
Comparison of 22G Fork-Tip and Franseen Needles and Usefulness of Contrast-Enhanced Endoscopic Ultrasound for Diagnosis of Upper Gastrointestinal Subepithelial Lesions
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Eligibility Criteria
2.3. EUS-FNB Needles (Figure 1)

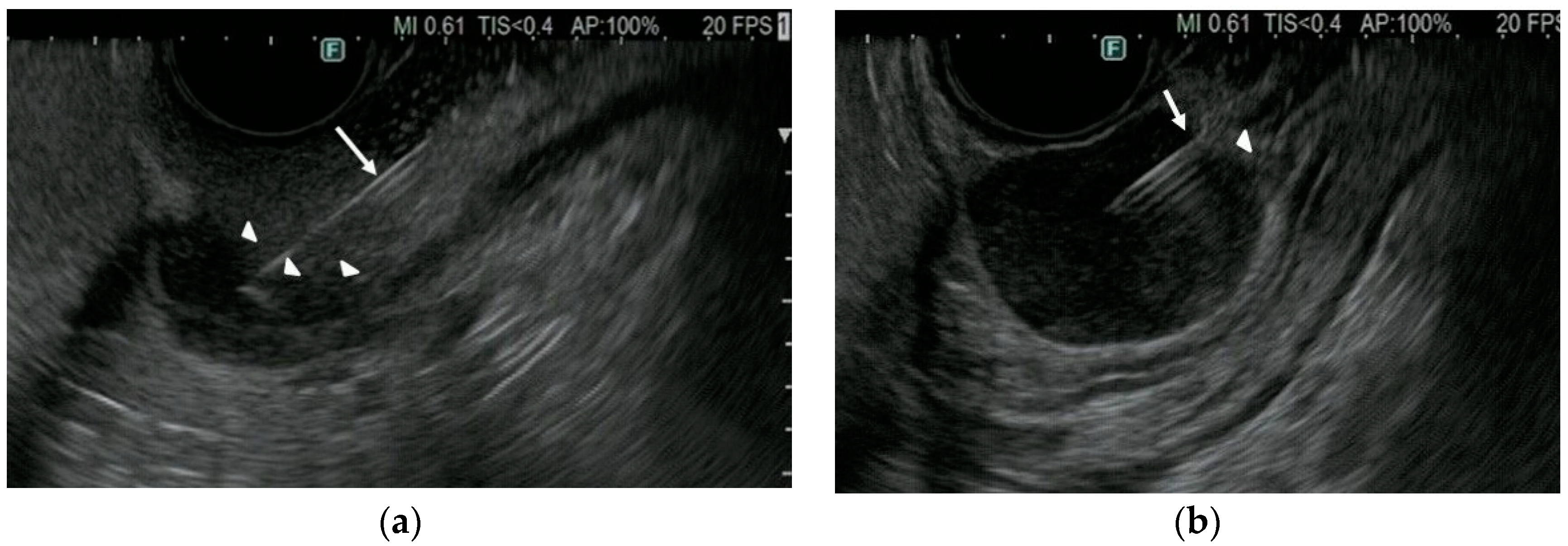
2.4. Procedures
2.5. Pathological Diagnosis
2.6. Final Diagnosis
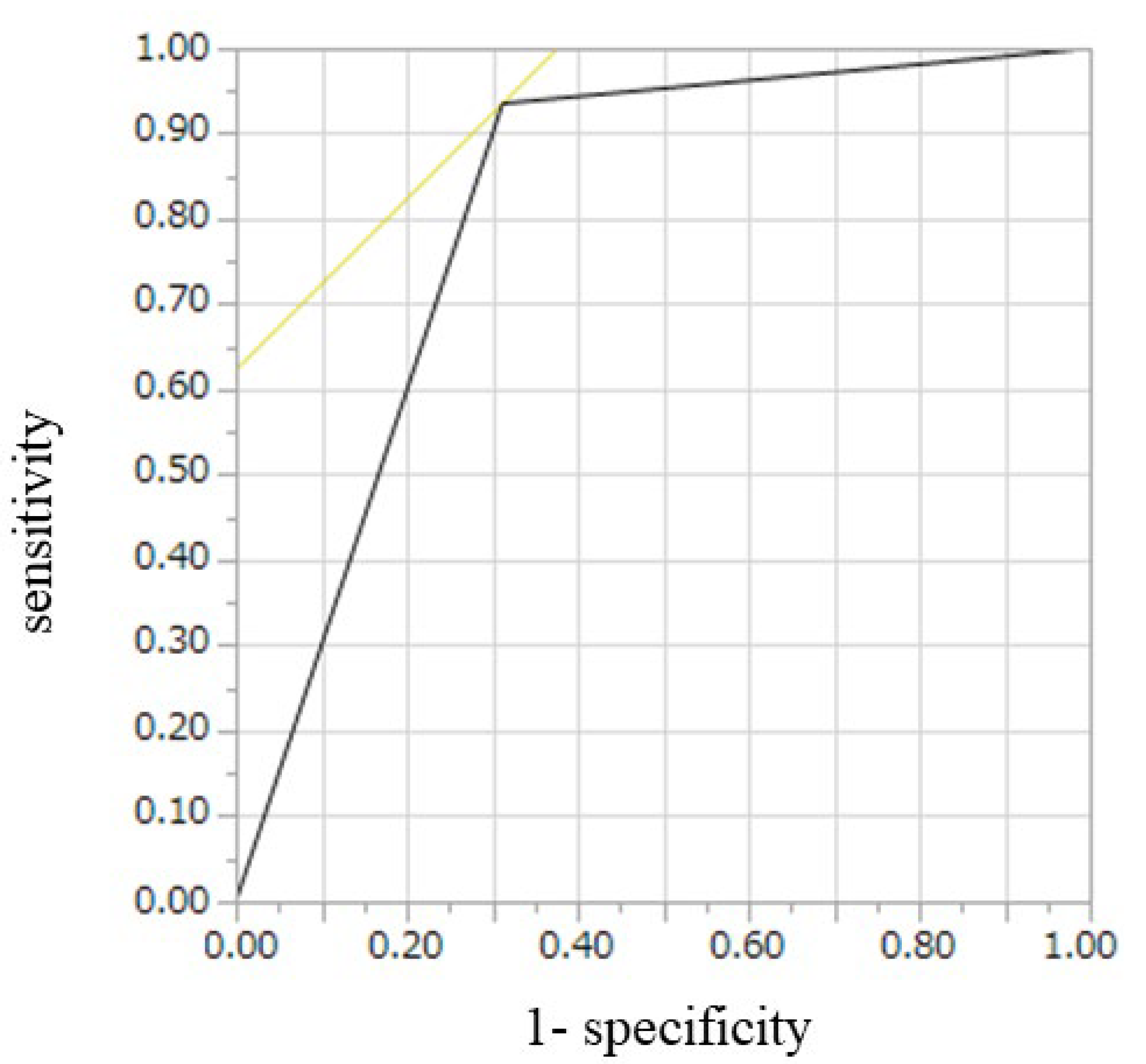
2.7. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Nilsson, B.; Bumming, P.; Meis-Kindblom, J.M.; Odén, A.; Dortok, A.; Gustavsson, B.; Sablinska, K.; Kindblom, L.G. Gastrointestinal stromal tumors: The incidence, prevalence, clinical course, and prognostication in the preimatinib mesylate era--a population-based study in western Sweden. Cancer 2005, 103, 821–829. [Google Scholar] [CrossRef] [PubMed]
- Monges, G.; Bisot-Locard, S.; Blay, J.Y.; Bouvier, A.M.; Urbieta, M.; Coindre, J.M.; Scoazec, J.Y. The estimated incidence of gastrointestinal stromal tumors in France. Results of PROGIST study conducted among pathologists. Bull. Cancer 2010, 97, E16–E22. [Google Scholar] [CrossRef] [PubMed]
- Cassier, P.A.; Ducimetiere, F.; Lurkin, A.; Ranchère-Vince, D.; Scoazec, J.Y.; Bringuier, P.P.; Decouvelaere, A.V.; Méeus, P.; Cellier, D.; Blay, J.Y.; et al. A prospective epidemiological study of new incident GISTs during two consecutive years in Rhone Alpes region: Incidence and molecular distribution of GIST in a European region. Br. J. Cancer 2010, 103, 165–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mastrangelo, G.; Coindre, J.M.; Ducimetiere, F.; Dei Tos, A.P.; Fadda, E.; Blay, J.Y.; Buja, A.; Fedeli, U.; Cegolon, L.; Frasson, A.; et al. Incidence of soft tissue sarcoma and beyond: A population-based prospective study in 3 European regions. Cancer 2012, 118, 5339–5348. [Google Scholar] [CrossRef]
- Miettinen, M.; Lasota, J. Gastrointestinal stromal tumors: Review on morphology, molecular pathology, prognosis, and differential diagnosis. Arch. Pathol. Lab. Med. 2006, 130, 1466–1478. [Google Scholar] [CrossRef]
- Rubin, B.P. Gastrointestinal stromal tumours. An update. Histopathology 2006, 48, 83–96. [Google Scholar] [CrossRef]
- Miettinen, M.; Sarlomo-Rikala, M.; Lasota, J. Gastrointestinal stromal tumors: Recent advances in understanding of their biology. Hum. Pathol. 1999, 30, 1213–1220. [Google Scholar] [CrossRef]
- ESMO/European Sarcoma Network Working Group. Gastrointestinal stromal tumors: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2012, 23 (Suppl. S7), vii49–vii55. [Google Scholar]
- Akahoshi, K.; Sumida, Y.; Matsui, N.; Oya, M.; Akinaga, R.; Kubokawa, M.; Motomura, Y.; Honda, K.; Watanabe, M.; Nagaie, T. Preoperative diagnosis of gastrointestinal stromal tumor by endoscopic ultrasound-guided fine needle aspiration. World J. Gastroenterol. 2007, 13, 2077–2082. [Google Scholar] [CrossRef]
- Nishida, T.; Kawai, N.; Yamaguchi, S.; Nishida, Y. Submucosal tumors: Comprehensive guide for the diagnosis and therapy of gastrointestinal submucosal tumors. Dig. Endosc. 2013, 25, 479–489. [Google Scholar] [CrossRef]
- Nishida, T.; Hirota, S.; Yanagisawa, A.; Sugino, Y.; Minami, M.; Yamamura, Y.; Otani, Y.; Shimada, Y.; Takahashi, F.; Kubota, T.; et al. Clinical practice guidelines for gastrointestinal stromal tumor (GIST) in Japan: English version. Int. J. Clin. Oncol. 2008, 13, 416–430. [Google Scholar] [CrossRef] [PubMed]
- Polkowski, M.; Butruk, E. Submucosal lesions. Gastrointest. Endosc. Clin. 2005, 15, 33–54. [Google Scholar] [CrossRef] [PubMed]
- Landi, B.; Palazzo, L. The role of endosonography in submucosal tumours. Best Pract. Res. Clin. Gastroenterol. 2009, 23, 679–701. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.H.; Saunders, M.D.; Rulyak, S.J.; Shaw, S.; Nietsch, H.; Kimmey, M.B. A prospective study comparing endoscopy and EUS in the evaluation of GI subepithelial masses. Gastrointest. Endosc. 2005, 62, 202–208. [Google Scholar] [CrossRef]
- Reddy, N.K.; Ioncica, A.M.; Saftoiu, A.; Vilmann, P.; Bhutani, M.S. Contrast-enhanced endoscopic ultrasonography. World J. Gastroenterol. 2011, 17, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Kamata, K.; Takenaka, M.; Kitano, M.; Omoto, S.; Miyata, T.; Minaga, K.; Yamao, K.; Imai, H.; Sakurai, T.; Watanabe, T.; et al. Contrast-enhanced harmonic endoscopic ultrasonography for differential diagnosis of submucosal tumors of the upper gastrointestinal tract. J. Gastroenterol. Hepatol. 2017, 32, 1686–1692. [Google Scholar] [CrossRef]
- Buscaglia, J.M.; Nagula, S.; Jayaraman, V.; Robbins, D.H.; Vadada, D.; Gross, S.A.; DiMaio, C.J.; Pais, S.; Patel, K.; Sejpal, D.V.; et al. Diagnostic yield and safety of jumbo biopsy forceps in patients with subepithelial lesions of the upper and lower GI tract. Gastrointest. Endosc. 2012, 75, 1147–1152. [Google Scholar] [CrossRef]
- Ji, J.S.; Lee, B.I.; Choi, K.Y.; Kim, B.W.; Choi, H.; Huh, M.; Chung, W.C.; Chae, H.S.; Chung, I.S. Diagnostic yield of tissue sampling using a bite-on-bite technique for incidental subepithelial lesions. Korean J. Intern. Med. 2009, 24, 101–105. [Google Scholar] [CrossRef]
- Volmar, K.E.; Vollmer, R.T.; Jowell, P.S.; Nelson, R.C.; Xie, H.B. Pancreatic FNA in 1000 cases: A comparison of imaging modalities. Gastrointest. Endosc. 2005, 61, 854–861. [Google Scholar] [CrossRef]
- Iglesias-Garcia, J.; Dominguez-Munoz, J.E.; Abdulkader, I.; Larino-Noia, J.; Eugenyeva, E.; Lozano-Leon, A.; Forteza-Vila, J. Influence of on-site cytopathology evaluation on the diagnostic accuracy of endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) of solid pancreatic masses. Am. J. Gastroenterol. 2011, 106, 1705–1710. [Google Scholar] [CrossRef]
- Moon, J.S. Endoscopic ultrasound-guided fine needle aspiration in submucosal lesion. Clin. Endosc. 2012, 45, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Akahoshi, K.; Oya, M.; Koga, T.; Koga, H.; Motomura, Y.; Kubokawa, M.; Gibo, J.; Nakamura, K. Clinical usefulness of endoscopic ultrasound-guided fine needle aspiration for gastric subepithelial lesions smaller than 2 cm. J. Gastrointest. Liver Dis. 2014, 23, 405–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attila, T.; Aydın, Ö. Lesion size determines diagnostic yield of EUS-FNA with onsite cytopathologic evaluation for upper gastrointestinal subepithelial lesions. Turk. J. Gastroenterol. 2018, 29, 436–441. [Google Scholar] [CrossRef] [PubMed]
- Adler, D.G.; Muthusamy, V.R.; Ehrlich, D.S.; Parasher, G.; Thosani, N.C.; Chen, A.; Buscaglia, J.M.; Appannagari, A.; Quintero, E.; Aslanian, H.; et al. A multicenter evaluation of a new EUS core biopsy needle: Experience in 200 patients. Endosc. Ultrasound 2019, 8, 99–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DiMaio, C.J.; Kolb, J.M.; Benias, P.C.; Shah, H.; Shah, S.; Haluszka, O.; Maranki, J.; Sharzehi, K.; Lam, E.; Gordon, S.R.; et al. Initial experience with a novel EUS-guided core biopsy needle (SharkCore): Results of a large North American multicenter study. Endosc. Int. Open 2016, 4, E974–E979. [Google Scholar] [CrossRef] [Green Version]
- Kim, G.H.; Cho, Y.K.; Kim, E.Y.; Kim, H.K.; Cho, J.W.; Lee, T.H.; Moon, J.S.; Korean EUS Study Group. Comparison of 22-gauge aspiration needle with 22-gauge biopsy needle in endoscopic ultrasonography-guided subepithelial tumor sampling. Scand. J. Gastroenterol. 2014, 49, 347–354. [Google Scholar] [CrossRef]
- Hedenström, P.; Marschall, H.U.; Nilsson, B.; Demir, A.; Lindkvist, B.; Nilsson, O.; Sadik, R. High clinical impact and diagnostic accuracy of EUS-guided biopsy sampling of subepithelial lesions: A prospective, comparative study. Surg. Endosc. 2018, 32, 1304–1313. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, C.D.; Berman, J.J.; Corless, C.; Gorstein, F.; Lasota, J.; Longley, B.; Miettinen, M.; O’Leary, T.J.; Remotti, H.; Rubin, B.P.; et al. Diagnosis of gastrointestinal stromal tumors: A consensus approach. Hum. Pathol. 2002, 33, 459–465. [Google Scholar] [CrossRef] [Green Version]
- Miettinen, M.; Sobin, L.H.; Lasota, J. Gastrointestinal stromal tumors of the stomach: A clinicopathologic, immunohistochemical, and molecular genetic study of 1765 cases with long-term follow-up. Am. J. Surg. Pathol. 2005, 29, 52–68. [Google Scholar] [CrossRef]
- Yang, Z.; Feng, X.; Zhang, P.; Chen, T.; Qiu, H.; Zhou, Z.; Li, G.; Tao, K.X.; Li, Y.; China Gastrointestinal Stromal Tumor Study Group (CN-GIST). Clinicopathological features and prognosis of 276 cases of primary small (≤2 cm) gastric gastrointestinal stromal tumors: A multicenter data review. Surg. Endosc. 2019, 33, 2982–2990. [Google Scholar] [CrossRef]
- Zhang, X.C.; Li, Q.L.; Yu, Y.F.; Yao, L.Q.; Xu, M.D.; Zhang, Y.Q.; Zhong, Y.S.; Chen, W.F.; Zhou, P.H. Diagnostic efficacy of endoscopic ultrasound-guided needle sampling for upper gastrointestinal subepithelial lesions: A meta-analysis. Surg. Endosc. 2016, 30, 2431–2441. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Sun, X.; Ge, N.; Wang, S.; Guo, J.; Liu, X.; Wang, G.; Sun, S. The necessarity of treatment for small gastric subepithelial tumors (1-2 cm) originating from muscularis propria: An analysis of 972 tumors. BMC Gastroenterol. 2022, 22, 182. [Google Scholar] [CrossRef] [PubMed]
- Iwai, T.; Kida, M.; Imaizumi, H.; Miyazawa, S.; Okuwaki, K.; Yamauchi, H.; Kaneko, T.; Hasegawa, R.; Miyata, E.; Koizumi, W. Randomized crossover trial comparing EUS-guided fine-needle aspiration with EUS-guided fine-needle biopsy for gastric subepithelial tumors. Diagn. Cytopathol. 2018, 46, 228–233. [Google Scholar] [CrossRef]
- Bang, J.Y.; Hebert-Magee, S.; Navaneethan, U.; Hasan, M.K.; Hawes, R.; Varadarajulu, S. Randomized trial comparing the Franseen and Fork-tip needles for EUS-guided fine-needle biopsy sampling of solid pancreatic mass lesions. Gastrointest. Endosc. 2018, 87, 1432–1438. [Google Scholar] [CrossRef] [PubMed]
- Ashat, M.; Klair, J.S.; Rooney, S.L.; Vishal, S.J.; Jensen, C.; Sahar, N.; Murali, A.R.; El-Abiad, R.; Gerke, H. Randomized controlled trial comparing the Franseen needle with the Fork-tip needle for EUS-guided fine-needle biopsy. Gastrointest. Endosc. 2021, 93, 140–150. [Google Scholar] [CrossRef] [PubMed]
- Mohan, B.P.; Shakhatreh, M.; Garg, R.; Asokkumar, R.; Jayaraj, M.; Ponnada, S.; Navaneethan, U.; Adler, D.G. Comparison of Franseen and fork-tip needles for EUS-guided fine-needle biopsy of solid mass lesions: A systematic review and meta-analysis. Endosc. Ultrasound 2019, 8, 382–391. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Fork-Tip Needle (n = 23) | Franseen Needle (n = 34) | p-Value | |
|---|---|---|---|
| Age, year, median (range) | 69 (24–77) | 66 (32–81) | 0.59 |
| Sex, male/female | 12/11 | 16/18 | 0.79 |
| Size of mass, mm, median (range) | 18 (7–20) | 15 (10–20) | 0.23 |
| Location | |||
| Esophagus | 0 | 3 | 0.27 |
| Stomach | 23 | 30 | 0.14 |
| Duodenum | 0 | 1 | 1.0 |
| Final diagnosis | |||
| GIST | 15 | 16 | 0.28 |
| Very low risk | 8 | 7 | |
| Low risk | 3 | 6 | |
| Intermediate risk | 2 | 3 | |
| Unknown | 2 | ||
| Non-GIST | 5 | 9 | |
| Leiomyoma | 6 | 8 | |
| Inflamed fibrous stromal tissue | 0 | 1 | |
| Lipoma | 1 | 0 | |
| Not diagnosed | 1 | 9 |
| Fork-Tip Needle (n = 23) | Franseen Needle (n = 34) | p-Value | |
|---|---|---|---|
| Number of needle passes | 2.5 (1–7) | 3 (1–5) | 0.86 |
| Technical success (puncture success) | 100% (23/23) | 100% (34/34) | - |
| Adverse event | 0% (0/23) | 2.9% (1/34) | 1.0 |
| Adequate sampling acquisition rate | 96% (22/23) | 74% (25/34) | 0.038 |
| Final Diagnosis | ||
|---|---|---|
| GIST (n = 31) | Non-GIST (n = 16) | |
| Hyper- or iso-enhancement pattern on CH-EUS | 29 | 5 |
| Hypo-enhancement pattern on CH-EUS | 2 | 11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamashita, Y.; Ashida, R.; Yamazaki, H.; Kawaji, Y.; Shimokawa, T.; Tamura, T.; Hatamaru, K.; Itonaga, M.; Kitano, M. Comparison of 22G Fork-Tip and Franseen Needles and Usefulness of Contrast-Enhanced Endoscopic Ultrasound for Diagnosis of Upper Gastrointestinal Subepithelial Lesions. Diagnostics 2022, 12, 3122. https://doi.org/10.3390/diagnostics12123122
Yamashita Y, Ashida R, Yamazaki H, Kawaji Y, Shimokawa T, Tamura T, Hatamaru K, Itonaga M, Kitano M. Comparison of 22G Fork-Tip and Franseen Needles and Usefulness of Contrast-Enhanced Endoscopic Ultrasound for Diagnosis of Upper Gastrointestinal Subepithelial Lesions. Diagnostics. 2022; 12(12):3122. https://doi.org/10.3390/diagnostics12123122
Chicago/Turabian StyleYamashita, Yasunobu, Reiko Ashida, Hirofumi Yamazaki, Yuki Kawaji, Toshio Shimokawa, Takashi Tamura, Keiichi Hatamaru, Masahiro Itonaga, and Masayuki Kitano. 2022. "Comparison of 22G Fork-Tip and Franseen Needles and Usefulness of Contrast-Enhanced Endoscopic Ultrasound for Diagnosis of Upper Gastrointestinal Subepithelial Lesions" Diagnostics 12, no. 12: 3122. https://doi.org/10.3390/diagnostics12123122