Deep Learning Classifies Low- and High-Grade Glioma Patients with High Accuracy, Sensitivity, and Specificity Based on Their Brain White Matter Networks Derived from Diffusion Tensor Imaging. Diagnostics. 2022; 12(12):3216. https://doi.org/10.3390/diagnostics12123216
Chicago/Turabian StyleVidyadharan, Sreejith, Budhiraju Veera Venkata Satya Naga Prabhakar Rao, Yogeeswari Perumal, Kesavadas Chandrasekharan, and Venkateswaran Rajagopalan. 2022. "Deep Learning Classifies Low- and High-Grade Glioma Patients with High Accuracy, Sensitivity, and Specificity Based on Their Brain White Matter Networks Derived from Diffusion Tensor Imaging" Diagnostics 12, no. 12: 3216. https://doi.org/10.3390/diagnostics12123216