
Asphyxia-Induced Bacterial Translocation in an Animal Experimental Model in Neonatal Piglets

 ,
,  , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal Preparation
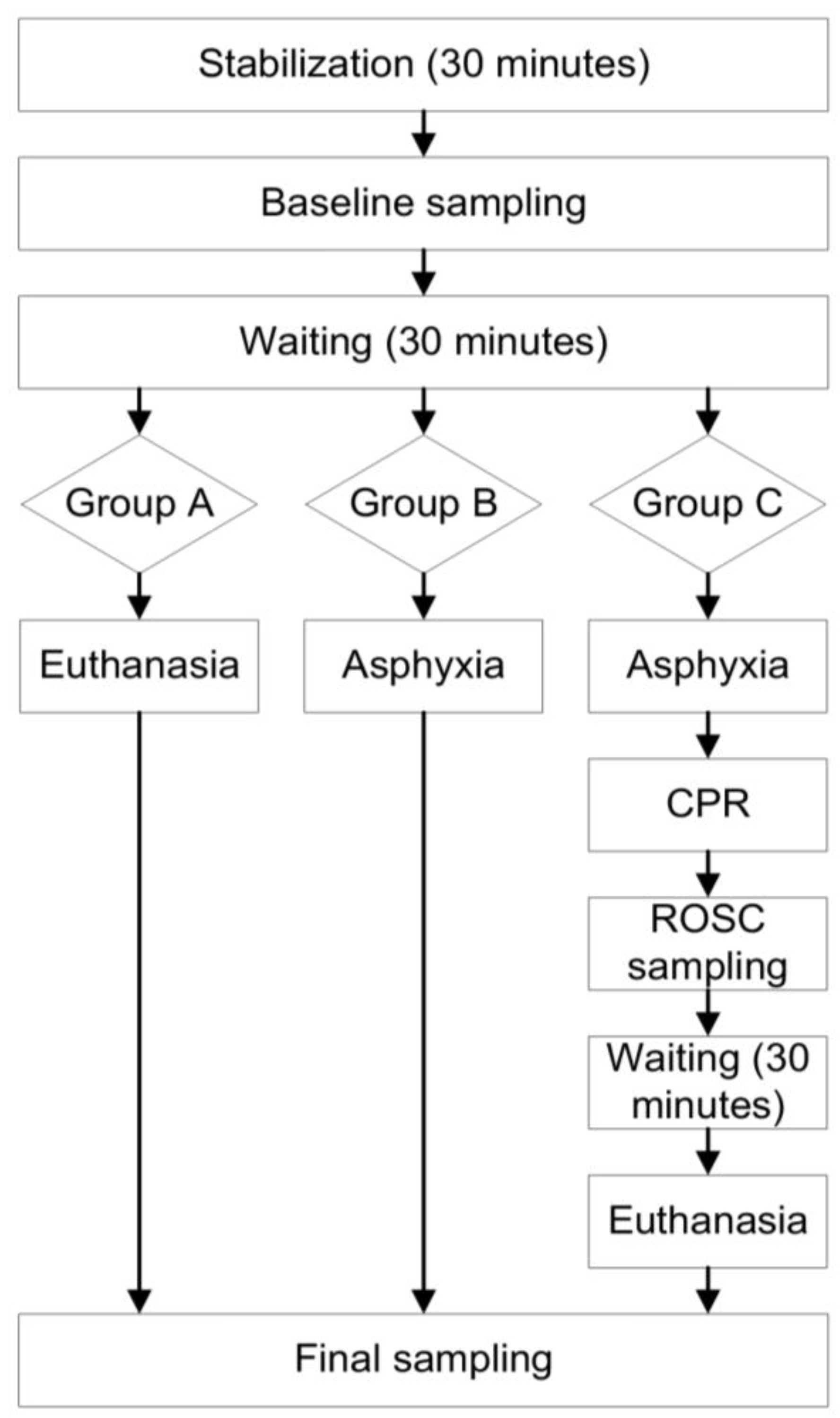
2.2. Experimental Procedure
2.3. Experiment Outcome Points
- Main outcome: presence of endotoxin in MLNs, aorta and portal vein;
- Secondary outcome: hemodynamic parameters.
2.4. Endotoxin Analysis
2.5. Statistical Analysis
3. Results
3.1. Haemodynamic Parameters & Basic Laboratory Tests
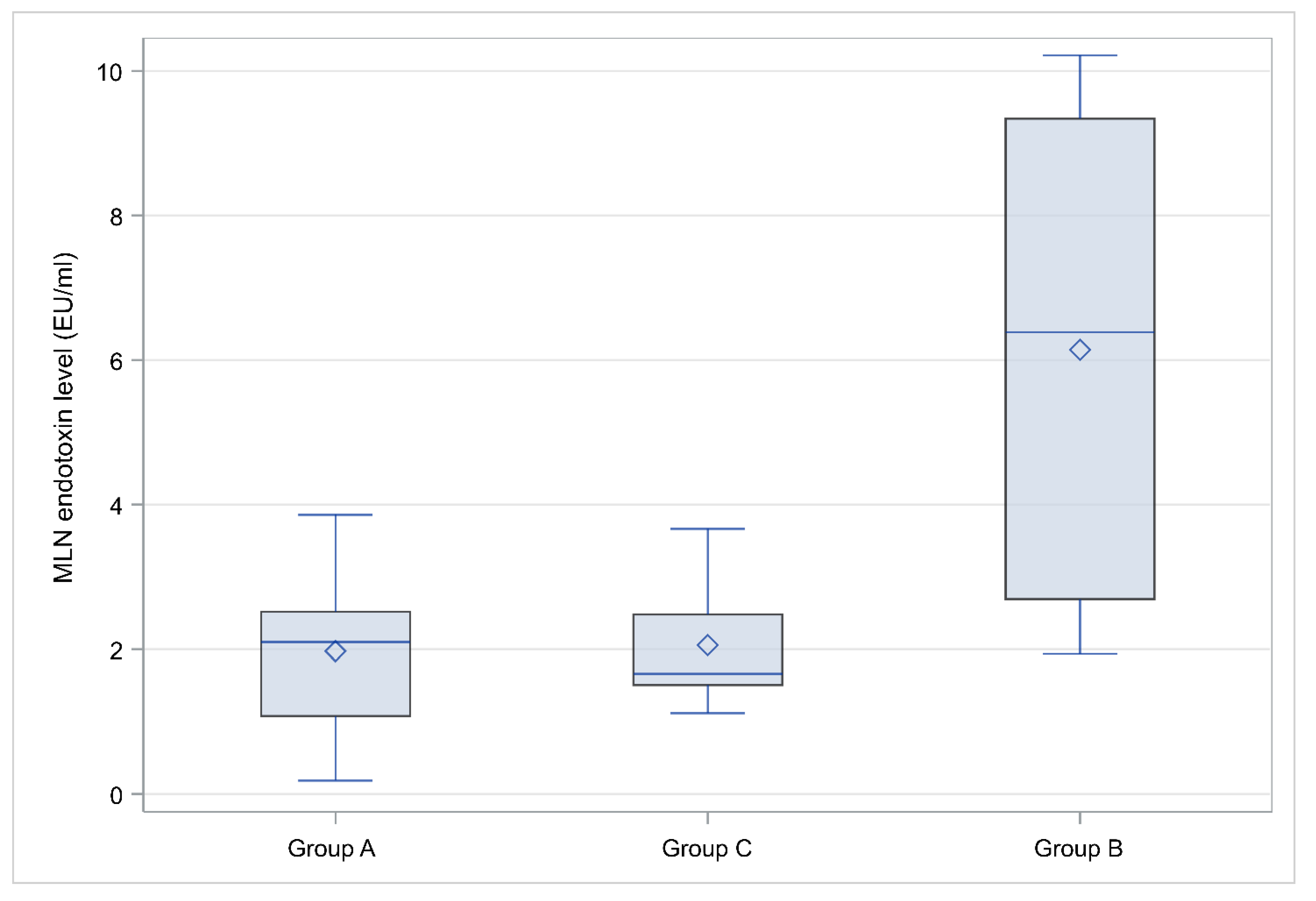
3.2. Endotoxin Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Millar, L.J.; Shi, L.; Hoerder-Suabedissen, A.; Molnar, Z. Neonatal Hypoxia Ischaemia: Mechanisms, Models, and Therapeutic Challenges. Front. Cell. Neurosci. 2017, 11, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonucci, R.; Porcella, A.; Pilloni, M.D. Perinatal asphyxia in the term newborn. J. Pediatr. Neonatal Individ. Med. 2014, 3, e030269. [Google Scholar]
- Rainaldi, M.A.; Perlman, J.M. Pathophysiology of Birth Asphyxia. Clin. Perinatol. 2016, 43, 409–422. [Google Scholar] [CrossRef]
- Matara, D.I.; Pouliakis, A.; Xanthos, T.; Sokou, R.; Kafalidis, G.; Iliodromiti, Z.; Boutsikou, T.; Iacovidou, N.; Salakos, C. Microbial Translocation and Perinatal Asphyxia/Hypoxia: A Systematic Review. Diagnostics 2022, 12, 214. [Google Scholar] [CrossRef]
- Short, S.S.; Papillon, S.; Berel, D.; Ford, H.R.; Frykman, P.K.; Kawaguchi, A. Late onset of necrotizing enterocolitis in the full-term infant is associated with increased mortality: Results from a two-center analysis. J. Pediatr. Surg. 2014, 49, 950–953. [Google Scholar] [CrossRef] [Green Version]
- Iben, S.; Rodriguez, R.J. Neonatal necrotizing enterocolitis. In Pediatric Gastrointestinal and Liver Disease, 4th ed.; Wyllie, R., Hyams, J., Eds.; Elsevier: Amsterdam, The Netherlands, 2011; p. 1104. [Google Scholar]
- Patel, R.M.; Denning, P.W. Intestinal microbiota and its relationship with necrotizing enterocolitis. Pediatr. Res. 2015, 78, 232–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beutler, B.; Rietschel, E.T. Innate immune sensing and its roots: The story of endotoxin. Nat. Rev. Immunol. 2003, 3, 169–176. [Google Scholar] [CrossRef]
- Jiang, J.; Bahrami, S.; Leichtfried, G.; Redl, H.; Ohlinger, W.; Schlag, G. Kinetics of endotoxin and tumor necrosis factor appearance in portal and systemic circulation after hemorrhagic shock in rats. Ann. Surg. 1995, 221, 100–106. [Google Scholar] [CrossRef]
- Hackam, D.J.; Upperman, J.S.; Grishin, A.; Ford, H.R. Disordered enterocyte signaling and intestinal barrier dysfunction in the pathogenesis of necrotizing enterocolitis. Semin. Pediatr. Surg. 2005, 14, 49–57. [Google Scholar] [CrossRef]
- Ares, G.J.; McElroy, S.J.; Hunter, C.J. The science and necessity of using animal models in the study of necrotizing enterocolitis. Semin. Pediatr. Surg. 2018, 27, 29–33. [Google Scholar] [CrossRef]
- Azcarate-Peril, M.A.; Foster, D.M.; Cadenas, M.B.; Stone, M.R.; Jacobi, S.K.; Stauffer, S.H.; Pease, A.; Gookin, J.L. Acute necrotizing enterocolitis of preterm piglets is characterized by dysbiosis of ileal mucosa-associated bacteria. Gut Microbes 2011, 2, 234–243. [Google Scholar] [CrossRef] [PubMed]
- Barre-Sinoussi, F.; Montagutelli, X. Animal models are essential to biological research: Issues and perspectives. Future Sci. OA 2015, 1, FSO63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raffay, V.; Chalkias, A.; Lelovas, P.; Karlis, G.; Koutsovasilis, A.; Papalois, A.; Jevdjic, J.; Fiser, Z.; Xanthos, T. Addition of glucagon to adrenaline improves hemodynamics in a porcine model of prolonged ventricular fibrillation. Am. J. Emerg. Med. 2014, 32, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Papalexopoulou, K.; Chalkias, A.; Pliatsika, P.; Papalois, A.; Papapanagiotou, P.; Papadopoulos, G.; Arnaoutoglou, E.; Petrou, A.; Gulati, A.; Xanthos, T. Centhaquin Effects in a Swine Model of Ventricular Fibrillation: Centhaquin and Cardiac Arrest. Heart Lung Circ. 2017, 26, 856–863. [Google Scholar] [CrossRef]
- Chalkias, A.; Spyropoulos, V.; Koutsovasilis, A.; Papalois, A.; Kouskouni, E.; Xanthos, T. Cardiopulmonary Arrest and Resuscitation in Severe Sepsis and Septic Shock: A Research Model. Shock 2015, 43, 285–291. [Google Scholar] [CrossRef]
- Kontouli, Z.; Staikou, C.; Iacovidou, N.; Mamais, I.; Kouskouni, E.; Papalois, A.; Papapanagiotou, P.; Gulati, A.; Chalkias, A.; Xanthos, T. Resuscitation with centhaquin and 6% hydroxyethyl starch 130/0.4 improves survival in a swine model of hemorrhagic shock: A randomized experimental study. Eur. J. Trauma Emerg. Surg. 2019, 45, 1077–1085. [Google Scholar] [CrossRef]
- Madar, J.; Roehr, C.C.; Ainsworth, S.; Ersdal, H.; Morley, C.; Rudiger, M.; Skare, C.; Szczapa, T.; Te Pas, A.; Trevisanuto, D.; et al. European Resuscitation Council Guidelines 2021: Newborn resuscitation and support of transition of infants at birth. Resuscitation 2021, 161, 291–326. [Google Scholar] [CrossRef]
- Wyllie, J.; Bruinenberg, J.; Roehr, C.C.; Rudiger, M.; Trevisanuto, D.; Urlesberger, B. European Resuscitation Council Guidelines for Resuscitation 2015: Section 7. Resuscitation and support of transition of babies at birth. Resuscitation 2015, 95, 249–263. [Google Scholar] [CrossRef] [Green Version]
- Lewis, D.I. Animal experimentation: Implementation and application of the 3Rs. Emerg. Top. Life Sci. 2019, 3, 675–679. [Google Scholar] [CrossRef]
- Smith, A.J.; Lilley, E. The Role of the Three Rs in Improving the Planning and Reproducibility of Animal Experiments. Anim. Open Access J. 2019, 9, 975. [Google Scholar] [CrossRef] [Green Version]
- Brouillette, R.T.; Waxman, D.H. Evaluation of the newborn’s blood gas status. National Academy of Clinical Biochemistry. Clin. Chem. 1997, 43, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Chalkias, A.; Mamais, I.; Xanthos, T. Microcirculation-mediated preconditioning and intracellular hypothermia. Med. Hypotheses 2018, 115, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Varvarousis, D.; Xanthos, T.; Ferino, G.; Noto, A.; Iacovidou, N.; Mura, M.; Scano, P.; Chalkias, A.; Papalois, A.; De-Giorgio, F.; et al. Metabolomics profiling reveals different patterns in an animal model of asphyxial and dysrhythmic cardiac arrest. Sci. Rep. 2017, 7, 16575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tassopoulos, A.; Chalkias, A.; Papalois, A.; Karlovasiti, P.; Zanda, J.S.A.; Chatzidakis, S.; Gazouli, M.; Iacovidou, N.; Fanni, D.; Xanthos, T. Assessment of Post-Resuscitation Intestinal Injury and Timing of Bacterial Translocation in Swine Anaesthetized With Propofol-Based Total Intravenous Anaesthesia. Cureus 2020, 12, e10362. [Google Scholar] [CrossRef] [PubMed]
- Grimaldi, D.; Sauneuf, B.; Guivarch, E.; Ricome, S.; Geri, G.; Charpentier, J.; Zuber, B.; Dumas, F.; Spaulding, C.; Mira, J.P.; et al. High Level of Endotoxemia Following Out-of-Hospital Cardiac Arrest Is Associated With Severity and Duration of Postcardiac Arrest Shock. Crit. Care Med. 2015, 43, 2597–2604. [Google Scholar] [CrossRef]
- van Deventer, S.J.; ten Cate, J.W.; Tytgat, G.N. Intestinal endotoxemia. Clinical significance. Gastroenterology 1988, 94, 825–831. [Google Scholar] [CrossRef]
- Munford, R.S. Endotoxemia-menace, marker, or mistake? J. Leukoc. Biol. 2016, 100, 687–698. [Google Scholar] [CrossRef] [Green Version]
- Chalkias, A.; Xanthos, T.; Papageorgiou, E.; Anania, A.; Beloukas, A.; Pavlopoulos, F. Intraoperative initiation of a modified ARDSNet protocol increases survival of septic patients with severe acute respiratory distress syndrome. Heart Lung 2018, 47, 616–621. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Group A | Group B | Group C | ||
|---|---|---|---|---|
| Characteristic | Median [Q1–Q3] | Median [Q1–Q3] | Median [Q1–Q3] | p |
| Body Weight (gr) | 1600 [1400–1800] | 1550 [1100–1700] | 1500 [1260–1600] | 0.7475 |
| Group A | Group B | Group C | ||
|---|---|---|---|---|
| Characteristic (Baseline) | Median [Q1–Q3] | Median [Q1–Q3] | Median [Q1–Q3] | p |
| WBC (103/μL) | 6.2 [5–10.8] | 4.4 [1.4–8.4] | 2.7 [2.3–5.7] | 0.2607 |
| Hb (g/dL) | 6.85 [6.6–7.2] | 6.7 [5.9–7.2] | 6.2 [5.6–7.3] | 0.9292 |
| AP (mmHg) | 55 [53–57] | 58 [49–64] | 53 [50–64] | 0.9609 |
| HR (beats per min) | 151 [136–164] | 136 [120–175] | 152 [130–172] | 0.9774 |
| spO2 (%) | 100 [99–100] | 100 [99–100] | 100 [99–100] | 0.9646 |
| CVP (mmHg) | 3.5 [1–7] | 4 [2–4] | 3 [2–7] | 0.9762 |
| Temperature (°C) | 38 [37.9–38.2] | 38 [37.7–38.1] | 38 [37.2–38.5] | 0.8843 |
| pH | 7.315 [7.3–7.45] | 7.3 [7.3–7.36] | 7.3 [7.3–7.38] | 0.7348 |
| HCO3 (mEq/L) | 24.8 [23.4–28.4] | 26.3 [24.5–27.6] | 25.3 [22.5–27.9] | 0.7595 |
| BE (mEq/L) | 1.45 [−2.7–2.3] | −0.7 [−2–1.4] | −1.4 [−2.3–2.4] | 0.8624 |
| Lac (mg/dL) | 0.65 [0.56–0.78] | 0.65 [0.47–0.88] | 0.63 [0.42–0.91] | 0.8517 |
| Group B | Group C | ||
|---|---|---|---|
| Characteristic (Asphyxia) | Median [Q1–Q3] | Median [Q1–Q3] | p |
| AP (mmHg) | 27 [15–51] | 28.5 [18–41] | 0.7963 |
| HR (beats per min) | 57 [42–57] | 57 [56–58] | 0.3723 |
| pH | 6.85 [6.63–7.1] | 6.75 [6.63–6.98] | 0.7745 |
| HCO3 (mEq/L) | 23 [22.9–24] | 19.1 [17.6–20] | 0.1441 |
| BE (mEq/L) | ΝA | −13.7 [−13.7–−13.7] | NA |
| Lac (mg/dL) | 11.55 [11.5–11.6] | 9.4 [5.46–12.4] | 0.5637 |
| Group C | |
|---|---|
| Characteristic (ROSC) | Median [Q1–Q3] |
| AP (mmHg) | 52 [30–90] |
| HR (beats per min) | 158 [133–172] |
| spO2 (%) | 100 [97–100] |
| CVP (mmHg) | 4.5 [1–8] |
| pH | 7 [6.82–7.03] |
| HCO3 (mEq/L) | 17.2 [16.2–19.6] |
| BE (mEq/L) | −13.7 [−15.4–10.6] |
| Lac (mg/dL) | 6.14 [4.83–7.03] |
| Group A | Group B | Group C | ||
|---|---|---|---|---|
| Characteristic (Final) | Median [Q1–Q3] | Median [Q1–Q3] | Median [Q1–Q3] | p |
| AP (mmHg) | 55.5 [53–58] | 42 [42–42] | 56 [50–74] | 0.2696 |
| HR (beats per min) | 146 [130–162] | 128 [128–128] | 165 [151–181] | 0.0868 |
| spO2 (%) | 100 [99–100] | 99 [99–99] | 100 [99–100] | 0.5857 |
| CVP (mmHg) | 2.5 [2–5] | 3 [3–3] | 4 [2–5] | 0.8041 |
| pH | 7.315 [7.3–7.49] | 6.86 [6.86–6.86] | 7.17 [7.1–7.2] | 0.0367 |
| HCO3 (mEq/L) | 24.35 [23.4–28.3] | ΝA | 22.1 [19.1–22.4] | 0.0223 |
| BE (mEq/L) | −0.85 [−2.1–1.8] | ΝA | −6 [−9–−5.1] | 0.0223 |
| Lac (mg/dL) | 0.74 [0.63–0.83] | ΝA | 3.37 [2.71–6.28] | 0.0027 |
| Group A | Group B | Group C | ||
|---|---|---|---|---|
| Anatomic Location | Median [Q1–Q3] | Median [Q1–Q3] | Median [Q1–Q3] | p |
| Endotoxinportal (EU/mL) | 12.5 [11.9–14.3] | 8.1 [0.7–15.7] | 8.1 [2.5–13.6] | 0.1917 |
| Endotoxinaorta (EU/mL) | 11.7 [7.5–12.8] | 7.9 [5.8–10.1] | 9.3 [7.5–10.2] | 0.4438 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matara, D.-I.; Sokou, R.; Xanthos, T.; Pouliakis, A.; Sarantaki, A.; Boutsikou, T.; Iliodromiti, Z.; Salakos, C.; Gazouli, M.; Iacovidou, N. Asphyxia-Induced Bacterial Translocation in an Animal Experimental Model in Neonatal Piglets. Diagnostics 2022, 12, 3103. https://doi.org/10.3390/diagnostics12123103
Matara D-I, Sokou R, Xanthos T, Pouliakis A, Sarantaki A, Boutsikou T, Iliodromiti Z, Salakos C, Gazouli M, Iacovidou N. Asphyxia-Induced Bacterial Translocation in an Animal Experimental Model in Neonatal Piglets. Diagnostics. 2022; 12(12):3103. https://doi.org/10.3390/diagnostics12123103
Chicago/Turabian StyleMatara, Dimitra-Ifigeneia, Rozeta Sokou, Theodoros Xanthos, Abraham Pouliakis, Antigoni Sarantaki, Theodora Boutsikou, Zoi Iliodromiti, Christos Salakos, Maria Gazouli, and Nicoletta Iacovidou. 2022. "Asphyxia-Induced Bacterial Translocation in an Animal Experimental Model in Neonatal Piglets" Diagnostics 12, no. 12: 3103. https://doi.org/10.3390/diagnostics12123103