
Ultrasound Versus Computed Tomography for Diaphragmatic Thickness and Skeletal Muscle Index during Mechanical Ventilation

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
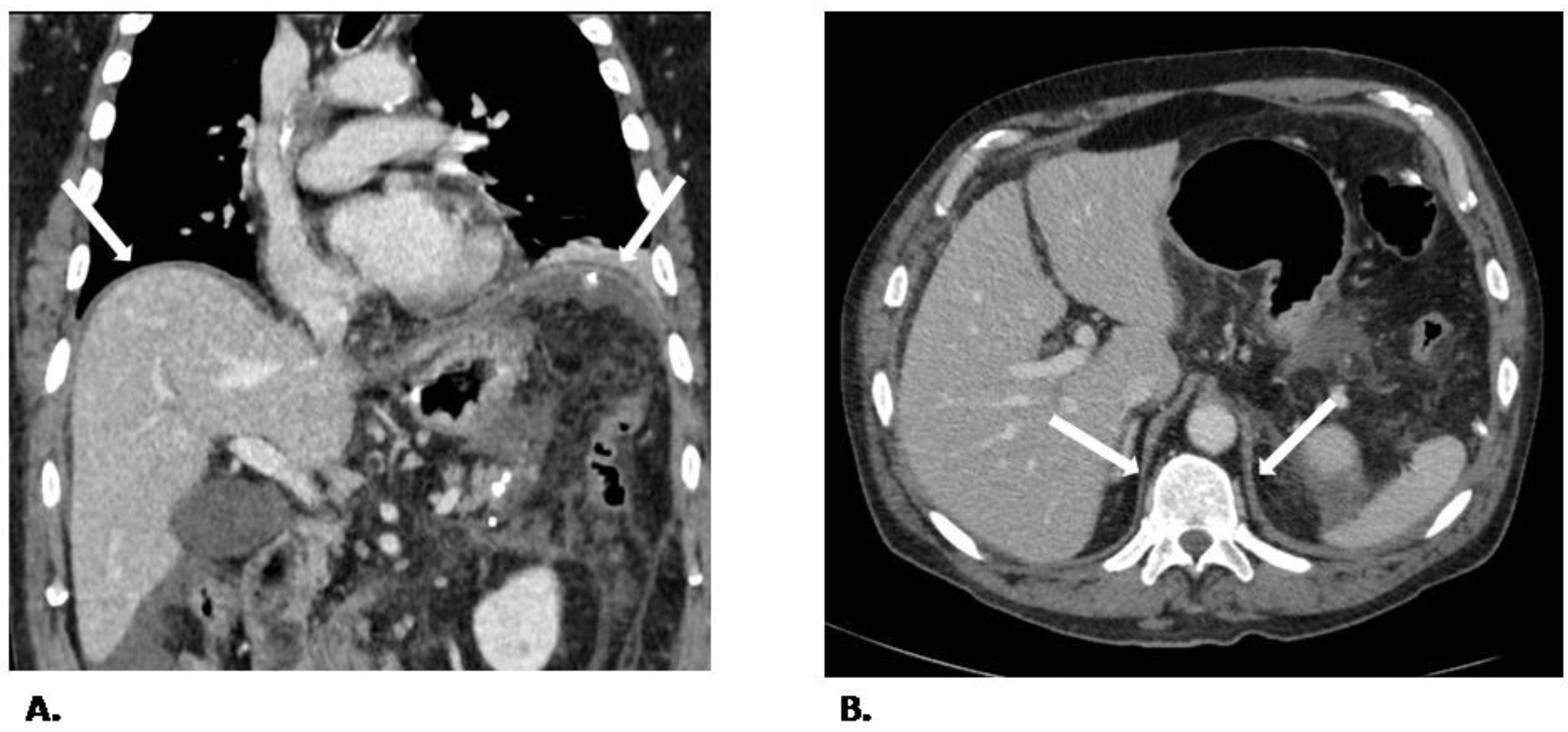
2.1. CT Protocol and Image Analysis
2.2. US Protocol and Image Analysis
3. Statistical Analysis
4. Sample Size
5. Results
5.1. Study Population
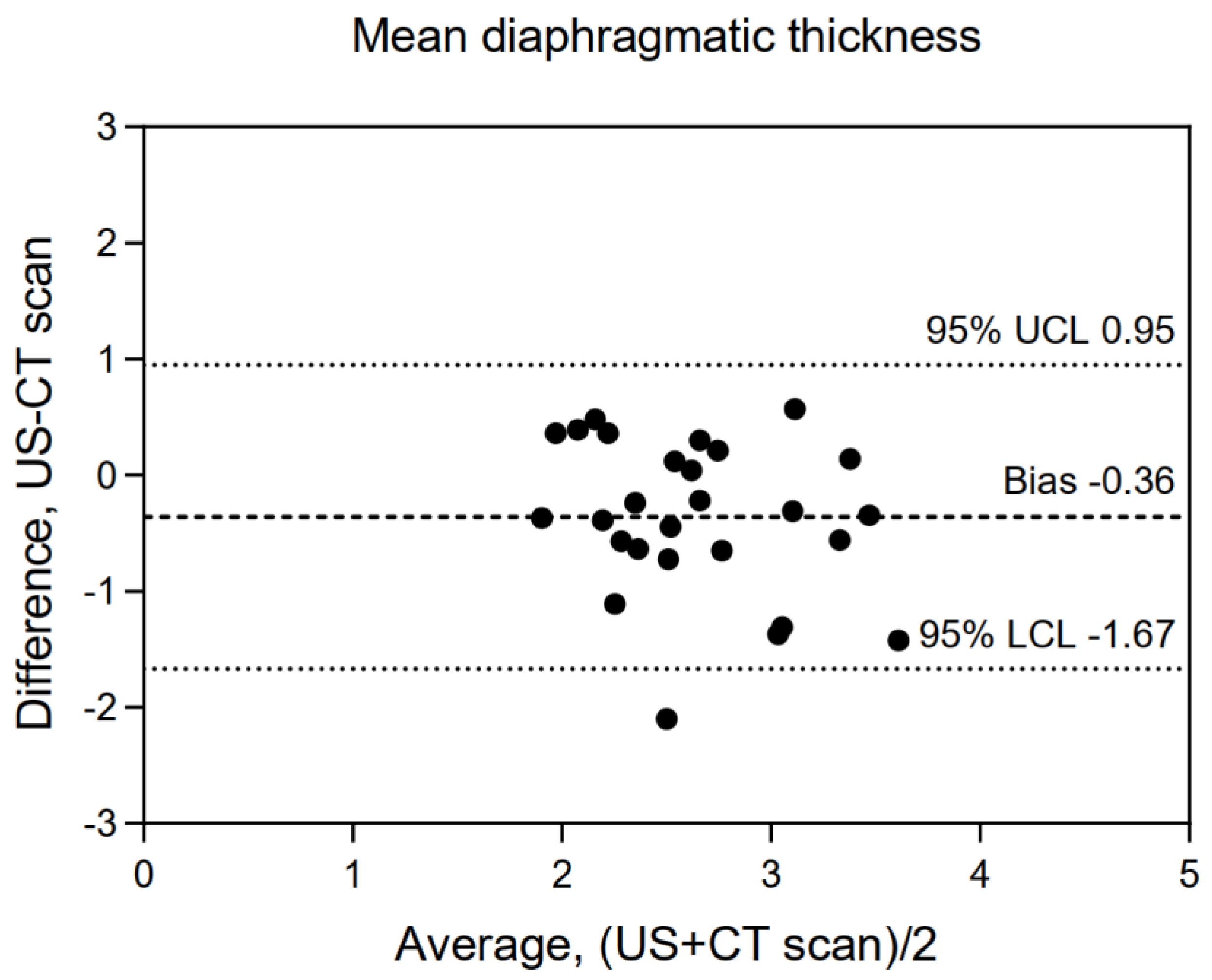
5.2. Coherence between Imaging Techniques
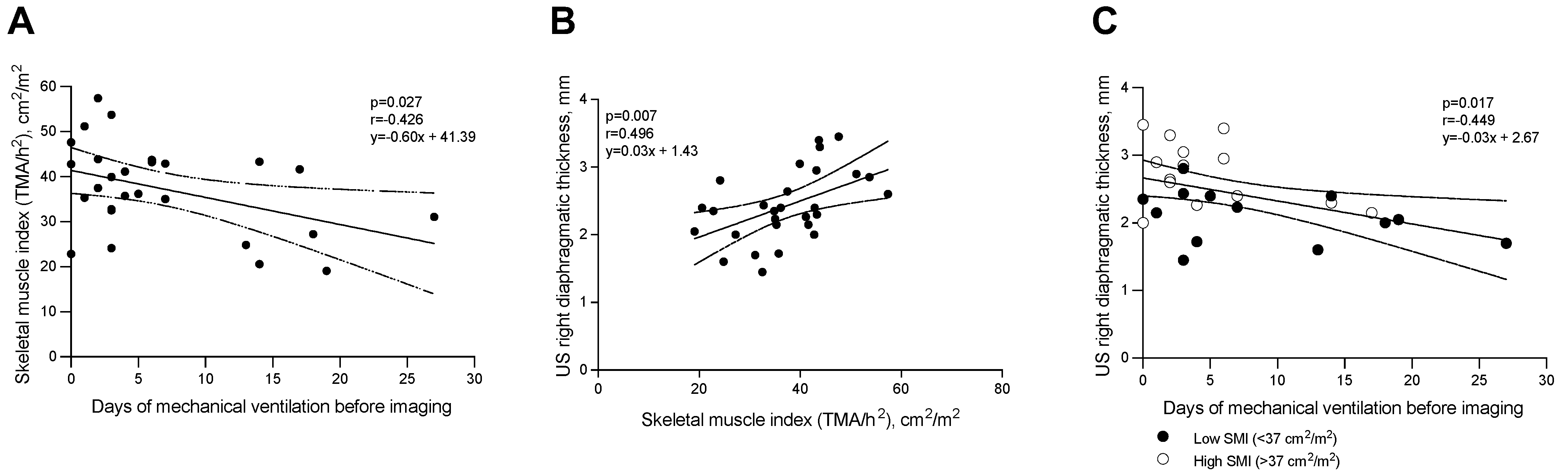
5.3. Correlation between Diaphragmatic Thickness and Duration of Mechanical Ventilation
5.4. Sarcopenia, Diaphragmatic Thickness, and Mechanical Ventilation
5.5. Comparison between ICU Patients and Healty Patients
6. Discussion
- In a mixed population of patients undergoing MV, the diaphragmatic thickness measured by CT scan in the left posterior pillars showed a moderate correlation with the measurements obtained using US;
- The diaphragmatic thickness evaluated by US was negatively correlated with the duration of controlled MV before enrollment while the mean diaphragmatic thickness showed a trend towards significance;
- The diaphragmatic thickness measured by US was moderately correlated with sarcopenia measured by CT scan and the smaller the thickness of the diaphragm was, the lower SMI was, a parameter that may suggest the presence of sarcopenia.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hermans, G.; Van den Berghe, G. Clinical review: Intensive care unit acquired weakness. Crit. Care Lond Engl. 2015, 19, 274. [Google Scholar] [CrossRef] [Green Version]
- Jaber, S.; Petrof, B.J.; Jung, B.; Chanques, G.; Berthet, J.P.; Rabuel, C.; Bouyabrine, H.; Courouble, P.; Koechlin-Ramonatxo, C.; Sebbane, M.; et al. Rapidly progressive diaphragmatic weakness and injury during mechanical ventilation in humans. Am. J. Respir. Crit. Care Med. 2011, 183, 364–371. [Google Scholar] [CrossRef]
- Levine, S.; Nguyen, T.; Taylor, N.; Friscia, M.E.; Budak, M.T.; Rothenberg, P.; Zhu, J.; Sachdeva, R.; Sonnad, S.; Kaiser, L.R.; et al. Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. N. Engl. J. Med. 2008, 358, 1327–1335. [Google Scholar] [CrossRef] [PubMed]
- Vassilakopoulos, T.; Petrof, B.J. Ventilator-induced diaphragmatic dysfunction. Am. J. Respir. Crit. Care Med. 2004, 169, 336–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Jonghe, B.; Bastuji-Garin, S.; Sharshar, T.; Outin, H.; Brochard, L. Does ICU-Acquired paresis lengthen weaning from mechanical ventilation? Intensive Care Med. 2004, 30, 1117–1121. [Google Scholar] [CrossRef]
- Testelmans, D.; Maes, K.; Wouters, P.; Gosselin, N.; Deruisseau, K.; Powers, S.; Sciot, R.; Decramer, M.; Gayan-Ramirez, G. Rocuronium exacerbates mechanical ventilation-induced diaphragm dysfunction in rats. Crit. Care Med. 2006, 34, 3018–3023. [Google Scholar] [CrossRef] [PubMed]
- Sassoon, C.S.; Zhu, E.; Pham, H.T.; Nelson, R.S.; Fang, L.; Baker, M.J.; Caiozzo, V.J. Acute effects of high-dose methylprednisolone on diaphragm muscle function. Muscle Nerve 2008, 38, 1161–1172. [Google Scholar] [CrossRef]
- Ochala, J.; Renaud, G.; Llano Diez, M.; Banduseela, V.C.; Aare, S.; Ahlbeck, K.; Radell, P.J.; Eriksson, L.I.; Larsson, L. Diaphragm muscle weakness in an experimental porcine intensive care unit model. PLoS ONE 2011, 6, e20558. [Google Scholar] [CrossRef] [Green Version]
- Sassoon, C.S.; Zhu, E.; Fang, L.; Ramar, K.; Jiao, G.Y.; Caiozzo, V.J. Interactive effects of corticosteroid and mechanical ventilation on diaphragm muscle function. Muscle Nerve 2011, 43, 103–111. [Google Scholar] [CrossRef]
- American Thoracic Society/European Respiratory Society. ATS/ERS Statement on respiratory muscle testing. Am. J. Respir. Crit. Care Med. 2002, 166, 518–624. [Google Scholar] [CrossRef]
- Hermans, G.; Agten, A.; Testelmans, D.; Decramer, M.; Gayan-Ramirez, G. Increased duration of mechanical ventilation is associated with decreased diaphragmatic force: A prospective observational study. Crit. Care Lond Engl. 2010, 14, R127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laghi, F.; Cattapan, S.E.; Jubran, A.; Parthasarathy, S.; Warshawsky, P.; Choi, Y.S.; Tobin, M.J. Is weaning failure caused by low-frequency fatigue of the diaphragm? Am. J. Respir. Crit. Care Med. 2003, 167, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Doorduin, J.; van Hees, H.W.H.; van der Hoeven, J.G.; Heunks, L.M. Monitoring of the respiratory muscles in the critically ill. Am. J. Respir. Crit. Care Med. 2013, 187, 20–27. [Google Scholar] [CrossRef]
- Goligher, E.C.; Laghi, F.; Detsky, M.E.; Farias, P.; Murray, A.; Brace, D.; Brochard, L.J.; Bolz, S.S.; Rubenfeld, G.D.; Kavanagh, B.P.; et al. Measuring diaphragm thickness with ultrasound in mechanically ventilated patients: Feasibility, reproducibility and validity. Intensive Care Med. 2015, 41, 642–649. [Google Scholar] [CrossRef]
- Goligher, E.C.; Fan, E.; Herridge, M.S.; Murray, A.; Vorona, S.; Brace, D.; Rittayamai, N.; Lanys, A.; Tomlinson, G.; Singh, J.M.; et al. Evolution of Diaphragm Thickness during Mechanical Ventilation. Impact of Inspiratory Effort. Am. J. Respir. Crit. Care Med. 2015, 192, 1080–1088. [Google Scholar] [CrossRef]
- Schepens, T.; Verbrugghe, W.; Dams, K.; Corthouts, B.; Parizel, P.M.; Jorens, P.G. The course of diaphragm atrophy in ventilated patients assessed with ultrasound: A longitudinal cohort study. Crit. Care Lond Engl. 2015, 19, 422. [Google Scholar] [CrossRef] [Green Version]
- Matamis, D.; Soilemezi, E.; Tsagourias, M.; Akoumianaki, E.; Dimassi, S.; Boroli, F.; Richard, J.C.; Brochard, L. Sonographic evaluation of the diaphragm in critically ill patients. Technique and clinical applications. Intensive Care Med. 2013, 39, 801–810. [Google Scholar] [CrossRef]
- Poole, D.C.; Sexton, W.L.; Farkas, G.A.; Powers, S.K.; Reid, M.B. Diaphragm structure and function in health and disease. Med. Sci. Sports Exerc. 1997, 29, 738–754. [Google Scholar] [CrossRef] [PubMed]
- Bellani, G.; Rouby, J.J.; Constantin, J.M.; Pesenti, A. Looking closer at acute respiratory distress syndrome: The role of advanced imaging techniques. Curr. Opin. Crit. Care 2017, 23, 30–37. [Google Scholar] [CrossRef]
- Peterson, S.J.; Braunschweig, C.A. Prevalence of sarcopenia and associated outcomes in the clinical setting. Nutr. Clin. Pract. 2016, 31, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Toptas, M.; Yalcin, M.; Akkoc, İ.; Demir, E.; Metin, C.; Savas, Y.; Kalyoncuoglu, M.; Can, M.M. The relation between sarcopenia and mortality in patients at intensive care unit. Biomed Res. Int. 2018, 2018, 5263208. [Google Scholar] [CrossRef] [PubMed]
- Ligthart-Melis, G.C.; Luiking, Y.C.; Kakourou, A.; Cederholm, T.; Maier, A.B.; de van der Schueren, M.A.E. Frailty, sarcopenia, and malnutrition frequently (co-)occur in hospitalized older adults: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2020, 21, 1216–1228. [Google Scholar] [CrossRef] [PubMed]
- Giani, M.; Rezoagli, E.; Grassi, A.; Porta, M.; Riva, L.; Famularo, S.; Barbaro, A.; Bernasconi, D.; Ippolito, D.; Bellani, G.; et al. Low skeletal muscle index and myosteatosis as predictors of mortality in critically ill surgical patients. Nutrition 2022, 101, 111687. [Google Scholar] [CrossRef] [PubMed]
- Rangel, E.L.; Rios-Diaz, A.J.; Uyeda, J.W.; Castillo-Angeles, M.; Cooper, Z.; Olufajo, O.A.; Salim, A.; Sodickson, A.D. Sarcopenia increases risk of long-term mortality in elderly patients undergoing emergency abdominal surgery. J. Trauma Acute Care Surg. 2017, 83, 1179–1186. [Google Scholar] [CrossRef]
- Zhang, X.M.; Zhang, W.W.; Yu, X.Z.; Dou, Q.L.; Cheng, A.S. Comparing the performance of SOFA, TPA combined with SOFA and APACHE-II for predicting ICU mortality in critically ill surgical patients: A secondary analysis. Clin. Nutr. 2020, 39, 2902–2909. [Google Scholar] [CrossRef]
- Kubiak, C.A.; Ranganathan, K.; Matusko, N.; Jacobson, J.A.; Wang, S.C.; Park, P.K.; Levi, B.L. Computed tomography evidence of psoas muscle atrophy without concomitant tendon wasting in early sepsis. J. Surg. Res. 2019, 234, 210–216. [Google Scholar] [CrossRef]
- Tapper, E.B.; Zhang, P.; Garg, R.; Nault, T.; Leary, K.; Krishnamurthy, V.; Su, G.L. Body composition predicts mortality and decompensation in compensated cirrhosis patients: A prospective cohort study. JHEP Rep. 2020, 2, 100061. [Google Scholar] [CrossRef] [Green Version]
- Nemec, U.; Heidinger, B.; Sokas, C.; Chu, L.; Eisenberg, R.L. Diagnosing Sarcopenia on Thoracic Computed Tomography: Quantitative Assessment of Skeletal Muscle Mass in Patients Undergoing Transcatheter Aortic Valve Replacement. Acad. Radiol. 2017, 24, 1154–1161. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative.The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [Green Version]
- Iochum, S.; Ludig, T.; Walter, F.; Sebbag, H.; Grosdidier, G.; Blum, A.G. Imaging of diaphragmatic injury: A diagnostic challenge? Radiographics 2002, 22, S103–S116. [Google Scholar] [CrossRef]
- Magu, S.; Agarwal, S.; Singla, S. Computed Tomography in the Evaluation of Diaphragmatic Hernia following Blunt Trauma. Indian J. Surg. 2012, 74, 288–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, B.; Nougaret, S.; Conseil, M.; Coisel, Y.; Futier, E.; Chanques, G.; Molinari, N.; Lacampagne, A.; Matecki, S.; Jaber, S. Sepsis is associated with a preferential diaphragmatic atrophy: A critically ill patient study using tridimensional computed tomography. Anesthesiology 2014, 120, 1182–1191. [Google Scholar] [CrossRef] [PubMed]
- Loosen, S.H.; Schulze-Hagen, M.; Püngel, T.; Bündgens, L.; Wirtz, T.; Kather, J.N.; Vucur, M.; Paffenholz, P.; Demir, M.; Bruners, P.; et al. Skeletal Muscle Composition Predicts Outcome in Critically Ill Patients. Crit. Care Explor. 2020, 2, e0171. [Google Scholar] [CrossRef]
- Eşme, M.; Karcıoğlu, O.; Öncel, A.; Ayçiçek, G.Ş.; Deniz, O.; Ulaşlı, S.S.; Köksal, D.; Doğu, B.B.; Cankurtaran, M.; Halil, M. Ultrasound Assessment of Sarcopenia in Patients With Sarcoidosis. J. Ultrasound Med. 2021, 41, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Deniz, O.; Coteli, S.; Karatoprak, N.B.; Pence, M.C.; Varan, H.D.; Kizilarslanoglu, M.C.; Oktar, S.O.; Goker, B. Diaphragmatic muscle thickness in older people with and without sarcopenia. Aging Clin. Exp. Res. 2021, 33, 573–580. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
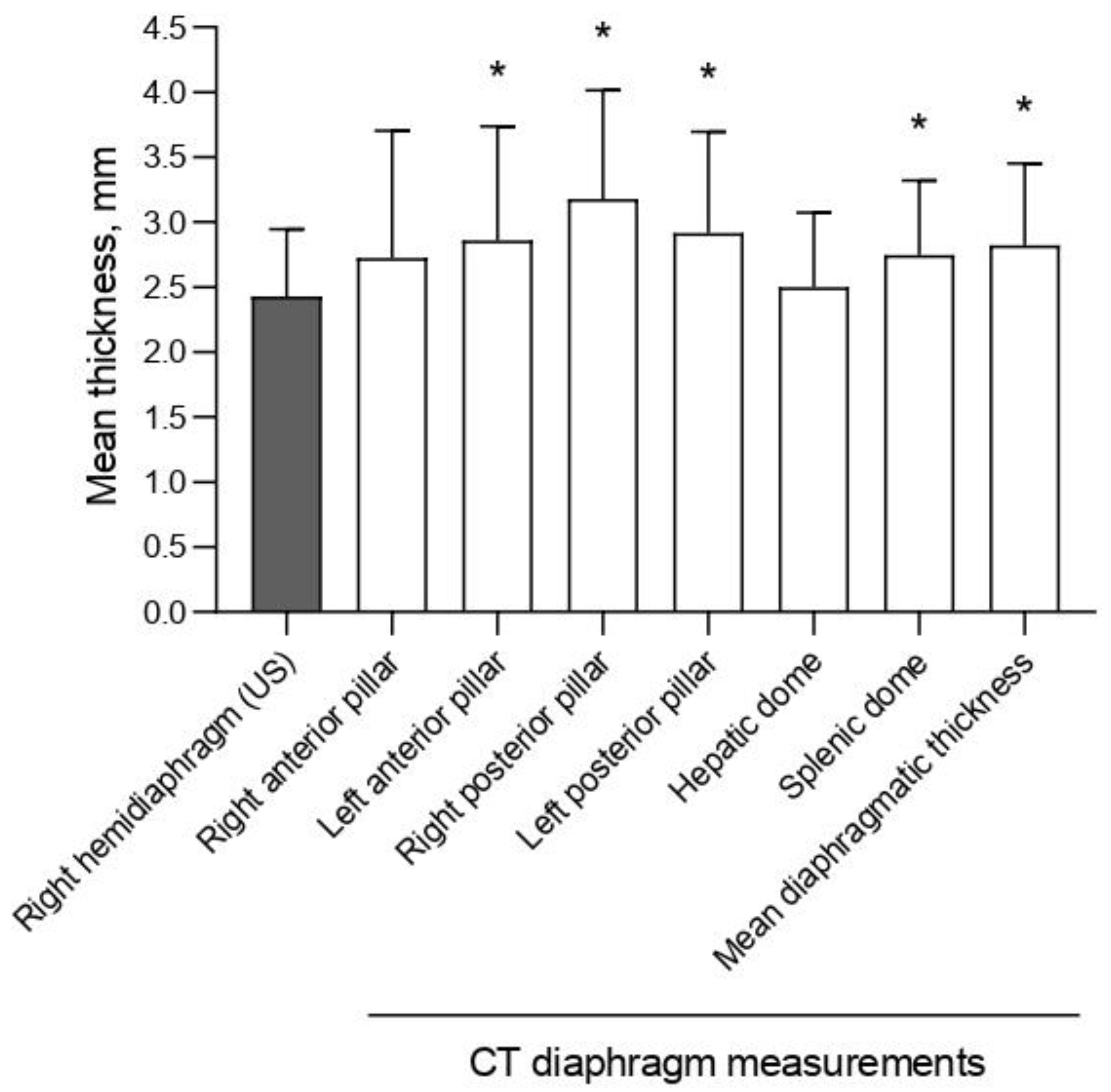
| Diaphragmatic Areas Sampled by CT Scan | Mean Thickness (mm) | Correlation with US Thickness (r) | |
|---|---|---|---|
| r | p-Value | ||
| Right anterior pillar | 2.73 ± 0.98 | 0.346 | 0.072 |
| Right posterior pillar | 3.18 ± 0.84 | 0.310 | 0.108 |
| Hepatic dome | 2.50 ± 0.57 | 0.163 | 0.408 |
| Left anterior pillar | 2.86 ± 0.88 | 0.081 | 0.682 |
| Left posterior pillar | 2.91 ± 0.78 | 0.488 | 0.008 |
| Splenic dome | 2.75 ± 0.57 | 0.287 | 0.139 |
| Mean diaphragmatic thickness | 2.82 ± 0.63 | 0.343 | 0.074 |
| US right hemidiaphragm | 2.44 ± 0.52 | / | / |
| Duration of MV | ||||||
|---|---|---|---|---|---|---|
| Total | Controlled | Assisted | ||||
| r | p-Value | r | p-Value | r | p-Value | |
| CT scan right anterior pillar | −0.332 | 0.084 | −0.412 | 0.029 | −0.033 | 0.868 |
| CT scan right posterior pillar | 0 | 0.984 | −0.111 | 0.573 | 0.140 | 0.477 |
| CT scan hepatic dome | 0 | 0.972 | −0.184 | 0.349 | 0.231 | 0.238 |
| CT scan heft anterior pillar | −0.118 | 0.550 | −0.246 | 0.208 | 0.120 | 0.544 |
| CT scan left posterior pillar | −0.184 | 0.348 | −0.358 | 0.061 | 0.153 | 0.437 |
| CT scan splenic dome | −0.349 | 0.069 | −0.428 | 0.023 | −0.040 | 0.838 |
| CT scan mean diaphragmatic thickness | −0.206 | 0.294 | −0.353 | 0.065 | 0.109 | 0.580 |
| US thickness | −0.371 | 0.047 | −0.449 | 0.017 | −0.063 | 0.745 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gatti, S.; Abbruzzese, C.; Ippolito, D.; Lombardi, S.; De Vito, A.; Gandola, D.; Meroni, V.; Sala, V.L.; Sironi, S.; Pesenti, A.; et al. Ultrasound Versus Computed Tomography for Diaphragmatic Thickness and Skeletal Muscle Index during Mechanical Ventilation. Diagnostics 2022, 12, 2890. https://doi.org/10.3390/diagnostics12112890
Gatti S, Abbruzzese C, Ippolito D, Lombardi S, De Vito A, Gandola D, Meroni V, Sala VL, Sironi S, Pesenti A, et al. Ultrasound Versus Computed Tomography for Diaphragmatic Thickness and Skeletal Muscle Index during Mechanical Ventilation. Diagnostics. 2022; 12(11):2890. https://doi.org/10.3390/diagnostics12112890
Chicago/Turabian StyleGatti, Stefano, Chiara Abbruzzese, Davide Ippolito, Sophie Lombardi, Andrea De Vito, Davide Gandola, Veronica Meroni, Vittoria Ludovica Sala, Sandro Sironi, Antonio Pesenti, and et al. 2022. "Ultrasound Versus Computed Tomography for Diaphragmatic Thickness and Skeletal Muscle Index during Mechanical Ventilation" Diagnostics 12, no. 11: 2890. https://doi.org/10.3390/diagnostics12112890