
The Efficiency of Photodynamic Therapy in the Bacterial Decontamination of Periodontal Pockets and Its Impact on the Patient
 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants Selection
- Men and women > 25 years
- No periodontal treatment or intake of antibiotics in the last 6 months
- At least 12 natural teeth present in the oral cavity distributed in all four quadrants
- Satisfactory individual oral hygiene (Plaque index > 25%)
- The presence of bleeding during the periodontal survey
- At least 4 teeth with at least one periodontal pocket (PD) ≥ 4 mm at initial assessment, but not more than 30% of the existent teeth
- Clinical and radiographic signs of localized chronic periodontitis [18]
- Pregnancy and/or lactation period
- Allergy to Tolonium chloride (Toluidine Blue Gel 0.005%)
- Any systemic conditions that could affect the progression and treatment of periodontal diseases, such as type 1 and 2 diabetes
- Alcohol abuse
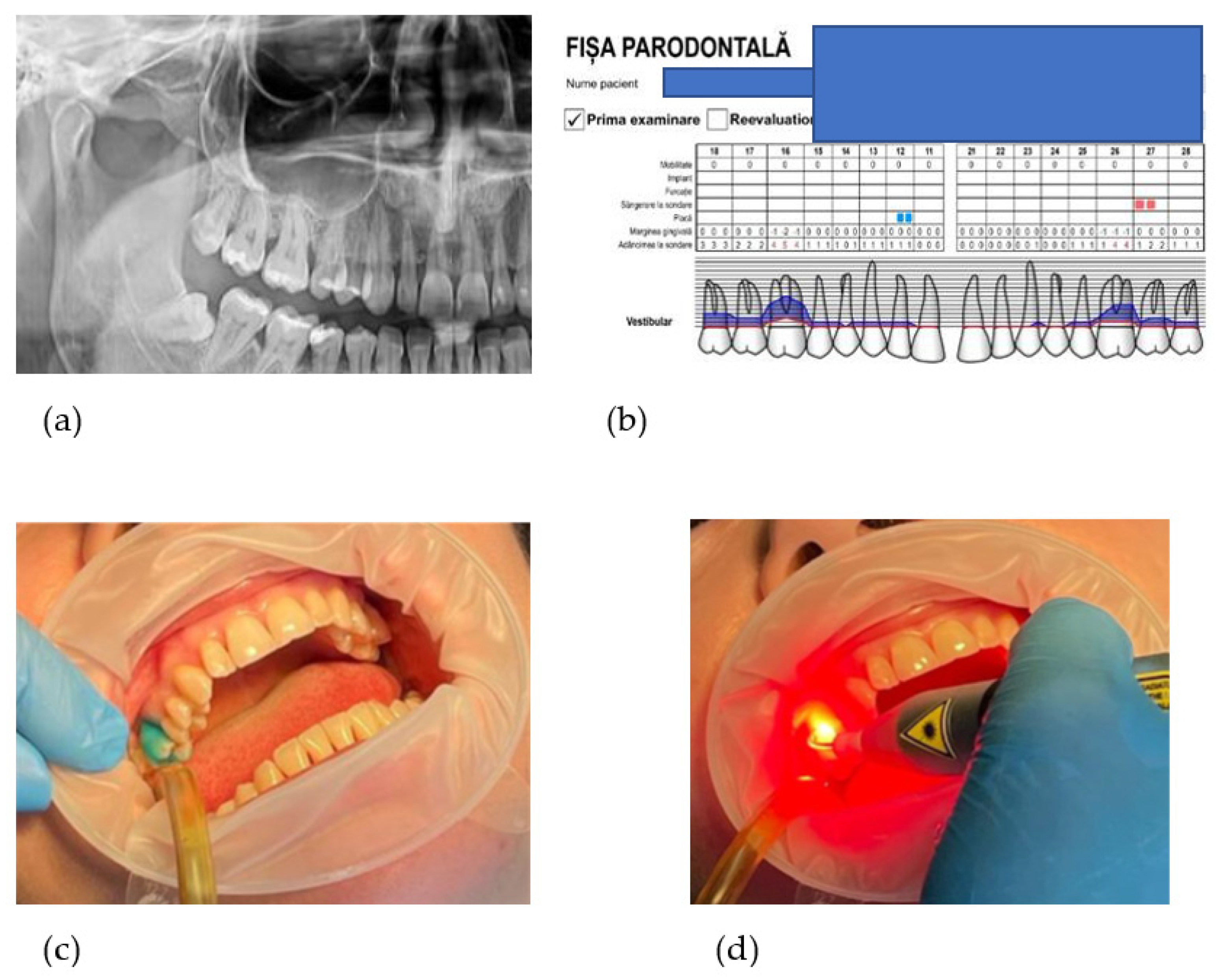
2.2. Oral Examination
2.3. Patient Perception Questionnaire
2.4. Sample Size Calculation
2.5. Treatment Protocol
2.6. Microbiological and Biochemical Evaluation-Crevicular Fluid Samples
- ○
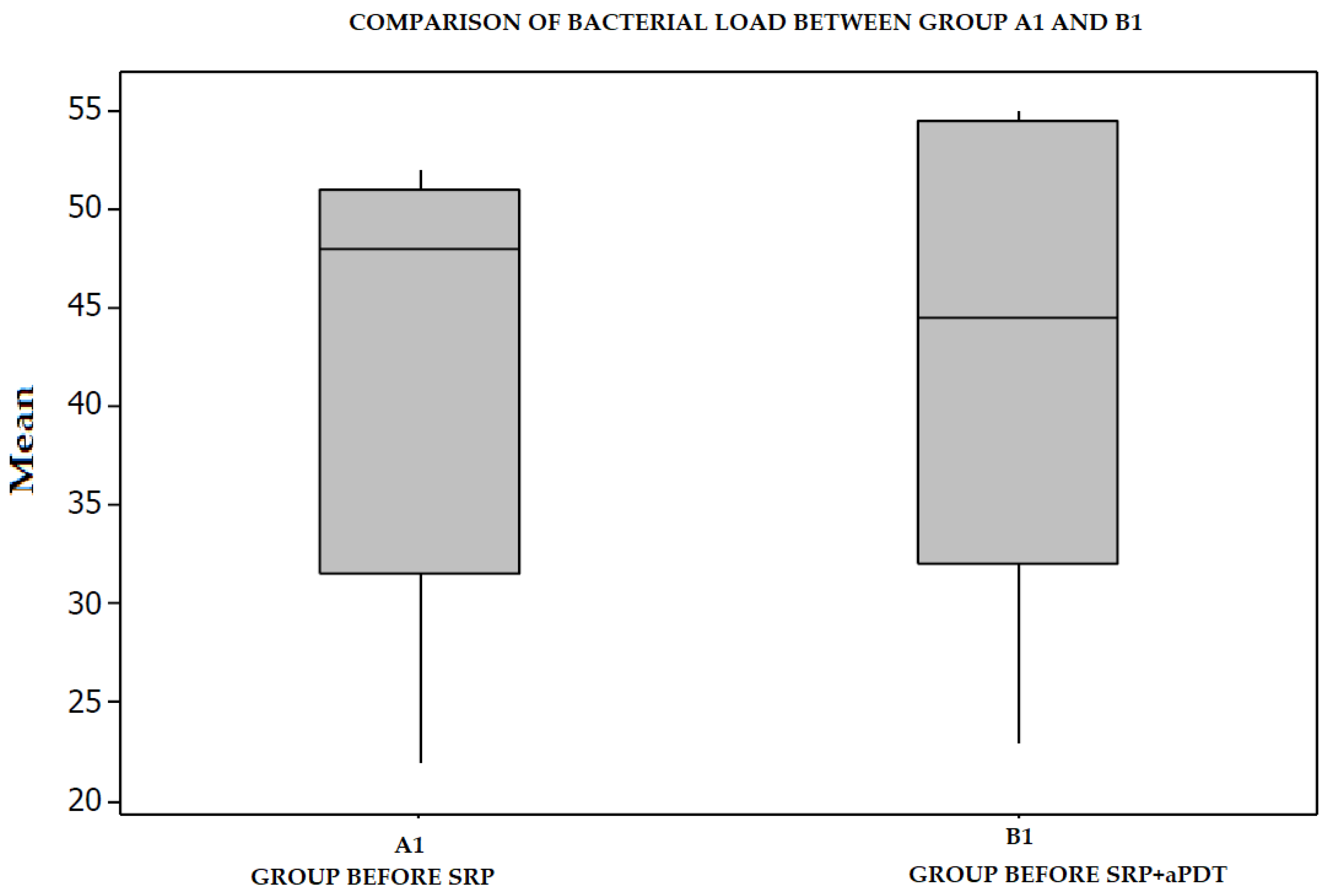
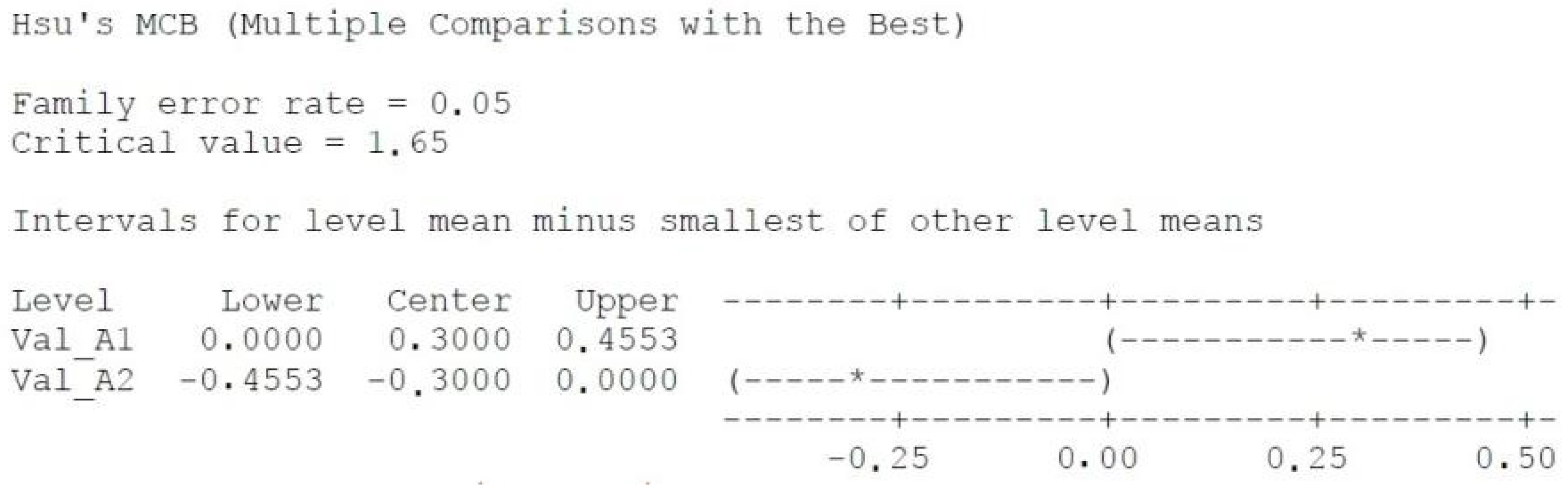
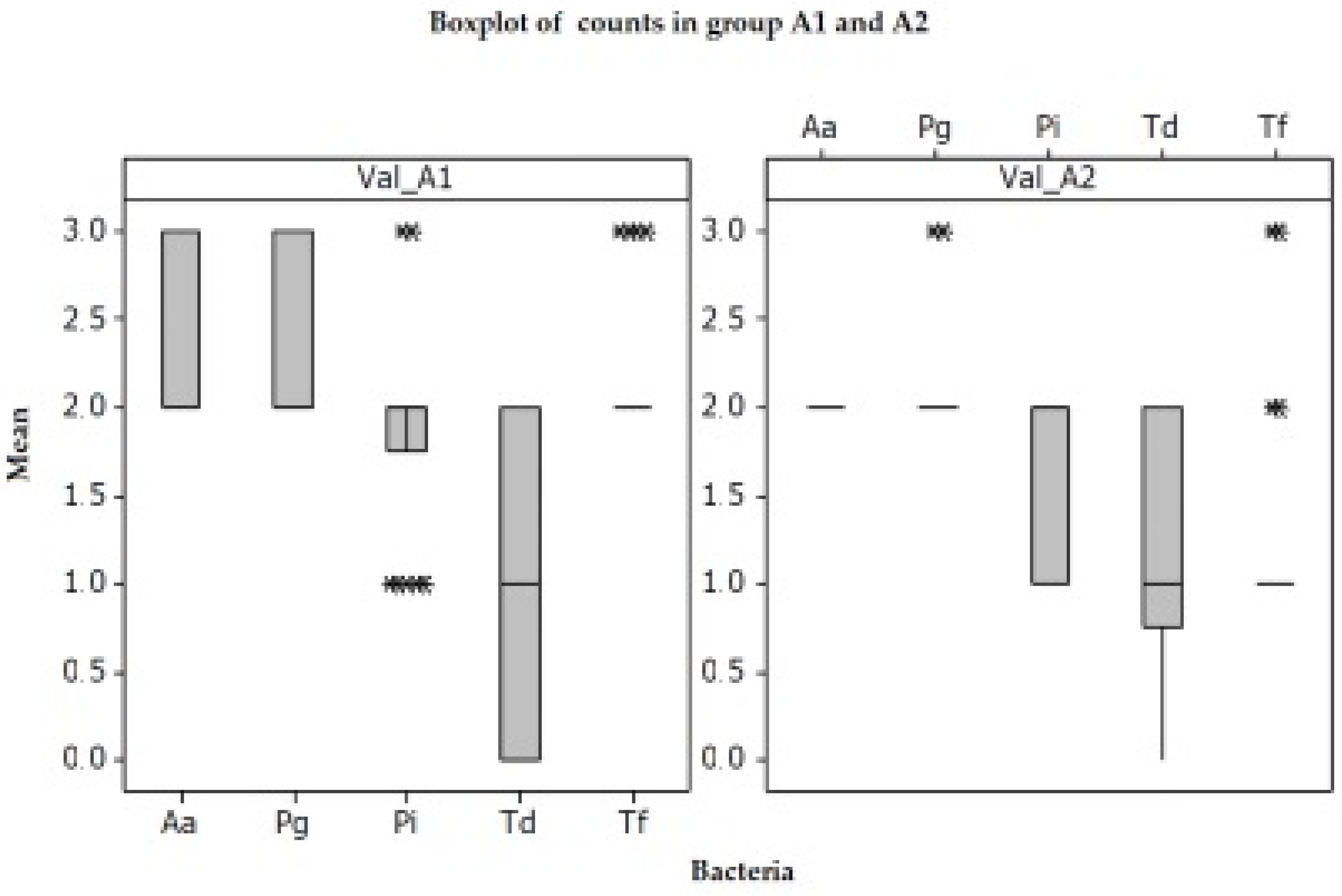
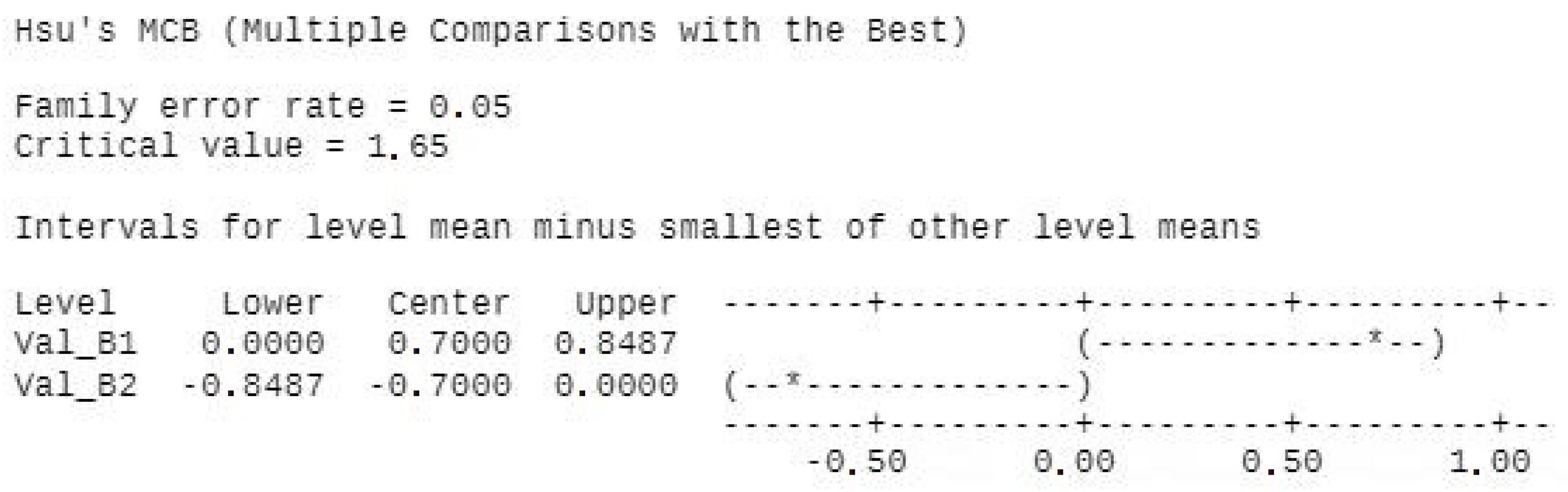
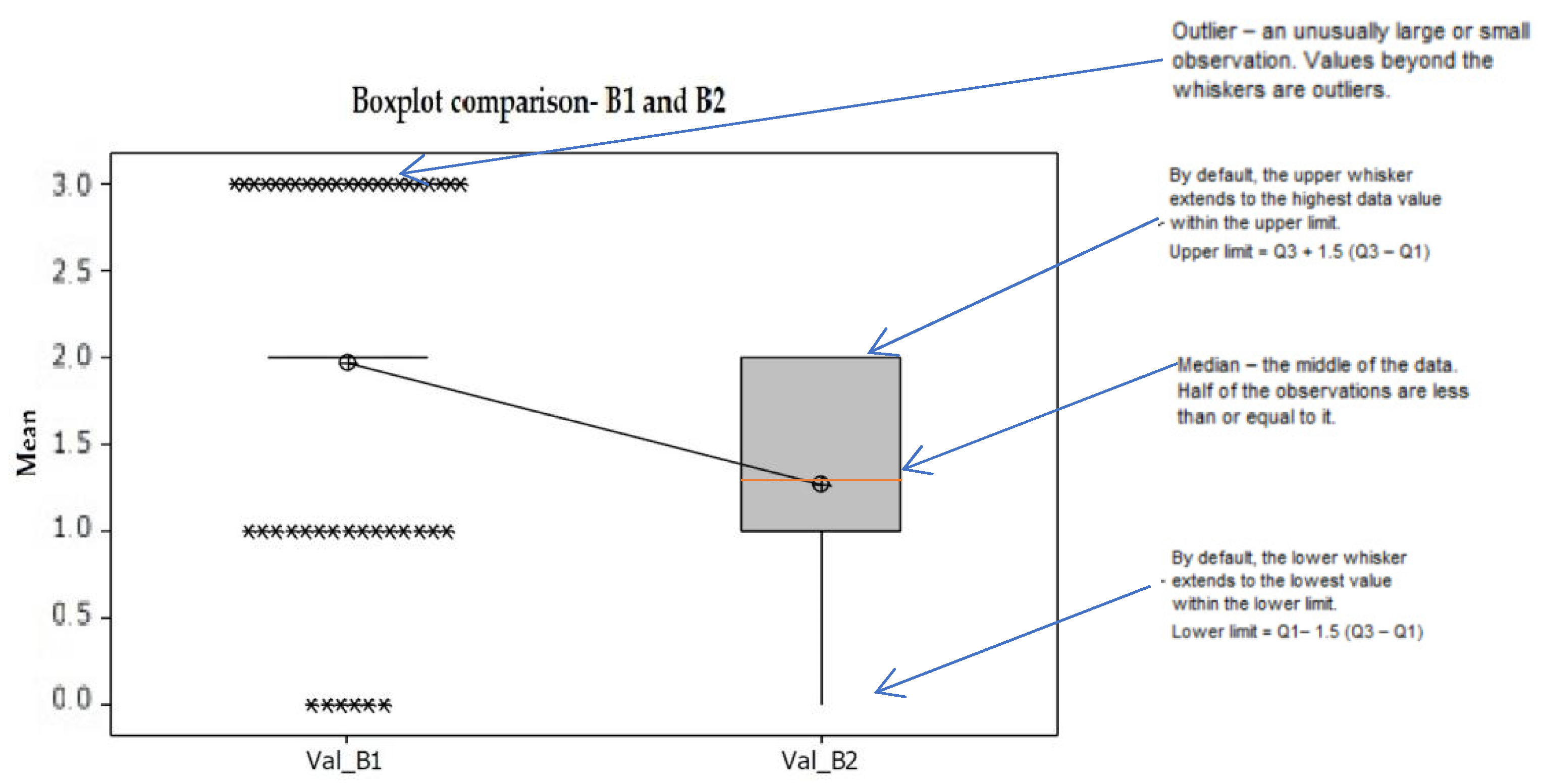
- A1 and B1 represent the negative control groups (all pockets before receiving any kind of treatment), as follows: A1—periodontal pocket before mechanical treatment (SRP), B1—periodontal pocket before mechanical treatment (SRP) and laser;
- ○
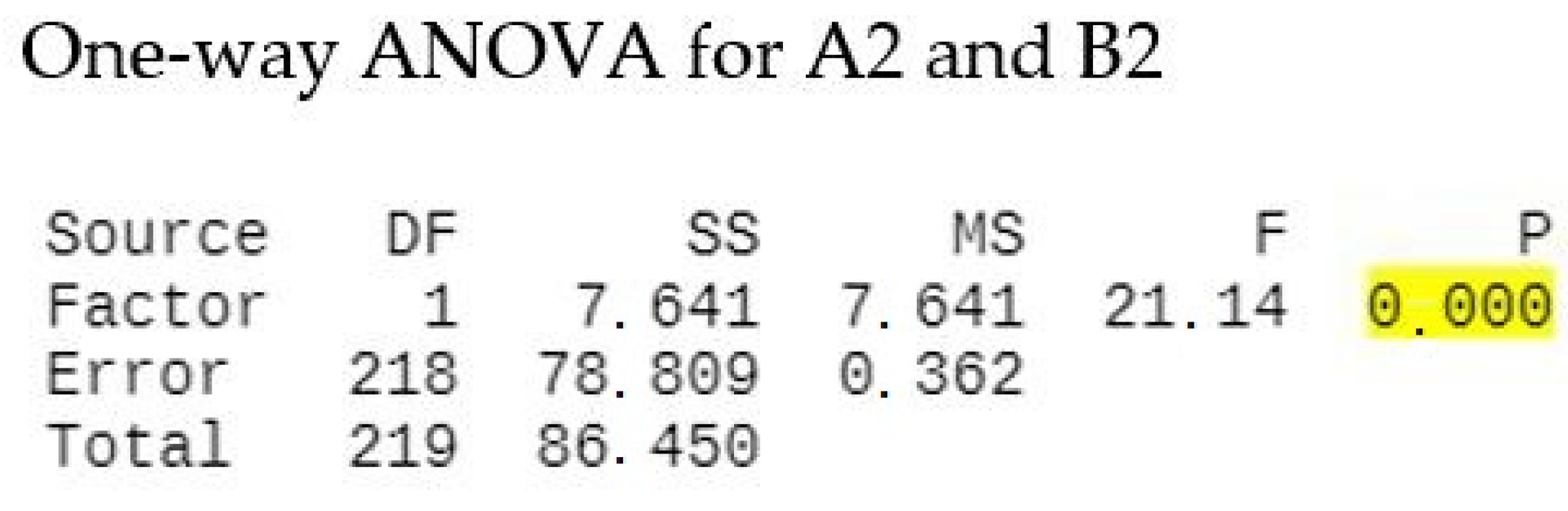
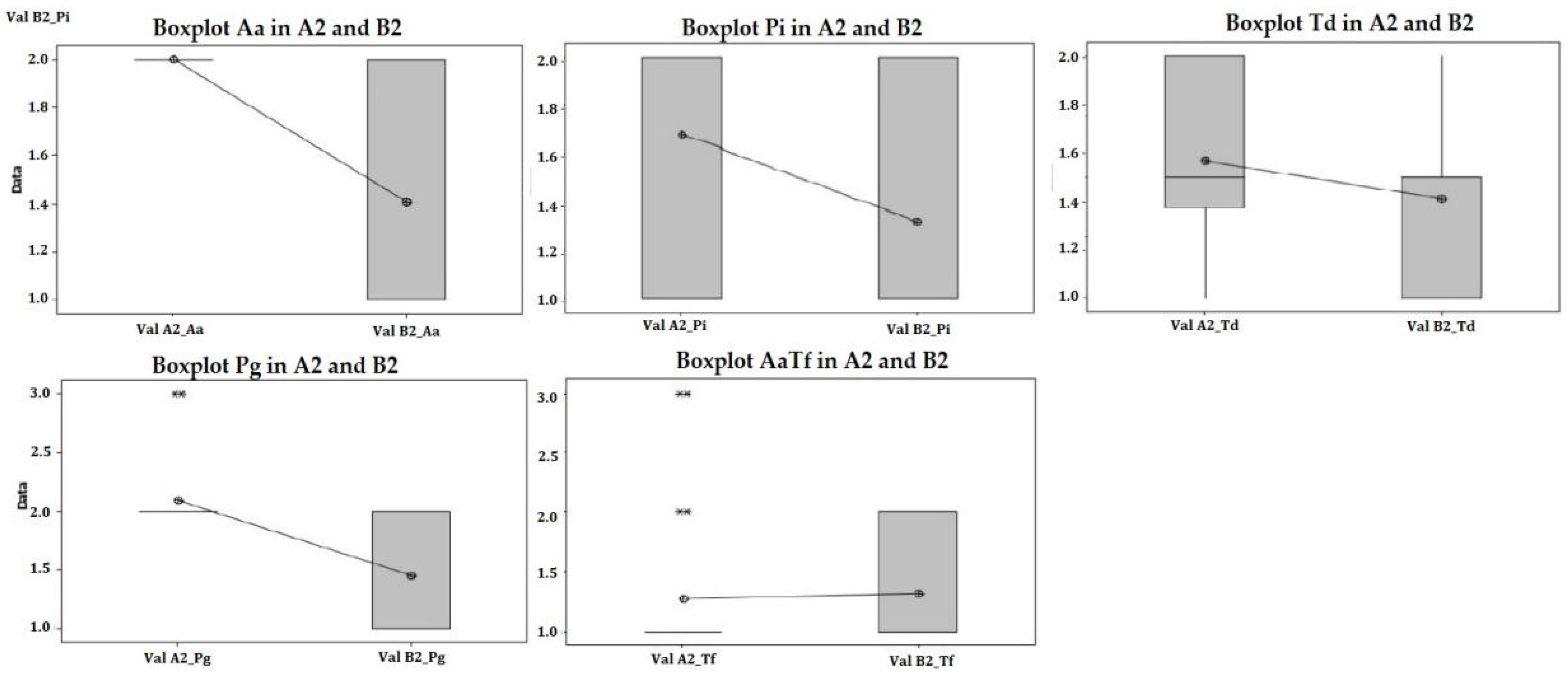
- A2 represents the positive control group: periodontal pocket after mechanical treatment (SRP);
- ○
- B2 represents the study group: periodontal pocket after mechanical treatment (SRP) and laser treatment (aPDT);
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PD | Pocket Depth- depth of the Periodontal Pockets in millimeters. |
| CAL | Clinical Attachment Level- measurements in millimeters. |
| BoP | Bleeding on Probing |
| SRP | Scaling and Root Planing |
| aPDT | antimicrobial Photodynamic Therapy |
| Nd:YAG | Neodymium-Doped Yttrium Aluminum Garnet |
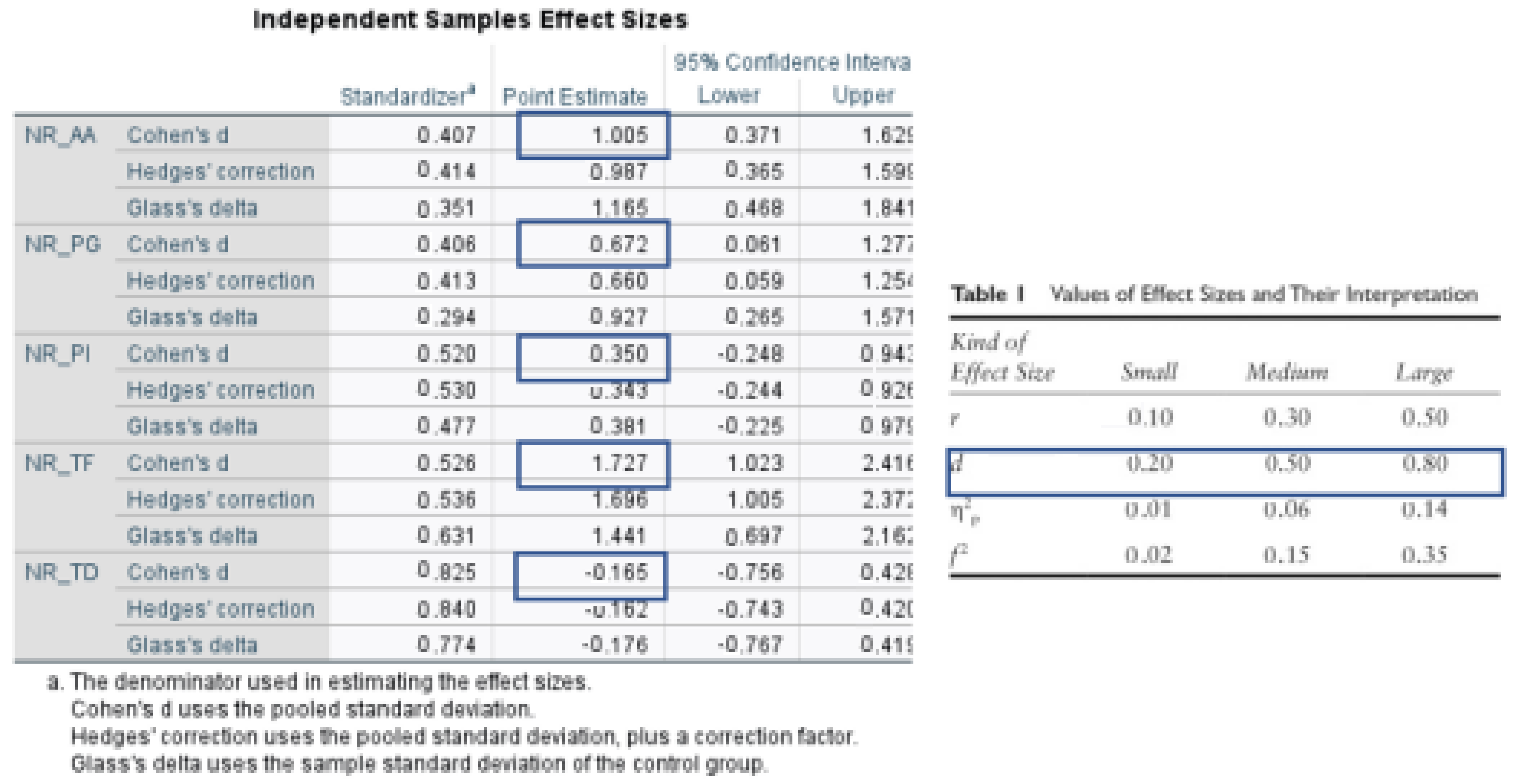
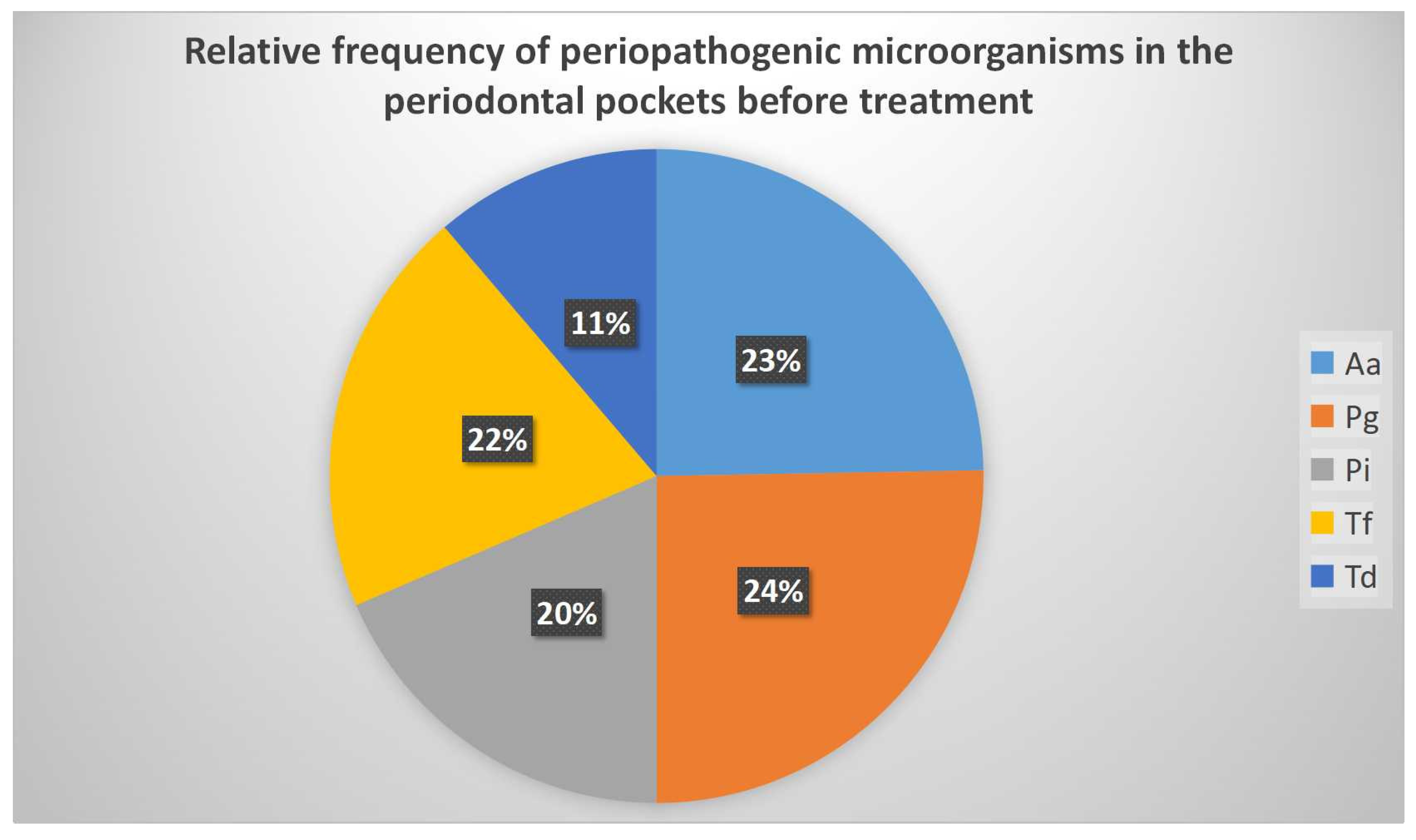
| Aa | Aggregatibacter Actinomycetemcomitans |
| Pg | Porphyromonas Gingivalis |
| Pi | Prevotella Intermedia |
| Td | Treponema Denticola |
| Tf | Tannerella Forsythia |
| DNA | Deoxyribonucleic Acid |
| PCR | Polymerase Chain Reaction |
Appendix A
References
- Hyvärinen, K.; Laitinen, S.; Paju, S.; Hakala, A.; Suominen-Taipale, L.; Skurnik, M.; Pussinen, P.J. Detection and quantification of five major periodontal pathogens by single copy gene-based real-time PCR. Innate Immun. 2009, 15, 195–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinane, D.; Stathopoulou, P.; Papapanou, P. Periodontal diseases. Nat. Rev. Dis. Prim. 2017, 3, 17038. [Google Scholar] [CrossRef] [PubMed]
- Elsadek, M.F.; Farahat, M.F. Effectiveness of photodynamic therapy as an adjunct to periodontal scaling for treating periodontitis in geriatric patients. Eur. Rev. Med. Pharm. Sci. 2022, 26, 1832–1838. [Google Scholar]
- Dewhirst, F.E.; Chen, T.; Izard, J.; Paster, B.J.; Tanner, A.C.; Yu, W.H.; Lakshmanan, A.; Wade, W.G. The human oral microbiome. J. Bacteriol. 2010, 192, 5002–5017. [Google Scholar] [CrossRef] [Green Version]
- Bui, F.Q.; Almeida-da-Silva, C.L.C.; Huynh, B.; Trinh, A.; Liu, J.; Woodward, J.; Asadi, H.; Ojcius, D.M. Association between periodontal pathogens and systemic disease. Biomed. J. 2019, 42, 27–35. [Google Scholar] [CrossRef]
- Chan, E.C.; McLaughlin, R. Taxonomy and virulence of oral spirochetes. Oral Microbiol. Immunol. 2000, 15, 1–9. [Google Scholar] [CrossRef]
- Van Winkelhoff, A.J.; Loos, B.G.; van der Reijden, W.A.; van der Velden, U. Porphyromonas gingivalis, Bacteroides forsythus and other putative periodontal pathogens in subjects with and without periodontal destruction. J. Clin. Periodontol. 2002, 29, 1023–1028. [Google Scholar] [CrossRef]
- Könönen, E.; Jousimies-Somer, H.; Asikainen, S. The most frequently isolated gram-negative anaerobes in saliva and subgingival samples taken from young women. Oral Microbiol Immunol. 1994, 9, 126–128. [Google Scholar] [CrossRef]
- Hajishengallis, G.; Chavakis, T. Local and systemic mechanisms linking periodontal disease and inflammatory comorbidities. Nat. Rev. Immunol. 2021, 21, 426–440. [Google Scholar] [CrossRef]
- Graeber, J.J. Scaling and root planing. J. Am. Dent. Assoc. 2015, 146, 865. [Google Scholar] [CrossRef]
- Wu, J.; Lin, L.; Xiao, J.; Zhao, J.; Wang, N.; Zhao, X.; Tan, B. Efficacy of scaling and root planning with periodontal endoscopy for residual pockets in the treatment of chronic periodontitis: A randomized controlled clinical trial. Clin. Oral Investig. 2021, 26, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Smiley, C.J.; Tracy, S.L.; Abt, E.; Michalowicz, B.S.; John, M.T.; Gunsolley, J.; Cobb, C.M.; Rossmann, J.; Harrel, S.K.; Forrest, J.L.; et al. Systematic review and meta-analysis on the nonsurgical treatment of chronic periodontitis by means of scaling and root planning with or without adjuncts. J. Am. Dent. Assoc. 2015, 146, 508–524.e5. [Google Scholar] [CrossRef] [PubMed]
- Takasaki, A.A.; Aoki, A.; Mizutani, K.; Schwarz, F.; Sculean, A.; Wang, C.Y.; Koshy, G.; Romanos, G.; Ishikawa, I.; Izumi, Y. Application of antimicrobial photodynamic therapy in periodontal and peri-implant diseases. Periodontol. 2000 2009, 51, 109–140. [Google Scholar] [CrossRef] [PubMed]
- Bundidpun, P.; Srisuwantha, R.; Laosrisin, N. Clinical effects of photodynamic therapy as an adjunct to full-mouth ultrasonic scaling and root planing in treatment of chronic periodontitis. Laser 2018, 27, 33–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maisch, T. Anti-microbial photodynamic therapy: Useful in the future? Lasers Med. Sci. 2007, 22, 83–91. [Google Scholar] [CrossRef]
- Takasaki, A.A.; Aoki, A.; Mizutani, K.; Kikuchi, S.; Oda, S.; Ishikawa, I. Er:YAG laser therapy for peri-implant infection: A histological study. Lasers Med. Sci. 2007, 22, 143–157. [Google Scholar] [CrossRef]
- Faragalla, A.I.; Awooda, A.M.; Bolad, A.K.; Ghandour, I.A. Knowledge, Perceptions and Satisfaction towards Diode Laser as Adjunctive to Non-surgical Management of Periodontitis. Ann. Med. Health Sci. Res. 2020, 10, 1070–1073. [Google Scholar]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S173–S182. [Google Scholar] [CrossRef] [Green Version]
- Palmer, R.; Floyd, P. Periodontal Examination and Screening. In Periodontology; Palmer, R., Floyd, P., Eds.; BDJ Clinician’s Guides; Springer: Cham, Switzerland, 2021. [Google Scholar] [CrossRef]
- Weiner, G.P. Laser dentistry practice management. Dent. Clin. N. Am. 2004, 48, 1105–1126. [Google Scholar] [CrossRef]
- Soo, L.; Leichter, J.W.; Windle, J.; Monteith, B.; Williams, S.M.; Seymour, G.J.; Cullinan, M.P. A comparison of Er:YAG laser and mechanical debridement for the non-surgical treatment of chronic periodontitis: A randomized, prospective clinical study. J. Clin. Periodontol. 2012, 39, 537–545. [Google Scholar] [CrossRef]
- Grabarz, D.; VillaNova, J.; Sarti, P.; Ribeiro, A.; de Souza, F.T. Satisfaction Questionnaire after use of Low Level Laser Therapy to Decrease Side Effects during Treatment of Head and Neck Tumors with Radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, S680–S681. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis. Curr. Dir. Psychol. Sci. 1992, 1, 98–101. [Google Scholar] [CrossRef]
- Salvi, G.E.; Stähli, A.; Schmidt, J.C.; Ramseier, C.A.; Sculean, A.; Walter, C. Adjunctive laser or antimicrobial photodynamic therapy to non-surgical mechanical instrumentation in patients with untreated periodontitis: A systematic review and meta-analysis. J. Clin. Periodontol. 2020, 47, 176–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Peloso Ribeiro, É.; Bittencourt, S.; Sallum, E.A.; Nociti, F.H.; Gonçalves, R.B.; Casati, M.Z. Periodontal debridement as a therapeutic approach for severe chronic periodontitis: A clinical, microbiological and immunological study. J. Clin. Periodontol. 2008, 35, 789–798. [Google Scholar] [CrossRef] [PubMed]
- Tomás, I.; Regueira-Iglesias, A.; López, M.; Arias-Bujanda, N.; Novoa, L.; Balsa-Castro, C.; Tomás, M. Quantification by qPCR of Pathobionts in Chronic Periodontitis: Development of Predictive Models of Disease Severity at Site-Specific Level. Front. Microbiol. 2017, 8, 1443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boutaga, K.; Van Winkelhoff, A.J.; Vandenbroucke-Grauls, C.M.J.E.; Savelkoul, P.H.M. The additional value of real-time PCR in the quantitative detection of periodontal pathogens. J. Clin. Periodontol. 2006, 33, 427–433. [Google Scholar] [CrossRef]
- Haffajee, A.D.; Yaskell, T.; Torresyap, G.; Teles, R.; Socransky, S.S. Comparison between polymerase chain reaction-based and checkerboard DNA hybridization techniques for microbial assessment of subgingival plaque samples. J. Clin. Periodontol. 2009, 36, 642–649. [Google Scholar] [CrossRef]
- Santigli, E.; Leitner, E.; Wimmer, G.; Kessler, H.H.; Feierl, G.; Grube, M.; Eberhard, K.; Klug, B. Accuracy of commercial kits and published primer pairs for the detection of periodontopathogens. Clin. Oral Investig. 2016, 20, 2515–2528. [Google Scholar] [CrossRef] [Green Version]
- Mielczarek-Badora, E.; Szulc, M. Photodynamic therapy and its role in periodontitis treatment. Postep. Hig. Med. Dosw. (Online) 2013, 67, 1058–1065. [Google Scholar] [CrossRef]
- Talebi, M.; Taliee, R.; Mojahedi, M.; Meymandi, M.; Torshabi, M. Microbiological efficacy of photodynamic therapy as an adjunct to non-surgical periodontal treatment: A clinical trial. J. Lasers Med. Sci. 2016, 7, 126. [Google Scholar] [CrossRef] [Green Version]
- Alvarenga, L.H.; Gomes, A.C.; Carribeiro, P.; Godoy-Miranda, B.; Noschese, G.; Ribeiro, M.S.; Prates, R.A. Parameters for antimicrobial photodynamic therapy on periodontal pocket—Randomized clinical trial. Photodiagn. Photodyn. 2019, 27, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Cobb, C.M. Lasers in Periodontics: A Review of the Literature. J. Clin. Periodontol. 2006, 77, 545–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Convissar, R.A. Princípios e Práticas Do Laser na Odontologia; Elsevier: Rio de Janeiro, Brasil, 2011. [Google Scholar]
- Obeid, P.R.; D’Hoore, W.; Bercy, P. Comparative clinical responses related to the use of various periodontal instrumentation. J. Clin. Periodontol. 2004, 31, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Christodoulides, N.; Nikolidakis, D.; Chondros, P.; Becker, J.; Schwarz, F.; Rössler, R.; Sculean, A. Photodynamic Therapy as an Adjunct to Non-Surgical Periodontal Treatment: A Randomized, Controlled Clinical Trial. J. Clin. Periodontol. 2008, 79, 1638–1644. [Google Scholar] [CrossRef]
- Polat, E.; Kang, K. Natural photosensitizers in antimicrobial photodynamic therapy. Biomedicines 2021, 9, 584. [Google Scholar] [CrossRef] [PubMed]
- Chawla, K.; Lamba, A.K.; Verma, M. Antimicrobial Photodynamic Therapy and Er,Cr:YSGG Laser-assisted Periodontal Pocket Therapy for Treatment of aggressive Periodontitis: A Randomized Controlled Clinical Trial. World J. Dent. 2022, 13, 473–478. [Google Scholar]
- Meisel, P.; Kocher, T. Photodynamic therapy for periodontal diseases: State of the art. J. Photochem. Photobiol. B 2005, 79, 159–170. [Google Scholar] [CrossRef]
- Dörtbudak, O.; Haas, R.; Bernhart, T.; Mailath-Pokorny, G. Lethal photosensitization for decontamination of implant surfaces in the treatment of peri-implantitis. Clin. Oral Implant. Res. 2001, 12, 104–108. [Google Scholar] [CrossRef] [Green Version]
- De Oliveira, R.R.; Schwartz-Filho, H.O.; Novaes, A.B., Jr.; Taba, M., Jr. Antimicrobial photodynamic therapy in the non-surgical treatment of aggressive periodontitis: A preliminary randomized controlled clinical study. J. Periodontol. 2007, 78, 965–973. [Google Scholar] [CrossRef]
- Rhemrev, G.E.; Timmerman, M.F.; Veldkamp, I.; van Winkelhoff, A.J.; van der Velden, U. Immediate effect of instrumentation on the subgingival microflora in deep inflamed pockets under strict plaque control. J. Clin. Periodontol. 2006, 33, 42–48. [Google Scholar] [CrossRef]
- Rühling, A.; Fanghänel, J.; Houshmand, M.; Kuhr, A.; Meisel, P.; Schwahn, C.; Kocher, T. Photodynamic therapy of persistent pockets in maintenance patients—A clinical study. Clin. Oral Investig. 2010, 14, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, S.L.; Donega, J.M.; Seabra, L.M.; Adabo, M.D.; Lopes, T.; Carmo, T.H.D.D.; Ribeiro, M.C.; Bertolini, P.F.R. Capacity of photodynamic therapy for microbial reduction in periodontal pockets. Lasers Med. Sci. 2010, 25, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, S.; Kuru, B.; Kuru, L.; Noyan, U.; Argun, D.; Kadir, T. Effect of gallium arsenide diode laser on human periodontal disease: A microbiological and clinical study. Lasers Surg. Med. 2002, 30, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Chondros, P.; Nikolidakis, D.; Christodoulides, N.; Rossler, R.; Gutknecht, N.; Sculean, A. Photodynamic therapy as adjunct to non-surgical periodontal treatment in patients on periodontal maintenance: A randomized controlled clinical trial. Lasers Med. Sci. 2009, 24, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Theodoro, L.H.; Silva, S.P.; Pires, J.R.; Soares, G.H.; Pontes, A.E.; Zuza, E.P.; Spolidorio, D.M.; de Toledo, B.E.; Garcia, V. Clinical and microbiological effects of photodynamic therapy associated with nonsurgical periodontal treatment. A 6-month follow-up. Lasers Med. Sci. 2011, 27, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Cappuyns, I.; Cionca, N.; Wick, P.; Giannopoulou, C.; Mombelli, A. Treatment of residual pockets with photodynamic therapy, diode laser, or deep scaling. A randomized, split-mouth controlled clinical trial. Lasers Med. Sci. 2012, 27, 979–986. [Google Scholar] [CrossRef] [Green Version]
- Sgolastra, F.; Petrucci, A.; Gatto, R.; Marzo, G.; Monaco, A. Photodynamic therapy in the treatment of chronic periodontitis: A systematic review and meta-analysis. Lasers Med. Sci. 2011, 28, 669–682. [Google Scholar] [CrossRef] [PubMed]
- Polansky, R.; Haas, M.; Heschl, A.; Wimmer, G. Clinical effectiveness of photodynamic therapy in the treatment of periodontitis. J. Clin. Periodontol. 2009, 36, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Kömerik, N.; Nakanishi, H.; MacRobert, A.J.; Henderson, B.; Speight, P.; Wilson, M. In Vivo Killing of Porphyromonas gingivalis by Toluidine Blue-Mediated Photosensitization in an Animal Model. Antimicrob. Agents Chemother. 2003, 47, 932–940. [Google Scholar] [CrossRef] [Green Version]
- Shen, J.; Liang, Q.; Su, G.; Zhang, Y.; Wang, Z.; Baudouin, C.; Labbé, A. In Vitro Effect of Toluidine Blue Antimicrobial Photodynamic Chemotherapy on Staphylococcus epidermidis and Staphylococcus aureus Isolated from Ocular Surface Infection. Transl. Vis. Sci. Technol. 2019, 8, 45. [Google Scholar] [CrossRef] [Green Version]
- Anju, V.T.; Paramanantham, P.; Sruthil Lal, S.B.; Sharan, A.; Syed, A.; Bahkali, N.A.; Alsaedi, M.H.; Kaviyarasu, K.; Busi, S. Antimicrobial photodynamic activity of toluidine blue-carbon nanotube conjugate against Pseudomonas aeruginosa and Staphylococcus aureus—Understanding the mechanism of action. Photodiagn. Photodyn. Ther. 2019, 27, 305–316. [Google Scholar] [CrossRef]
- He, Y.; Pang, J.; Yang, Z.; Zheng, M.; Yu, Y.; Liu, Z.; Zhao, B.; Hu, G.; Yin, R. Toluidine blue O-induced photoinactivation inhibit the biofilm formation of methicillin-resistant Staphylococcus aureus. Photodiagn. Photodyn. Ther. 2022, 39, 102902. [Google Scholar] [CrossRef] [PubMed]
- Sigusch, B.W.; Engelbrecht, M.; Völpel, A.; Holletschke, A.; Pfister, W.; Schütze, J. Full-Mouth Antimicrobial Photodynamic Therapy in Fusobacterium nucleatum–Infected Periodontitis Patients. J. Periodontol. 2010, 81, 975–981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munteanu, I.R.; Todea, C.; Luca, R.E.; Mocuta, D.E. Photodynamic therapy in periodontology: A systematic review. In Proceedings of the Proc. SPIE 10831, Seventh International Conference on Lasers in Medicine, Timisoara, Romania, 13–15 July 2017; p. 108310B. [Google Scholar] [CrossRef]
- Valderas, J.M.; Alonso, J. Patient reported outcome measures: A model-based classification system for research and clinical practice. Qual. Life Res. 2008, 17, 1125–1135. [Google Scholar] [CrossRef] [PubMed]
- Betsy, J.; Prasanth, C.S.; Baiju, K.V.; Presanthila, J.; Subhash, N. Patients’ perceptions of antimicrobial photodynamic therapy in the management of chronic periodontitis. Photodiagn. Photodyn. 2016, 14, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.K.; Leung, W.K. A community study on the relationship of dental anxiety with oral health status and oral health-related quality of life. Community Dent. Oral Epidemiol. 2008, 36, 347–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Latheef, P.; Sirajuddin, S.; Gundapaneni, V.; Mn, K.; Apine, A. Iatrogenic Damage to the Periodontium Caused by Periodontal Treatment Procedures. Open Dent. J. 2015, 9, 203–207. [Google Scholar] [CrossRef] [Green Version]
- Kolbe, M.F.; Ribeiro, F.V.; Luchesi, V.H.; Casarin, R.C.; Sallum, E.A.; Nociti, F.H., Jr.; Ambrosano, G.M.; Cirano, F.R.; Pimentel, S.P.; Casati, M.Z. Photodynamic therapy during supportive periodontal care: Clinical, microbiologic, immunoinflammatory, and patient-centered performance in a split-mouth randomized clinical trial. J. Periodontol. 2014, 85, e277–e286. [Google Scholar] [CrossRef]










Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Munteanu, I.R.; Luca, R.E.; Mateas, M.; Darawsha, L.D.; Boia, S.; Boia, E.-R.; Todea, C.D. The Efficiency of Photodynamic Therapy in the Bacterial Decontamination of Periodontal Pockets and Its Impact on the Patient. Diagnostics 2022, 12, 3026. https://doi.org/10.3390/diagnostics12123026
Munteanu IR, Luca RE, Mateas M, Darawsha LD, Boia S, Boia E-R, Todea CD. The Efficiency of Photodynamic Therapy in the Bacterial Decontamination of Periodontal Pockets and Its Impact on the Patient. Diagnostics. 2022; 12(12):3026. https://doi.org/10.3390/diagnostics12123026
Chicago/Turabian StyleMunteanu, Ioana R., Ruxandra E. Luca, Marius Mateas, Laura Diana Darawsha, Simina Boia, Eugen-Radu Boia, and Carmen D. Todea. 2022. "The Efficiency of Photodynamic Therapy in the Bacterial Decontamination of Periodontal Pockets and Its Impact on the Patient" Diagnostics 12, no. 12: 3026. https://doi.org/10.3390/diagnostics12123026