
Intraoperative Assessment of High-Risk Thyroid Nodules Based on Electrical Impedance Measurements: A Feasibility Study
 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
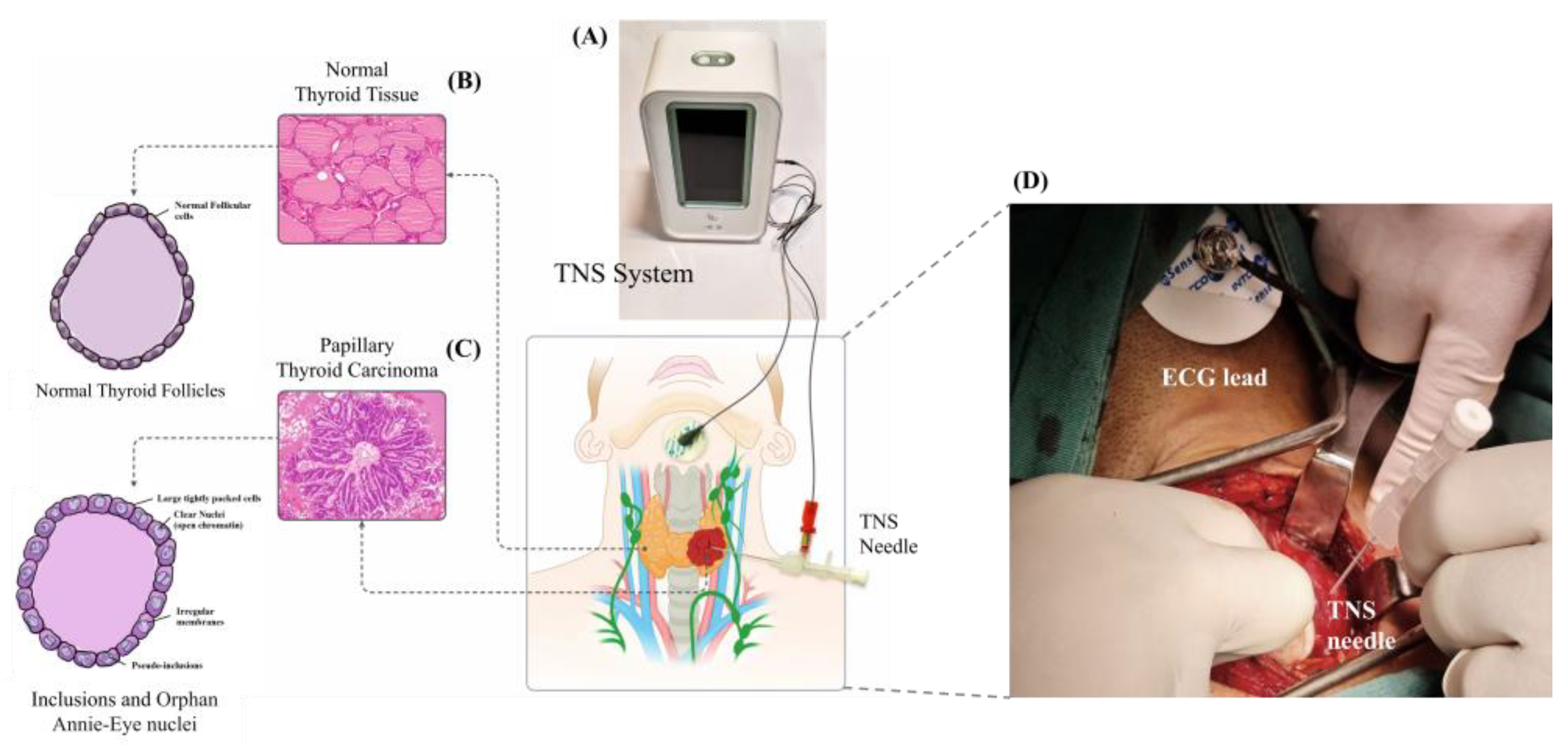
2.1. TN-IMS Measurement System and Mechanism
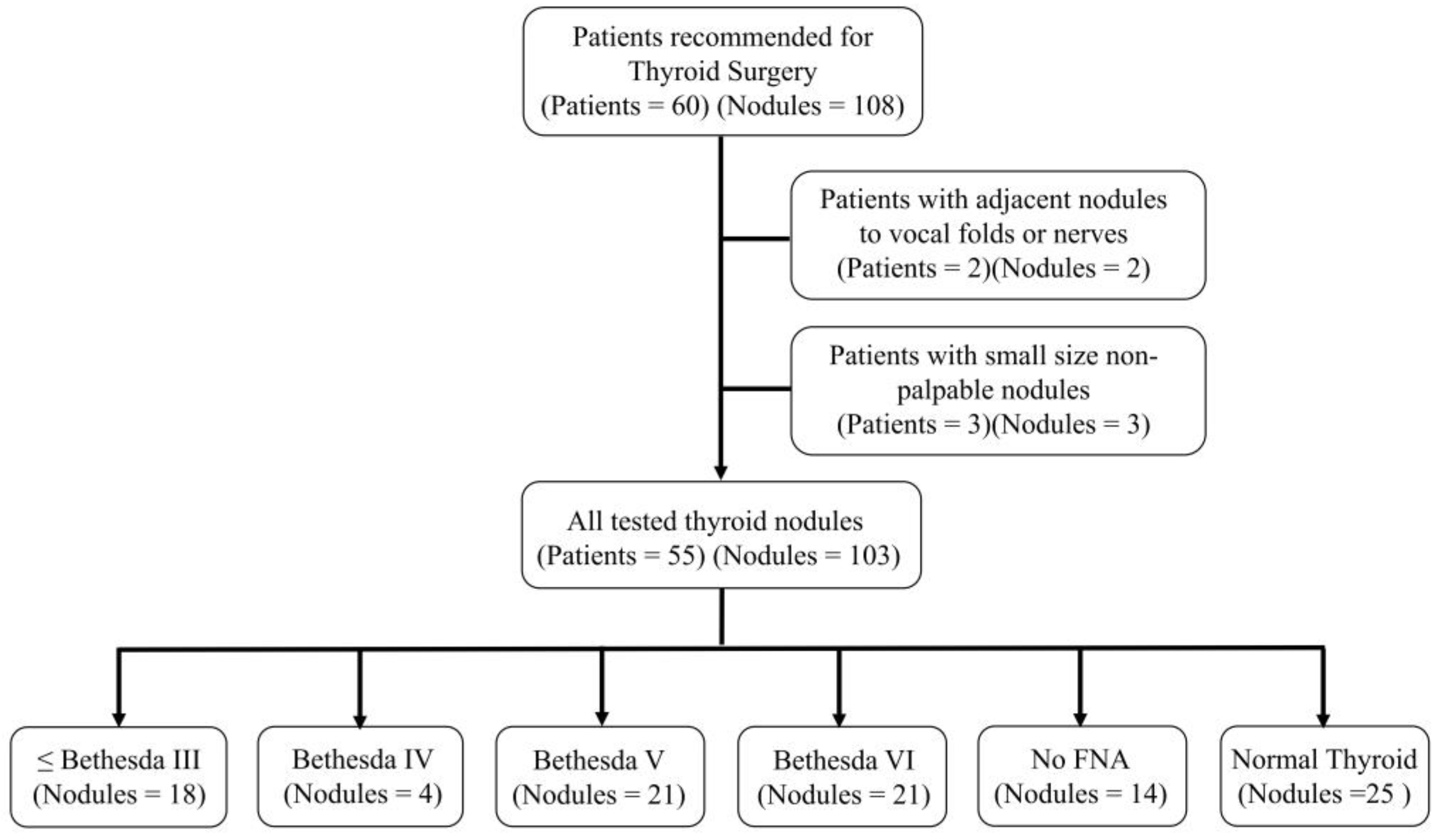
2.2. TN-IMS Measurement Protocol
2.3. Statistical Analysis
2.4. Ethics
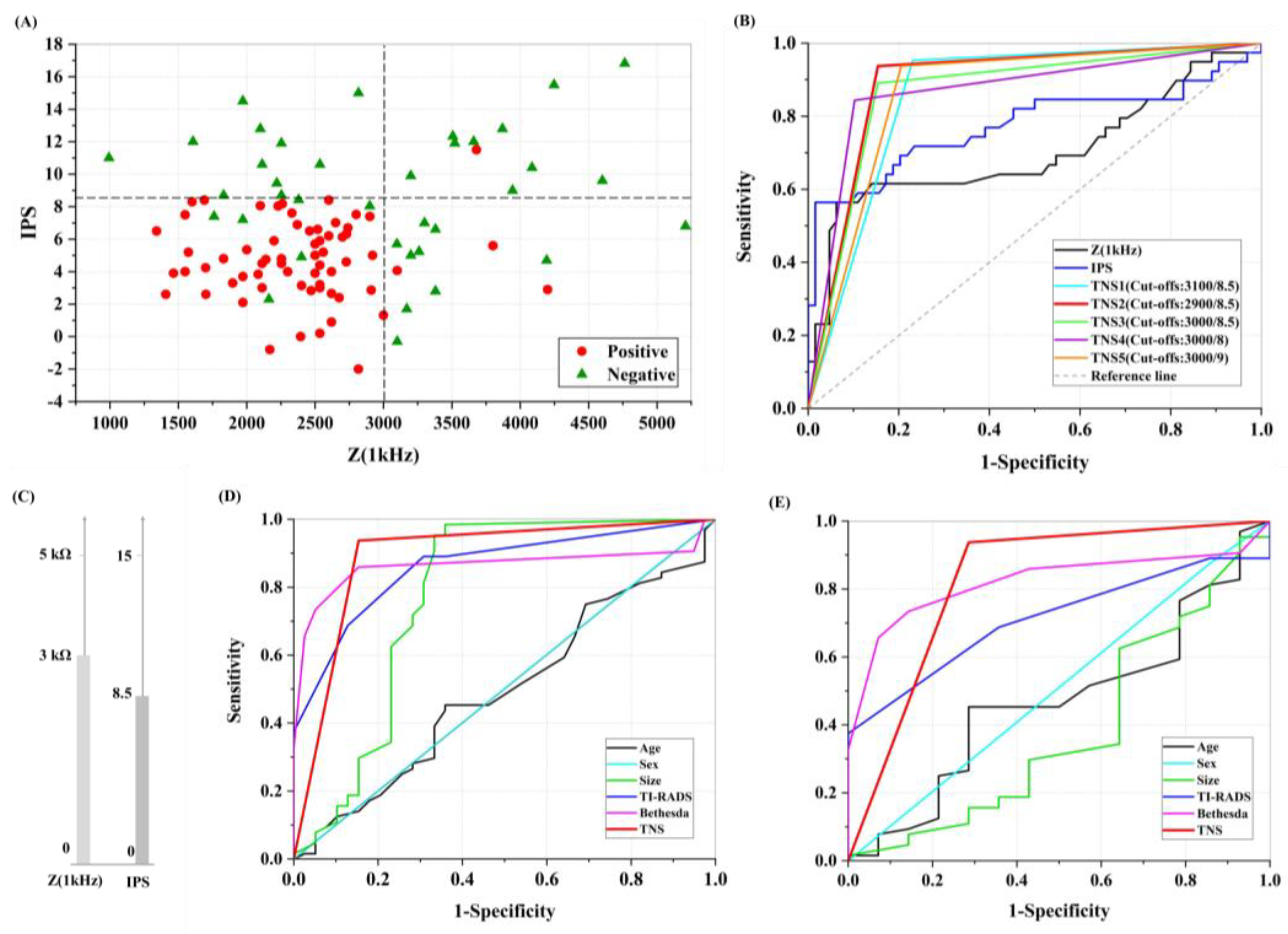
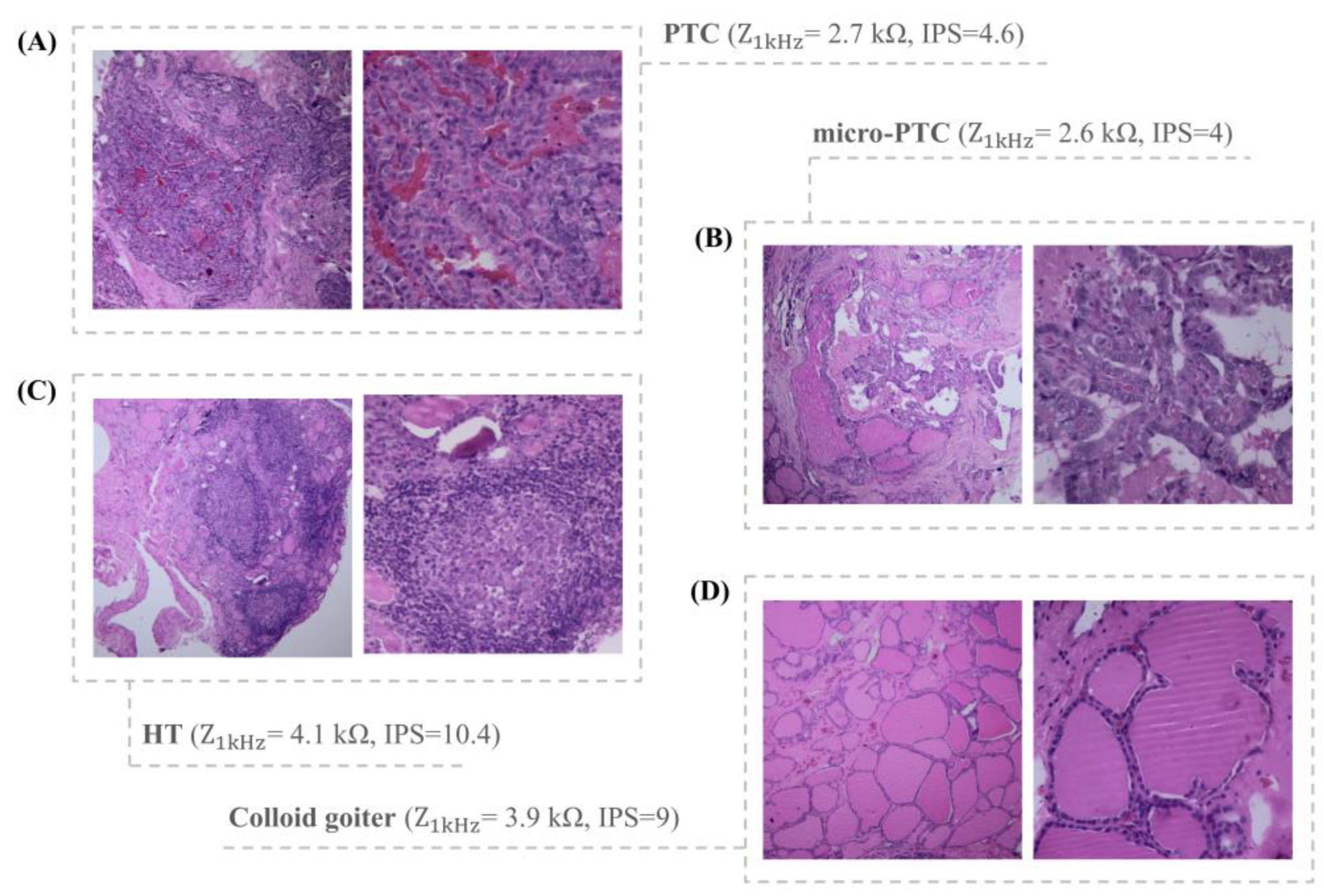
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Roshandel, G.; Ferlay, J.; Ghanbari-Motlagh, A.; Partovipour, E.; Salavati, F.; Aryan, K.; Mohammadi, G.; Khoshaabi, M.; Sadjadi, A.; Davanlou, M.; et al. Cancer in Iran 2008 to 2025: Recent Incidence Trends and Short-Term Predictions of the Future Burden. Int. J. Cancer 2021, 149, 594–605. [Google Scholar] [CrossRef] [PubMed]
- Vigneri, R.; Malandrino, P.; Vigneri, P. The Changing Epidemiology of Thyroid Cancer: Why Is Incidence Increasing? Curr. Opin. Oncol. 2015, 27, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ahn, H.S.; Kim, H.J.; Kim, K.H.; Lee, Y.S.; Han, S.J.; Kim, Y.; Ko, M.J.; Brito, J.P. Thyroid Cancer Screening in South Korea Increases Detection of Papillary Cancers with No Impact on Other Subtypes or Thyroid Cancer Mortality. Thyroid 2016, 26, 1535–1540. [Google Scholar] [CrossRef]
- Nissan, A.; Peoples, G.E.; Abu-Wasel, B.; Adair, C.F.; Prus, D.; Howard, R.S.; Lenington, S.G.; Fields, S.I.; Freund, H.R.; Peretz, T.; et al. Prospective Trial Evaluating Electrical Impedance Scanning of Thyroid Nodules before Thyroidectomy: Final Results. Ann. Surg. 2008, 247, 843–853. [Google Scholar] [CrossRef]
- Christou, N.; Mathonnet, M. Complications after Total Thyroidectomy. J. Visc. Surg. 2013, 150, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Reeve, T.; Thompson, N.W. Complications of Thyroid Surgery: How to Avoid Them, How to Manage Them, and Observations on Their Possible Effect on the Whole Patient. World J. Surg. 2000, 24, 971–975. [Google Scholar] [CrossRef]
- Kandil, E.; Krishnan, B.; Noureldine, S.I.; Yao, L.; Tufano, R.P. Hemithyroidectomy: A Meta-Analysis of Postoperative Need for Hormone Replacement and Complications. Orl 2013, 75, 6–17. [Google Scholar] [CrossRef]
- D’Orazi, V.; Panunzi, A.; Di Lorenzo, E.; Ortensi, A.; Cialini, M.; Anichini, S.; Ortensi, A. Use of Loupes Magnification and Microsurgical Technique in Thyroid Surgery: Ten Years Experience in a Single Center. Il G. Chir. 2016, 37, 101–107. [Google Scholar] [CrossRef]
- Chung, S.R.; Baek, J.H.; Choi, Y.J.; Sung, T.Y.; Song, D.E.; Kim, T.Y.; Lee, J.H. The Role of Core Needle Biopsy for the Evaluation of Thyroid Nodules with Suspicious Ultrasound Features. Korean J. Radiol. 2019, 20, 158–165. [Google Scholar] [CrossRef]
- Grimmichová, T.; Pačesová, P.; Srbová, L.; Vrbíkova, J.; Havrdová, T.; Hill, M. The Gold Standard of Thyroid Nodule Examination? Prospective Validation of the ACR TI-RADS in a Secondary Referral Center. Physiol. Res. 2020, 69, 329–337. [Google Scholar] [CrossRef]
- Zheng, B.; Tublin, M.E.; Lederman, D.; Klym, A.H.; Brown, E.D.; Gur, D. Assessing Risk of Thyroid Cancer Using Resonance-Frequency Based Electrical Impedance Measurements. In Medical Imaging 2011: Image Perception, Observer Performance, and Technology Assessment; SPIE: Bellingham, WA, USA, 2011; Volume 7966, pp. 369–376. [Google Scholar] [CrossRef]
- Jung, C.K.; Baek, J.H. Recent Advances in Core Needle Biopsy for Thyroid Nodules. Endocrinol. Metab. 2017, 32, 407–412. [Google Scholar] [CrossRef]
- Houdek, D.; Cooke-Hubley, S.; Puttagunta, L.; Morrish, D. Factors Affecting Thyroid Nodule Fine Needle Aspiration Non-diagnostic Rates: A Retrospective Association Study of 1975 Thyroid Biopsies. Thyroid Res. 2021, 14, 4–9. [Google Scholar] [CrossRef]
- Ziemiańska, K.; Kopczyński, J.; Kowalska, A. Repeated Nondiagnostic Result of Thyroid Fine-Needle Aspiration Biopsy. Wspolczesna Onkol. 2016, 20, 491–495. [Google Scholar] [CrossRef] [Green Version]
- Choi, Y.J.; Baek, J.H.; Ha, E.J.; Lim, H.K.; Lee, J.H.; Kim, J.K.; Song, D.E.; Shong, Y.K.; Hong, S.J. Differences in Risk of Malignancy and Management Recommendations in Subcategories of Thyroid Nodules with Atypia of Undetermined Significance or Follicular Lesion of Undetermined Significance: The Role of Ultrasound-Guided Core-Needle Biopsy. Thyroid 2014, 24, 494–501. [Google Scholar] [CrossRef]
- Uçan, B.; Şahin, M.; Özbek, M.; Kizilgül, M.; Sayki Arslan, M.; Çalişkan, M.; Saylam, G.; Çakal, E. Lobectomy May Not Be Suitable for Patients with Follicular Neoplasm Cytology. Turkish J. Med. Sci. 2020, 50, 8–11. [Google Scholar] [CrossRef]
- Polistena, A.; Sanguinetti, A.; Lucchini, R.; Avenia, S.; Galasse, S.; Farabi, R.; Monacelli, M.; Avenia, N. Follicular Proliferation TIR3B: The Role of Total Thyroidectomy vs Lobectomy. BMC Surg. 2019, 18, 22. [Google Scholar] [CrossRef] [Green Version]
- Almquist, M.; Muth, A. Surgical Management of Cytologically Indeterminate Thyroid Nodules. Gland Surg. 2019, 8, S105–S111. [Google Scholar] [CrossRef]
- Turkdogan, S.; Pusztaszeri, M.; Forest, V.-I.; Hier, M.P.; Payne, R.J. Are Bethesda III Thyroid Nodules More Aggressive than Bethesda IV Thyroid Nodules When Found to Be Malignant? Cancers 2020, 12, 2563. [Google Scholar] [CrossRef]
- Hahn, S.Y.; Shin, J.H.; Oh, Y.L.; Park, K.W.; Lim, Y. Comparison Between Fine Needle Aspiration and Core Needle Biopsy for the Diagnosis of Thyroid Nodules: Effective Indications According to US Findings. Sci. Rep. 2020, 10, 4969. [Google Scholar] [CrossRef] [Green Version]
- Ahn, S.H. Usage and Diagnostic Yield of Fine-Needle Aspiration Cytology and Core Needle Biopsy in Thyroid Nodules: A Systematic Review and Meta-Analysis of Literature Published by Korean Authors. Clin. Exp. Otorhinolaryngol. 2021, 14, 116–130. [Google Scholar] [CrossRef]
- Appukutty, S.J.; Paterson, A.; Patel, N.S.; Duckworth, A.; Chan, J.; O’Donovan, M.; Marker, A.J. Thyroid Diagnostic Modalities (Fine Needle Aspiration and Core Needle Biopsy) with Histology Correlation: A Tertiary Centre Experience. J. Clin. Pathol. 2022, 75, 620–626. [Google Scholar] [CrossRef]
- Bera, T.K. Bioelectrical Impedance Methods for Noninvasive Health Monitoring: A Review. J. Med. Eng. 2014, 2014, 1–28. [Google Scholar] [CrossRef] [Green Version]
- Ng, E.Y.; Subbhuraam, V.S. The Use of Tissue Electrical Characteristics for Breast Cancer Detection: A Perspective Review. Technol. Cancer Res. Treat. 2008, 7, 295–308. [Google Scholar] [CrossRef] [Green Version]
- Magar, H.S.; Hassan, R.Y.A.; Mulchandani, A. Electrochemical Impedance Spectroscopy (EIS): Principles, Construction, and Biosensing Applications. Sensors 2021, 21, 6578. [Google Scholar]
- Xu, B. Thyroid & Parathyroid, Papillary Thyroid Carcinoma Overview. Available online: https://www.pathologyoutlines.com/topic/thyroidpapillary.html (accessed on 27 December 2021).
- Mahdavi, R.; Mehrvarz, S.; Hoseinpour, P.; Yousefpour, N.; Abbasvandi, F.; Tayebi, M.; Ataee, H.; Parniani, M.; Abdolhoseini, S.; Hajighasemi, F.; et al. Intraradiological Pathology-Calibrated Electrical Impedance Spectroscopy in the Evaluation of Excision-Required Breast Lesions. Med. Phys. 2022, 49, 2746–2760. [Google Scholar] [CrossRef]
- Mahdavi, R.; Hosseinpour, P.; Abbasvandi, F.; Mehrvarz, S.; Yousefpour, N.; Ataee, H.; Parniani, M.; Mamdouh, A.; Ghafari, H.; Abdolahad, M. Bioelectrical Pathology of the Breast; Real-Time Diagnosis of Malignancy by Clinically Calibrated Impedance Spectroscopy of Freshly Dissected Tissue. Biosens. Bioelectron. 2020, 165, 112421. [Google Scholar] [CrossRef]
- Goemann, I.M.; Paixão, F.; Migliavacca, A.; Guimarães, J.R.; Scheffel, R.S.; Maia, A.L. Intraoperative Frozen Section Performance for Thyroid Cancer Diagnosis. Arch. Endocrinol. Metab. 2022, 66, 50–57. [Google Scholar] [CrossRef]
- Chen, H.Y.; Benjamin, L.B.; Chen, M.F. Hurthle Cell Tumor. Int. Surg. 1996, 81, 168–170. [Google Scholar]
- Pisanu, A.; Sias, L.; Uccheddu, A. Factors Predicting Malignancy of Hurthle Cell Tumors of the Thyroid: Influence on Surgical Treatment. World J. Surg. 2004, 28, 761–765. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Category | Abundance |
|---|---|---|
| Age (years) | >40 | 31 (56%) |
| ≤40 | 24 (44%) | |
| Sex | Female | 47 (85%) |
| Male | 8 (15%) | |
| Nodule Size | <1 cm | 28 (36%) |
| Between 1 and 3 cm | 34 (44%) | |
| >3 cm | 16 (20%) | |
| TI-RADS | 2 | 2 (2%) |
| 3 | 20 (19.3%) | |
| 4 | 25 (24.3%) | |
| 5 | 24 (23%) | |
| Not detected | 7 (7%) | |
| No nodule | 25 (24.3%) | |
| Bethesda | I, II, III | 18 (17.5%) |
| IV | 4 (3.8%) | |
| V | 21 (20.4%) | |
| VI | 21 (20.4%) | |
| No FNA reports | 14 (13.6%) | |
| Normal thyroid tissue | 25 (24.3%) | |
| Pathological Type | PTC | 42 (40.7%) |
| Micro-PTC | 18 (17.5%) | |
| HCC | 3 (3%) | |
| HCN | 1 (0.9%) | |
| HT | 3 (3%) | |
| MNG | 11 (10.7%) | |
| Normal tissue | 25 (24.3%) |
| Permanent Pathological Evaluation | TN-IMS Score | ||||||
|---|---|---|---|---|---|---|---|
| TP | TN | FP | FN | ||||
| Nodules with intraoperative frozen pathology | Positive | PTC | 2 | 3 (100%) | 0 | 0 | 0 |
| micro-PTC | 3 | 3 (100%) | 0 | 0 | 0 | ||
| HCC | 2 | 2 (100%) | 0 | 0 | 0 | ||
| Negative | HT | 1 | 0 | 1 (100%) | 0 | 0 | |
| Bethesda II (Benign Follicular nodules) | Positive | PTC | 2 | 2 (100%) | 0 | 0 | 0 |
| Negative | MNG | 2 | 0 | 1 (50%) | 1 (50%) | 0 | |
| HT | 1 | 0 | 1 (100%) | 0 | 0 | ||
| Bethesda III (AUS/FLUS) | Positive | HCN | 1 | 1 (100%) | 0 | 0 | 0 |
| HCC | 2 | 2 (100%) | 0 | 0 | 0 | ||
| PTC | 2 | 2 (100%) | 0 | 0 | 0 | ||
| micro-PTC | 1 | 1 (100%) | 0 | 0 | 0 | ||
| Negative | MNG | 1 | 0 | 1 (100%) | 0 | 0 | |
| HT | 2 | 0 | 2 (100%) | 0 | 0 | ||
| Bethesda IV (Suspicious for follicular neoplasm) | Positive | PTC | 2 | 2 (100%) | 0 | 0 | 0 |
| micro-PTC | 2 | 2 (100%) | 0 | 0 | 0 | ||
| Nodules with micro-PTC post-surgical evaluations | Detected as a nodule in radiological evaluations | 12 | 12 (100%) | 0 | 0 | 0 | |
| Detected as a nodule in surgical evaluations | 5 | 5 (100%) | 0 | 0 | 0 | ||
| Only detected in permanent pathology | 1 | 1 (100%) | 0 | 0 | 0 | ||
| Nodules with TI-RADS3 score in presurgical evaluations | Positive | PTC | 9 | 9 (100%) | 0 | 0 | 0 |
| micro-PTC | 2 | 2 (100%) | 0 | 0 | 0 | ||
| HCC | 2 | 2 (100%) | 0 | 0 | 0 | ||
| Negative | - | 7 | 0 | 5 (71%) | 2 (29%) | 0 | |
| Follicular variant of PTC in post-surgical evaluations | 11 | 11 (100%) | 0 | 0 | 0 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beheshti Firoozabadi, J.; Mahdavi, R.; Shamsi, K.; Ataee, H.; Shafiee, A.; Ebrahiminik, H.; Chegini, H.; Hoseinpour, P.; Moradi, A.; Yousefpour, N.; et al. Intraoperative Assessment of High-Risk Thyroid Nodules Based on Electrical Impedance Measurements: A Feasibility Study. Diagnostics 2022, 12, 2950. https://doi.org/10.3390/diagnostics12122950
Beheshti Firoozabadi J, Mahdavi R, Shamsi K, Ataee H, Shafiee A, Ebrahiminik H, Chegini H, Hoseinpour P, Moradi A, Yousefpour N, et al. Intraoperative Assessment of High-Risk Thyroid Nodules Based on Electrical Impedance Measurements: A Feasibility Study. Diagnostics. 2022; 12(12):2950. https://doi.org/10.3390/diagnostics12122950
Chicago/Turabian StyleBeheshti Firoozabadi, Jalil, Reihane Mahdavi, Khosro Shamsi, Hossein Ataee, Abdollah Shafiee, Hojat Ebrahiminik, Hossein Chegini, Parisa Hoseinpour, Afshin Moradi, Narges Yousefpour, and et al. 2022. "Intraoperative Assessment of High-Risk Thyroid Nodules Based on Electrical Impedance Measurements: A Feasibility Study" Diagnostics 12, no. 12: 2950. https://doi.org/10.3390/diagnostics12122950